

Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal Infections (PANDAS): Myth or Reality? The State of the Art on a Controversial Disease
 , , , ,
, , , , 

Abstract
1. Introduction
2. Epidemiology
3. Pathophysiology
3.1. Animal Model Studies
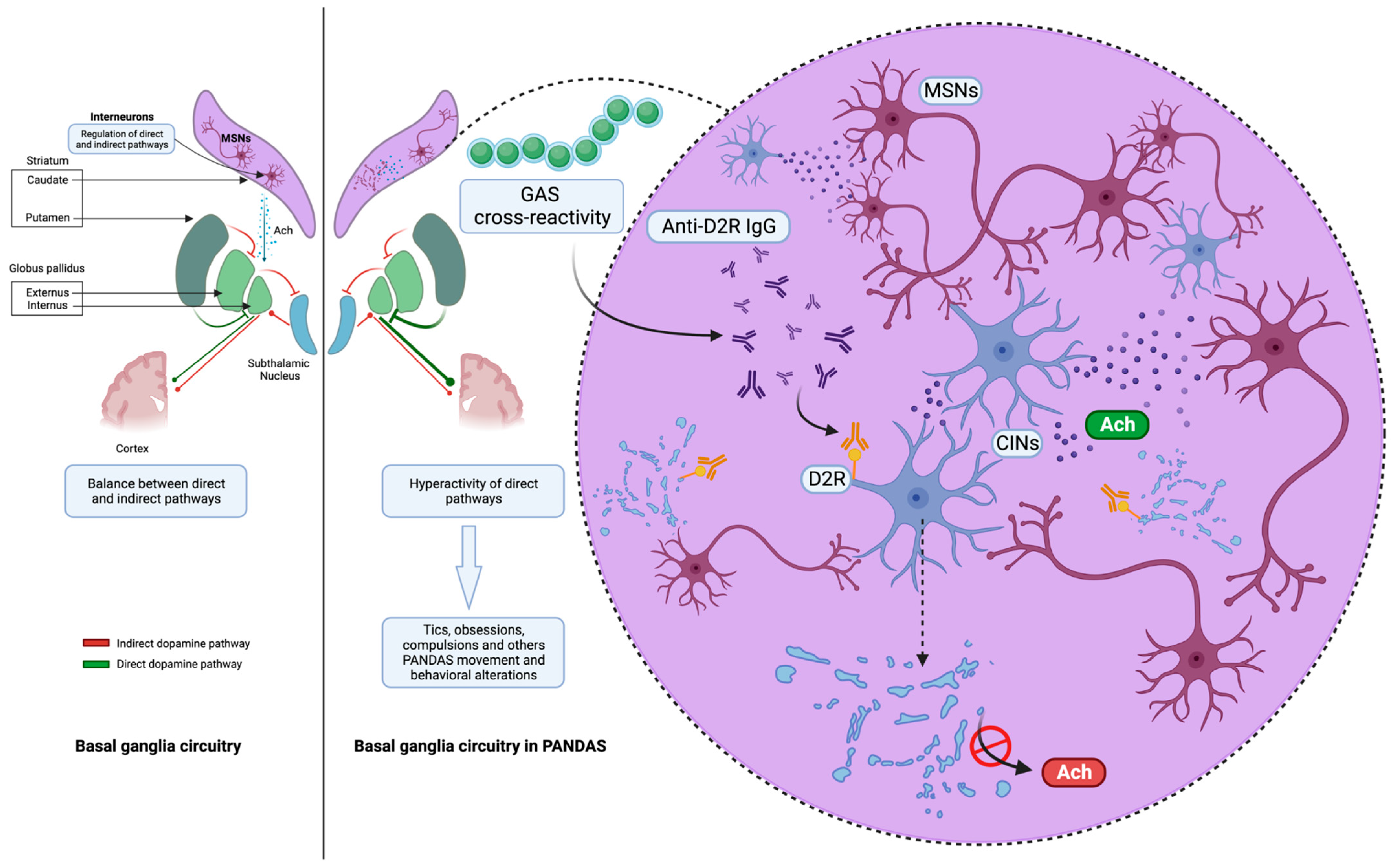
3.2. Striatal Cholinergic Interneurons: Latest Evidence of a New Key Player in PANDAS Pathophysiology
3.3. Imaging Studies
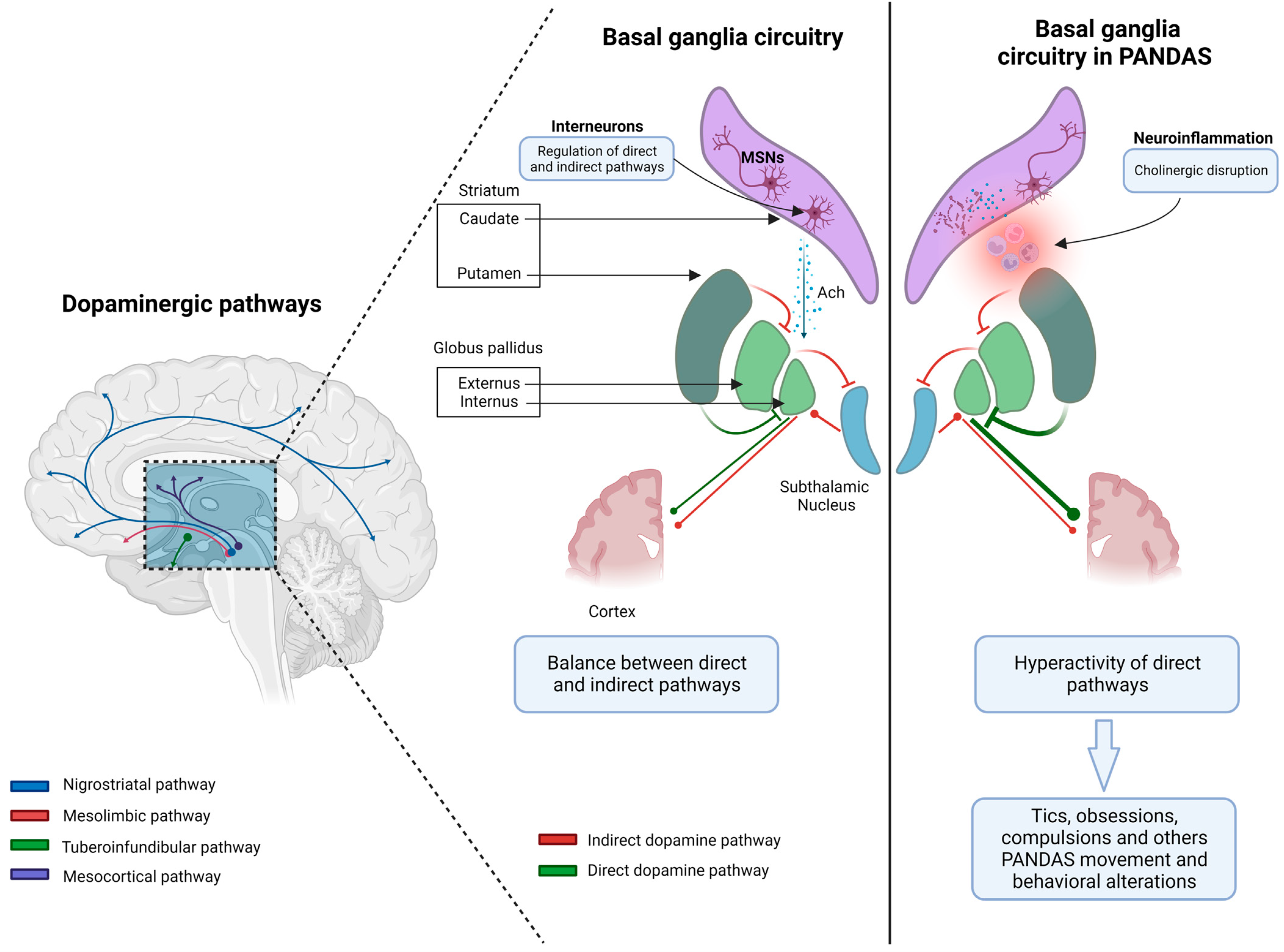
3.4. The Complex Network of Basal Ganglia: From Physiology to Pathophysiology
4. Clinical Features and Classification Criteria
- (1)
- Presence of OCD and/or a tic disorder;
- (2)
- Prepubertal symptom onset;
- (3)
- Acute onset of symptoms with a relapsing/remitting disease course;
- (4)
- A clear temporal association between GAS infection and symptom onset or exacerbation;
- (5)
- Association with other neurological abnormalities (particularly motoric hyperactivity and choreiform movements).
4.1. The Causal and Temporal Relationship between PANDAS and GAS Infection
- (1)
- GAS infection is common among children attending communities and schools.
- (2)
- Similarly, vocal and/or motor tics and OCD are not uncommon in children.
- (3)
- ASO and ADB may be found to be elevated in older GAS infections as well, resulting in false-positive tests.
- (4)
- ASO may rise due to chronic liver disease, hypergammaglobulinemia, and hypercholesterolemia [52].
4.2. Clinical Characteristics
5. Treatment Options and Disease Course
6. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Swedo, S.E.; Leonard, H.L.; Garvey, M.; Mittleman, B.; Allen, A.J.; Perlmutter, S.; Dow, S.; Zamkoff, J.; Dubbert, B.K.; Lougee, L. Pediatric Autoimmune Neuropsychiatric Disorders Associated With Streptococcal Infections: Clinical Description of the First 50 Cases. Am. J. Psychiatry 1998, 155, 264–271. [Google Scholar] [CrossRef]
- Dop, D.; Marcu, I.; Padureanu, R.; Niculescu, C.; Padureanu, V. Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal Infections (Review). Exp. Ther. Med. 2020, 21, 94. [Google Scholar] [CrossRef] [PubMed]
- Gewitz, M.H.; Baltimore, R.S.; Tani, L.Y.; Sable, C.A.; Shulman, S.T.; Carapetis, J.; Remenyi, B.; Taubert, K.A.; Bolger, A.F.; Beerman, L.; et al. Revision of the Jones Criteria for the Diagnosis of Acute Rheumatic Fever in the Era of Doppler Echocardiography: A Scientific Statement from the American Heart Association. Circulation 2015, 131, 1806–1818. [Google Scholar] [CrossRef] [PubMed]
- Oosterveer, D.M.; Overweg-Plandsoen, W.C.T.; Roos, R.A.C. Sydenham’s Chorea: A Practical Overview of the Current Literature. Pediatr. Neurol. 2010, 43, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.W.; Grant, J.E.; Kim, S.I.; Swanson, T.A.; Bernstein, G.A.; Jaszcz, W.B.; Williams, K.A.; Schlievert, P.M. A Possible Association of Recurrent Streptococcal Infections and Acute Onset of Obsessive-Compulsive Disorder. J. Neuropsychiatry Clin. Neurosci. 2004, 16, 252–260. [Google Scholar] [CrossRef] [PubMed]
- Cardoso, F. Sydenham’s Chorea. Handb. Clin. Neurol. 2011, 100, 221–229. [Google Scholar] [CrossRef]
- Mercadante, M.T.; Campos, M.C.; Marques-Dias, M.J.; Miguel, E.C.; Leckman, J. Vocal Tics in Sydenham’s Chorea. J. Am. Acad. Child Adolesc. Psychiatry 1997, 36, 305–306. [Google Scholar] [CrossRef]
- Perrin, E.M.; Murphy, M.L.; Casey, J.R.; Pichichero, M.E.; Runyan, D.K.; Miller, W.C.; Snider, L.A.; Swedo, S.E. Does Group A β-Hemolytic Streptococcal Infection Increase Risk for Behavioral and Neuropsychiatric Symptoms in Children? Arch. Pediatr. Adolesc. Med. 2004, 158, 848. [Google Scholar] [CrossRef]
- Chiarello, F.; Spitoni, S.; Hollander, E.; Matucci Cerinic, M.; Pallanti, S. An Expert Opinion on PANDAS/PANS: Highlights and Controversies. Int. J. Psychiatry Clin. Pract. 2017, 21, 91–98. [Google Scholar] [CrossRef]
- Wilbur, C.; Bitnun, A.; Kronenberg, S.; Laxer, R.M.; Levy, D.M.; Logan, W.J.; Shouldice, M.; Yeh, E.A. PANDAS/PANS in Childhood: Controversies and Evidence. Paediatr. Child Health 2019, 24, 85–91. [Google Scholar] [CrossRef]
- Prato, A.; Gulisano, M.; Scerbo, M.; Barone, R.; Vicario, C.M.; Rizzo, R. Diagnostic Approach to Pediatric Autoimmune Neuropsychiatric Disorders Associated With Streptococcal Infections (PANDAS): A Narrative Review of Literature Data. Front. Pediatr. 2021, 9, 746639. [Google Scholar] [CrossRef] [PubMed]
- Calaprice, D.; Tona, J.; Parker-Athill, E.C.; Murphy, T.K. A Survey of Pediatric Acute-Onset Neuropsychiatric Syndrome Characteristics and Course. J. Child Adolesc. Psychopharmacol. 2017, 27, 607–618. [Google Scholar] [CrossRef] [PubMed]
- Gagliano, A.; Carta, A.; Tanca, M.G.; Sotgiu, S. Pediatric Acute-Onset Neuropsychiatric Syndrome: Current Perspectives. Neuropsychiatr. Dis. Treat. 2023, 19, 1221–1250. [Google Scholar] [CrossRef] [PubMed]
- Swedo, S.E.; Leonard, H.L.; Rapoport, J.L. The Pediatric Autoimmune Neuropsychiatric Disorders Associated With Streptococcal Infection (PANDAS) Subgroup: Separating Fact From Fiction. Pediatrics 2004, 113, 907–911. [Google Scholar] [CrossRef]
- Cunningham, M.W.; Cox, C.J. Autoimmunity against Dopamine Receptors in Neuropsychiatric and Movement Disorders: A Review of Sydenham Chorea and Beyond. Acta Physiol. 2016, 216, 90–100. [Google Scholar] [CrossRef]
- Cox, C.J.; Sharma, M.; Leckman, J.F.; Zuccolo, J.; Zuccolo, A.; Kovoor, A.; Swedo, S.E.; Cunningham, M.W. Brain Human Monoclonal Autoantibody from Sydenham Chorea Targets Dopaminergic Neurons in Transgenic Mice and Signals Dopamine D2 Receptor: Implications in Human Disease. J. Immunol. Baltim. 2013, 191, 5524–5541. [Google Scholar] [CrossRef]
- Ben-Pazi, H.; Stoner, J.A.; Cunningham, M.W. Dopamine Receptor Autoantibodies Correlate with Symptoms in Sydenham’s Chorea. PLoS ONE 2013, 8, e73516. [Google Scholar] [CrossRef]
- Kirvan, C.A.; Swedo, S.E.; Heuser, J.S.; Cunningham, M.W. Mimicry and Autoantibody-Mediated Neuronal Cell Signaling in Sydenham Chorea. Nat. Med. 2003, 9, 914–920. [Google Scholar] [CrossRef]
- Hoffman, K.L.; Hornig, M.; Yaddanapudi, K.; Jabado, O.; Lipkin, W.I. A Murine Model for Neuropsychiatric Disorders Associated with Group A Beta-Hemolytic Streptococcal Infection. J. Neurosci. Off. J. Soc. Neurosci. 2004, 24, 1780–1791. [Google Scholar] [CrossRef]
- Yaddanapudi, K.; Hornig, M.; Serge, R.; De Miranda, J.; Baghban, A.; Villar, G.; Lipkin, W.I. Passive Transfer of Streptococcus-Induced Antibodies Reproduces Behavioral Disturbances in a Mouse Model of Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal Infection. Mol. Psychiatry 2010, 15, 712–726. [Google Scholar] [CrossRef]
- Brimberg, L.; Benhar, I.; Mascaro-Blanco, A.; Alvarez, K.; Lotan, D.; Winter, C.; Klein, J.; Moses, A.E.; Somnier, F.E.; Leckman, J.F.; et al. Behavioral, Pharmacological, and Immunological Abnormalities after Streptococcal Exposure: A Novel Rat Model of Sydenham Chorea and Related Neuropsychiatric Disorders. Neuropsychopharmacol. Off. Publ. Am. Coll. Neuropsychopharmacol. 2012, 37, 2076–2087. [Google Scholar] [CrossRef] [PubMed]
- Dale, R.C.; Merheb, V.; Pillai, S.; Wang, D.; Cantrill, L.; Murphy, T.K.; Ben-Pazi, H.; Varadkar, S.; Aumann, T.D.; Horne, M.K.; et al. Antibodies to Surface Dopamine-2 Receptor in Autoimmune Movement and Psychiatric Disorders. Brain 2012, 135, 3453–3468. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Liu, R.-J.; Fahey, S.; Frick, L.; Leckman, J.; Vaccarino, F.; Duman, R.S.; Williams, K.; Swedo, S.; Pittenger, C. Antibodies From Children With PANDAS Bind Specifically to Striatal Cholinergic Interneurons and Alter Their Activity. Am. J. Psychiatry 2021, 178, 48–64. [Google Scholar] [CrossRef] [PubMed]
- Bertran-Gonzalez, J.; Chieng, B.C.; Laurent, V.; Valjent, E.; Balleine, B.W. Striatal Cholinergic Interneurons Display Activity-Related Phosphorylation of Ribosomal Protein S6. PLoS ONE 2012, 7, e53195. [Google Scholar] [CrossRef]
- Lennington, J.B.; Coppola, G.; Kataoka-Sasaki, Y.; Fernandez, T.V.; Palejev, D.; Li, Y.; Huttner, A.; Pletikos, M.; Sestan, N.; Leckman, J.F.; et al. Transcriptome Analysis of the Human Striatum in Tourette Syndrome. Biol. Psychiatry 2016, 79, 372–382. [Google Scholar] [CrossRef]
- Kataoka, Y.; Kalanithi, P.S.A.; Grantz, H.; Schwartz, M.L.; Saper, C.; Leckman, J.F.; Vaccarino, F.M. Decreased Number of Parvalbumin and Cholinergic Interneurons in the Striatum of Individuals with Tourette Syndrome. J. Comp. Neurol. 2010, 518, 277–291. [Google Scholar] [CrossRef]
- Kumar, A.; Williams, M.T.; Chugani, H.T. Evaluation of Basal Ganglia and Thalamic Inflammation in Children With Pediatric Autoimmune Neuropsychiatric Disorders Associated With Streptococcal Infection and Tourette Syndrome: A Positron Emission Tomographic (PET) Study Using 11C-[R]-PK11195. J. Child Neurol. 2015, 30, 749–756. [Google Scholar] [CrossRef]
- Giedd, J.N.; Rapoport, J.L.; Garvey, M.A.; Perlmutter, S.; Swedo, S.E. MRI Assessment of Children with Obsessive-Compulsive Disorder or Tics Associated with Streptococcal Infection. Am. J. Psychiatry 2000, 157, 281–283. [Google Scholar] [CrossRef]
- Fazl, A.; Fleisher, J. Anatomy, Physiology, and Clinical Syndromes of the Basal Ganglia: A Brief Review. Semin. Pediatr. Neurol. 2018, 25, 2–9. [Google Scholar] [CrossRef]
- Benarroch, E.E. Effects of Acetylcholine in the Striatum: Recent Insights and Therapeutic Implications. Neurology 2012, 79, 274–281. [Google Scholar] [CrossRef]
- DeLong, M.; Wichmann, T. Update on Models of Basal Ganglia Function and Dysfunction. Park. Relat. Disord. 2009, 15, S237–S240. [Google Scholar] [CrossRef] [PubMed]
- Graybiel, A.M. Neurochemically Specified Subsystems in the Basal Ganglia. In Novartis Foundation Symposia; Evered, D., O’Connor, M., Eds.; Wiley: Hoboken, NJ, USA, 1984; pp. 114–149. ISBN 978-0-470-66425-4. [Google Scholar]
- Van Vulpen, E.H.S.; Van Der Kooy, D. Striatal Cholinergic Interneurons: Birthdates Predict Compartmental Localization. Dev. Brain Res. 1998, 109, 51–58. [Google Scholar] [CrossRef] [PubMed]
- Oldenburg, I.A.; Ding, J.B. Cholinergic Modulation of Synaptic Integration and Dendritic Excitability in the Striatum. Curr. Opin. Neurobiol. 2011, 21, 425–432. [Google Scholar] [CrossRef] [PubMed]
- Aliane, V.; Pérez, S.; Bohren, Y.; Deniau, J.-M.; Kemel, M.-L. Key Role of Striatal Cholinergic Interneurons in Processes Leading to Arrest of Motor Stereotypies. Brain 2011, 134, 110–118. [Google Scholar] [CrossRef]
- Kilbertus, S.; Brannan, R.; Sell, E.; Doja, A. No Cases of PANDAS on Follow-Up of Patients Referred to a Pediatric Movement Disorders Clinic. Front. Pediatr. 2014, 2, 104. [Google Scholar] [CrossRef]
- Jaspers-Fayer, F.; Han, S.H.J.; Chan, E.; McKenney, K.; Simpson, A.; Boyle, A.; Ellwyn, R.; Stewart, S.E. Prevalence of Acute-Onset Subtypes in Pediatric Obsessive-Compulsive Disorder. J. Child Adolesc. Psychopharmacol. 2017, 27, 332–341. [Google Scholar] [CrossRef]
- Gamucci, A.; Uccella, S.; Sciarretta, L.; D’Apruzzo, M.; Calevo, M.G.; Mancardi, M.M.; Veneselli, E.; De Grandis, E. PANDAS and PANS: Clinical, Neuropsychological, and Biological Characterization of a Monocentric Series of Patients and Proposal for a Diagnostic Protocol. J. Child Adolesc. Psychopharmacol. 2019, 29, 305–312. [Google Scholar] [CrossRef]
- Baj, J.; Sitarz, E.; Forma, A.; Wróblewska, K.; Karakuła-Juchnowicz, H. Alterations in the Nervous System and Gut Microbiota after β-Hemolytic Streptococcus Group A Infection—Characteristics and Diagnostic Criteria of PANDAS Recognition. Int. J. Mol. Sci. 2020, 21, 1476. [Google Scholar] [CrossRef]
- Thienemann, M.; Murphy, T.; Leckman, J.; Shaw, R.; Williams, K.; Kapphahn, C.; Frankovich, J.; Geller, D.; Bernstein, G.; Chang, K.; et al. Clinical Management of Pediatric Acute-Onset Neuropsychiatric Syndrome: Part I—Psychiatric and Behavioral Interventions. J. Child Adolesc. Psychopharmacol. 2017, 27, 566–573. [Google Scholar] [CrossRef]
- Mell, L.K.; Davis, R.L.; Owens, D. Association between Streptococcal Infection and Obsessive-Compulsive Disorder, Tourette’s Syndrome, and Tic Disorder. Pediatrics 2005, 116, 56–60. [Google Scholar] [CrossRef]
- Murphy, T.K.; Snider, L.A.; Mutch, P.J.; Harden, E.; Zaytoun, A.; Edge, P.J.; Storch, E.A.; Yang, M.C.K.; Mann, G.; Goodman, W.K.; et al. Relationship of Movements and Behaviors to Group A Streptococcus Infections in Elementary School Children. Biol. Psychiatry 2007, 61, 279–284. [Google Scholar] [CrossRef] [PubMed]
- Orlovska, S.; Vestergaard, C.H.; Bech, B.H.; Nordentoft, M.; Vestergaard, M.; Benros, M.E. Association of Streptococcal Throat Infection With Mental Disorders: Testing Key Aspects of the PANDAS Hypothesis in a Nationwide Study. JAMA Psychiatry 2017, 74, 740–746. [Google Scholar] [CrossRef] [PubMed]
- Leckman, J.F.; King, R.A.; Gilbert, D.L.; Coffey, B.J.; Singer, H.S.; Dure, L.S.; Grantz, H.; Katsovich, L.; Lin, H.; Lombroso, P.J.; et al. Streptococcal Upper Respiratory Tract Infections and Exacerbations of Tic and Obsessive-Compulsive Symptoms: A Prospective Longitudinal Study. J. Am. Acad. Child Adolesc. Psychiatry 2011, 50, 108–118. [Google Scholar] [CrossRef] [PubMed]
- Kurlan, R.; Johnson, D.; Kaplan, E.L.; Tourette Syndrome Study Group. Streptococcal Infection and Exacerbations of Childhood Tics and Obsessive-Compulsive Symptoms: A Prospective Blinded Cohort Study. Pediatrics 2008, 121, 1188–1197. [Google Scholar] [CrossRef]
- Nielsen, M.Ø.; Köhler-Forsberg, O.; Hjorthøj, C.; Benros, M.E.; Nordentoft, M.; Orlovska-Waast, S. Streptococcal Infections and Exacerbations in PANDAS: A Systematic Review and Meta-Analysis. Pediatr. Infect. Dis. J. 2019, 38, 189–194. [Google Scholar] [CrossRef]
- Delice, S. Detection of Anti- DNase B Antibody Upper Normal Values in Children’s Age Groups Who Were Admitted to Hospital with Noninfectious Reasons. North. Clin. Istanb. 2015, 2, 136–141. [Google Scholar] [CrossRef][Green Version]
- Sen, E.S.; Ramanan, A.V. How to Use Antistreptolysin O Titre. Arch. Dis. Child.-Educ. Pract. Ed. 2014, 99, 231–237. [Google Scholar] [CrossRef]
- Cohen, J.F.; Bertille, N.; Cohen, R.; Chalumeau, M. Rapid Antigen Detection Test for Group A Streptococcus in Children with Pharyngitis. Cochrane Database Syst. Rev. 2016, 7, CD010502. [Google Scholar] [CrossRef]
- Chang, K.; Frankovich, J.; Cooperstock, M.; Cunningham, M.W.; Latimer, M.E.; Murphy, T.K.; Pasternack, M.; Thienemann, M.; Williams, K.; Walter, J.; et al. Clinical Evaluation of Youth with Pediatric Acute-Onset Neuropsychiatric Syndrome (PANS): Recommendations from the 2013 PANS Consensus Conference. J. Child Adolesc. Psychopharmacol. 2015, 25, 3–13. [Google Scholar] [CrossRef]
- Feigin, R.D. (Ed.) Feigin & Cherry’s Textbook of Pediatric Infectious Diseases, 6th ed.; Saunders/Elsevier: Philadelphia, PA, USA, 2009; ISBN 978-1-4160-4044-6. [Google Scholar]
- Shet, A.; Kaplan, E.L. Clinical Use and Interpretation of Group A Streptococcal Antibody Tests: A Practical Approach for the Pediatrician or Primary Care Physician. Pediatr. Infect. Dis. J. 2002, 21, 420–426. [Google Scholar] [CrossRef]
- Johnson, D.R.; Kurlan, R.; Leckman, J.; Kaplan, E.L. The Human Immune Response to Streptococcal Extracellular Antigens: Clinical, Diagnostic, and Potential Pathogenetic Implications. Clin. Infect. Dis. 2010, 50, 481–490. [Google Scholar] [CrossRef] [PubMed]
- Jadah, R.H.S.; Mujeeb, A.A. Neuropsychiatric Symptoms Following Sore Throat in a Young Boy. BMJ Case Rep. 2019, 12, e227540. [Google Scholar] [CrossRef] [PubMed]
- Murphy, T.K.; Kurlan, R.; Leckman, J. The Immunobiology of Tourette’s Disorder, Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcus, and Related Disorders: A Way Forward. J. Child Adolesc. Psychopharmacol. 2010, 20, 317–331. [Google Scholar] [CrossRef] [PubMed]
- Allen, A.J.; Leonard, H.L.; Swedo, S.E. Case Study: A New Infection-Triggered, Autoimmune Subtype of Pediatric OCD and Tourette’s Syndrome. J. Am. Acad. Child Adolesc. Psychiatry 1995, 34, 307–311. [Google Scholar] [CrossRef]
- Bernstein, G.A.; Victor, A.M.; Pipal, A.J.; Williams, K.A. Comparison of Clinical Characteristics of Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal Infections and Childhood Obsessive-Compulsive Disorder. J. Child Adolesc. Psychopharmacol. 2010, 20, 333–340. [Google Scholar] [CrossRef]
- Calkin, C.V.; Carandang, C.G. Certain Eating Disorders May Be a Neuropsychiatric Manifestation of PANDAS: Case Report. J. Can. Acad. Child Adolesc. Psychiatry 2007, 16, 132–135. [Google Scholar]
- Williams, K.A.; Swedo, S.E. Post-Infectious Autoimmune Disorders: Sydenham’s Chorea, PANDAS and Beyond. Brain Res. 2015, 1617, 144–154. [Google Scholar] [CrossRef]
- Murphy, M.L.; Pichichero, M.E. Prospective Identification and Treatment of Children With Pediatric Autoimmune Neuropsychiatric Disorder Associated With Group A Streptococcal Infection (PANDAS). Arch. Pediatr. Adolesc. Med. 2002, 156, 356. [Google Scholar] [CrossRef]
- Crealey, M.; Allen, N.M.; Webb, D.; Bouldin, A.; Mc Sweeney, N.; Peake, D.; Tirupathi, S.; Butler, K.; King, M.D. Sydenham’s Chorea: Not Gone but Perhaps Forgotten. Arch. Dis. Child. 2015, 100, 1160–1162. [Google Scholar] [CrossRef]
- Murphy, T.K.; Goodman, W.K.; Ayoub, E.M.; Voeller, K.K. On Defining Sydenham’s Chorea: Where Do We Draw the Line? Biol. Psychiatry 2000, 47, 851–857. [Google Scholar] [CrossRef]
- Leon, J.; Hommer, R.; Grant, P.; Farmer, C.; D’Souza, P.; Kessler, R.; Williams, K.; Leckman, J.F.; Swedo, S. Longitudinal Outcomes of Children with Pediatric Autoimmune Neuropsychiatric Disorder Associated with Streptococcal Infections (PANDAS). Eur. Child Adolesc. Psychiatry 2018, 27, 637–643. [Google Scholar] [CrossRef] [PubMed]
- Murphy, T.K.; Storch, E.A.; Lewin, A.B.; Edge, P.J.; Goodman, W.K. Clinical Factors Associated with Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal Infections. J. Pediatr. 2012, 160, 314–319. [Google Scholar] [CrossRef] [PubMed]
- Orefici, G.; Cardona, F.; Cox, C.J.; Cunningham, M.W. Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal Infections (PANDAS). In Streptococcus Pyogenes: Basic Biology to Clinical Manifestations [Internet]; University of Oklahoma Health Sciences Center: Oklahoma City, OK, USA, 2016. [Google Scholar]
- O’Dor, S.L.; Homayoun, S.; Downer, O.M.; Hamel, M.A.; Zagaroli, J.S.; Williams, K.A. A Survey of Demographics, Symptom Course, Family History, and Barriers to Treatment in Children with Pediatric Acute-Onset Neuropsychiatric Disorders and Pediatric Autoimmune Neuropsychiatric Disorder Associated with Streptococcal Infections. J. Child Adolesc. Psychopharmacol. 2022, 32, 476–487. [Google Scholar] [CrossRef] [PubMed]
- Burchi, E.; Pallanti, S. Antibiotics for PANDAS? Limited Evidence: Review and Putative Mechanisms of Action. Prim. Care Companion CNS Disord. 2018, 20, 26629. [Google Scholar] [CrossRef]
- Garvey, M.A.; Perlmutter, S.J.; Allen, A.J.; Hamburger, S.; Lougee, L.; Leonard, H.L.; Witowski, M.E.; Dubbert, B.; Swedo, S.E. A Pilot Study of Penicillin Prophylaxis for Neuropsychiatric Exacerbations Triggered by Streptococcal Infections. Biol. Psychiatry 1999, 45, 1564–1571. [Google Scholar] [CrossRef]
- Snider, L.A.; Lougee, L.; Slattery, M.; Grant, P.; Swedo, S.E. Antibiotic Prophylaxis with Azithromycin or Penicillin for Childhood-Onset Neuropsychiatric Disorders. Biol. Psychiatry 2005, 57, 788–792. [Google Scholar] [CrossRef]
- Wang, H.-C.; Lau, C.-I.; Lin, C.-C.; Chang, A.; Kao, C.-H. Group A Streptococcal Infections Are Associated With Increased Risk of Pediatric Neuropsychiatric Disorders: A Taiwanese Population-Based Cohort Study. J. Clin. Psychiatry 2016, 77, e848–e854. [Google Scholar] [CrossRef]
- Hesselmark, E.; Bejerot, S. Patient Satisfaction and Treatments Offered to Swedish Patients with Suspected Pediatric Acute-Onset Neuropsychiatric Syndrome and Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal Infections. J. Child Adolesc. Psychopharmacol. 2019, 29, 634–641. [Google Scholar] [CrossRef]
- Pavone, P.; Rapisarda, V.; Serra, A.; Nicita, F.; Spalice, A.; Parano, E.; Rizzo, R.; Maiolino, L.; Di Mauro, P.; Vitaliti, G.; et al. Pediatric Autoimmune Neuropsychiatric Disorder Associated with Group a Streptococcal Infection: The Role of Surgical Treatment. Int. J. Immunopathol. Pharmacol. 2014, 27, 371–378. [Google Scholar] [CrossRef]
- Perlmutter, S.J.; Leitman, S.F.; Garvey, M.A.; Hamburger, S.; Feldman, E.; Leonard, H.L.; Swedo, S.E. Therapeutic Plasma Exchange and Intravenous Immunoglobulin for Obsessive-Compulsive Disorder and Tic Disorders in Childhood. Lancet 1999, 354, 1153–1158. [Google Scholar] [CrossRef]
- Frankovich, J.; Swedo, S.; Murphy, T.; Dale, R.C.; Agalliu, D.; Williams, K.; Daines, M.; Hornig, M.; Chugani, H.; Sanger, T.; et al. Clinical Management of Pediatric Acute-Onset Neuropsychiatric Syndrome: Part II-Use of Immunomodulatory Therapies. J. Child Adolesc. Psychopharmacol. 2017, 27, 574–593. [Google Scholar] [CrossRef] [PubMed]
- Tucker, D.M.; Leckman, J.F.; Scahill, L.; Wilf, G.E.; LaCamera, R.; Cardona, L.; Cohen, P.; Heidmann, S.; Goldstein, J.; Judge, J.; et al. A Putative Poststreptococcal Case of OCD with Chronic Tic Disorder, Not Otherwise Specified. J. Am. Acad. Child Adolesc. Psychiatry 1996, 35, 1684–1691. [Google Scholar] [CrossRef] [PubMed]
- Beşiroğlu, L.; Ağargün, M.Y.; Ozbebit, O.; Sözen, M.; Dilek, I.; Güleç, M. Therapeutic response to plasmapheresis in four cases with obsessive-compulsive disorder and tic disorder triggered by streptococcal infections. Turk Psikiyatr. Derg. Turk. J. Psychiatry 2007, 18, 270–276. [Google Scholar]
- Hachiya, Y.; Miyata, R.; Tanuma, N.; Hongou, K.; Tanaka, K.; Shimoda, K.; Kanda, S.; Hoshino, A.; Hanafusa, Y.; Kumada, S.; et al. Autoimmune Neurological Disorders Associated with Group-A Beta-Hemolytic Streptococcal Infection. Brain Dev. 2013, 35, 670–674. [Google Scholar] [CrossRef]
- Sigra, S.; Hesselmark, E.; Bejerot, S. Treatment of PANDAS and PANS: A Systematic Review. Neurosci. Biobehav. Rev. 2018, 86, 51–65. [Google Scholar] [CrossRef]
- Weinstein, R. Therapeutic Apheresis in Neurological Disorders: A Survey of the Evidence in Support of Current Category I and II Indications for Therapeutic Plasma Exchange. J. Clin. Apher. 2008, 23, 196–201. [Google Scholar] [CrossRef]
- Williams, K.A.; Swedo, S.E.; Farmer, C.A.; Grantz, H.; Grant, P.J.; D’Souza, P.; Hommer, R.; Katsovich, L.; King, R.A.; Leckman, J.F. Randomized, Controlled Trial of Intravenous Immunoglobulin for Pediatric Autoimmune Neuropsychiatric Disorders Associated With Streptococcal Infections. J. Am. Acad. Child Adolesc. Psychiatry 2016, 55, 860–867. [Google Scholar] [CrossRef]
- Bellanti, J.A. The PANDAS/PANS Disorders. Is It Time for More Allergist-Immunologists to Get Involved? Allergy Asthma Proc. 2023, 44, 296–305. [Google Scholar] [CrossRef]
- Cocuzza, S.; Maniaci, A.; La Mantia, I.; Nocera, F.; Caruso, D.; Caruso, S.; Iannella, G.; Vicini, C.; Privitera, E.; Lechien, J.R.; et al. Obsessive-Compulsive Disorder in PANS/PANDAS in Children: In Search of a Qualified Treatment-A Systematic Review and Metanalysis. Children 2022, 9, 155. [Google Scholar] [CrossRef]
- Cooperstock, M.S.; Swedo, S.E.; Pasternack, M.S.; Murphy, T.K. Clinical Management of Pediatric Acute-Onset Neuropsychiatric Syndrome: Part III-Treatment and Prevention of Infections. J. Child Adolesc. Psychopharmacol. 2017, 27, 594–606. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Timing | Anti-Streptolisin O | Anti-DNAse B |
|---|---|---|
| Starting to increase (weeks) | 1 | 2 |
| Peak (weeks) | 3–5 | 6–8 |
| Starting to decrease (weeks) | 6–8 | 12 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
La Bella, S.; Scorrano, G.; Rinaldi, M.; Di Ludovico, A.; Mainieri, F.; Attanasi, M.; Spalice, A.; Chiarelli, F.; Breda, L. Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal Infections (PANDAS): Myth or Reality? The State of the Art on a Controversial Disease. Microorganisms 2023, 11, 2549. https://doi.org/10.3390/microorganisms11102549
La Bella S, Scorrano G, Rinaldi M, Di Ludovico A, Mainieri F, Attanasi M, Spalice A, Chiarelli F, Breda L. Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal Infections (PANDAS): Myth or Reality? The State of the Art on a Controversial Disease. Microorganisms. 2023; 11(10):2549. https://doi.org/10.3390/microorganisms11102549
Chicago/Turabian StyleLa Bella, Saverio, Giovanna Scorrano, Marta Rinaldi, Armando Di Ludovico, Francesca Mainieri, Marina Attanasi, Alberto Spalice, Francesco Chiarelli, and Luciana Breda. 2023. "Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal Infections (PANDAS): Myth or Reality? The State of the Art on a Controversial Disease" Microorganisms 11, no. 10: 2549. https://doi.org/10.3390/microorganisms11102549
APA StyleLa Bella, S., Scorrano, G., Rinaldi, M., Di Ludovico, A., Mainieri, F., Attanasi, M., Spalice, A., Chiarelli, F., & Breda, L. (2023). Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal Infections (PANDAS): Myth or Reality? The State of the Art on a Controversial Disease. Microorganisms, 11(10), 2549. https://doi.org/10.3390/microorganisms11102549