
Consortium of Indigenous Fecal Bacteria in the Treatment of Metabolic Syndrome

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Characteristics of the Study Participants
2.2. Ethics Approval
2.3. Study Design
2.4. Preparation of Indigenous Consortium
2.5. Intestinal Microbiota Study
2.6. Bacteriological Study of Indigenous Consortium
2.7. Quantitative Polymerase Chain Reaction
2.8. Microbiome (16S rRNA) Study
2.9. Biochemical Analysis
2.10. Physical Examination
2.11. Eating Behavior
2.12. Gastro Diary
2.13. Statistical Analysis
3. Results
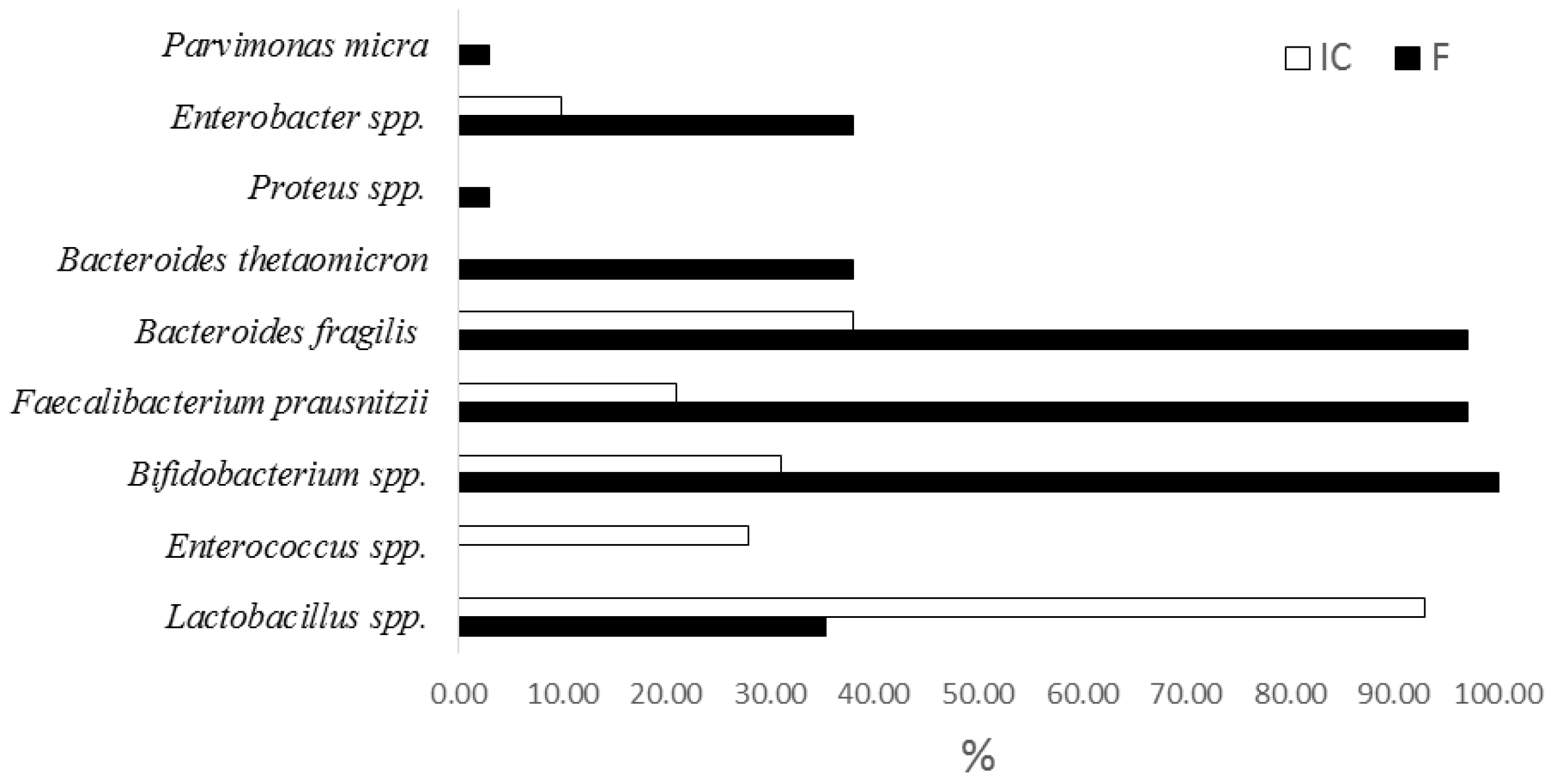
3.1. Indigenous Consortium Content
3.1.1. qPCR
3.1.2. Metagenome Study 16S rRNA
3.2. Influence of the Indigenous Consortium Consumption on the Condition of Patients with MS and Their Microbiota
3.2.1. Clinical and Laboratory Parameters before and after Therapy
Gastro Diaries
Eating Behavior
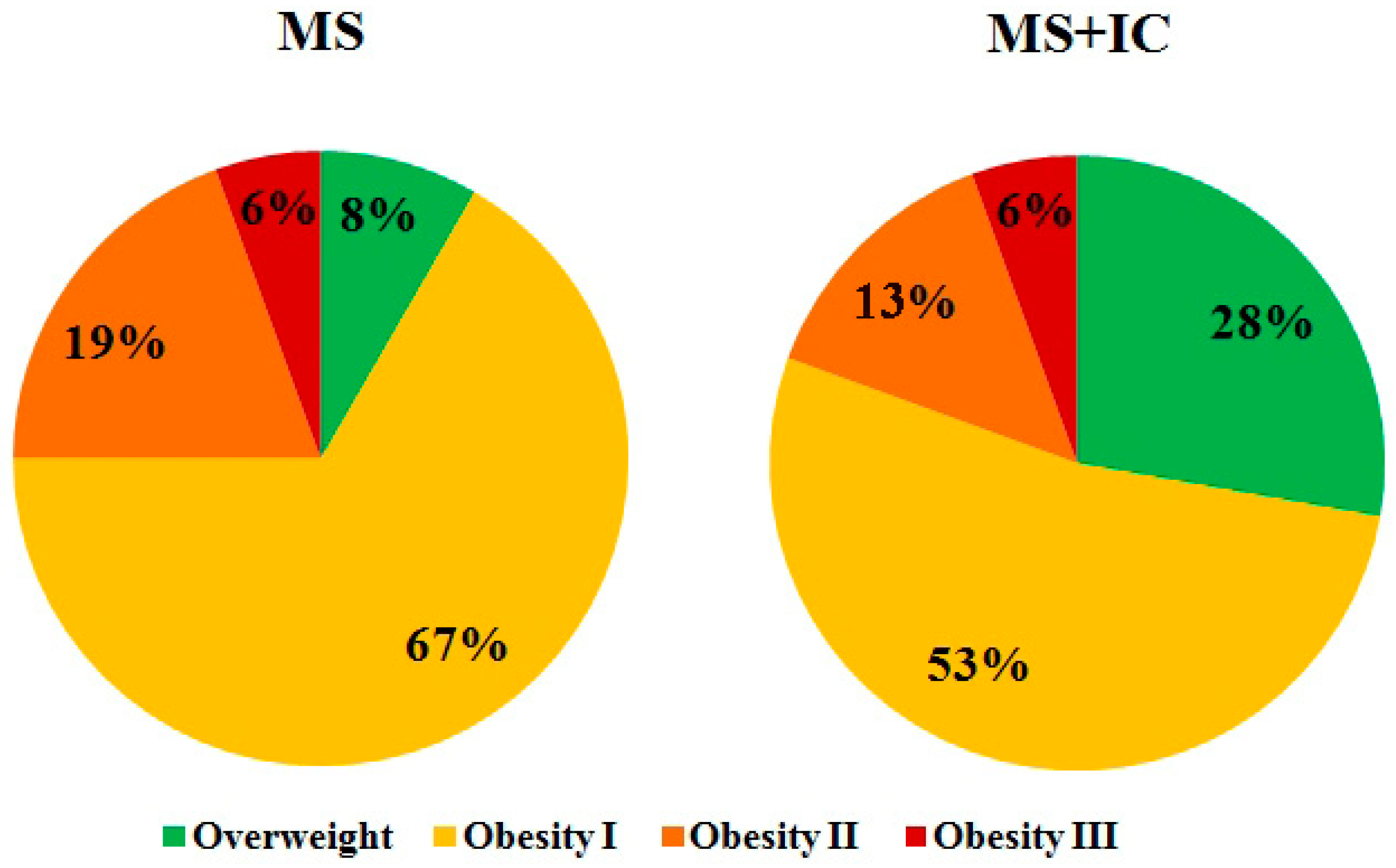
Antropometria Results for Evaluation of Obesity Symptoms Study
Biochemical Parameters
3.2.2. Microbiota Content before and after Therapy
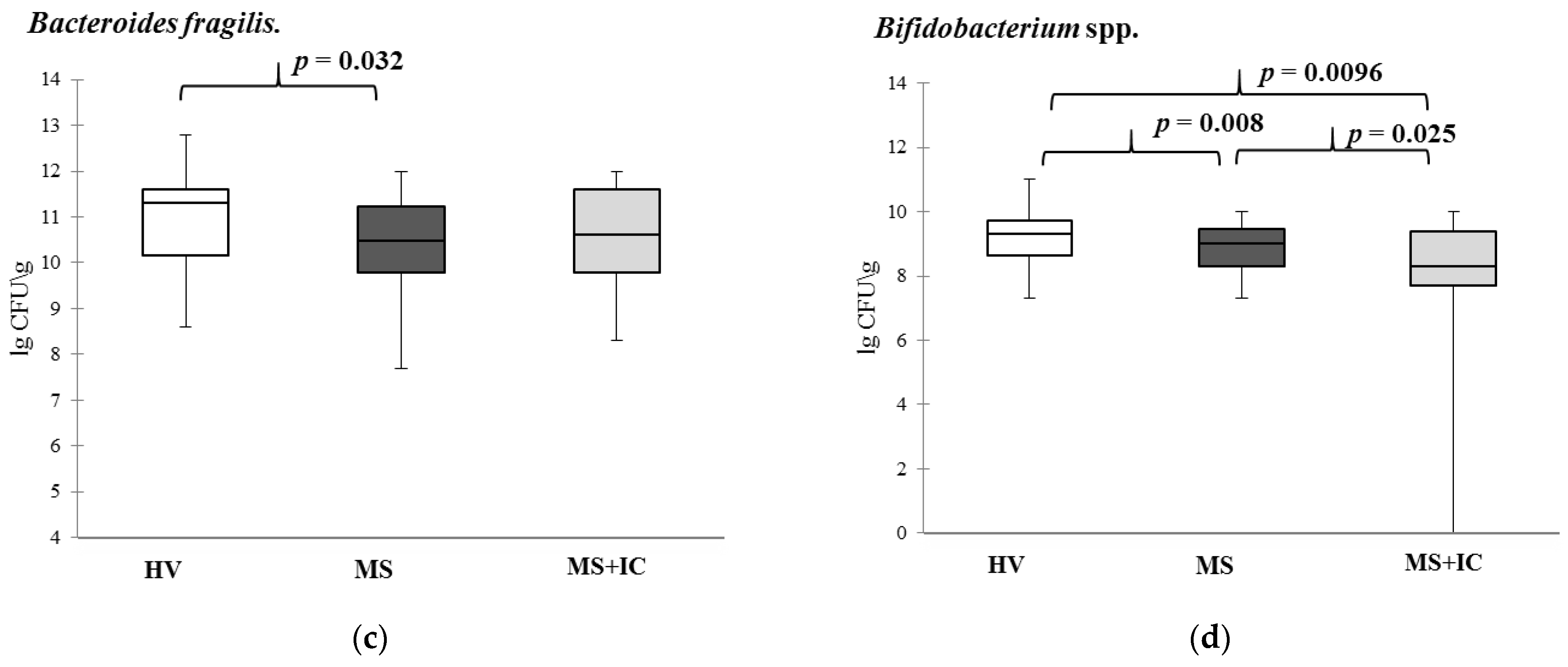
Quantitative Polymerase Chain Reaction
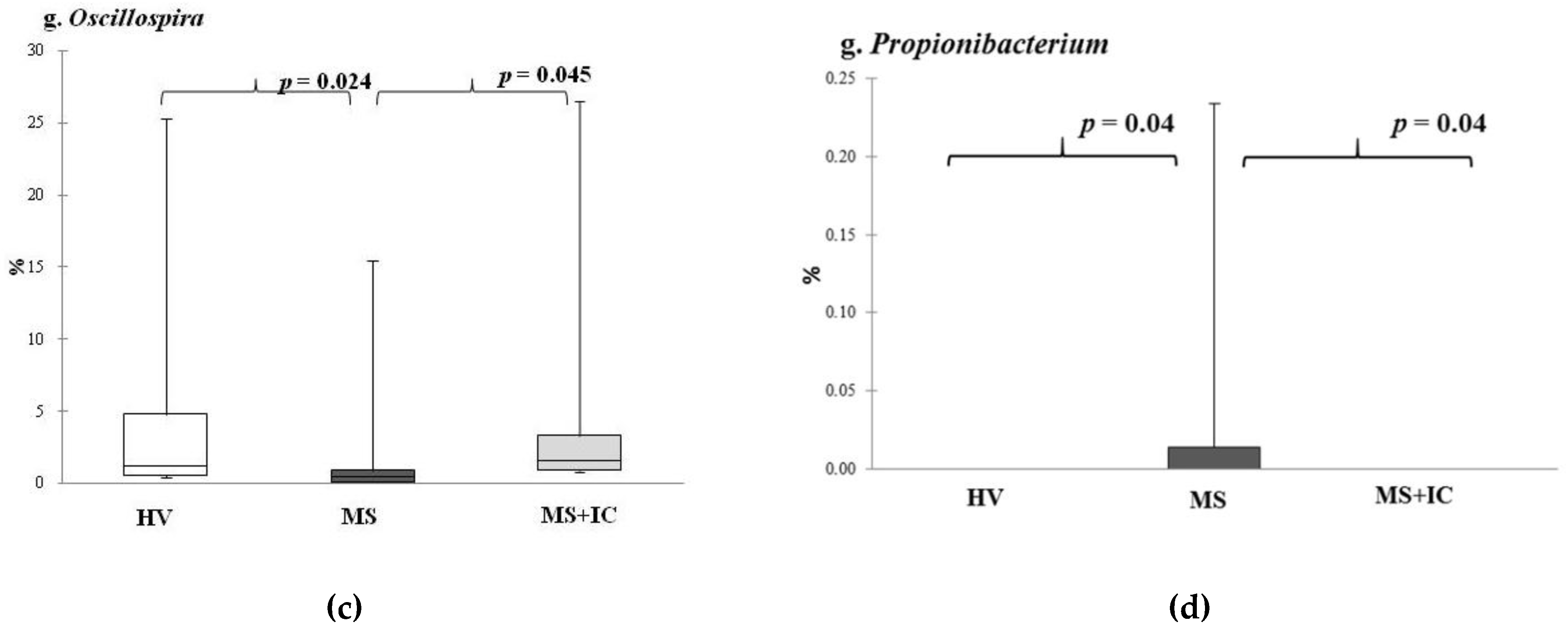
Metagenome 16S rRNA Study
3.3. Summary Results and Correlation Analysis between Bacterial Taxa and Clinic and Laboratory Parameters
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z. The metabolic syndrome. Lancet 2005, 365, 1415–1428. [Google Scholar] [CrossRef]
- Laaksonen, D.E.; Niskanen, L.; Lakka, H.M.; Lakka, T.A.; Uusitupa, M. Epidemiology and treatment of the metabolic syndrome. Ann. Med. 2004, 36, 332–346. [Google Scholar] [CrossRef] [PubMed]
- Kurmangulov, A.A.; Dorodneva, E.F.; Isakova, D.N. Functional activity of intestinal microbiota with metabolic syndrome. Obes. Metab. 2016, 13, 16–19. [Google Scholar] [CrossRef] [Green Version]
- Buttó, L.; Haller, D. Dysbiosis in intestinal inflammation: Cause or consequence. Int. J. Med. Microbiol. 2016, 306, 302–309. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.X.; Deng, X.R.; Zhang, C.H.; Yuan, H.J. Gut microbiota and metabolic syndrome. Chin. Med. J. 2020, 133, 808–816. [Google Scholar] [CrossRef] [PubMed]
- Santini, A.; Novellino, E. Nutraceuticals-shedding light on the grey area between pharmaceuticals and food. Expert Rev. Clin. Pharmacol. 2018, 11, 545–547. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Festi, D.; Schiumerini, R.; Eusebi, L.H.; Marasco, G.; Taddia, M.; Colecchia, A. Gut microbiota and metabolic syndrome. World J. Gastroenterol. 2014, 20, 16079–16094. [Google Scholar] [CrossRef]
- Solov’eva, O.I.; Simanenkov, V.I.; Suvorov, A.N.; Ermolenko, E.I.; Shumihina, I.A.; Svirido, D.A. The use of probiotics and autoprobiotics in the treatment of irritable bowel syndrome. Clin. Exp. Gastroenterol. 2017, 7, 115–120. [Google Scholar]
- Suvorov, A.; Karaseva, A.; Kotyleva, M.; Kondratenko, Y.; Lavrenova, N.; Korobeynikov, A.; Kozyrev, P.; Kramskaya, T.; Leontieva, G.; Kudryavtsev, I.; et al. Autoprobiotics as an approach for restoration of personalised microbiota. Front. Microbiol. 2018, 9, 1–9. [Google Scholar] [CrossRef]
- Gromova, L.V.; Ermolenko, E.I.; Sepp, A.L.; Dmitrieva, Y.V.; Alekseeva, A.S.; Lavrenova, N.S.; Kotyleva, M.P.; Kramskaya, T.A.; Karaseva, A.B.; Suvorov, A.N.; et al. Gut Digestive Function and Microbiome after Correction of Experimental Dysbiosis in Rats by Indigenous Bifidobacteria. Microorganisms 2021, 9, 522. [Google Scholar] [CrossRef]
- Suvorov, A.; Simanenkov, V.; Gromova, L.; Kolodjieva, V.; Tsapieva, A.; Chernish, A.; Solovieva, O.; Ermolenko, E. Enterococci as probiotics or autoprobiotics. In Prebiotics and Probiotics Potential for Human Health; Ivanova, I., Ed.; Paisi Hilendarski: Sofia, Bulgaria, 2011; pp. 104–112. [Google Scholar]
- de Groot, P.F.; Frissen, M.N.; de Clercq, N.C.; Nieuwdorp, M. Fecal microbiota transplantation in metabolic syndrome: History, present and future. Gut Microbes 2017, 8, 253–267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kahn, S.A.; Gorawara-Bhat, R.; Rubin, D.T. Fecal bacteriotherapy for ulcerative colitis: Patients are ready, are we? Inflamm. Bowel Dis. 2012, 18, 676–684. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [Green Version]
- Li, W.; Chang, Y. CD-HIT-OTU-MiSeq, an improved approach for clustering and analyzing paired end MiSeq 16S rRNA sequences. BioRxiv 2017, 153783. [Google Scholar] [CrossRef] [Green Version]
- DeSantis, T.; Hugenholtz, P.; Larsen, N.; Rojas, M.; Brodie, E.; Keller, K.; Huber, T.; Dalevi, D.; Hu, P.; Andersen, G. Greengenes, a chimera-checked 16S rRNA gene database and workbench compatible with ARB. Appl. Environ. Microbiol. 2006, 72, 5069–5072. [Google Scholar] [CrossRef] [Green Version]
- van Strien, T.; Frijters, J.E.R.; Bergers, G.P.A.; Defares, P.B. The Dutch Eating Behavior Questionnaire (DEBQ) for assessment of restrained, emotional, and external eating behavior. Int. J. Eat. Disord. 1986, 5, 295–315. [Google Scholar] [CrossRef]
- Simanenkov, V.; Tikhonov, S.; Lischuk, N. Treatment compliance at initial and maintenance therapy at gastroesophageal reflux disease. Russ. J. Gastroenterol. Hepatol. Coloproctol. 2017, 27, 29–34. [Google Scholar] [CrossRef]
- Yu, E.W.; Gao, L.; Stastka, P.; Cheney, M.C.; Mahabamunuge, J.; Torres Soto, M.; Ford, C.B.; Bryant, J.A.; Henn, M.R.; Hohmann, E.L. Fecal microbiota transplantation for the improvement of metabolism in obesity: The FMT-TRIM double-blind placebo-controlled pilot trial. PLoS Med. 2020, 17, e1003051. [Google Scholar] [CrossRef]
- Suez, J.; Zmora, N.; Segal, E.; Elinav, E. The pros, cons, and many unknowns of probiotics. Nat. Med. 2019, 25, 716–729. [Google Scholar] [CrossRef]
- Park, S.Y.; Seo, G.S. Fecal Microbiota Transplantation: Is It Safe? Clin. Endosc. 2021, 54, 157–160. [Google Scholar] [CrossRef]
- Cani, P.D.; Possemiers, S.; Van De Wiele, T.; Guiot, Y.; Everard, A.; Rottier, O.; Geurts, L.; Naslain, D.; Neyrinck, A.; Lambert, D.M.; et al. Changes in gut microbiota control inflammation in obese mice through a mechanism involving GLP-2-driven improvement of gut permeability. Gut 2009, 58, 1091–1103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cicero, A.F.G.; Fogacci, F.; Bove, M.; Giovannini, M.; Borghi, C. Impact of a short-term synbiotic supplementation on metabolic syndrome and systemic inflammation in elderly patients: A randomized placebo-controlled clinical trial. Eur. J. Nutr. 2021, 60, 655–663. [Google Scholar] [CrossRef] [PubMed]
- Rabiei, S.; Hedayati, M.; Rashidkhani, B.; Saadat, N.; Shakerhossini, R. The Effects of Synbiotic Supplementation on Body Mass Index, Metabolic and Inflammatory Biomarkers, and Appetite in Patients with Metabolic Syndrome: A Triple-Blind Randomized Controlled Trial. J. Diet. Suppl. 2019, 16, 294–306. [Google Scholar] [CrossRef]
- Lanthier, N.; Rodriguez, J.; Nachit, M.; Hiel, S.; Trefois, P.; Neyrinck, A.M.; Cani, P.D.; Bindels, L.B.; Thissen, J.P.; Delzenne, N.M. Microbiota analysis and transient elastography reveal new extra-hepatic components of liver steatosis and fibrosis in obese patients. Sci. Rep. 2021, 11, 1–14. [Google Scholar] [CrossRef]
- Garcia-Mantrana, I.; Selma-Royo, M.; Alcantara, C.; Collado, M.C. Shifts on gut microbiota associated to mediterranean diet adherence and specific dietary intakes on general adult population. Front. Microbiol. 2018, 9, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Gophna, U.; Konikoff, T.; Nielsen, H.B. Oscillospira and related bacteria—From metagenomic species to metabolic features. Environ. Microbiol. 2017, 19, 835–841. [Google Scholar] [CrossRef] [Green Version]
- Konikoff, T.; Gophna, U. Oscillospira: A central, enigmatic component of the human gut microbiota. Trends Microbiol. 2016, 24, 523–524. [Google Scholar] [CrossRef]
- Beaumont, M.; Goodrich, J.K.; Jackson, M.A.; Yet, I.; Davenport, E.R.; Vieira-Silva, S.; Debelius, J.; Pallister, T.; Mangino, M.; Raes, J.; et al. Heritable components of the human fecal microbiome are associated with visceral fat. Genome Biol. 2016, 17, 189. [Google Scholar] [CrossRef] [Green Version]
- Yang, J.; Li, Y.; Wen, Z.; Liu, W.; Meng, L.; Huang, H. Oscillospira—A candidate for the next-generation probiotics. Gut Microbes 2021, 13, 1987783. [Google Scholar] [CrossRef]
- Wexler, H.M. Bacteroides: The good, the bad, and the nitty-gritty. Clin. Microbiol. Rev. 2007, 20, 593–621. [Google Scholar] [CrossRef] [Green Version]
- Sun, F.; Zhang, Q.; Zhao, J.; Zhang, H.; Zhai, Q.; Chen, W. A potential species of next-generation probiotics? The dark and light sides of Bacteroides fragilis in health. Food Res. Int. 2019, 126, 108590. [Google Scholar] [CrossRef] [PubMed]
- Chatzidaki-Livanis, M.; Coyne, M.J.; Comstock, L.E. An antimicrobial protein of the gut symbiont Bacteroides fragilis with a MACPF domain of host immune proteins. Mol. Microbiol. 2014, 94, 1361–1374. [Google Scholar] [CrossRef] [PubMed] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Genera in Which Frequency of Identification Was Increased | Genera of Opportunistic Bacteria in Which Frequency of Identification Was Decreased |
|---|---|
| Agrobacterium, Bacillus Enterococcus, Lactobacillus, Pediococcus | Campylobacter, Citrobacter, Desulfovibrio, Haemophilus, Bilophila, Paraprevotella, Prevotella, Steptococcus, Granulicatella Burkholderia, Pseudomonas, Veillonella, Propionibacterium |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ermolenko, E.; Kotyleva, M.; Kotrova, A.; Tichonov, S.; Lavrenova, N.; Voropaeva, L.; Topalova, Y.; Karaseva, A.; Azarov, D.; Ermolenko, K.; et al. Consortium of Indigenous Fecal Bacteria in the Treatment of Metabolic Syndrome. Microorganisms 2022, 10, 1574. https://doi.org/10.3390/microorganisms10081574
Ermolenko E, Kotyleva M, Kotrova A, Tichonov S, Lavrenova N, Voropaeva L, Topalova Y, Karaseva A, Azarov D, Ermolenko K, et al. Consortium of Indigenous Fecal Bacteria in the Treatment of Metabolic Syndrome. Microorganisms. 2022; 10(8):1574. https://doi.org/10.3390/microorganisms10081574
Chicago/Turabian StyleErmolenko, Elena, Marina Kotyleva, Anna Kotrova, Sergey Tichonov, Nadezhda Lavrenova, Lyubov Voropaeva, Yulia Topalova, Alena Karaseva, Daniil Azarov, Konstantin Ermolenko, and et al. 2022. "Consortium of Indigenous Fecal Bacteria in the Treatment of Metabolic Syndrome" Microorganisms 10, no. 8: 1574. https://doi.org/10.3390/microorganisms10081574
APA StyleErmolenko, E., Kotyleva, M., Kotrova, A., Tichonov, S., Lavrenova, N., Voropaeva, L., Topalova, Y., Karaseva, A., Azarov, D., Ermolenko, K., Druzhininskii, D., Dmitriev, A., Shishkin, A., & Suvorov, A. (2022). Consortium of Indigenous Fecal Bacteria in the Treatment of Metabolic Syndrome. Microorganisms, 10(8), 1574. https://doi.org/10.3390/microorganisms10081574