
Tooth-Specific Streptococcus mutans Distribution and Associated Microbiome

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Ethics
2.2. Recruitment and Sampling
2.3. DNA Extraction
2.4. Quantitative Polymerase Chain Reaction (q-PCR)
2.5. Microbial Community Analysis
2.6. Power Analysis
2.7. Statistical Analysis
3. Results
3.1. Study Demographics
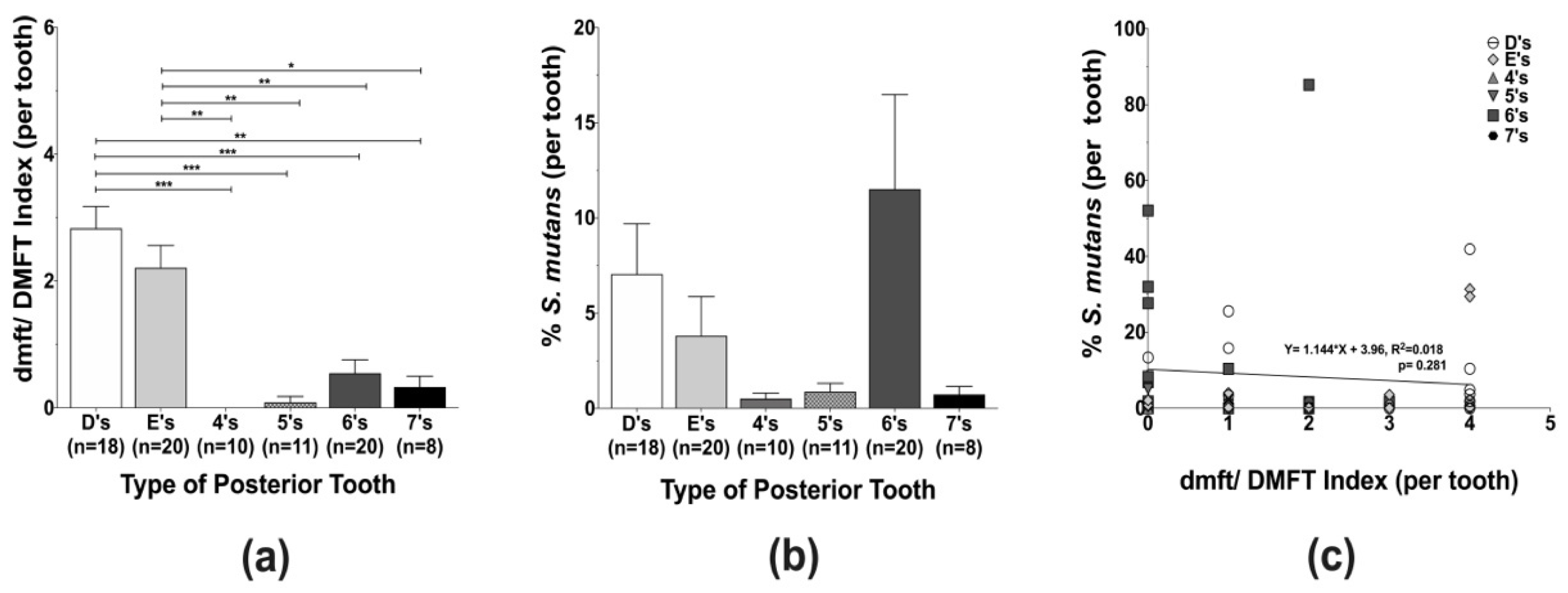
3.2. Caries Experience and Streptococcus mutans Localization in Different Types of Posterior Teeth
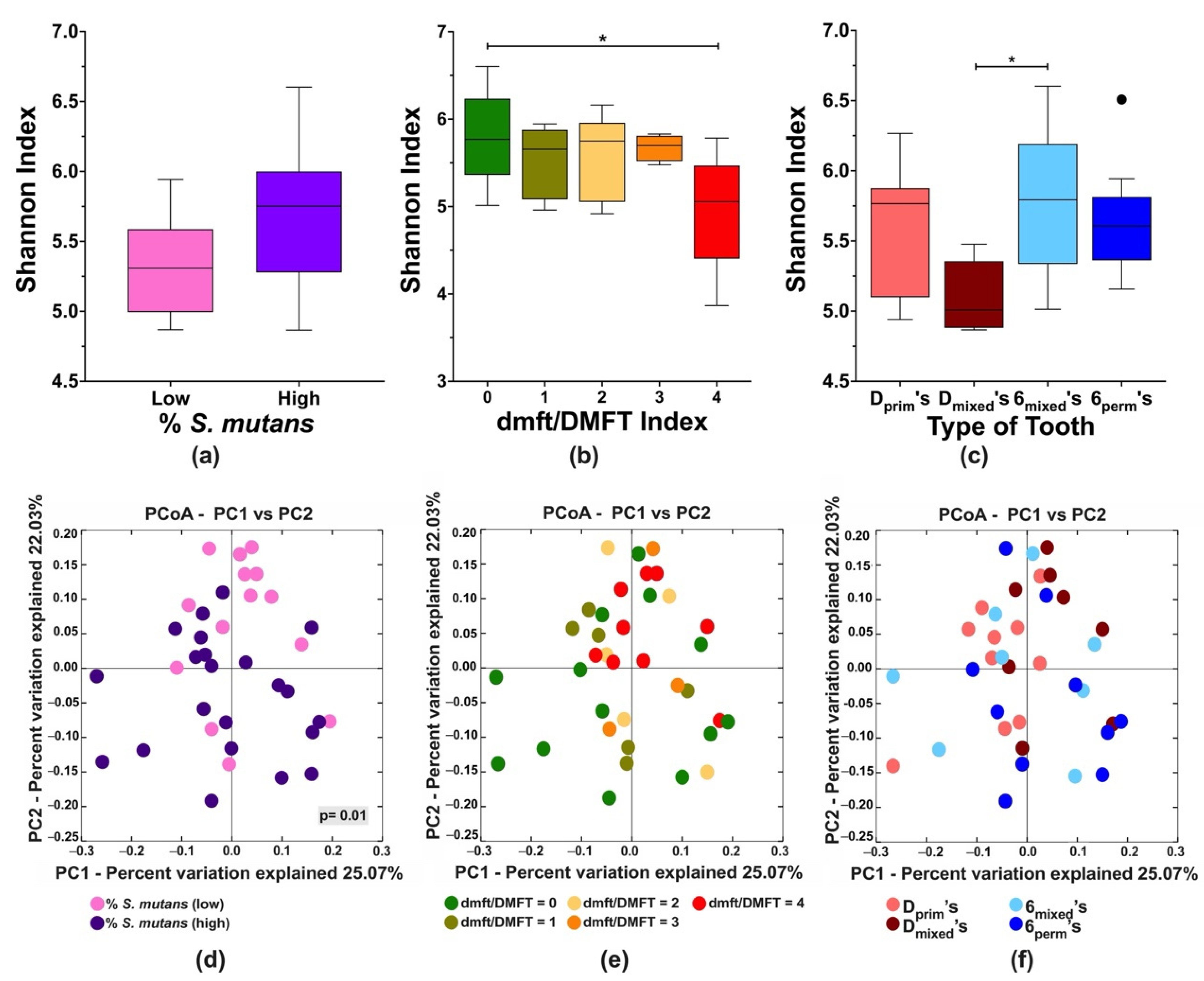
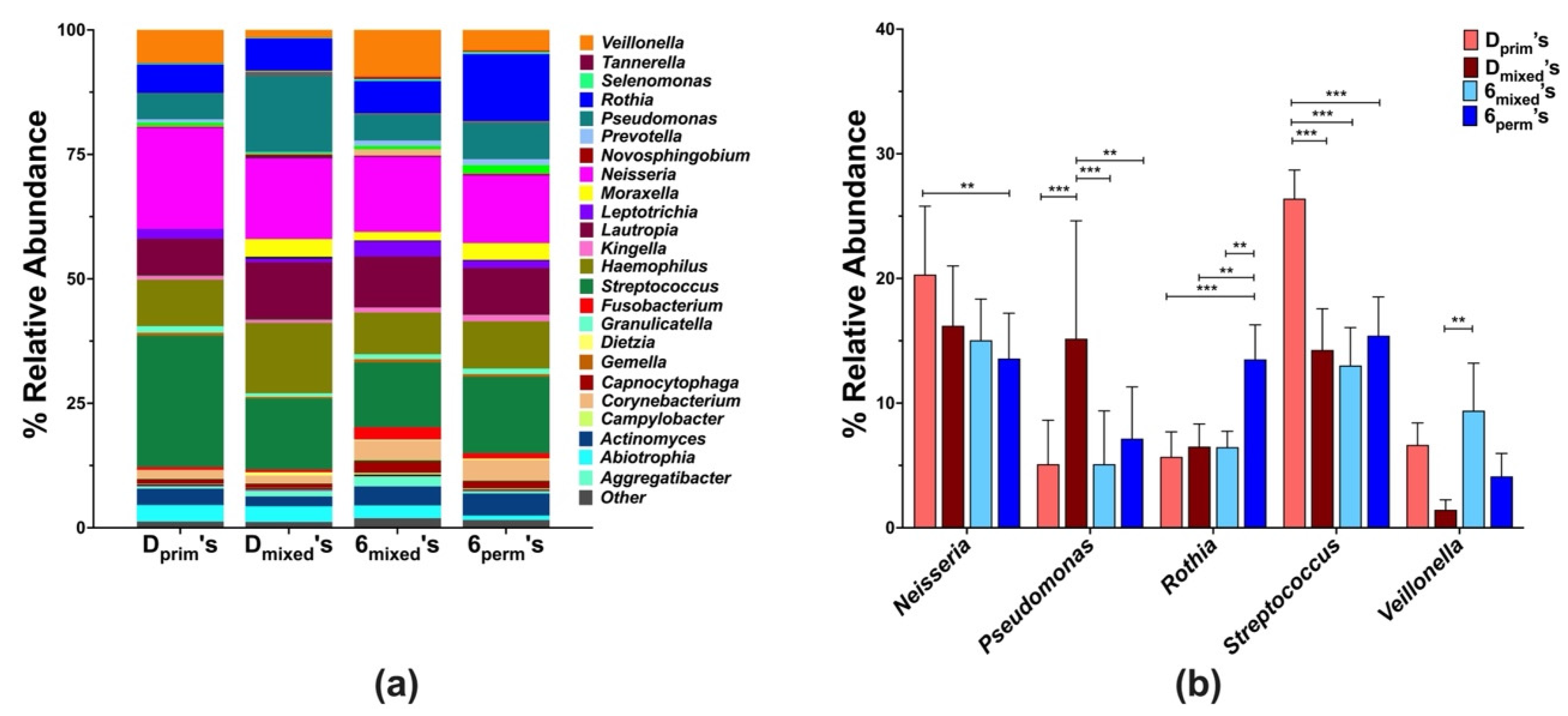
3.3. Community Profiling of D’s and 6’s
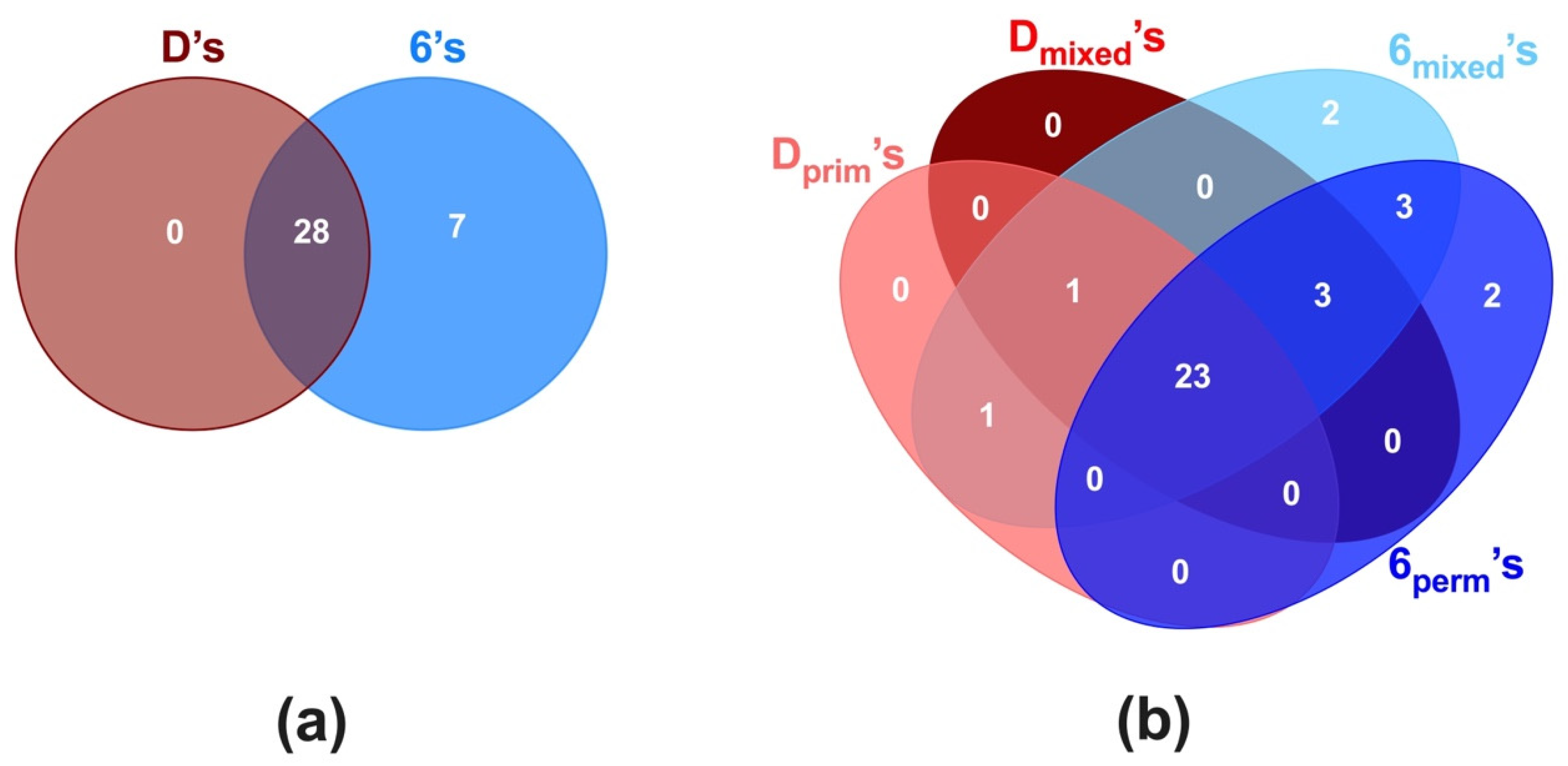
3.4. Core Microbiome of D’s and 6’s
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Dentition Stage | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Primary (2–5 y) (n = 10 Participants) | Mixed (6–10 y) (n = 10 Participants) | Permanent (11–15 y) (n = 10 Participants) | |||||||||||
| dmft/DMFT Index | |||||||||||||
| Type of Posterior Tooth | Code | d | m | f | n° Tooth | d/D | m/M | f/F | n° Tooth | D | M | F | n° Tooth |
| Primary 1st molar | D’s | 0.3 ± 0.7 | 0.0 ± 0.0 | 1.8 ± 1.7 | n = 10 | 0.4 ± 1.0 | 0.3 ± 0.7 | 2.6 ± 1.4 | n = 8 | ||||
| Primary 2nd molar | E’s | 0.4 ± 0.7 | 0.0 ± 0.0 | 1.4 ± 1.4 | n = 10 | 0.4 ± 0.9 | 0.0 ± 0.0 | 1.7 ± 1.2 | n = 10 | ||||
| Permanent 1st pre-molar | 4’s | 0.0 ± 0.0 | 0.0 ± 0.0 | 0.0 ± 0.0 | n = 1 | 0.0 ± 0.0 | 0.0 ± 0.0 | 0.0 ± 0.0 | n = 9 | ||||
| Permanent 2nd pre-molar | 5’s | 0.0 ± 0.0 | 0.0 ± 0.0 | 0.0 ± 0.0 | n = 1 | 0.0 ± 0.0 | 0.0 ± 0.0 | 0.1 ± 0.3 | n = 10 | ||||
| Permanent 1st molar | 6’s | 0.2 ± 0.6 | 0.0 ± 0.0 | 0.1 ± 0.3 | n = 10 | 0.0 ± 0.0 | 0.0 ± 0.0 | 0.8 ± 1.1 | n = 10 | ||||
| Permanent 2nd molar | 7’s | 0.0 ± 0.0 | 0.0 ± 0.0 | 0.0 ± 0.0 | n = 1 | 0.1 ± 0.3 | 0.0 ± 0.0 | 0.2 ± 0.4 | n = 7 | ||||
References
- Dye, B.A.; Thornton-Evans, G.; Li, X.; Iafolla, T.J. Dental Caries and Sealant Prevalence in Children and Adolescents in the United States, 2011–2012; NCHS Data Brief; CDC: Atlanta, GA, USA, 2015. [Google Scholar]
- Kassebaum, N.J.; Smith, A.G.C.; Bernabé, E.; Fleming, T.D.; Reynolds, A.E.; Vos, T.; Murray, C.J.L.; Marcenes, W. Global, regional, and national prevalence, incidence, and disability-adjusted life years for oral conditions for 195 countries, 1990–2015: A systematic analysis for the global burden of diseases, injuries, and risk factors. J. Dent. Res. 2017, 96, 380–387. [Google Scholar] [CrossRef] [PubMed]
- Guarnizo-Herreño, C.C.; Wehby, G.L. Children’s dental health, school performance, and psychosocial well-being. J. Pediatr. 2012, 161, 1153–1159. [Google Scholar] [CrossRef] [PubMed]
- De Soet, J.J.; Van Gemert-Schriks, M.C.M.; Laine, M.L.; Van Amerongen, W.E.; Morré, S.A.; Van Winkelhoff, A.J. Host and microbiological factors related to dental caries development. Caries Res. 2008, 42, 340–347. [Google Scholar] [CrossRef] [PubMed]
- Lynch, R.J. The primary and mixed dentition, post-eruptive enamel maturation and dental caries: A review. Int. Dent. J. 2013, 63, 3–13. [Google Scholar] [CrossRef]
- Saethre-Sundli, H.B.; Wang, N.J.; Wigen, T.I. Do enamel and dentine caries at 5 years of age predict caries development in newly erupted teeth? A prospective longitudinal study. Acta Odontol. Scand. 2020, 78, 509–514. [Google Scholar] [CrossRef]
- Zhang, Q.; Van Palenstein Helderman, W.H. Caries experience variables as indicators in caries risk assessment in 6–7-year-old Chinese children. J. Dent. 2006, 34, 676–681. [Google Scholar] [CrossRef]
- Topaloglu-Ak, A.; Eden, E. Caries in primary molars of 6–7-year-old Turkish children as risk indicators for future caries development in permanent molars. J. Dent. Sci. 2010, 5, 150–155. [Google Scholar] [CrossRef][Green Version]
- Carvalho, J.C. Caries process on occlusal surfaces: Evolving evidence and understanding. Caries Res. 2014, 48, 339–346. [Google Scholar] [CrossRef]
- Carvalho, J.C.; Ekstrand, K.R.; Thylstrup, A. Dental plaque and caries on occlusal surfaces of first permanent molars in relation to stage of eruption. J. Dent. Res. 1989, 68, 773–779. [Google Scholar] [CrossRef]
- Ekstrand, K.R.; Nielsen, L.A.; Carvalho, J.C.; Thylstrup, A. Dental plaque and caries on permanent first molar occlusal surfaces in relation to sagittal occlusion. Scand. J. Dent. Res. 1993, 101, 9–15. [Google Scholar] [CrossRef]
- Tanzer, J.; Livingston, J.; Thompson, A. The microbiology of primary dental caries in humans. J. Dent. Edu. 2001, 65, 1028–1037. [Google Scholar] [CrossRef]
- Loesche, W.J.; Rowan, J.; Straffon, L.H.; Loos, P.J. Association of Streptococcus mutants with human dental decay. Infect. Immun. 1975, 11, 1252–1260. [Google Scholar] [CrossRef] [PubMed]
- Loesche, W.J.; Straffon, L.H. Longitudinal investigation of the role of Streptococcus mutans in human fissure decay. Infect. Immun. 1979, 26, 498. [Google Scholar] [CrossRef] [PubMed]
- Köhler, B.; Bratthall, P.B.D. Streptococcus mutans in plaque and saliva and the development of caries. Scand. J. Dent. Res. 1981, 89, 19–25. [Google Scholar] [CrossRef] [PubMed]
- Damle, S.G.; Loomba, A.; Dhindsa, A.; Loomba, A.; Beniwal, V. Correlation between dental caries experience and mutans streptococci counts by microbial and molecular (polymerase chain reaction) assay using saliva as microbial risk indicator. Dent. Res. J. 2016, 13, 552–559. [Google Scholar] [CrossRef]
- Alaluusua, S.; Renkonen, O.V. Streptococcus mutans establishment and dental caries experience in children from 2 to 4 years old. Scand. J. Dent. Res. 1983, 91, 453–457. [Google Scholar] [CrossRef]
- Köhler, B.; Andréen, I.; Jonsson, B. The earlier the colonization by mutans streptococci, the higher the caries prevalence at 4 years of age. Oral Microbiol. Immunol. 1988, 3, 14–17. [Google Scholar] [CrossRef]
- Granath, L.; Cleaton-Jones, P.; Fatti, L.P.; Grossman, E.S. Prevalence of dental caries in 4- to 5-year-old children partly explained by presence of salivary mutans streptococci. J. Clin. Microbiol. 1993, 31, 66–70. [Google Scholar] [CrossRef]
- Loesche, W.J.; Eklund, S.; Earnest, R.; Burt, B. Longitudinal investigation of bacteriology of human fissure decay: Epidemiological studies in molars shortly after eruption. Infect. Immun. 1984, 46, 765–772. [Google Scholar] [CrossRef]
- Carlsson, P.; Olsson, B.; Bratthall, D. The relationship between the bacterium Streptococcus mutans in the saliva and dental caries in children in Mozambique. Arch. Oral Biol. 1985, 30, 265–268. [Google Scholar] [CrossRef]
- Aas, J.A.; Griffen, A.L.; Dardis, S.R.; Lee, A.M.; Olsen, I.; Dewhirst, F.E.; Leys, E.J.; Paster, B.J. Bacteria of dental caries in primary and permanent teeth in children and young adults. J. Clin. Microbiol. 2008, 46, 1407. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; He, J.; Xue, J.; Wang, Y.; Li, K.; Zhang, K.; Guo, Q.; Liu, X.; Zhou, Y.; Cheng, L.; et al. Oral cavity contains distinct niches with dynamic microbial communities. Environ. Microbiol. 2015, 17, 699–710. [Google Scholar] [CrossRef] [PubMed]
- Shi, W.; Qin, M.; Chen, F.; Xia, B. Supragingival microbial profiles of permanent and deciduous teeth in children with mixed dentition. PLoS ONE 2016, 11, e0146938. [Google Scholar] [CrossRef] [PubMed]
- Mason, M.R.; Chambers, S.; Dabdoub, S.M.; Thikkurissy, S.; Kumar, P.S. Characterizing oral microbial communities across dentition states and colonization niches. Microbiome 2018, 6, 67. [Google Scholar] [CrossRef]
- Shi, W.; Tian, J.; Xu, H.; Zhou, Q.; Qin, M. Distinctions and associations between the microbiota of saliva and supragingival plaque of permanent and deciduous teeth. PLoS ONE 2018, 13, e0200337. [Google Scholar] [CrossRef]
- Liu, S.; Wang, Y.; Zhao, L.; Sun, X.; Feng, Q. Microbiome succession with increasing age in three oral sites. Aging 2020, 12, 7874–7907. [Google Scholar] [CrossRef]
- Xu, L.; Chen, X.; Wang, Y.; Jiang, W.; Wang, S.; Ling, Z.; Chen, H. Dynamic alterations in salivary microbiota related to dental caries and age in preschool children with deciduous dentition: A 2-year follow-up study. Front. Physiol. 2018, 9, 342. [Google Scholar] [CrossRef]
- Jiang, S.; Gao, X.; Jin, L.; Lo, E.C.M. Salivary microbiome diversity in caries-free and caries-affected children. Int. J. Mol. Sci. 2016, 17, 1978. [Google Scholar] [CrossRef]
- Luo, A.H.; Yang, D.Q.; Xin, B.C.; Paster, B.J.; Qin, J. Microbial profiles in saliva from children with and without caries in mixed dentition. Oral Dis. 2012, 18, 595–601. [Google Scholar] [CrossRef]
- Gross, E.L.; Leys, E.J.; Gasparovich, S.R.; Firestone, N.D.; Schwartzbaum, J.A.; Janies, D.A.; Asnani, K.; Griffen, A.L. Bacterial 16S sequence analysis of severe caries in young permanent teeth. J. Clin. Microbiol. 2010, 48, 4121. [Google Scholar] [CrossRef]
- Crielaard, W.; Zaura, E.; Schuller, A.A.; Huse, S.M.; Montijn, R.C.; Keijser, B.J.F. Exploring the oral microbiota of children at various developmental stages of their dentition in the relation to their oral health. BMC Med. Genom. 2011, 4, 22. [Google Scholar] [CrossRef] [PubMed]
- Mannaa, A.; Carlén, A.; Campus, G.; Lingström, P. Supragingival plaque microbial analysis in reflection to caries experience. BMC Oral Health 2013, 13, 5. [Google Scholar] [CrossRef] [PubMed]
- Johansson, I.; Witkowska, E.; Kaveh, B.; Lif Holgerson, P.; Tanner, A.C.R. The microbiome in populations with a low and high prevalence of caries. J. Dent. Res. 2015, 95, 80–86. [Google Scholar] [CrossRef]
- Ribeiro, A.A.; Azcarate-Peril, M.A.; Cadenas, M.B.; Butz, N.; Paster, B.J.; Chen, T.; Bair, E.; Arnold, R.R. The oral bacterial microbiome of occlusal surfaces in children and its association with diet and caries. PLoS ONE 2017, 12, e0180621. [Google Scholar] [CrossRef] [PubMed]
- Brailsford, S.R.; Sheehy, E.C.; Gilbert, S.C.; Clark, D.T.; Kidd, E.A.M.; Zoitopoulos, L.; Adams, S.E.; Visser, J.M.; Beighton, D. The microflora of the erupting first permanent molar. Caries Res. 2005, 39, 78–84. [Google Scholar] [CrossRef] [PubMed]
- Gross, E.L.; Beall, C.J.; Kutsch, S.R.; Firestone, N.D.; Leys, E.J.; Griffen, A.L. Beyond Streptococcus mutans: Dental caries onset linked to multiple species by 16S rRNA community analysis. PLoS ONE 2012, 7, e47722. [Google Scholar] [CrossRef] [PubMed]
- Richards, V.P.; Alvarez, A.J.; Luce, A.R.; Bedenbaugh, M.; Mitchell, M.L.; Burne, R.A.; Nascimento, M.M. Microbiomes of site-specific dental plaques from children with different caries status. Infect. Immun. 2017, 85, e00106–e00117. [Google Scholar] [CrossRef]
- Inquimbert, C.; Bourgeois, D.; Bravo, M.; Viennot, S.; Tramini, P.; Llodra, J.C.; Molinari, N.; Dussart, C.; Giraudeau, N.; Carrouel, F. The oral bacterial microbiome of interdental surfaces in adolescents according to carious risk. Microorganisms 2019, 7, 319. [Google Scholar] [CrossRef]
- Peterson, S.N.; Snesrud, E.; Liu, J.; Ong, A.C.; Kilian, M.; Schork, N.J.; Bretz, W. The dental plaque microbiome in health and disease. PLoS ONE 2013, 8, e58487. [Google Scholar] [CrossRef]
- Xiao, C.; Ran, S.; Huang, Z.; Liang, J. Bacterial diversity and community structure of supragingival plaques in adults with dental health or caries revealed by 16S Pyrosequencing. Front. Microbiol. 2016, 7, 1145. [Google Scholar] [CrossRef]
- Hernández, M.; Planells, P.; Martínez, E.; Mira, A.; Carda-Diéguez, M. Microbiology of molar–incisor hypomineralization lesions. A pilot study. J. Oral Microbiol. 2020, 12, 1766166. [Google Scholar] [CrossRef] [PubMed]
- Petersen, P.E.; Baez, R.J.; World Health Organization. Oral Health Surveys: Basic Methods, 5th ed.; World Health Organization: Geneva, Switzerland, 2013.
- Dinis, M.; Agnello, M.; Cen, L.; Shokeen, B.; He, X.; Shi, W.; Wong, D.T.W.; Lux, R.; Tran, N.C. Oral Microbiome: Streptococcus mutans/Caries Concordant-Discordant Children. Front. Microbiol. 2022, 13, 782825. [Google Scholar] [CrossRef] [PubMed]
- Muyzer, G.; De Waal, E.C.; Uitterlinden, A.G. Profiling of complex microbial populations by denaturing gradient gel electrophoresis analysis of polymerase chain reaction-amplified genes coding for 16S rRNA. Appl. Environ. Microbiol. 1993, 59, 695–700. [Google Scholar] [CrossRef] [PubMed]
- Jung, W.-S.; Yang, I.L.H.; Lim, W.H.; Baek, S.-H.; Kim, T.-W.; Ahn, S.-J. Adhesion of mutans streptococci to self-ligating ceramic brackets: In vivo quantitative analysis with real-time polymerase chain reaction. Eur. J. Orthod. 2015, 37, 565–569. [Google Scholar] [CrossRef]
- Caporaso, J.G.; Kuczynski, J.; Stombaugh, J.; Bittinger, K.; Bushman, F.D.; Costello, E.K.; Fierer, N.; Peña, A.G.; Goodrich, J.K.; Gordon, J.I.; et al. QIIME allows analysis of high-throughput community sequencing data. Nat. Methods 2010, 7, 335–336. [Google Scholar] [CrossRef]
- Edgar, R.C. Search and clustering orders of magnitude faster than BLAST. Bioinformatics 2010, 26, 2460–2461. [Google Scholar] [CrossRef]
- Chen, T.; Yu, W.-H.; Izard, J.; Baranova, O.V.; Lakshmanan, A.; Dewhirst, F.E. The Human Oral Microbiome Database: A web accessible resource for investigating oral microbe taxonomic and genomic information. J. Biol. Databases Curation 2010, 2010, baq013. [Google Scholar] [CrossRef]
- Kuczynski, J.; Stombaugh, J.; Walters, W.A.; González, A.; Caporaso, J.G.; Knight, R. Using QIIME to analyze 16S rRNA gene sequences from microbial communities. Curr. Protoc. Microbiol. 2012, 1, 1E.5. [Google Scholar] [CrossRef]
- Bardou, P.; Mariette, J.; Escudié, F.; Djemiel, C.; Klopp, C. Jvenn: An interactive Venn diagram viewer. BMC Bioinform. 2014, 15, 293. [Google Scholar] [CrossRef]
- Lemos, J.A.; Palmer, S.R.; Zeng, L.; Wen, Z.T.; Kajfasz, J.K.; Freires, I.A.; Abranches, J.; Brady, L.J. The Biology of Streptococcus mutans. Microbiol. Spectrum 2019, 7. [Google Scholar] [CrossRef]
- Matee, M.I.N.; Mikx, F.H.M.; De Soet, J.S.; Maselle, S.Y.; De Graaff, J.; Van Palenstein Helderman, W.H. Mutans streptococci in caries-active and caries-free infants in Tanzania. Oral Microbiol. Immunol. 1993, 8, 322–324. [Google Scholar] [CrossRef]
- Matee, M.I.N.; Mikx, F.H.M.; Maselle, S.Y.M.; Van Palenstein Helderman, W.H. Mutans Streptococci and Lactobacilli in breast-fed children with rampant caries. Caries Res. 1992, 26, 183–187. [Google Scholar] [CrossRef]
- Lindquist, B.; Emilson, C.G. Distribution and prevalence of mutans streptococci in the human dentition. J. Dent. Res. 1990, 69, 1160–1166. [Google Scholar] [CrossRef] [PubMed]
- Baginska, J.; Rodakowska, E.; Milewski, R.; Kierklo, A. Dental caries in primary and permanent molars in 7–8-year-old schoolchildren evaluated with Caries Assessment Spectrum and Treatment (CAST) index. BMC Oral Health 2014, 14, 74. [Google Scholar] [CrossRef] [PubMed]
- Bhardwaj, V. Dental caries prevalence in individual tooth in primary and permanent dentition among 6–12-year-old school children in Shimla, Himachal Pradesh. Int. J. Health Allied Sci. 2014, 3, 125–128. [Google Scholar] [CrossRef]
- Sampaio-Maia, B.; Monteiro-Silva, F. Acquisition and maturation of oral microbiome throughout childhood: An update. Dent. Res. J. 2014, 11, 291–301. [Google Scholar]
- Gomez, A.; Nelson, K.E. The oral microbiome of children: Development, disease, and implications beyond oral health. Microbial. Ecol. 2017, 73, 492–503. [Google Scholar] [CrossRef]




| Dentition Stage | ||||
|---|---|---|---|---|
| Primary (2–5 y) (n = 10 Participants) | Mixed (6–10 y) (n = 10 Participants) | Permanent (11–15 y) (n = 10 Participants) | ||
| dmft/DMFT Index | ||||
| Type of Posterior Tooth | Code | dmft | dmft/DMFT | DMFT |
| Primary 1st molar | D’s | 2.1 ± 1.7 (n = 10) | 3.3 ± 1.1 (n = 8) | |
| Primary 2nd molar | E’s | 2.0 ± 1.8 (n = 10) | 2.1 ± 1.5 (n = 10) | |
| Permanent 1st pre-molar | 4’s | 0.0 ± 0.0 (n = 1) | 0.0 ± 0.0 (n = 9) | |
| Permanent 2nd pre-molar | 5’s | 0.0 ± 0.0 (n = 1) | 0.1 ± 0.3 (n = 10) | |
| Permanent 1st molar | 6’s | 0.3 ± 0.7 (n = 10) | 0.8 ± 1.1 (n = 10) | |
| Permanent 2nd molar | 7’s | 0.0 ± 0.0 (n = 1) | 0.3 ± 0.5 (n = 7) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dinis, M.; Traynor, W.; Agnello, M.; Sim, M.-S.; He, X.; Shi, W.; Lux, R.; Tran, N.C. Tooth-Specific Streptococcus mutans Distribution and Associated Microbiome. Microorganisms 2022, 10, 1129. https://doi.org/10.3390/microorganisms10061129
Dinis M, Traynor W, Agnello M, Sim M-S, He X, Shi W, Lux R, Tran NC. Tooth-Specific Streptococcus mutans Distribution and Associated Microbiome. Microorganisms. 2022; 10(6):1129. https://doi.org/10.3390/microorganisms10061129
Chicago/Turabian StyleDinis, Márcia, William Traynor, Melissa Agnello, Myung-Shin Sim, Xuesong He, Wenyuan Shi, Renate Lux, and Nini Chaichanasakul Tran. 2022. "Tooth-Specific Streptococcus mutans Distribution and Associated Microbiome" Microorganisms 10, no. 6: 1129. https://doi.org/10.3390/microorganisms10061129
APA StyleDinis, M., Traynor, W., Agnello, M., Sim, M.-S., He, X., Shi, W., Lux, R., & Tran, N. C. (2022). Tooth-Specific Streptococcus mutans Distribution and Associated Microbiome. Microorganisms, 10(6), 1129. https://doi.org/10.3390/microorganisms10061129