
Epidemiology of Toxoplasmosis in SERBIA: A Cross-Sectional Study on Blood Donors

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Data Collection
2.2. Determining the Status of T. gondii Infection
2.3. Statistical Data Analysis
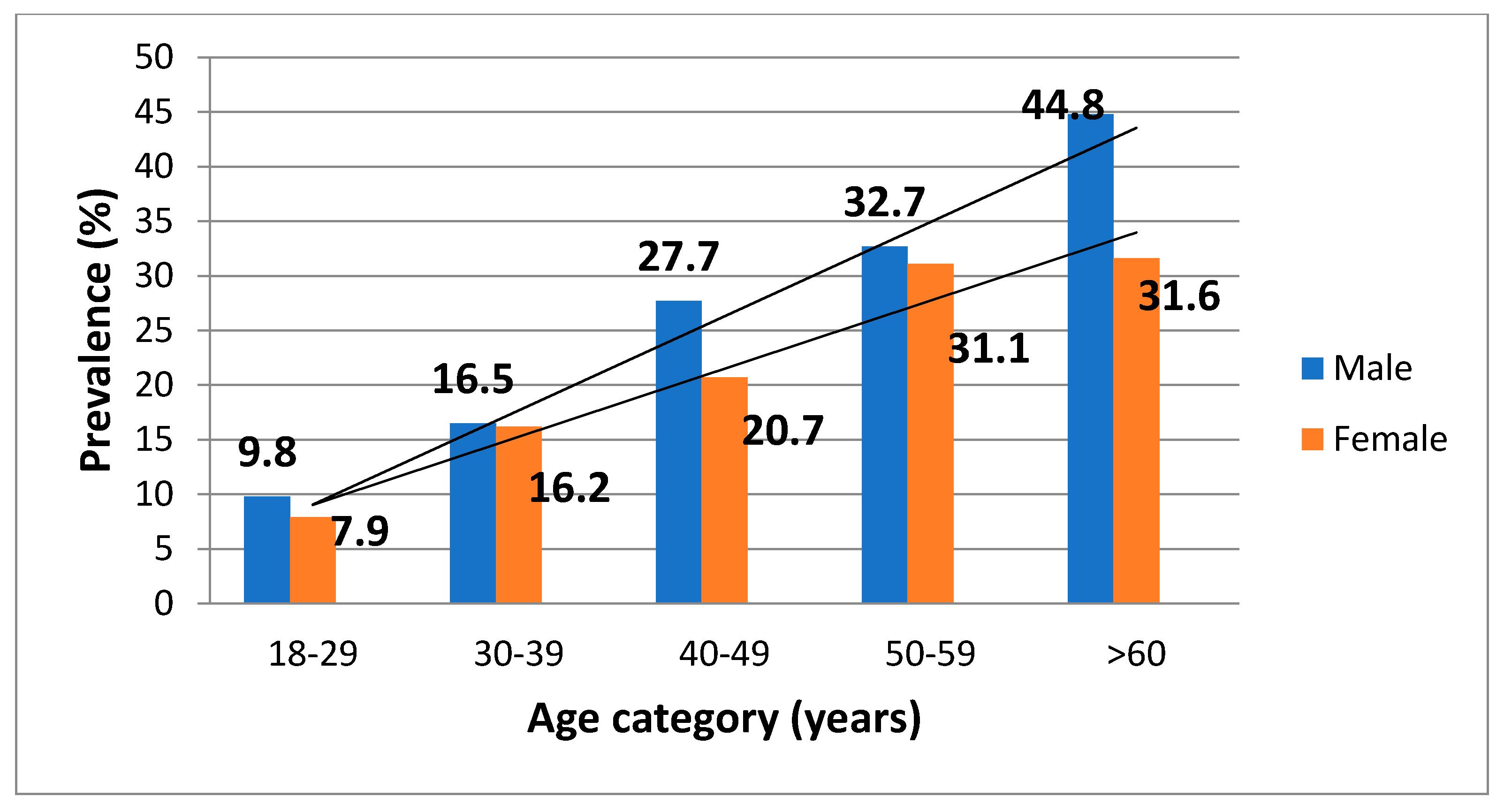
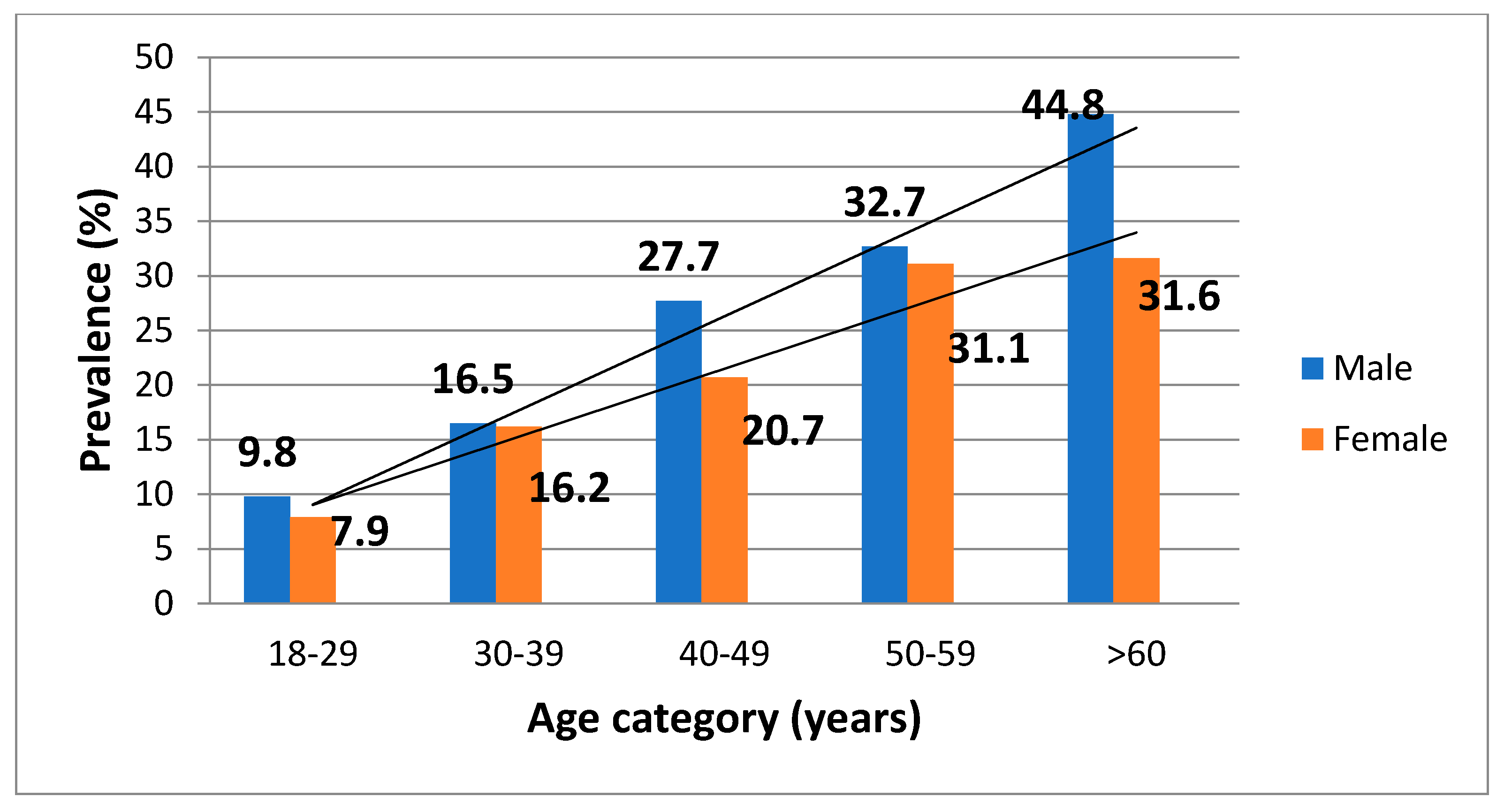
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dubey, J.P.; Beattie, C.P. Toxoplasmosis of Animals and Man, 2nd ed.; CRC Press: Boca Raton, FL, USA, 1988; 320p. [Google Scholar]
- Roth, J.A.; Siegel, S.E.; Levine, A.S.; Berard, C.W. Fatal recurrent toxoplasmosis in a patient initially infected via a leukocyte transfusion. Am. J. Clin. Pathol. 1971, 56, 601–605. [Google Scholar] [CrossRef] [PubMed]
- Siegel, S.E.; Lunde, M.N.; Gelderman, A.G.H.; Halterman, R.H.; Brown, J.A.; Levine, A.S.; Graw, R.G., Jr. Transmission of toxoplasmosis by leukocyte transfusion. Blood 1971, 37, 388–394. [Google Scholar] [CrossRef] [Green Version]
- Nelson, J.C.; Kauffmann, D.J.; Ciavarella, D.; Senisi, W.J. Acquired toxoplasmic retinochoroiditis after platelet transfusions. Ann. Ophthalmol. 1989, 21, 253–254. [Google Scholar]
- McAuley, J. Congenital toxoplasmosis. J. Pediatricic. Infect. Dis. Soc. 2014, 3, S30–S35. [Google Scholar] [CrossRef] [PubMed]
- Štajner, T.; Vujić, D.; Srbljanović, J.; Bauman, N.; Zečević, Ž.; Simić, M.; Djurković-Djaković, O. Risk of reactivated toxoplasmosis in haematopoietic stem cell transplant recipients: A prospective cohort study in a setting withholding prophylaxis. Clin. Microbiol. Infect. 2021; in press. ISSN 1198-743X. [Google Scholar] [CrossRef] [PubMed]
- Montoya, J.G.; Liesenfeld, O. Toxoplasmosis. Lancet 2004, 363, 1965–1976. [Google Scholar] [CrossRef]
- Bobić, B.; Nikolić, A.; Klun, I.; Djurković-Djaković, O. Kinetics of Toxoplasma infection in the Balkans. Wien. Klin. Wochenschr. 2011, 123 (Suppl. 1), 2–6. [Google Scholar] [CrossRef]
- Pappas, G.; Roussos, N.; Falagas, M.E. Toxoplasmosis snapshots: Global status of Toxoplasma gondii seroprevalence and implications for pregnancy and congenital toxoplasmosis. Int. J. Parasitol. 2009, 39, 1385–1394. [Google Scholar] [CrossRef]
- Desmonts, G.; Remington, J.S. Direct agglutination test for diagnosis of Toxoplasma infection: Method for increasing sensitivity and specificity. J. Clin. Microbiol. 1980, 1, 562–568. [Google Scholar] [CrossRef] [Green Version]
- Villena, I.; Ancelle, T.; Delmas, C.; Garcia, P.; Brezin, A.P.; Thulliez, P.; Wallon, M.; King, L.; Goulet, V. Toxosurv network and National Reference Centre for Toxoplasmosis. Congenital toxoplasmosis in France in 2007: First results from a national surveillance system. Eurosurveillance 2010, 15, 19600. [Google Scholar] [CrossRef] [Green Version]
- Aspöck, H.; Pollak, A. Prevention of prenatal toxoplasmosis by serological screening of pregnant women in Austria. Scand. J. Infect. Dis. 1992, 84, 32–37. [Google Scholar]
- Berghold, C.; Herzog, S.A.; Jakse, H.; Berghold, A. Prevalence and incidence of toxoplasmosis: A retrospective analysis of mother-child examinations, Styria, Austria, 1995 to 2012. Eurosurveillance 2016, 21, 30317. [Google Scholar] [CrossRef] [PubMed]
- Bobić, B.; Nikolić, A.; Djurković-Djaković, O. Identification of risk factors for infection with Toxoplasma gondii in Serbia as a basis of a programme for prevention of congenital toxoplasmosis. Srp. Arh. Celok. Lek. 2003, 131, 162–167. [Google Scholar] [CrossRef] [PubMed]
- Bobić, B.; Nikolić, A.; Klun, I.; Vujanić, M.; Djurković-Djaković, O. Undercooked meat consumption remains the major risk factor for Toxoplasma infection in Serbia. Parassitologia 2007, 49, 227–230. [Google Scholar]
- Šibalić, D.; Radović, M. Contribution la connaissance de la frequence de l’infection de Toxoplasma gondii chez l’homme dans la Serbia. GLAS CCLXXV. Acc. Serbe Sci. Arts Cl. Sci. Med. 1969, 22. [Google Scholar]
- Foroutan-Rad, M.; Majidiani, H.; Dalvand, S.; Daryani, A.; Kooti, W.; Saki, J.; Hedayati-Rad, F.; Ahmadpour, E. Toxoplasmosis in Blood Donors: A Systematic Review and Meta-Analysis. Transfus. Med. Rev. 2016, 30, 116–122. [Google Scholar] [CrossRef]
- Ðaković-Rode, O.; Židovec-Lepej, S.; Vodnica Martucci, M.; Lasica Polanda, V.; Begovac, J. Prevalence of antibodies against Toxoplasma gondii in patients infected with human immunodeficiency virus in Croatia. Croat. J. Infect. 2010, 30, 5–10. [Google Scholar]
- Bobić, B.; Milosavić, M.; Guzijan, G.; Djurković-Djaković, O. First Report on Toxoplasma gondii Infection in Bosnia and Herzegovina: Study in Blood Donors. Vector Borne Zoonotic Dis. 2016, 16, 807–809. [Google Scholar] [CrossRef]
- Alvarado-Esquivel, C.; Rascón-Careaga, A.; Hernández-Tinoco, J.; Corella-Madueño, M.A.; Sánchez-Anguiano, L.F.; Aldana-Madrid, M.L.; Velasquez-Vega, E.; Quizán-Plata, T.; Navarro-Henze, J.L.; Badell-Luzardo, J.A.; et al. Seroprevalence and Associated Risk Factors for Toxoplasma gondii Infection in Healthy Blood Donors: A Cross-Sectional Study in Sonora, Mexico. Biomed. Res. Int. 2016, 2016, 9597276. [Google Scholar] [CrossRef] [Green Version]
- Yang, S.J.; Song, R.H. Seroprevalence of Toxoplasma gondii antibodies in healthy voluntary blood donors from Shijiazhuang area. Chin. J. Schistosomiasis Control 2012, 24, 728–730. [Google Scholar]
- Sundar, P.; Mahadevan, A.; Jayshree, R.S.; Subbakrishna, D.K.; Shankar, S.K. Toxoplasma seroprevalence in healthy voluntary blood donors from urban Karnataka. Indian. J. Med. Res. 2007, 126, 50–55. [Google Scholar] [PubMed]
- Passweg, J.R.; Baldomero, H.; Bader, P.; Bonini, C.; Duarte, R.F.; Dufour, C.; Gennery, A.; Kröger, N.; Kuball, J.; Lanza, F.; et al. Use of haploidentical stem cell transplantation continues to increase: The 2015 European Society for Blood and Marrow Transplant activity survey report. Bone Marrow Transpl. 2017, 52, 811–817. [Google Scholar] [CrossRef] [PubMed]
- Vučetić, D.; Jovičić, M.; Maslovarić, I.; Bogdanović, S.; Antić, A.; Stanojković, Z.; Filimonović, G.; Ilić, V. Transfusion-transmissible infections among Serbian blood donors: Declining trends over the period 2005–2017. Blood Transfus. 2019, 17, 336–346. [Google Scholar] [CrossRef]
- Derouin, F.; Pelloux, H.; ESCMID Study Group on Clinical Parasitology. Prevention of toxoplasmosis in transplant patients. Clin. Microbiol. Infect. 2008, 14, 1089–1101. [Google Scholar] [CrossRef] [PubMed]
- Bobić, B.; Klun, I.; Vujanić, M.; Nikolić, A.; Ivović, V.; Živković, T.; Djurković-Djaković, O. Comparative and evaluation of three commercial Toxoplasma-specific IgG antibody avidity tests and significance in different clinical settings. J. Med. Microbiol. 2009, 58, 358–364. [Google Scholar] [CrossRef] [Green Version]
- American Association of Blood Banks (AABB). Toxoplasma gondii. Transfusion. 2009. Available online: https://www.aabb.org/docs/default-source/default-document-library/regulatory/eid/227s.pdf?sfvrsn=51e1708_2 (accessed on 3 January 2021).
- Bobić, B.; Jevremović, I.; Marinković, J.; Sibalić, D.; Djurković-Djaković, O. Risk factors for Toxoplasma infection in a reproductive age female population in the area of Belgrade (Yugoslavia). Eur. J. Epidemiol. 1998, 14, 605–610. [Google Scholar] [CrossRef]
- Spalding, S.M.; Amendoeira, M.R.; Klein, C.H.; Ribeiro, L.C. Serological screening and toxoplasmosis exposure factors among pregnant women in South of Brazil. Rev. Soc. Bras. Med. Trop. 2005, 38, 173–177. [Google Scholar] [CrossRef] [Green Version]
- Uneke, C.J.; Duhlinska, D.D.; Njoku, M.O.; Ngwu, B.A. Seroprevalence of acquired toxoplasmosis in HIV-infected and apparently healthy individuals in Jos, Nigeria. Parassitologia 2005, 47, 233–236. [Google Scholar]
- Alvarado-Esquivel, C.; Sifuentes-Alvarez, A.; Narro-Duarte, S.G.; Estrada-Martínez, S.; Díaz-García, J.H.; Liesenfeld, O.; Martínez-García, S.A.; Canales-Molina, A. Seroepidemiology of Toxoplasma gondii infection in pregnant women in a public hospital in northern Mexico. BMC Infect. Dis. 2006, 6, 113. [Google Scholar] [CrossRef] [Green Version]
- Frenkel, J.K.; Hassanein, K.M.; Hassanein, R.S.; Brown, E.; Thulliez, P.; Quintero-Nunez, R. Transmission of Toxoplasma gondii in Panama City, Panama: A five-year prospective cohort study of children, cats, rodents, birds, and soil. Am. J. Trop. Med. Hyg. 1995, 53, 458–468. [Google Scholar] [CrossRef]
- Weigel, R.M.; Dubey, J.P.; Dyer, D.; Siegel, A.M. Risk factors for infection with Toxoplasma gondii for residents and workers on swine farms in Illinois. Am. J. Trop. Med. Hyg. 1999, 60, 793–798. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, J.L.; Kruszon-Moran, D.; Wilson, M.; McQuillan, G.; Navin, T.; McAuley, J.B. Toxoplasma gondii infection in the United States: Seroprevalence and risk factors. Am. J. Epidemiol. 2001, 154, 357–365. [Google Scholar] [CrossRef] [PubMed]
- Cook, A.J.; Gilbert, R.E.; Buffolano, W.; Zufferey, J.; Petersen, E.; Jenum, P.A.; Foulon, W.; Semprini, A.E.; Dunn, D.T. Sources of Toxoplasma infection in pregnant women: European multicentre case-control study. European Research Network on Congenital Toxoplasmosis. BMJ 2000, 321, 142–147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dabritz, H.A.; Miller, M.A.; Atwill, E.R.; Gardner, I.A.; Leutenegger, C.M.; Melli, A.C.; Conrad, P.A. Detection of Toxoplasma gondii-like oocysts in cat feces and estimates of the environmental oocyst burden. J. Am. Vet. Med. Assoc. 2007, 231, 1676–1684. [Google Scholar] [CrossRef] [Green Version]
- Bobić, B.; Klun, I.; Nikolić, A.; Vujanić, M.; Zivković, T.; Ivović, V.; Djurković-Djaković, O. Seasonal variations in human Toxoplasma infection in Serbia. Vector Borne Zoonotic Dis. 2010, 10, 465–469. [Google Scholar] [CrossRef] [PubMed]
- Klun, I.; Djurkovic-Djakovic, O. Toxoplasma gondii in pork & pork products—Too much on our plate? Vet. Glas 2021, 75, 42–56. [Google Scholar] [CrossRef]

{kind=link}
| Demographic Characteristics | Total n (%) | T. gondii Seropositive n (%) | Univariate Logistic Regression OR (95% CI) |
|---|---|---|---|
| Age group | 1.095 (100) | 224 (100) | |
| 18–29 years | 263 (24.0) | 23 (10.3) | ref. |
| 30–39 years | 300 (27.4) | 49 (21.9) | 1.8 (1.05–3.19) |
| 40–49 years | 277 (25.3) | 67 (29.9) | 3.1 (1.79–5.24) |
| 50–59 years | 207 (18.9) | 66 (29.5) | 4.9 (2.82–8.39) |
| >60 years | 48 (4.4) | 19 (8.5) | 5.2 (2.15–12.71) |
| Gender | 1.095 (100) | 224 (100) | |
| Female | 541 (49.4) | 101 (45.1) | |
| Male | 554 (50.6) | 123 (54.9) | 1.1 (0.76–1.50) |
| Residence area | 1.095 (100) | 224 (100) | |
| Urban | 963 (87.9) | 180 (80.4) | |
| Suburban | 132 (12.1) | 44 (19.6) | 2.1 (1.31–3.41) |
| Level of education | 999 (100) | 196 (100) | |
| Elementary school | 58 (5.8) | 15 (7.7) | ref. |
| High school | 520 (52.1) | 114 (58.2) | 0.9 (0.50–1.82) |
| University | 421 (42.1) | 67 (34.2) | 0.8 (0.42–1.66) |
| Type of housing | 1.092 (100) | 224 (100) | |
| Townhouse with garden | 422 (38.6) | 99 (44.2) | 0.9 (0.66–1.31) |
| Flat in building | 670 (61.4) | 125 (55.8) |
| Lifestyle Habits | Total n (%) | T. gondii Seropositive n (%) | Univariate Logistic Regression OR (95% CI) |
|---|---|---|---|
| Contact with soil | 1.090 (100) | 222 (100) | |
| No | 777 (71.3) | 134 (60.4) | |
| Yes | 313 (28.7) | 88 (39.6) | 1.9 (1.38–2.56) |
| Contact with cat | 1.095 (100) | 224 (100) | |
| No Yes | 790 (72.1) 305 (27.9) | 152 (67.9) 72 (32.1) | 1.3 (0.94–1.78) |
| Consumption of raw/undercooked meat | 1.093 (100) | 224 (100) | |
| No | 423 (38.7) | 78 (34.8) | |
| Yes | 670 (61.3) | 146 (65.2) | 1.2 (0.91–1.67) |
| Variable | Multivariate Logistic Regression OR (95% CI) |
|---|---|
| Age group | |
| 18–29 years | ref. |
| 30–39 years | 1.9 (1.13–3.28) |
| 40–49 years | 3.2 (1.91–5.35) |
| 50–59 years | 4.6 (2.71–7.89) |
| >60 years | 6.8 (3.27–14.24) |
| Residence area | |
| Urban | |
| Suburban | 2.2 (1.43–3.34) |
| Contact with soil | |
| No | |
| Yes | 1.4 (1.01–1.94) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stopić, M.; Štajner, T.; Marković-Denić, L.; Nikolić, V.; Djilas, I.; Srzentić, S.J.; Djurković-Djaković, O.; Bobić, B. Epidemiology of Toxoplasmosis in SERBIA: A Cross-Sectional Study on Blood Donors. Microorganisms 2022, 10, 492. https://doi.org/10.3390/microorganisms10030492
Stopić M, Štajner T, Marković-Denić L, Nikolić V, Djilas I, Srzentić SJ, Djurković-Djaković O, Bobić B. Epidemiology of Toxoplasmosis in SERBIA: A Cross-Sectional Study on Blood Donors. Microorganisms. 2022; 10(3):492. https://doi.org/10.3390/microorganisms10030492
Chicago/Turabian StyleStopić, Milena, Tijana Štajner, Ljiljana Marković-Denić, Vladimir Nikolić, Iva Djilas, Snežana Jovanović Srzentić, Olgica Djurković-Djaković, and Branko Bobić. 2022. "Epidemiology of Toxoplasmosis in SERBIA: A Cross-Sectional Study on Blood Donors" Microorganisms 10, no. 3: 492. https://doi.org/10.3390/microorganisms10030492
APA StyleStopić, M., Štajner, T., Marković-Denić, L., Nikolić, V., Djilas, I., Srzentić, S. J., Djurković-Djaković, O., & Bobić, B. (2022). Epidemiology of Toxoplasmosis in SERBIA: A Cross-Sectional Study on Blood Donors. Microorganisms, 10(3), 492. https://doi.org/10.3390/microorganisms10030492