
Immune Responses to SARS-CoV-2 Infection and Vaccination in Dialysis Patients and Kidney Transplant Recipients

 , , , , , ,
, , , , , ,  and add
Show full author list
and add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design, Patients, and Ethical Statement
2.2. Serological Assays for the Detection of Anti-SARS-CoV-2 Antibodies
2.3. Determination of T-Cell Response to SARS-CoV-2
2.4. Statistics
3. Results
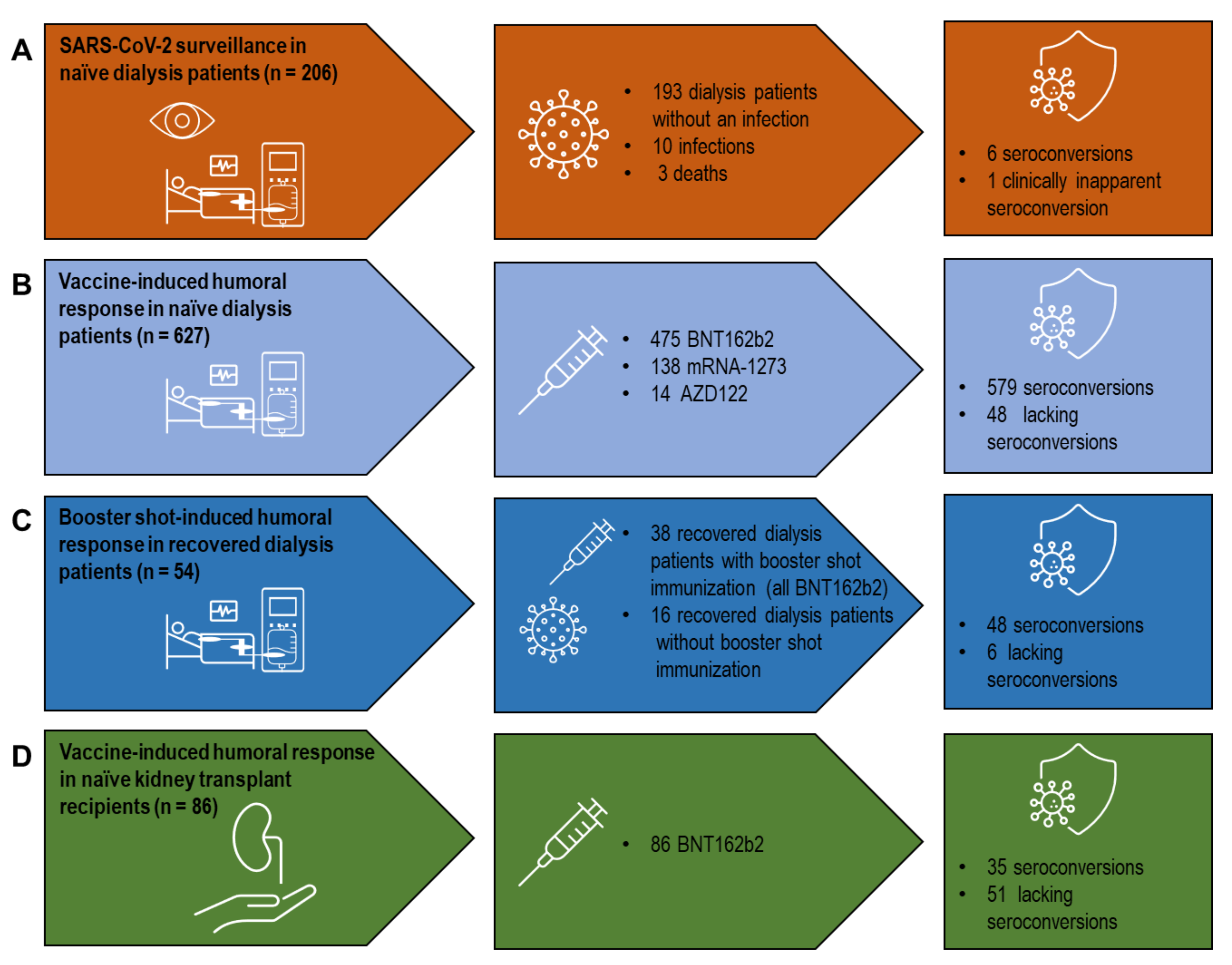
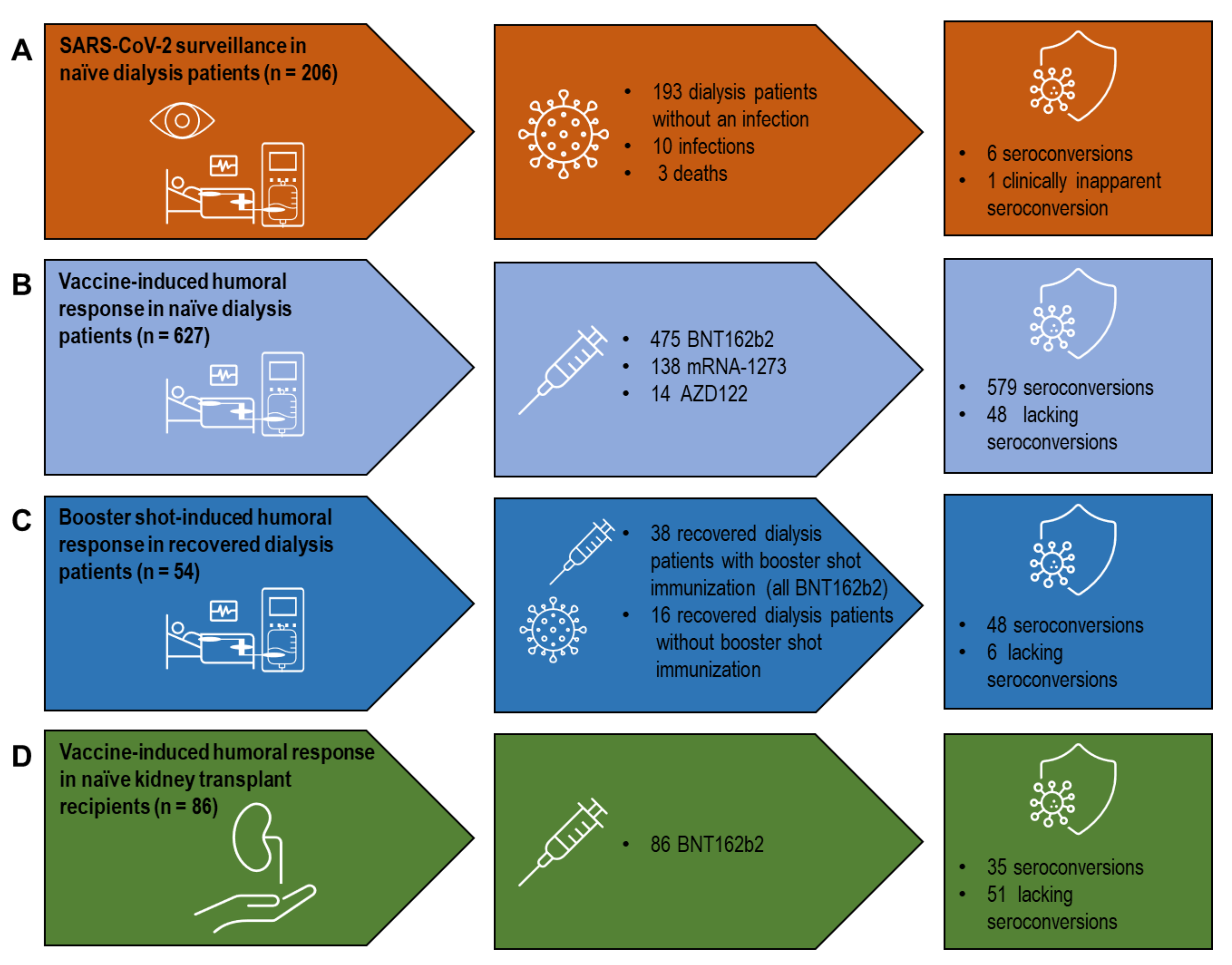
3.1. Humoral Immune Response in SARS-CoV-2-naïve Dialysis Patients after Infection
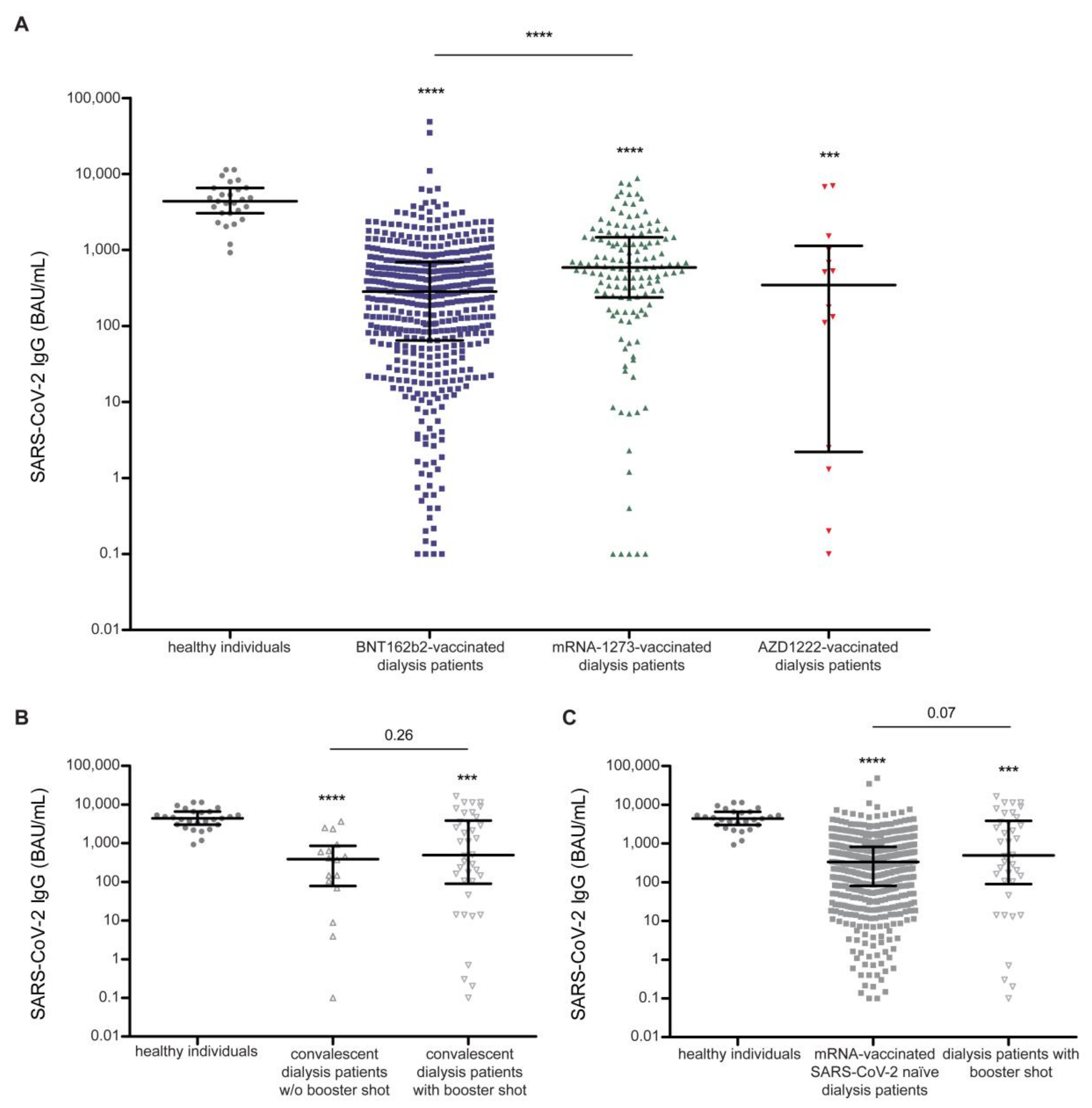
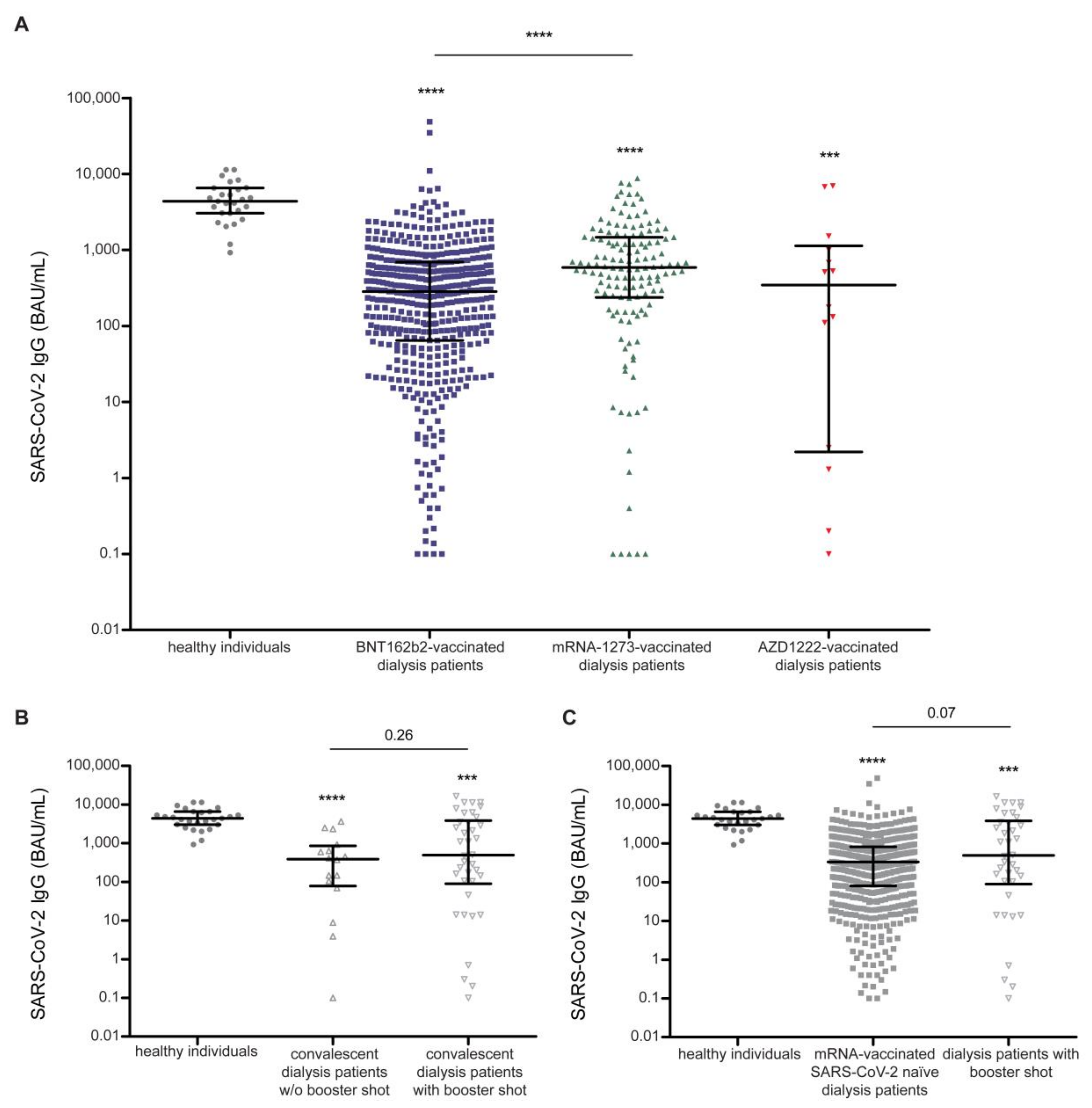
3.2. Humoral Response in SARS-CoV-2-naïve Dialysis Patients after Vaccination
3.3. Booster Shot-Induced Humoral Response in Dialysis Patients after Recovery from COVID-19
3.4. Comparisons between Standardized Anti-RBD and Anti-S1 IgG Titers
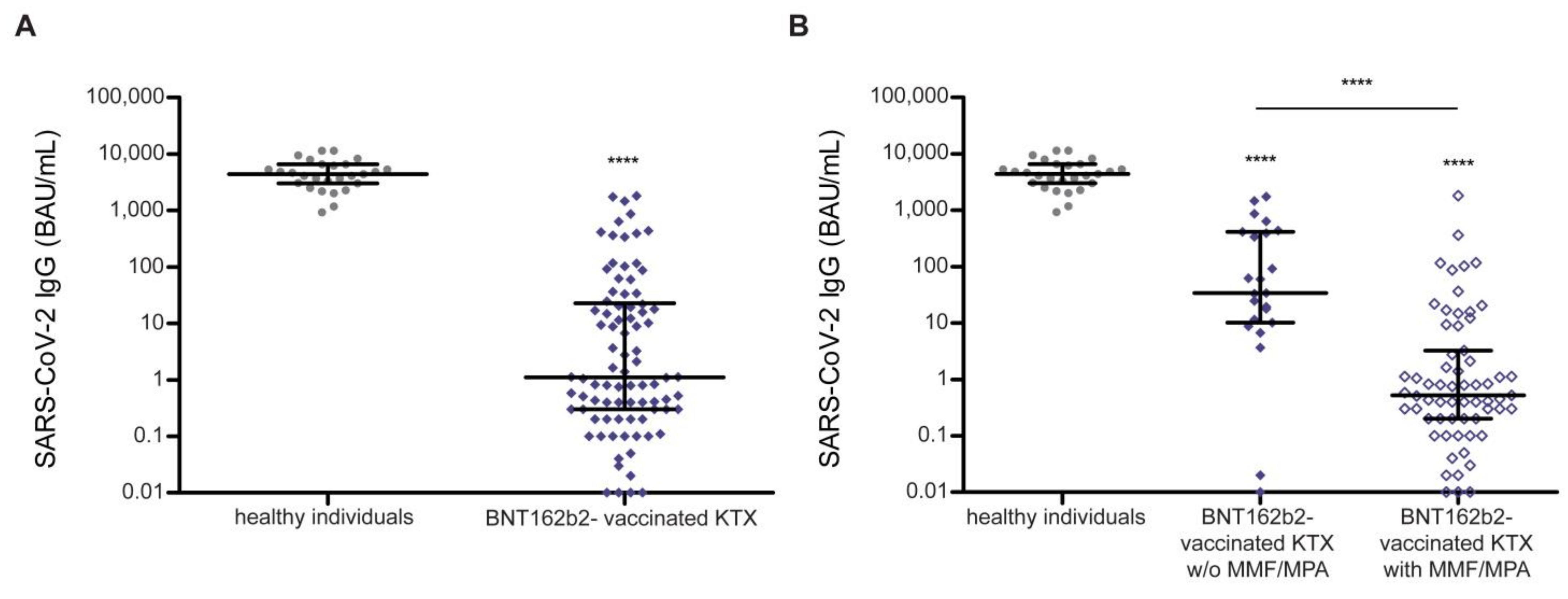
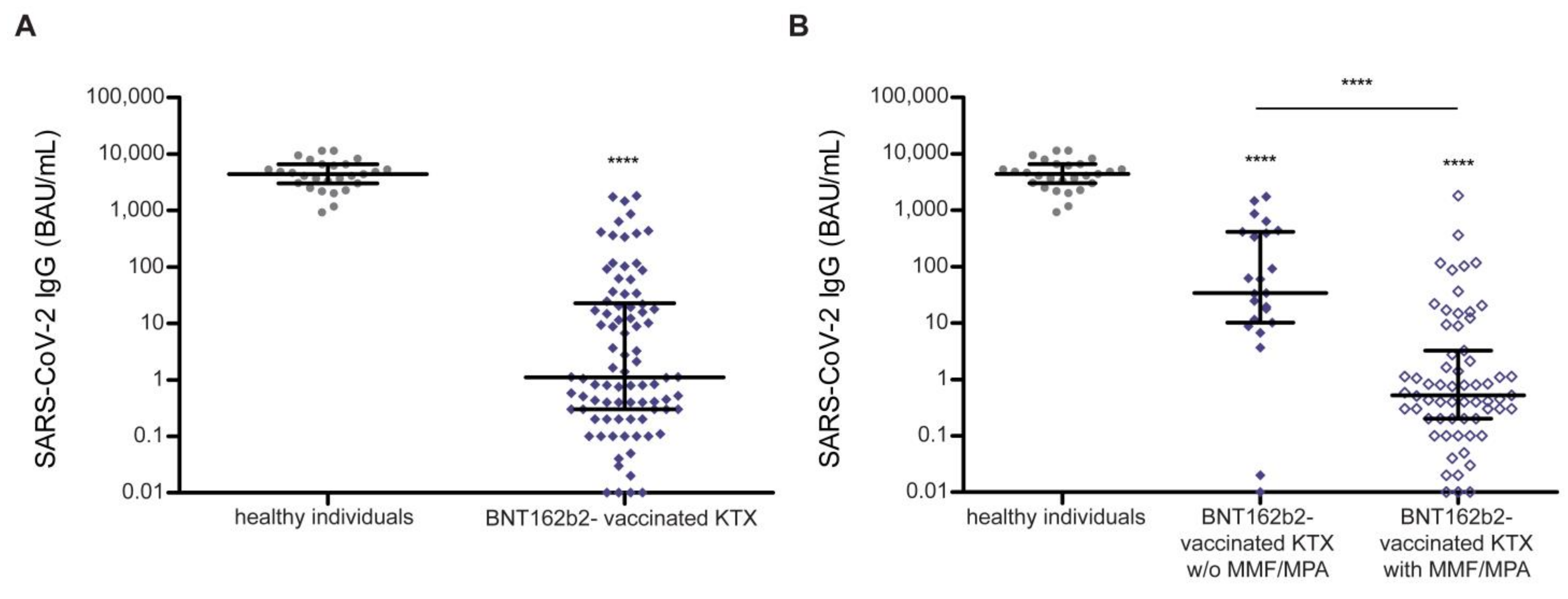
3.5. Humoral Response in SARS-CoV-2-Naïve Kidney Transplant Recipients Quantified by Anti-SARS-CoV-2 Serology after Vaccination
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Espi, M.; Charmetant, X.; Barba, T.; Koppe, L.; Pelletier, C.; Kalbacher, E.; Chalencon, E.; Mathias, V.; Ovize, A.; Cart-Tanneur, E.; et al. The ROMANOV study found impaired humoral and cellular immune responses to SARS-CoV-2 mRNA vaccine in virus-unexposed patients receiving maintenance hemodialysis. Kidney Int. 2021, 100, 928–936. [Google Scholar] [CrossRef]
- Akalin, E.; Azzi, Y.; Bartash, R.; Seethamraju, H.; Parides, M.; Hemmige, V.; Ross, M.; Forest, S.; Goldstein, Y.D.; Ajaimy, M.; et al. Covid-19 and Kidney Transplantation. N. Engl. J. Med. 2020, 382, 2475–2477. [Google Scholar] [CrossRef] [PubMed]
- Phadke, V.K.; Scanlon, N.; Jordan, S.C.; Rouphael, N.G. Immune Responses to SARS-CoV-2 in Solid Organ Transplant Recipients. Curr. Transplant. Rep. 2021, 1–13. [Google Scholar] [CrossRef]
- Caillard, S.; Chavarot, N.; Francois, H.; Matignon, M.; Greze, C.; Kamar, N.; Gatault, P.; Thaunat, O.; Legris, T.; Frimat, L.; et al. Is COVID-19 infection more severe in kidney transplant recipients? Am. J. Transplant. 2021, 21, 1295–1303. [Google Scholar] [CrossRef] [PubMed]
- Jung, C.; Flaatten, H.; Fjølner, J.; Bruno, R.R.; Wernly, B.; Artigas, A.; Bollen Pinto, B.; Schefold, J.C.; Wolff, G.; Kelm, M.; et al. The impact of frailty on survival in elderly intensive care patients with COVID-19: The COVIP study. Crit. Care 2021, 25, 149. [Google Scholar] [CrossRef] [PubMed]
- Jager, K.J.; Kramer, A.; Chesnaye, N.C.; Couchoud, C.; Sánchez-Álvarez, J.E.; Garneata, L.; Collart, F.; Hemmelder, M.H.; Ambühl, P.; Kerschbaum, J.; et al. Results from the ERA-EDTA Registry indicate a high mortality due to COVID-19 in dialysis patients and kidney transplant recipients across Europe. Kidney Int. 2020, 98, 1540–1548. [Google Scholar] [CrossRef]
- ERA-EDTA Council; ERACODA Working Group. Chronic kidney disease is a key risk factor for severe COVID-19: A call to action by the ERA-EDTA. Nephrol. Dial. Transplant. 2021, 36, 87–94. [Google Scholar] [CrossRef]
- Clarke, C.L.; Prendecki, M.; Dhutia, A.; Gan, J.; Edwards, C.; Prout, V.; Lightstone, L.; Parker, E.; Marchesin, F.; Griffith, M.; et al. Longevity of SARS-CoV-2 immune responses in hemodialysis patients and protection against reinfection. Kidney Int. 2021, 99, 1470–1477. [Google Scholar] [CrossRef]
- Giannella, M.; Pierrotti, L.C.; Helanterä, I.; Manuel, O. SARS-CoV-2 vaccination in solid-organ transplant recipients: What the clinician needs to know. Transpl. Int. 2021, 34, 1776–1788. [Google Scholar] [CrossRef]
- De Vriese, A.S.; Van Praet, J.; Reynders, M.; Heylen, L.; Viaene, L.; Caluwé, R.; Schoutteten, M.; De Bacquer, D. Longevity and correlation with disease severity of the humoral and cellular response to SARS-CoV-2 infection in haemodialysis patients. Clin. Kidney J. 2021, 14, 2446–2448. [Google Scholar] [CrossRef]
- Sakhi, H.; Dahmane, D.; Attias, P.; Kofman, T.; Bouvier, M.; Lapidus, N.; Fourati, S.; El Karoui, K. Kinetics of Anti-SARS-CoV-2 IgG Antibodies in Hemodialysis Patients Six Months after Infection. J. Am. Soc. Nephrol. 2021, 32, 1033–1036. [Google Scholar] [CrossRef]
- Simon, B.; Rubey, H.; Treipl, A.; Gromann, M.; Hemedi, B.; Zehetmayer, S.; Kirsch, B. Haemodialysis patients show a highly diminished antibody response after COVID-19 mRNA vaccination compared with healthy controls. Nephrol. Dial. Transplant. 2021, 36, 1709–1716. [Google Scholar] [CrossRef]
- Grupper, A.; Sharon, N.; Finn, T.; Cohen, R.; Israel, M.; Agbaria, A.; Rechavi, Y.; Schwartz, I.F.; Schwartz, D.; Lellouch, Y.; et al. Humoral Response to the Pfizer BNT162b2 Vaccine in Patients Undergoing Maintenance Hemodialysis. Clin. J. Am. Soc. Nephrol. 2021, 16, 1037–1042. [Google Scholar] [CrossRef] [PubMed]
- Speer, C.; Göth, D.; Benning, L.; Buylaert, M.; Schaier, M.; Grenz, J.; Nusshag, C.; Kälble, F.; Kreysing, M.; Reichel, P.; et al. Early Humoral Responses of Hemodialysis Patients after COVID-19 Vaccination with BNT162b2. Clin. J. Am. Soc. Nephrol. 2021, 16, 1073–1082. [Google Scholar] [CrossRef] [PubMed]
- Frantzen, L.; Cavaillé, G.; Thibeaut, S.; El-Haik, Y. Efficacy of the BNT162b2 mRNA COVID-19 vaccine in a haemodialysis cohort. Nephrol. Dial. Transplant. 2021, 36, 1756–1757. [Google Scholar] [CrossRef]
- Stumpf, J.; Siepmann, T.; Lindner, T.; Karger, C.; Schwöbel, J.; Anders, L.; Faulhaber-Walter, R.; Schewe, J.; Martin, H.; Schirutschke, H.; et al. Humoral and cellular immunity to SARS-CoV-2 vaccination in renal transplant versus dialysis patients: A prospective, multicenter observational study using mRNA-1273 or BNT162b2 mRNA vaccine. Lancet Reg. Health Eur. 2021, 10, 100178. [Google Scholar] [CrossRef] [PubMed]
- Rozen-Zvi, B.; Yahav, D.; Agur, T.; Zingerman, B.; Ben-Zvi, H.; Atamna, A.; Tau, N.; Mashraki, T.; Nesher, E.; Rahamimov, R. Antibody response to SARS-CoV-2 mRNA vaccine among kidney transplant recipients: A prospective cohort study. Clin. Microbiol. Infect. 2021, 27, 1173.e1171–1173.e1174. [Google Scholar] [CrossRef] [PubMed]
- Bertrand, D.; Hamzaoui, M.; Lemée, V.; Lamulle, J.; Hanoy, M.; Laurent, C.; Lebourg, L.; Etienne, I.; Lemoine, M.; Le Roy, F.; et al. Antibody and T Cell Response to SARS-CoV-2 Messenger RNA BNT162b2 Vaccine in Kidney Transplant Recipients and Hemodialysis Patients. J. Am. Soc. Nephrol. 2021, 32, 2147–2152. [Google Scholar] [CrossRef] [PubMed]
- Boyarsky, B.J.; Werbel, W.A.; Avery, R.K.; Tobian AA, R.; Massie, A.B.; Segev, D.L.; Garonzik-Wang, J.M. Antibody Response to 2-Dose SARS-CoV-2 mRNA Vaccine Series in Solid Organ Transplant Recipients. JAMA 2021, 325, 2204–2206. [Google Scholar] [CrossRef] [PubMed]
- Feng, S.; Phillips, D.J.; White, T.; Sayal, H.; Aley, P.K.; Bibi, S.; Dold, C.; Fuskova, M.; Gilbert, S.C.; Hirsch, I.; et al. Correlates of protection against symptomatic and asymptomatic SARS-CoV-2 infection. Nat. Med. 2021, 27, 2032–2040. [Google Scholar] [CrossRef]
- Martínez-Gallo, M.; Esperalba-Esquerra, J.; Pujol-Borrell, R.; Sandá, V.; Arrese-Muñoz, I.; Fernández-Naval, C.; Antón-Pagarolas, A.; Cardona, V.; Labrador-Horrillo, M.; Pumarola-Suñé, T.; et al. Commercialized kit to assess T-cell responses against SARS-CoV-2 S peptides. A pilot study in Health Care Workers. medRxiv 2021. [Google Scholar] [CrossRef]
- Jaganathan, S.; Stieber, F.; Rao, S.N.; Nikolayevskyy, V.; Manissero, D.; Allen, N.; Boyle, J.; Howard, J. Preliminary Evaluation of QuantiFERON SARS-CoV-2 and QIAreach Anti-SARS-CoV-2 Total Test in Recently Vaccinated Individuals. Infect. Dis. Ther. 2021, 10, 2765–2776. [Google Scholar] [CrossRef]
- Corbett, R.W.; Blakey, S.; Nitsch, D.; Loucaidou, M.; McLean, A.; Duncan, N.; Ashby, D.R. Epidemiology of COVID-19 in an Urban Dialysis Center. J. Am. Soc. Nephrol. 2020, 31, 1815–1823. [Google Scholar] [CrossRef] [PubMed]
- Couchoud, C.; Bayer, F.; Ayav, C.; Béchade, C.; Brunet, P.; Chantrel, F.; Frimat, L.; Galland, R.; Hourmant, M.; Laurain, E.; et al. Low incidence of SARS-CoV-2, risk factors of mortality and the course of illness in the French national cohort of dialysis patients. Kidney Int. 2020, 98, 1519–1529. [Google Scholar] [CrossRef] [PubMed]
- Yau, K.; Muller, M.P.; Lin, M.; Siddiqui, N.; Neskovic, S.; Shokar, G.; Fattouh, R.; Matukas, L.M.; Beaubien-Souligny, W.; Thomas, A.; et al. COVID-19 Outbreak in an Urban Hemodialysis Unit. Am. J. Kidney Dis. 2020, 76, 690–695.e691. [Google Scholar] [CrossRef] [PubMed]
- Tang, H.; Tian, J.B.; Dong, J.W.; Tang, X.T.; Yan, Z.Y.; Zhao, Y.Y.; Xiong, F.; Sun, X.; Song, C.X.; Xiang, C.G.; et al. Serologic Detection of SARS-CoV-2 Infections in Hemodialysis Centers: A Multicenter Retrospective Study in Wuhan, China. Am. J. Kidney Dis. 2020, 76, 490–499.e491. [Google Scholar] [CrossRef]
- Pizarro-Sánchez, M.S.; Avello, A.; Mas-Fontao, S.; Stock da Cunha, T.; Goma-Garcés, E.; Pereira, M.; Ortíz, A.; González-Parra, E. Clinical Features of Asymptomatic SARS-CoV-2 Infection in Hemodialysis Patients. Kidney Blood Press Res. 2021, 46, 126–134. [Google Scholar] [CrossRef] [PubMed]
- Voysey, M.; Clemens SA, C.; Madhi, S.A.; Weckx, L.Y.; Folegatti, P.M.; Aley, P.K.; Angus, B.; Baillie, V.L.; Barnabas, S.L.; Bhorat, Q.E.; et al. Safety and efficacy of the ChAdOx1 nCoV-19 vaccine (AZD1222) against SARS-CoV-2: An interim analysis of four randomised controlled trials in Brazil, South Africa, and the UK. Lancet 2021, 397, 99–111. [Google Scholar] [CrossRef]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- Hsu, C.M.; Weiner, D.E.; Aweh, G.N.; Manley, H.J.; Ladik, V.; Frament, J.; Miskulin, D.; Argyropoulos, C.; Abreo, K.; Chin, A.; et al. Seroresponse to SARS-CoV-2 Vaccines Among Maintenance Dialysis Patients. Am. J. Kidney Dis. 2021. [Google Scholar] [CrossRef]
- Saker, K.; Escuret, V.; Pitiot, V.; Massardier-Pilonchéry, A.; Paul, S.; Mokdad, B.; Langlois-Jacques, C.; Rabilloud, M.; Goncalves, D.; Fabien, N.; et al. Evaluation of commercial anti-SARS-CoV-2 antibody assays and comparison of standardized titers in vaccinated healthcare workers. J. Clin. Microbiol. 2021, Jcm0174621. [Google Scholar] [CrossRef] [PubMed]
- Kho, M.M.L.; Reinders, M.E.J.; Baan, C.C.; van Baarle, D.; Bemelman, F.J.; Diavatopoulos, D.A.; Gansevoort, R.T.; van der Klis FR, M.; Koopmans MP, G.; Messchendorp, A.L.; et al. The RECOVAC IR study: The immune response and safety of the mRNA-1273 COVID-19 vaccine in patients with chronic kidney disease, on dialysis or living with a kidney transplant. Nephrol. Dial. Transplant. 2021, 36, 1761–1764. [Google Scholar] [CrossRef] [PubMed]
- Sanders, J.F.; Bemelman, F.J.; Messchendorp, A.L.; Baan, C.C.; van Baarle, D.; van Binnendijk, R.; Diavatopoulos, D.A.; Frölke, S.C.; Geers, D.; GeurtsvanKessel, C.H.; et al. The RECOVAC Immune-response Study: The Immunogenicity, Tolerability, and Safety of COVID-19 Vaccination in Patients With Chronic Kidney Disease, on Dialysis, or Living With a Kidney Transplant. Transplantation 2021. [Google Scholar] [CrossRef] [PubMed]
- Benotmane, I.; Gautier-Vargas, G.; Cognard, N.; Olagne, J.; Heibel, F.; Braun-Parvez, L.; Martzloff, J.; Perrin, P.; Moulin, B.; Fafi-Kremer, S.; et al. Low immunization rates among kidney transplant recipients who received 2 doses of the mRNA-1273 SARS-CoV-2 vaccine. Kidney Int. 2021, 99, 1498–1500. [Google Scholar] [CrossRef] [PubMed]
- Cucchiari, D.; Egri, N.; Bodro, M.; Herrera, S.; Del Risco-Zevallos, J.; Casals-Urquiza, J.; Cofan, F.; Moreno, A.; Rovira, J.; Banon-Maneus, E.; et al. Cellular and humoral response after MRNA-1273 SARS-CoV-2 vaccine in kidney transplant recipients. Am. J. Transplant. 2021, 21, 2727–2739. [Google Scholar] [CrossRef]
- Amanna, I.J.; Slifka, M.K. Contributions of humoral and cellular immunity to vaccine-induced protection in humans. Virology 2011, 411, 206–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Devresse, A.; Saad Albichr, I.; Georgery, H.; Yombi, J.C.; De Greef, J.; Belkhir, L.; Mzougui, S.; Scohy, A.; Darius, T.; Buemi, A.; et al. T-cell and Antibody Response After 2 Doses of the BNT162b2 Vaccine in a Belgian Cohort of Kidney Transplant Recipients. Transplantation 2021, 105, e142–e143. [Google Scholar] [CrossRef] [PubMed]
- Benotmane, I.; Gautier, G.; Perrin, P.; Olagne, J.; Cognard, N.; Fafi-Kremer, S.; Caillard, S. Antibody Response After a Third Dose of the mRNA-1273 SARS-CoV-2 Vaccine in Kidney Transplant Recipients With Minimal Serologic Response to 2 Doses. JAMA 2021, 326, 1063–1065. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Vaccine Used in SARS-CoV-2- Naïve Dialysis Patients | Seroconversion, n (%) | Anti-SARS-CoV-2 IgG (BAU/mL), Median (IQR) |
|---|---|---|
| BNT162b2 (BioNTech/Pfizer), n = 475 | 440 (92.6) | 283.5 (628.5) |
| mRNA-1273 (Moderna), n = 138 | 129 (93.4) | 596.6 (1234.2) |
| AZD1222 (AstraZeneca/University of Oxford), n = 14 | 10 (71.4) | 345.1 (1128.2) |
| COVID-19 Recovered Dialysis Patients | ||
| No booster shot immunization, n = 16 | 14 (87.5) | 370.3 (565.5) |
| Booster shot (all BNT162b2, BioNTech/Pfizer), n = 38 | 34 (89.5) | 1103.0 (4570.0) |
| Baseline Characteristics | Seroconversion n = 579 | No Seroconversion n = 48 | p-Value |
|---|---|---|---|
| Age, yrs (± SD) | 68 (± 15) | 69 (± 16) | 0.823 |
| Sex, n (%) | |||
| Female | 218 (37.7) | 23 (47.9) | 0.160 |
| Pre-existing kidney disease, n (%) | |||
| Glomerulonephritis | 109 (18.8) | 8 (16.7) | 0.712 |
| Diabetic nephropathy | 101 (17.4) | 6 (6.3) | 0.045 |
| Hypertensive nephropathy | 143 (24.7) | 9 (18.8) | 0.355 |
| ADPKD | 41 (7.1) | 3 (6.3) | 0.828 |
| Other genetic nephropathy | 62 (10.7) | 12 (25.0) | 0.003 |
| Unknown/other | 103 (17.8) | 12 (25.0) | 0.215 |
| Haemodialysis, n (%) | 559 (96.5) | 47 (97.9) | |
| Years of Haemodialysis (IQR) | 4 (2–6) | 3 (1–6) | 0.343 |
| CAPD, n (%) | 20 (3.5) | 1 (2.1) | |
| Years of CAPD (IQR) | 2 (1–4) | 2 | 0.219 |
| Baseline Characteristics | Seroconversion n = 34 | No Seroconversion n = 52 | p-Value |
|---|---|---|---|
| Age, yrs (± SD) | 60.5 (± 15) | 63 (± 13) | 0.090 |
| Sex, n (%) | |||
| Female | 16 (47.1) | 23 (44.2) | 0.504 |
| Immunosuppression, n (%) | |||
| Tacrolimus | 26 (76.5) | 42 (80.8) | 0.632 |
| Cyclosporine A | 5 (14.7) | 9 (17.3) | 0.749 |
| Belatacept | 0 | 1 (1.9) | 0.416 |
| mTOR | 4 (11.8) | 3 (5.8) | 0.320 |
| Azathioprine | 3 (8.8) | 3 (5.8) | 0.587 |
| MMF/MPA | 15 (44.1) | 48 (92.3) | <0.001 |
| Steroid | 30 (88.2) | 50 (96.2) | 0.159 |
| Pre-existing kidney disease, n (%) | |||
| Glomerulonephritis | 9 (26.5) | 19 (36.5) | 0.330 |
| Diabetic nephropathy | 5 (14.7) | 3 (5.8) | 0.163 |
| Hypertensive nephropathy | 1 (2.9) | 1 (1.9) | 0.759 |
| ADPKD | 5 (14.7) | 4 (7.8) | 0.299 |
| Other genetic nephropathy | 6 (17.6) | 14 (26.9) | 0.319 |
| Unknown/other | 8 (23.5) | 10 (19.2) | 0.632 |
| Kidney transplantation mode, n (%) | |||
| Deceased | 16 (47.1) | 25 (48.1) | 0.926 |
| Living donor | 16 (47.1) | 24 (46.2) | 0.934 |
| Living donor AB0i | 2 (5.9) | 3 (5.8) | 0.983 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Affeldt, P.; Koehler, F.C.; Brensing, K.A.; Adam, V.; Burian, J.; Butt, L.; Gies, M.; Grundmann, F.; Hinrichs, S.; Johannis, W.; et al. Immune Responses to SARS-CoV-2 Infection and Vaccination in Dialysis Patients and Kidney Transplant Recipients. Microorganisms 2022, 10, 4. https://doi.org/10.3390/microorganisms10010004
Affeldt P, Koehler FC, Brensing KA, Adam V, Burian J, Butt L, Gies M, Grundmann F, Hinrichs S, Johannis W, et al. Immune Responses to SARS-CoV-2 Infection and Vaccination in Dialysis Patients and Kidney Transplant Recipients. Microorganisms. 2022; 10(1):4. https://doi.org/10.3390/microorganisms10010004
Chicago/Turabian StyleAffeldt, Patrick, Felix Carlo Koehler, Karl August Brensing, Vivien Adam, Julia Burian, Linus Butt, Martin Gies, Franziska Grundmann, Steffen Hinrichs, Wibke Johannis, and et al. 2022. "Immune Responses to SARS-CoV-2 Infection and Vaccination in Dialysis Patients and Kidney Transplant Recipients" Microorganisms 10, no. 1: 4. https://doi.org/10.3390/microorganisms10010004
APA StyleAffeldt, P., Koehler, F. C., Brensing, K. A., Adam, V., Burian, J., Butt, L., Gies, M., Grundmann, F., Hinrichs, S., Johannis, W., Kalisch, N., Meyer-Delpho, M., Oehm, S., Platen, E., Schöler, C., Heger, E., Steger, G., Stippel, D., Ziegelhöfer, A., ... Cristanziano, V. D. (2022). Immune Responses to SARS-CoV-2 Infection and Vaccination in Dialysis Patients and Kidney Transplant Recipients. Microorganisms, 10(1), 4. https://doi.org/10.3390/microorganisms10010004