Low-Cost, Open-Source Mechanical Ventilator with Pulmonary Monitoring for COVID-19 Patients




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
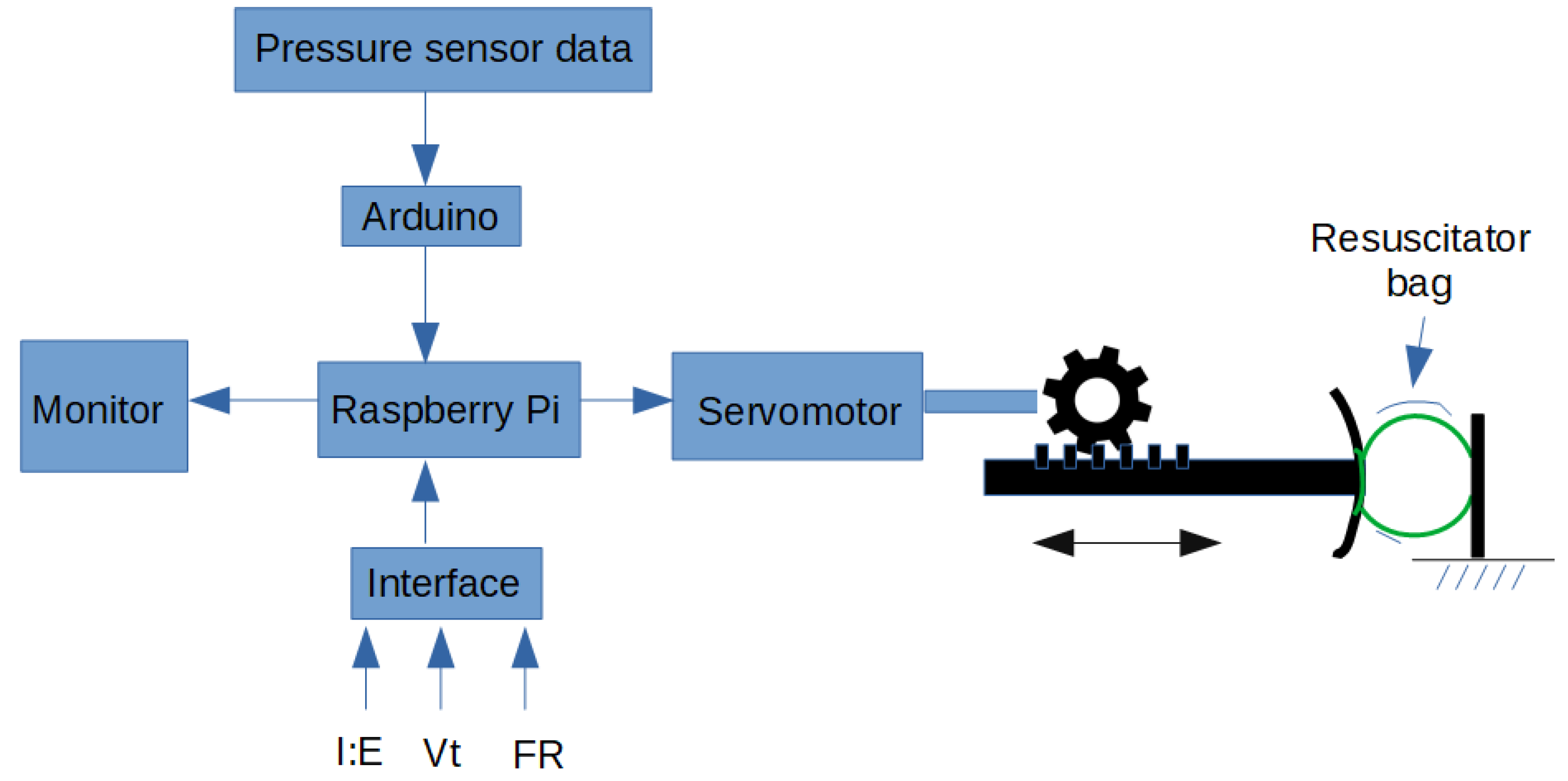
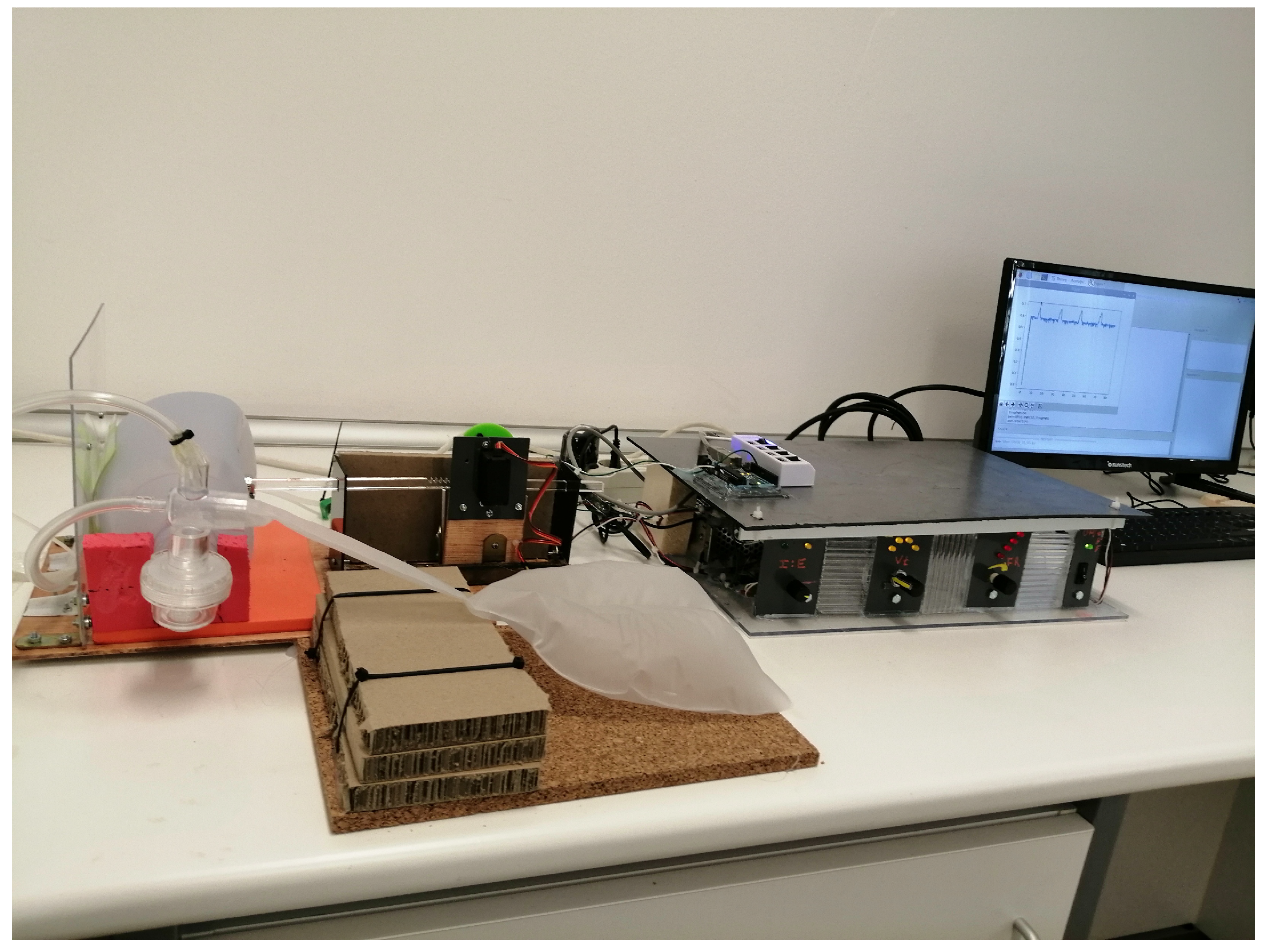
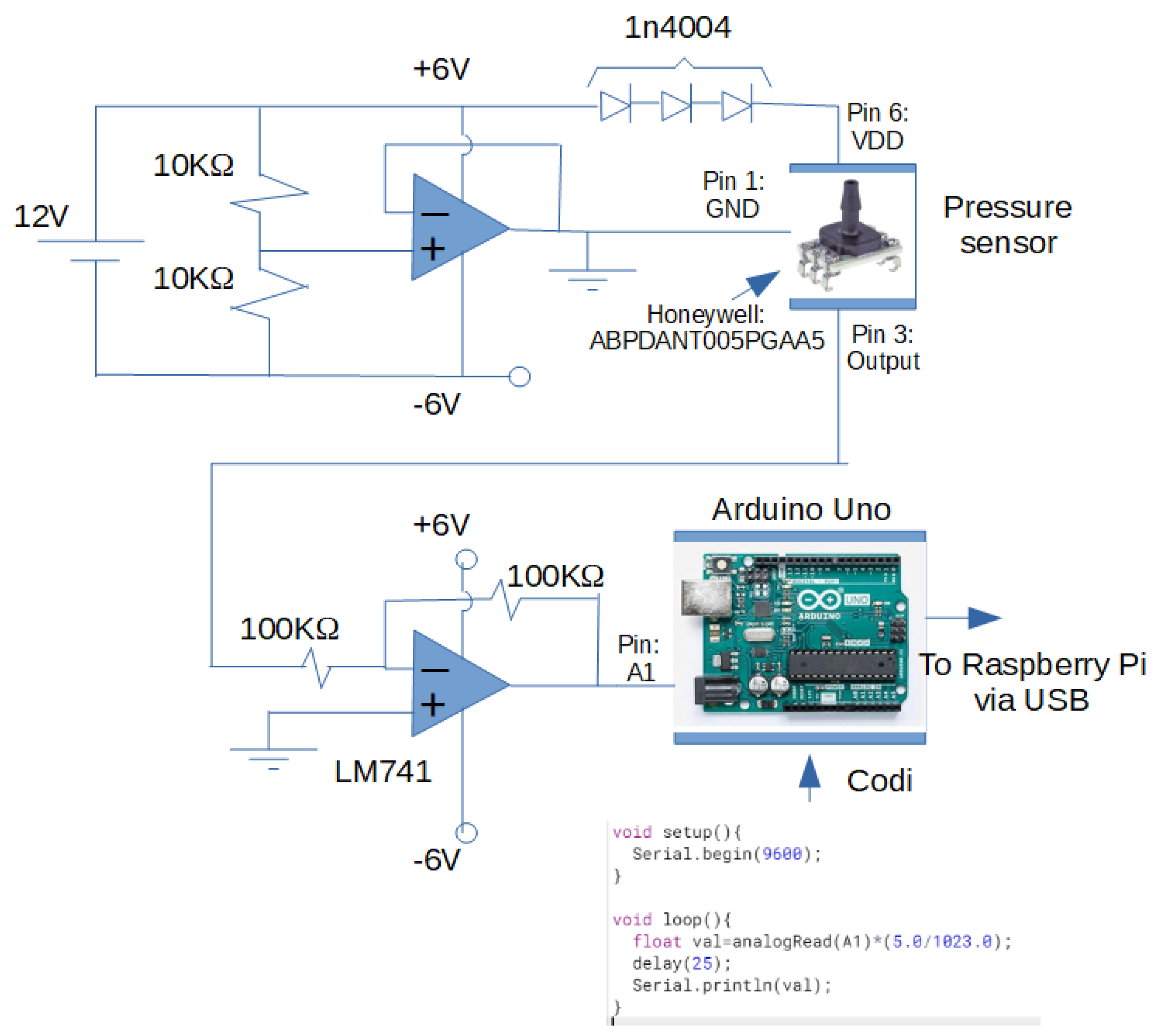
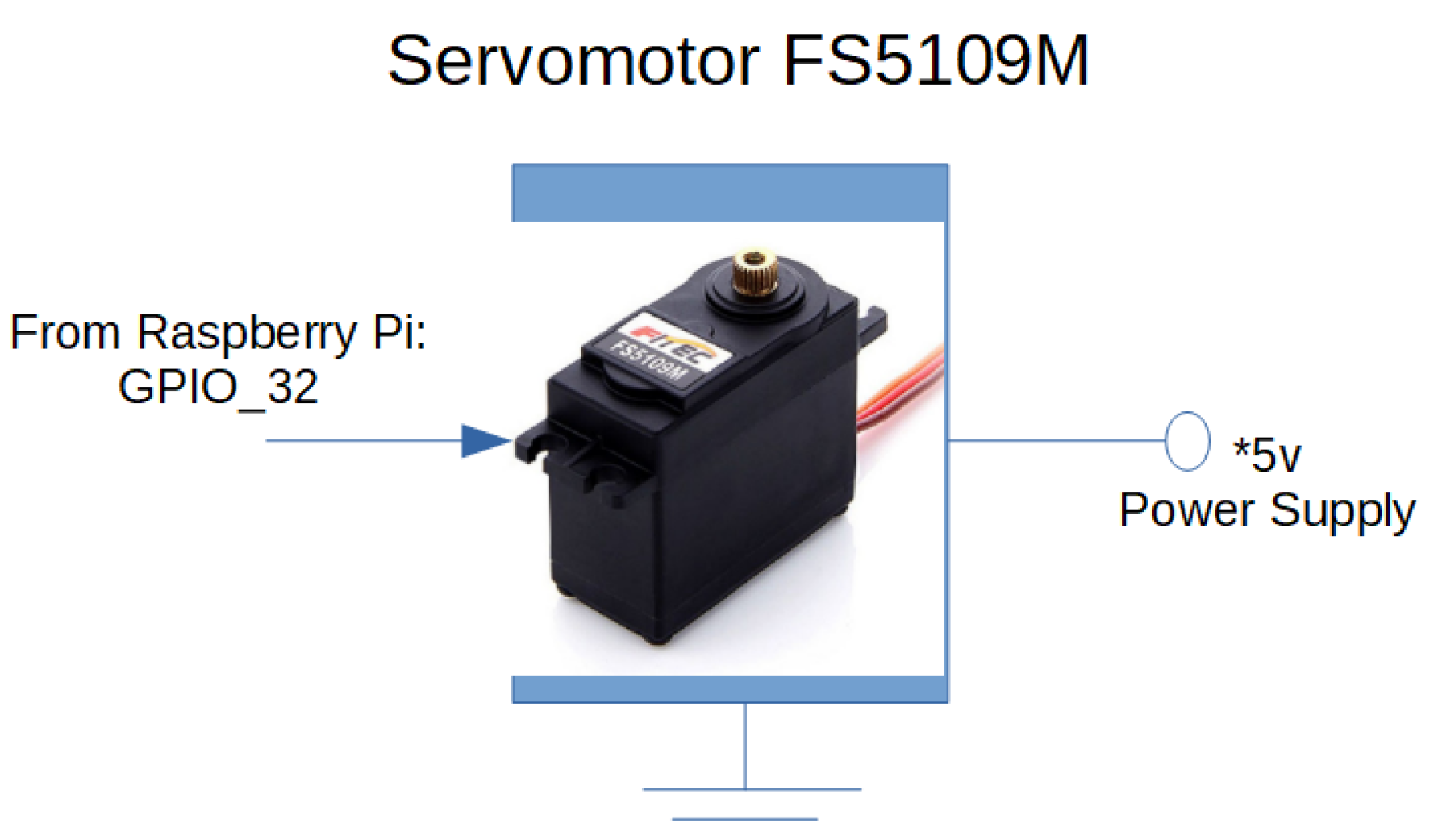
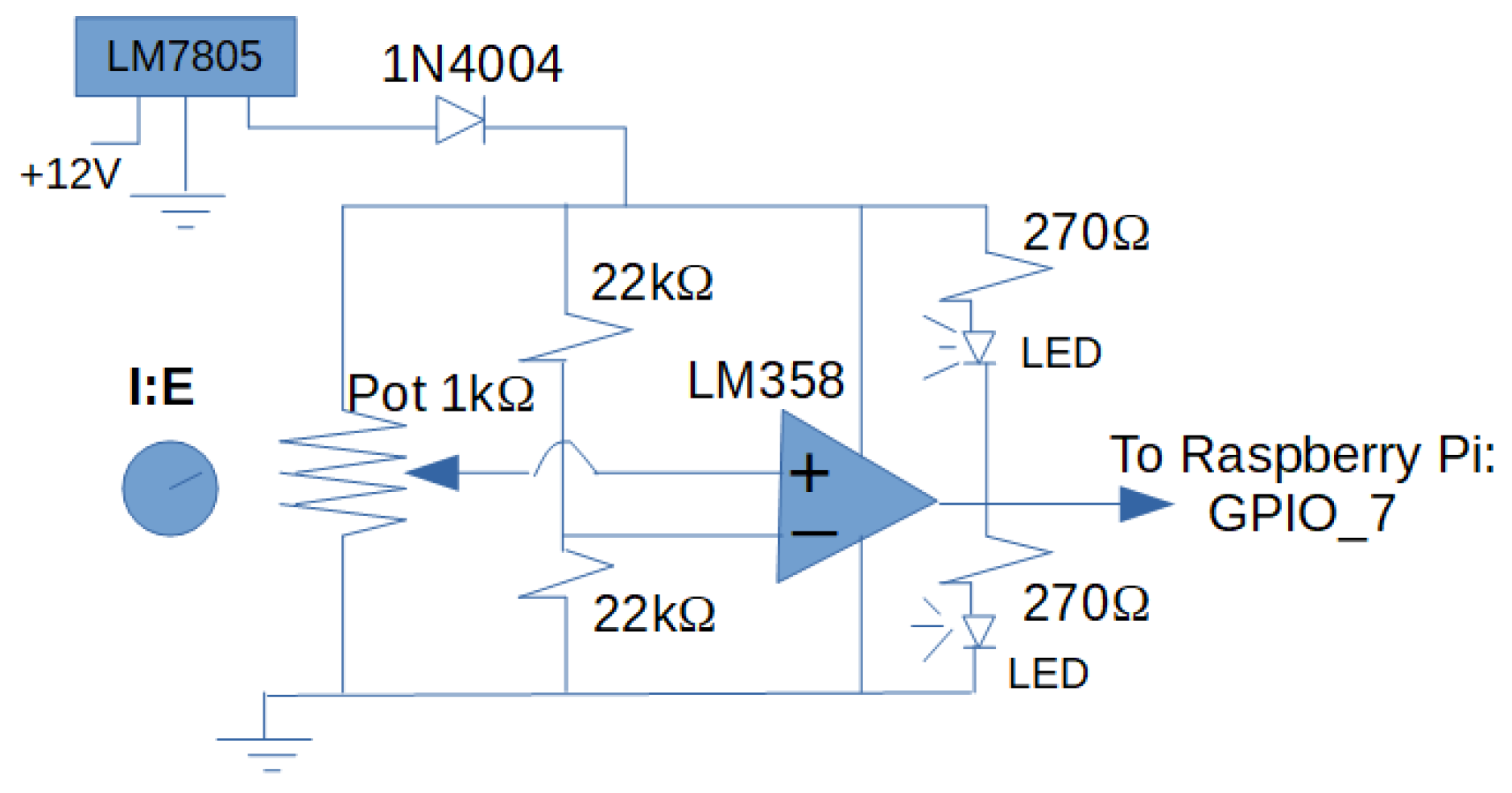
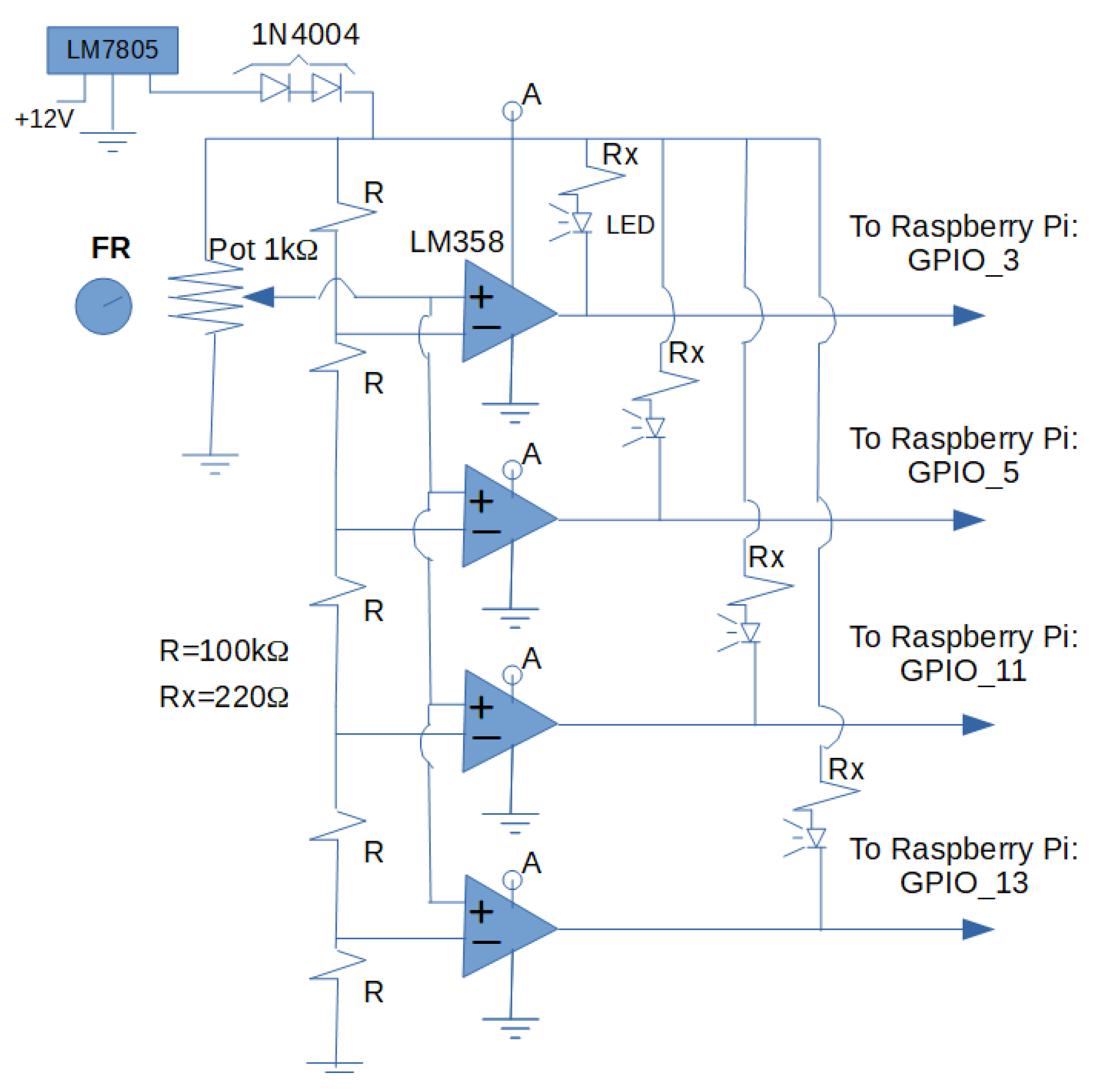
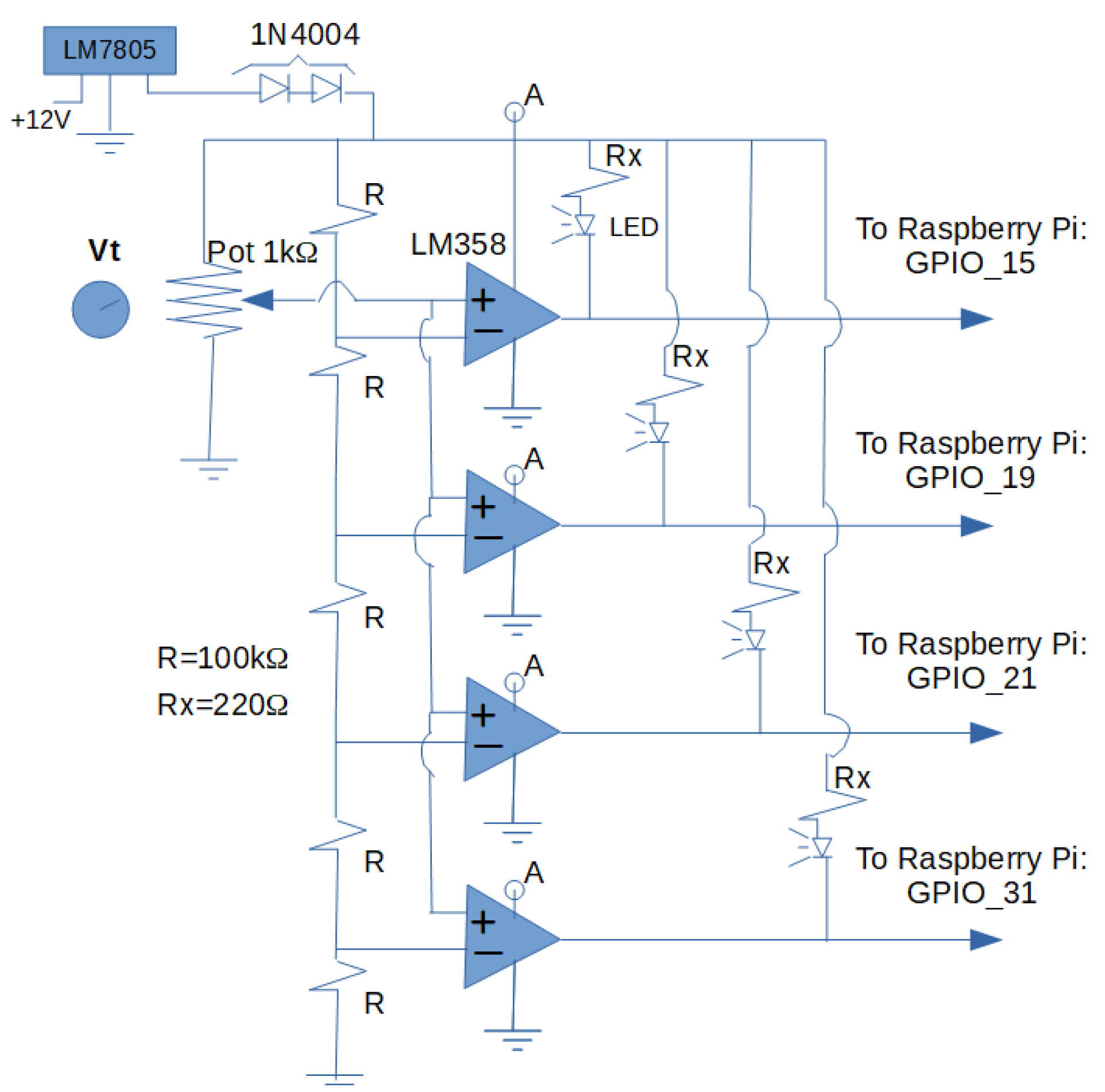
Instrumentation
3. Results and Discussion
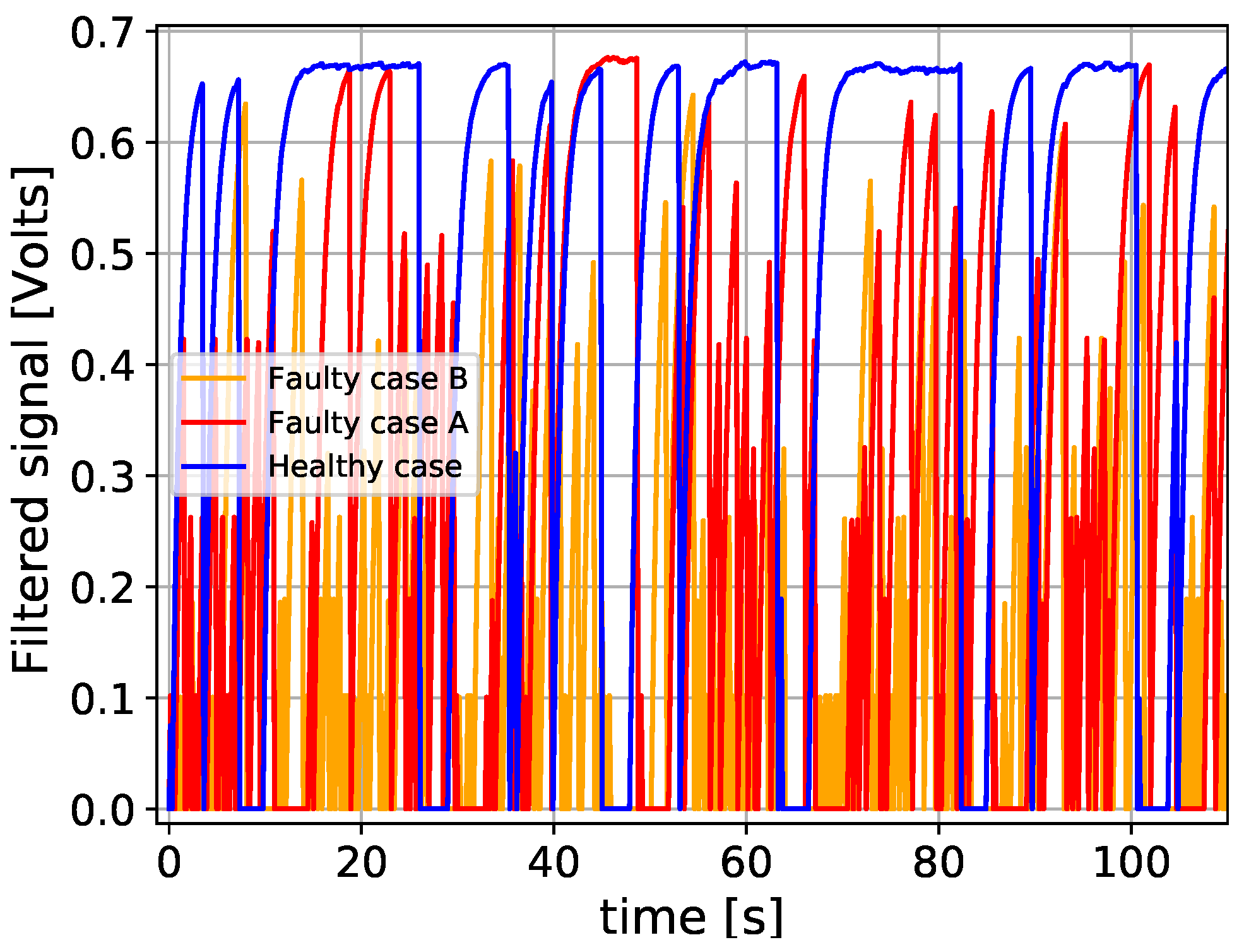
3.1. Challenges of Pulmonary Health Monitoring
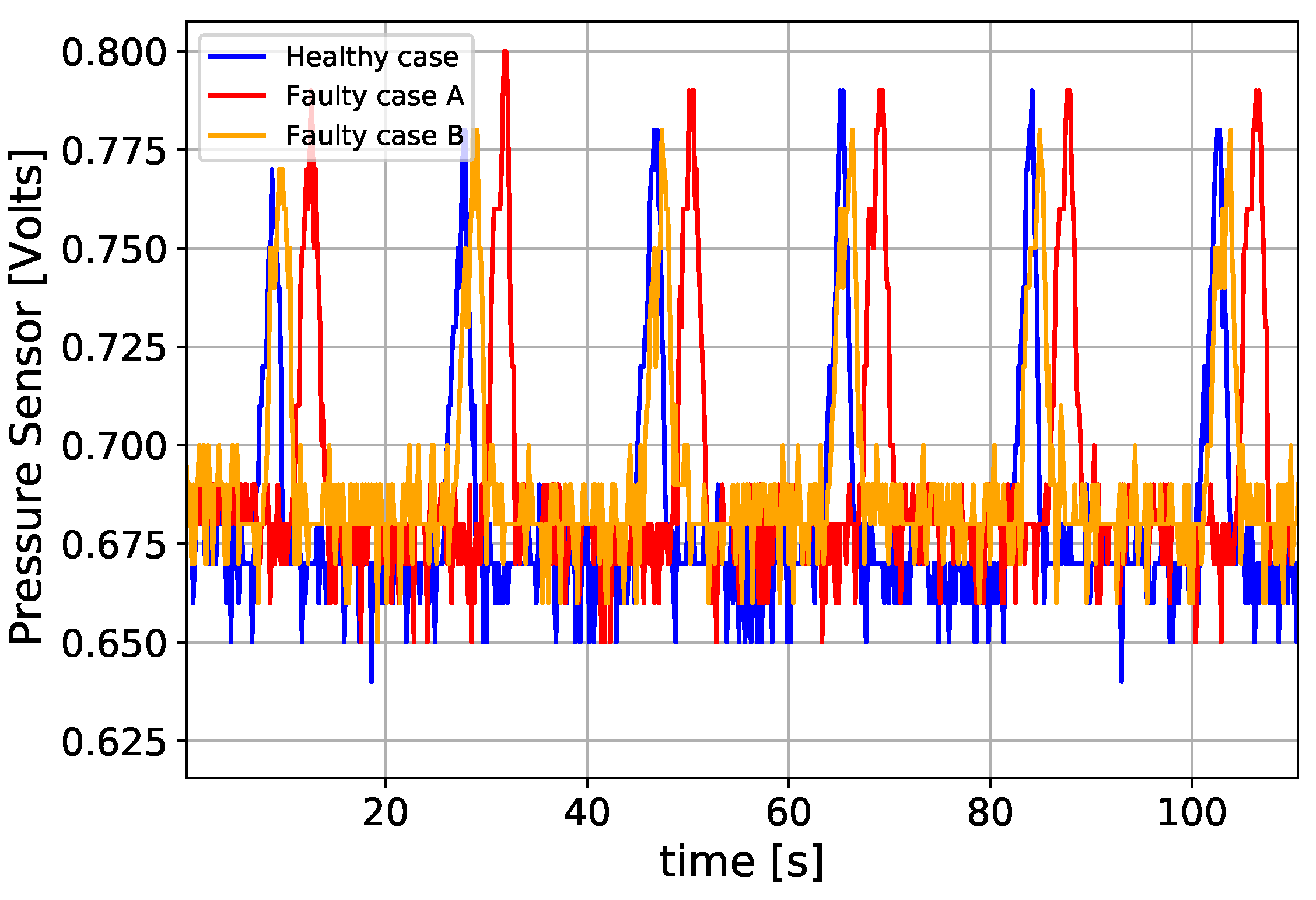
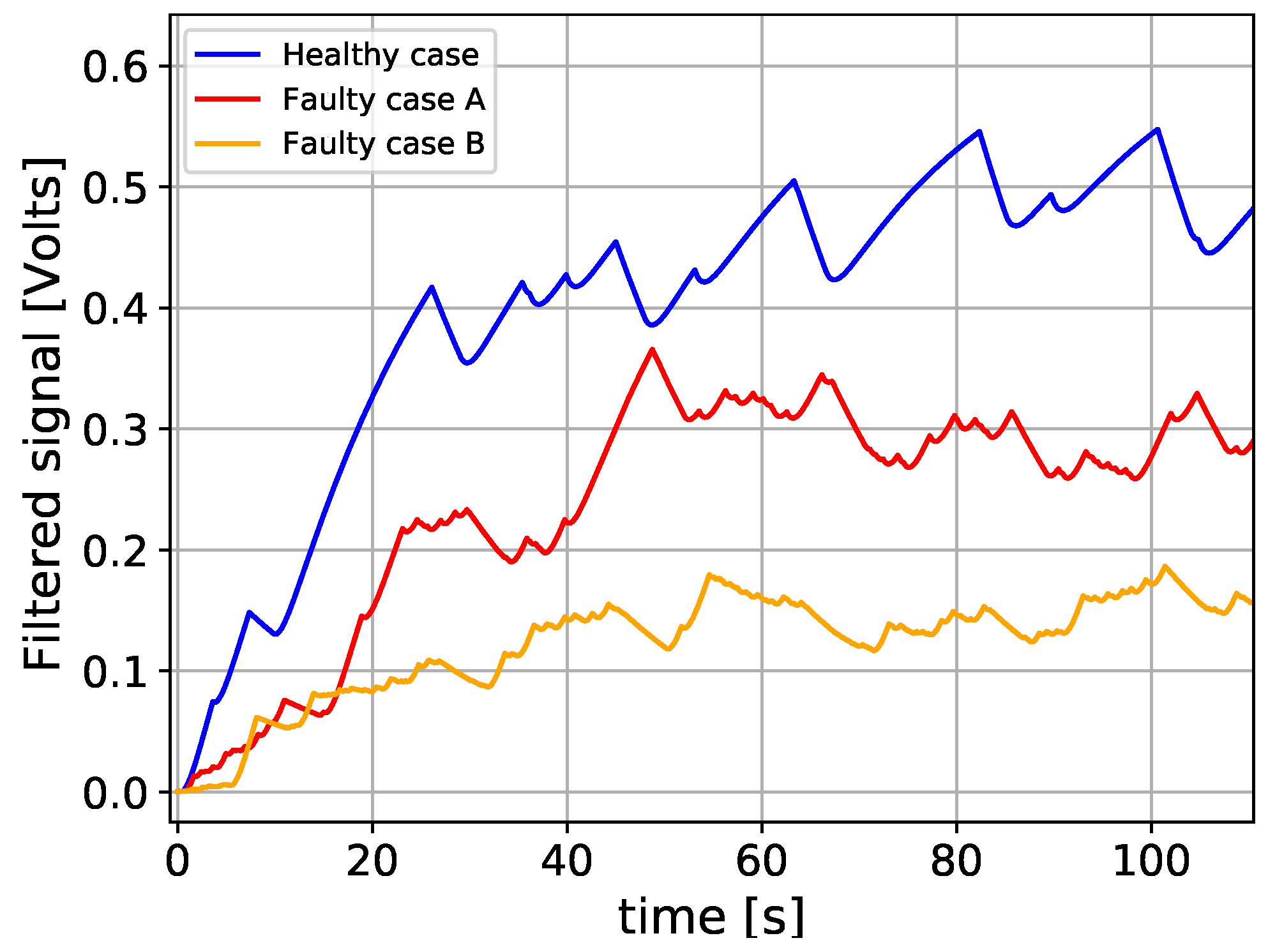
3.2. Numerical Method for the Classification of Healthy and Unhealthy Conditions
3.3. Limitations
4. Concluding Remarks
Author Contributions
Funding
Conflicts of Interest
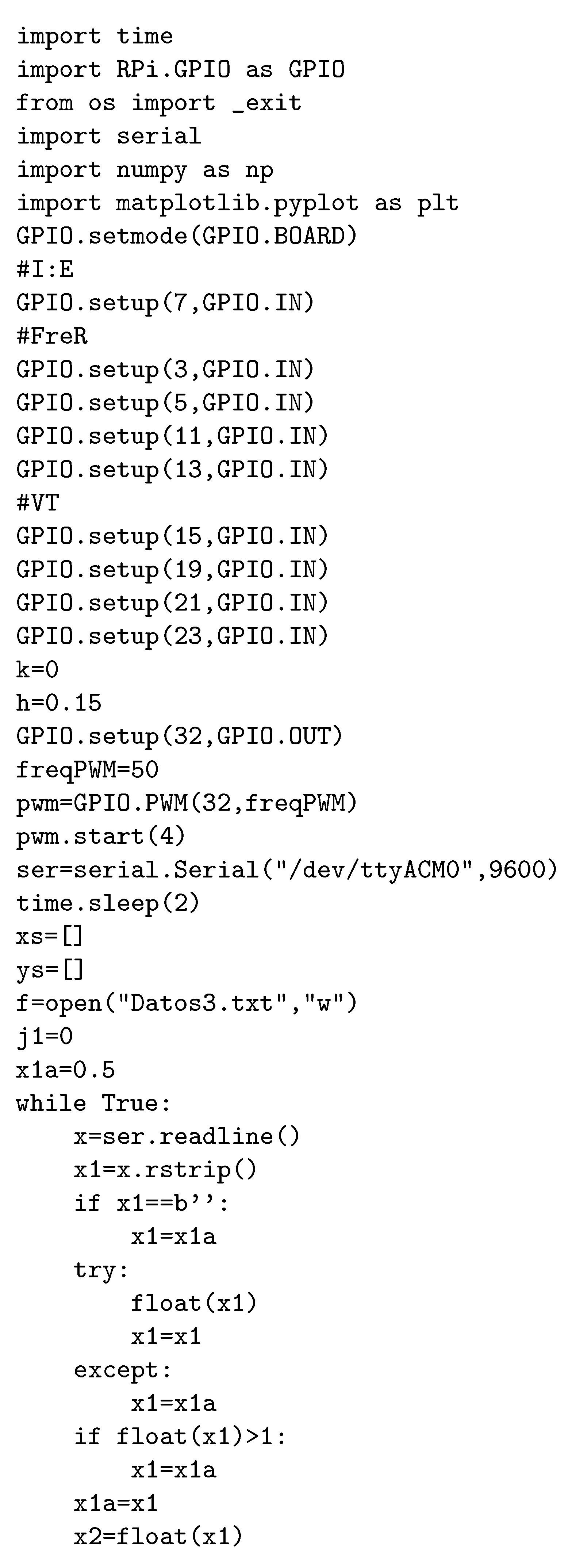
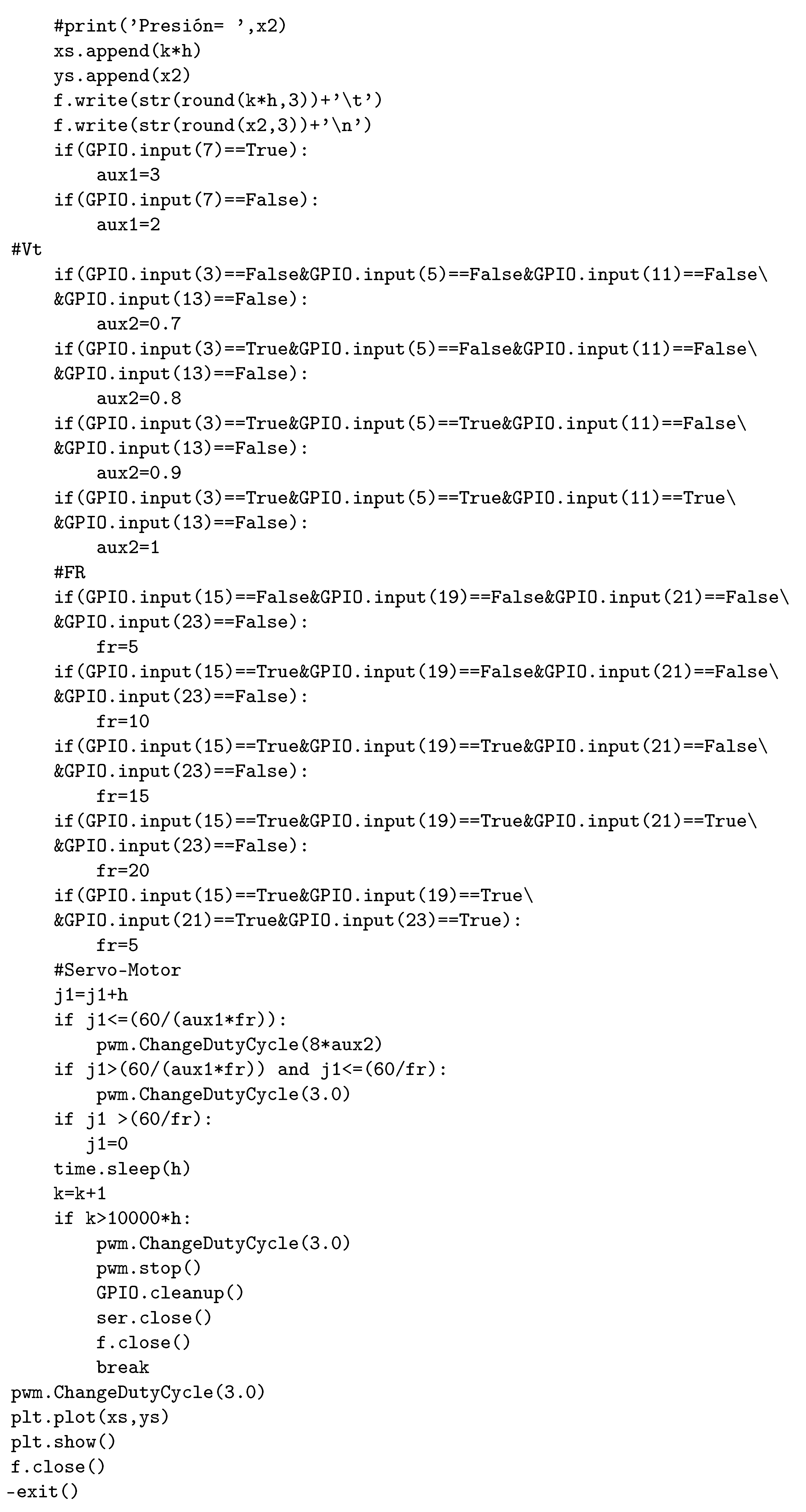
Appendix A


References
- Ranney, M.L.; Griffeth, V.; Jha, A.K. Critical Supply Shortages—The Need for Ventilators and Personal Protective Equipment during the Covid-19 Pandemic. N. Engl. J. Med. 2020, 382, e41. [Google Scholar] [CrossRef] [PubMed]
- Pons-Òdena, M.; Valls, A.; Grifols, J.; Farré, R.; Cambra Lasosa, F.J.; Rubin, B.K. COVID-19 and respiratory support devices. Paediatr. Respir. Rev. 2020, 35, 61–63. [Google Scholar] [CrossRef] [PubMed]
- Iyengar, K.; Bahl, S.; Raju, V.; Vaish, A. Challenges and solutions in meeting up the urgent requirement of ventilators for COVID-19 patients. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 499–501. [Google Scholar] [CrossRef] [PubMed]
- Ferrante, L.; Fearnside, P.M. Protect Indigenous peoples from COVID-19. Science 2020, 368, 251. [Google Scholar]
- Taylor, L. The pandemic’s new centre. New Sci. 2020, 246, 12–13. [Google Scholar] [CrossRef]
- Fitzgerald, D.A.; Maclean, J.; Rubin, B.K. COVID-19 pandemic: Impact on children, families and the future. Paediatr. Respir. Rev. 2020, 35, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Baqui, P.; Bica, I.; Marra, V.; Ercole, A.; van der Schaar, M. Ethnic and regional variations in hospital mortality from COVID-19 in Brazil: A cross-sectional observational study. Lancet Glob. Health 2020, 8, e1018–e1026. [Google Scholar] [CrossRef]
- Levin, M.A.; Shah, A.; Shah, R.; Kane, E.; Zhou, G.; Eisenkraft, J.B.; Chen, M.D. Differential Ventilation Using Flow Control Valves as a Potential Bridge to Full Ventilatory Support during the COVID-19 Crisis: From Bench to Bedside. medRxiv J. 2020, 21, 1–25. [Google Scholar] [CrossRef]
- Chase, J.G.; Chiew, Y.S.; Lambermont, B.; Morimont, P.; Shaw, G.M.; Desaive, T. Safe doubling of ventilator capacity: A last resort proposal for last resorts. Crit. Care 2020, 24, 1–4. [Google Scholar] [CrossRef]
- Herrmann, J.; Fonseca da Cruz, A.; Hawley, M.L.; Branson, R.D.; Kaczka, D.W. Shared Ventilation in the Era of COVID-19: A Theoretical Consideration of the Dangers and Potential Solutions. Respir. Care 2020, 65, 1–50. [Google Scholar] [CrossRef]
- Branson, R.D.; Blakeman, T.C.; Robinson, B.R.; Johannigman, J.A. Use of a Single Ventilator to Support 4 Patients: Laboratory Evaluation of a Limited Concept. Respir. Care 2012, 57, 399–403. [Google Scholar] [CrossRef] [PubMed]
- Huttner, B.; Catho, G.; Pano-Pardo, J.R.; Pulcini, C.; Schouten, J. COVID-19: Don’T neglect antimicrobial stewardship principles! Clin. Microbiol. Infect. 2020, 26, 808–810. [Google Scholar] [CrossRef] [PubMed]
- Zuckerberg, J.; Shaik, M.; Widmeier, K.; Kilbaugh, T.; Nelin, T.D. A lung for all: Novel mechanical ventilator for emergency and low-resource settings. Life Sci. 2020, 257, 118113. [Google Scholar] [CrossRef] [PubMed]
- Garmendia, O.; Rodríguez-Lazaro, M.A.; Otero, J.; Phan, P.; Stoyanova, A.; Dinh-Xuan, A.T.; Gozal, D.; Navajas, D.; Montserrat, J.M.; Farré, R. Low-cost, easy-to-build noninvasive pressure support ventilator for under-resourced regions: Open source hardware description, performance and feasibility testing. Eur. Respir. J. 2020, 55, 2000846. [Google Scholar] [CrossRef] [PubMed]
- Vasan, A.; Weekes, R.; Connacher, W.; Sieker, J.; Stambaugh, M.; Suresh, P.; Petersen, J. MADVent: A low-cost ventilator for patients with COVID-19. Med. Devices Sens. 2020, 3, e10106. [Google Scholar] [CrossRef] [PubMed]
- Fiorineschi, L.; Frillici, F.; Rotini, F. Challenging COVID-19 with Creativity: Supporting Design Space Exploration for Emergency Ventilators. Appl. Sci. 2020, 10, 4955. [Google Scholar] [CrossRef]
- El Majid, B.; El Hammoumi, A.; Motahhir, S.; Lebbadi, A.; El Ghzizal, A. Preliminary design of an innovative, simple, and easy-to-build portable ventilator for COVID-19 patients. Euro Mediterr. J. Environ. Integr. 2020, 23, 1–4. [Google Scholar] [CrossRef]
- Muscedere, J.; Mullen, J.; Gan, K.; Slutsky, A. Tidal ventilation at low airway pressures can augment lung injury. Am. J. Respir. Crit. Care Med. 1994, 149, 1327–1334. [Google Scholar] [CrossRef]
- Steinberg, J.M.; Schiller, H.J.; Halter, J.M.; Gatto, L.A.; Lee, H.M.; Pavone, L.A.; Nieman, G.F. Alveolar instability causes early ventilator-induced lung injury independent of neutrophils. Am. J. Respir. Crit. Care Med. 2004, 169, 57–63. [Google Scholar] [CrossRef]
- Gattinoni, L.; Quintel, M.; Marini, J.J. Volutrauma and atelectrauma: Which is worse? Crit. Care 2018, 22, 1–3. [Google Scholar] [CrossRef]
- Cressoni, M.; Chiumello, D.; Algieri, I.; Brioni, M.; Chiurazzi, C.; Colombo, A.; Colombo, A.; Crimella, F.; Guanziroli, M.; Tomic, I.; et al. Opening pressures and atelectrauma in acute respiratory distress syndrome. Intensiv. Care Med. 2017, 43, 603–611. [Google Scholar] [CrossRef] [PubMed]
- Tonetti, T.; Vasques, F.; Rapetti, F.; Maiolo, G.; Collino, F.; Romitti, F.; Camporota, L.; Cressoni, M.; Cadringher, P.; Quintel, M.; et al. Driving pressure and mechanical power: New targets for VILI prevention. Ann. Transl. Med. 2017, 5, 286. [Google Scholar] [CrossRef] [PubMed]
- Pelosi, P.; Rocco, P.R.M.; de Abreu, M.G. Close down the lungs and keep them resting to minimize ventilator-induced lung injury. Crit. Care 2018, 22, 72. [Google Scholar] [CrossRef] [PubMed]
- Gattinoni, L.; Collino, F.; Maiolo, G.; Rapetti, F.; Romitti, F.; Tonetti, T.; Vasques, F.; Quintel, M. Positive end-expiratory pressure: How to set it at the individual level. Ann. Transl. Med. 2017, 5, 288. [Google Scholar] [CrossRef]
- Bates, J.H. Lung Mechanics: An Inverse Modeling Approach; Cambridge University Press: New York, NY, USA, 2009. [Google Scholar]
- Schnell, D.; Timsit, J.F.; Darmon, M.; Vesin, A.; Goldgran-Toledano, D.; Dumenil, A.S.; Garrouste-Orgeas, M.; Adrie, C.; Bouadma, L.; Planquette, B.; et al. Noninvasive mechanical ventilation in acute respiratory failure: Trends in use and outcomes. Intensiv. Care Med. 2014, 40, 582–591. [Google Scholar] [CrossRef] [PubMed]
- Slutsky, A.S.; Ranieri, V.M. Ventilator-induced lung injury. N. Engl. J. Med. 2013, 369, 2126–2136. [Google Scholar] [CrossRef] [PubMed]
- Berlin, D.A.; Gulick, R.M.; Martinez, F.J. Severe Covid-19. N. Engl. J. Med. 2020, 5, 1–10. [Google Scholar] [CrossRef]
- Das, A.; Menon, P.H.J.; Bates, D. Optimization of Mechanical Ventilator Settings for Pulmonary Disease States. IEEE Trans. Biomed. Eng. 2013, 60, 1599–1607. [Google Scholar] [CrossRef]
- Clegg, J. A nonlinear integrator for servomechanisms. Trans. Am. Inst. Electr. Eng. Part II Appl. Ind. 1958, 77, 41–42. [Google Scholar] [CrossRef]
- Bunting, L.; Roy, S.; Pinson, H.; Greensweig, T. A novel inline PEEP valve design for differential multi-ventilation. Am. J. Emerg. Med. 2020. [Google Scholar] [CrossRef]
- Radogna, A.V.; Siciliano, P.A.; Sabina, S.; Sabato, E.; Capone, S. A Low-Cost Breath Analyzer Module in Domiciliary Non-Invasive Mechanical Ventilation for Remote COPD Patient Monitoring. Sensors 2020, 20, 653. [Google Scholar] [CrossRef] [PubMed]
- Al Husseini, A.M.; Lee, H.J.; Negrete, J.; Powelson, S.; Servi, A.T.; Slocum, A.H.; Saukkonen, J. Design and prototyping of a low-cost portable mechanical ventilator. J. Med. Devices 2010, 4, 027514. [Google Scholar] [CrossRef] [PubMed]
- Anzalone, G.C.; Zhang, C.; Wijnen, B.; Sanders, P.G.; Pearce, J.M. A Low-Cost Open-Source Metal 3-D Printer. IEEE Access 2013, 1, 803–810. [Google Scholar] [CrossRef]
- Nguyen, H.Q.; Loan, T.T.K.; Mao, B.D.; Huh, E.N. Low cost real-time system monitoring using Raspberry Pi. In Proceedings of the 2015 Seventh International Conference on Ubiquitous and Future Networks, Sapporo, Japan, 7–10 July 2015; pp. 857–859. [Google Scholar]
- Abaya, W.F.; Basa, J.; Sy, M.; Abad, A.C.; Dadios, E.P. Low cost smart security camera with night vision capability using Raspberry Pi and OpenCV. In Proceedings of the 2014 International Conference on Humanoid, Nanotechnology, Information Technology, Communication and Control, Environment and Management (HNICEM), Puerto Princesa, Philippines, 12–16 November 2014; pp. 1–6. [Google Scholar]
- Deshmukh, A.D.; Shinde, U.B. A low cost environment monitoring system using raspberry Pi and arduino with Zigbee. In Proceedings of the 2016 International Conference on Inventive Computation Technologies (ICICT), Coimbatore, India, 26–27 August 2016; Volume 3, pp. 1–6. [Google Scholar]
- Brown, B.; Roberts, J. Principles of artificial ventilation. Anaesth. Intensiv. Care Med. 2019, 20, 72–84. [Google Scholar] [CrossRef]
- Amato, M.B.P.; Marini, J.J. Pressure-controlled and inverse-ratio ventilation. In Principles and Practice of Mechanical Ventilation, 3rd ed.; Tobin, M.J., Ed.; McGraw-Hill: New York, NY, USA, 2013; pp. 227–251. [Google Scholar]
- Bhargava, A.; Kumar, A. Arduino controlled robotic arm. In Proceedings of the 2017 International conference of Electronics, Communication and Aerospace Technology (ICECA), Coimbatore, India, 20–22 April 2017; Volume 2, pp. 376–380. [Google Scholar]
- Klein, J.; Frie, K.G.; Blum, K.; von dem Knesebeck, O. Psychosocial stress at work and perceived quality of care among clinicians in surgery. BMC Health Serv. Res. 2011, 11, 109. [Google Scholar] [CrossRef] [PubMed]
- Weigl, M.; Schneider, A.; Hoffmann, F.; Angerer, P. Work stress, burnout, and perceived quality of care: A cross-sectional study among hospital pediatricians. Eur. J. Pediatr. 2015, 174, 1237–1246. [Google Scholar] [CrossRef]
- Acho Zuppa, L. Nonlinear reset integrator control design: Application to the active suspension control of vehicles. In Proceedings of the IASTED International Conference Modelling, Identification and Control (MIC 2014), Innsbruck, Austria, 17–19 February 2014; pp. 226–228. [Google Scholar]
- Hollot, C. Revisiting Clegg integrators: Periodicity, stability and IQCs. IFAC Proc. Vol. 1997, 30, 31–38. [Google Scholar] [CrossRef]
- Bates, J.H.T.; Smith, B.J. Ventilator-induced lung injury and lung mechanics. Ann. Transl. Med. 2018, 6, 378. [Google Scholar] [CrossRef]
- Nieman, G.F.; Gatto, L.A.; Andrews, P.; Satalin, J.; Camporota, L.; Daxon, B.; Blair, S.J.; Al-Khalisy, H.; Madden, M.; Kollisch-Singule, M.; et al. Prevention and treatment of acute lung injury with time-controlled adaptive ventilation: Physiologically informed modification of airway pressure release ventilation. Ann. Intensiv. Care 2020, 10, 1–16. [Google Scholar] [CrossRef]
- Jawde, S.B.; Walkey, A.J.; Majumdar, A.; O’Connor, G.T.; Smith, B.J.; Bates, J.H.; Lutchen, K.R.; Suki, B. Tracking respiratory mechanics around natural breathing rates via variable ventilation. Sci. Rep. 2020, 10, 1–12. [Google Scholar]
- Lellouche, F.; Delorme, M.; Brochard, L. Impact of respiratory rate and dead space in the current era of lung protective mechanical ventilation. Chest 2020, 158, 45–47. [Google Scholar] [CrossRef] [PubMed]











© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Acho, L.; Vargas, A.N.; Pujol-Vázquez, G. Low-Cost, Open-Source Mechanical Ventilator with Pulmonary Monitoring for COVID-19 Patients. Actuators 2020, 9, 84. https://doi.org/10.3390/act9030084
Acho L, Vargas AN, Pujol-Vázquez G. Low-Cost, Open-Source Mechanical Ventilator with Pulmonary Monitoring for COVID-19 Patients. Actuators. 2020; 9(3):84. https://doi.org/10.3390/act9030084
Chicago/Turabian StyleAcho, Leonardo, Alessandro N. Vargas, and Gisela Pujol-Vázquez. 2020. "Low-Cost, Open-Source Mechanical Ventilator with Pulmonary Monitoring for COVID-19 Patients" Actuators 9, no. 3: 84. https://doi.org/10.3390/act9030084
APA StyleAcho, L., Vargas, A. N., & Pujol-Vázquez, G. (2020). Low-Cost, Open-Source Mechanical Ventilator with Pulmonary Monitoring for COVID-19 Patients. Actuators, 9(3), 84. https://doi.org/10.3390/act9030084