Elevated Baseline Salivary Protease Activity May Predict the Steadiness of Gingival Inflammation During Periodontal Healing: A 12-Week Follow-Up Study on Adults

 , , ,
, , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
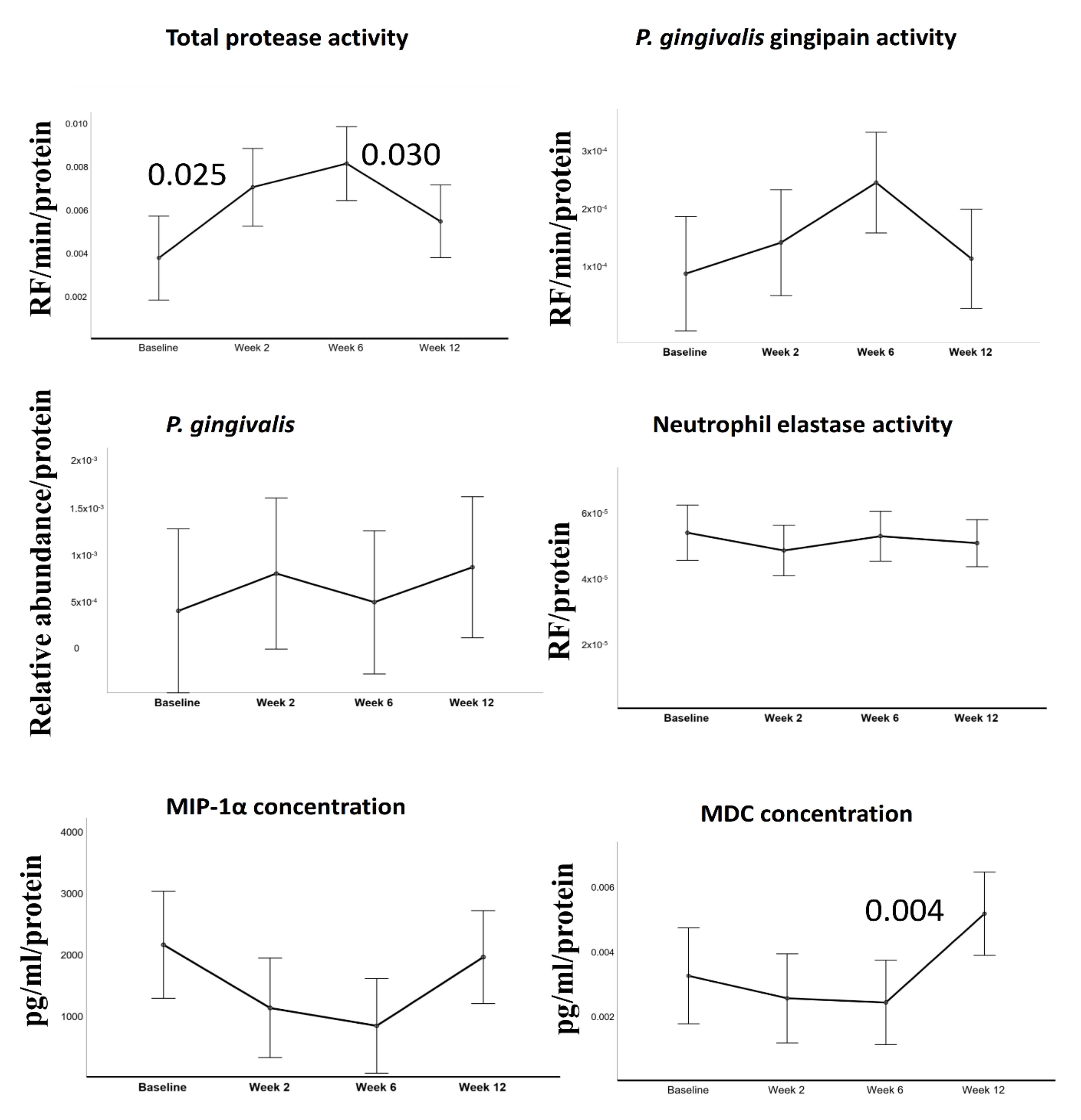
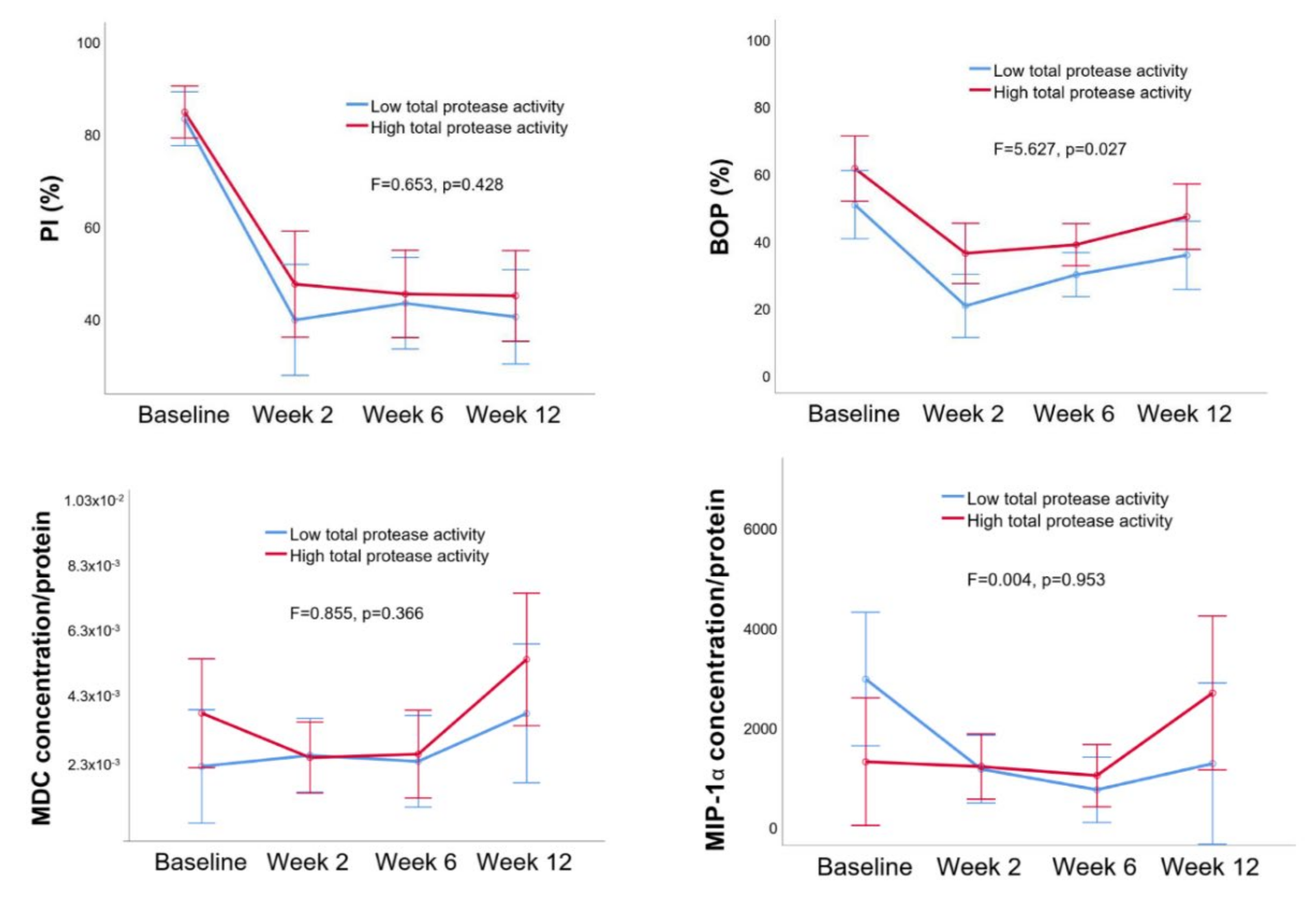
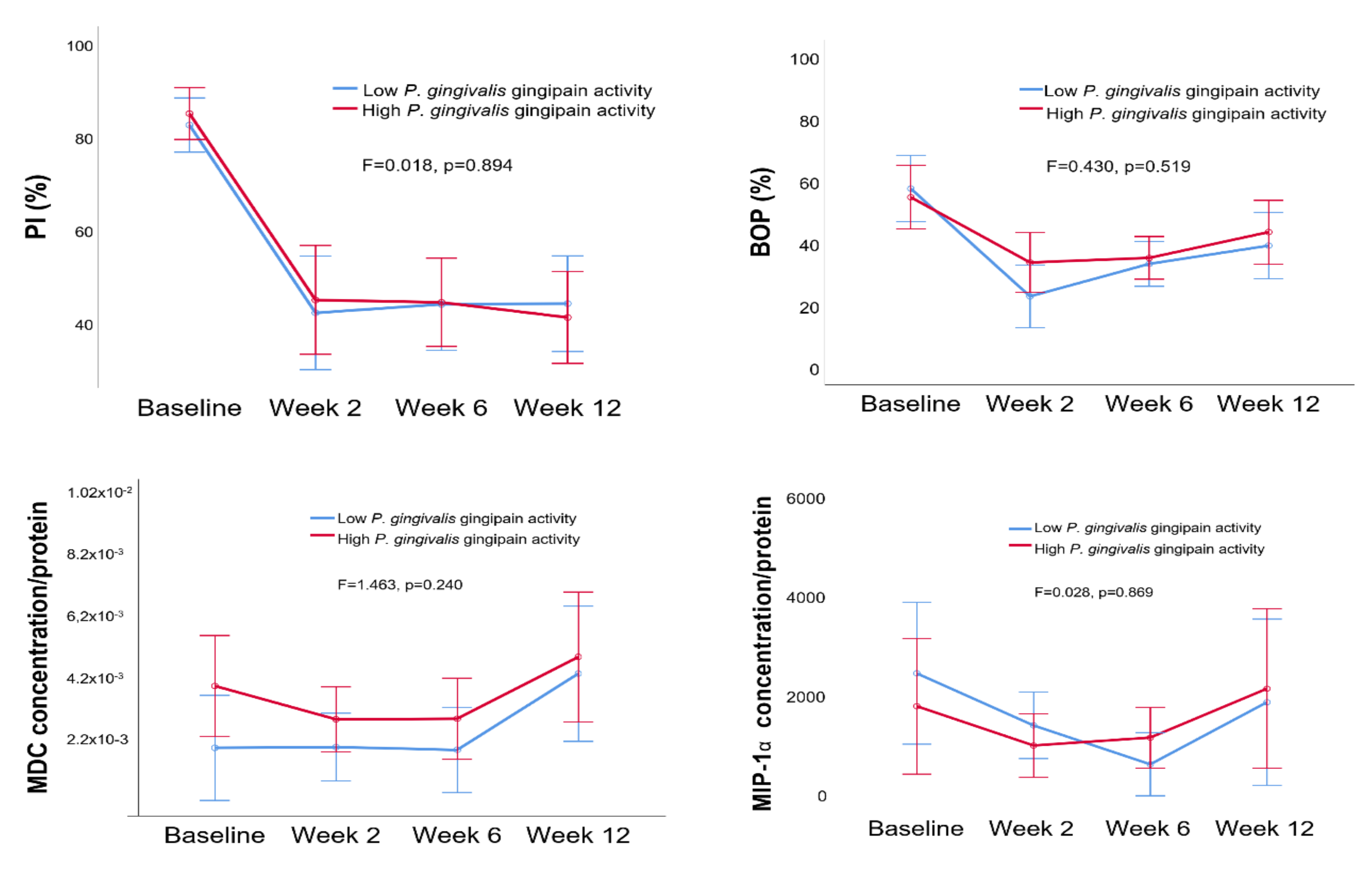
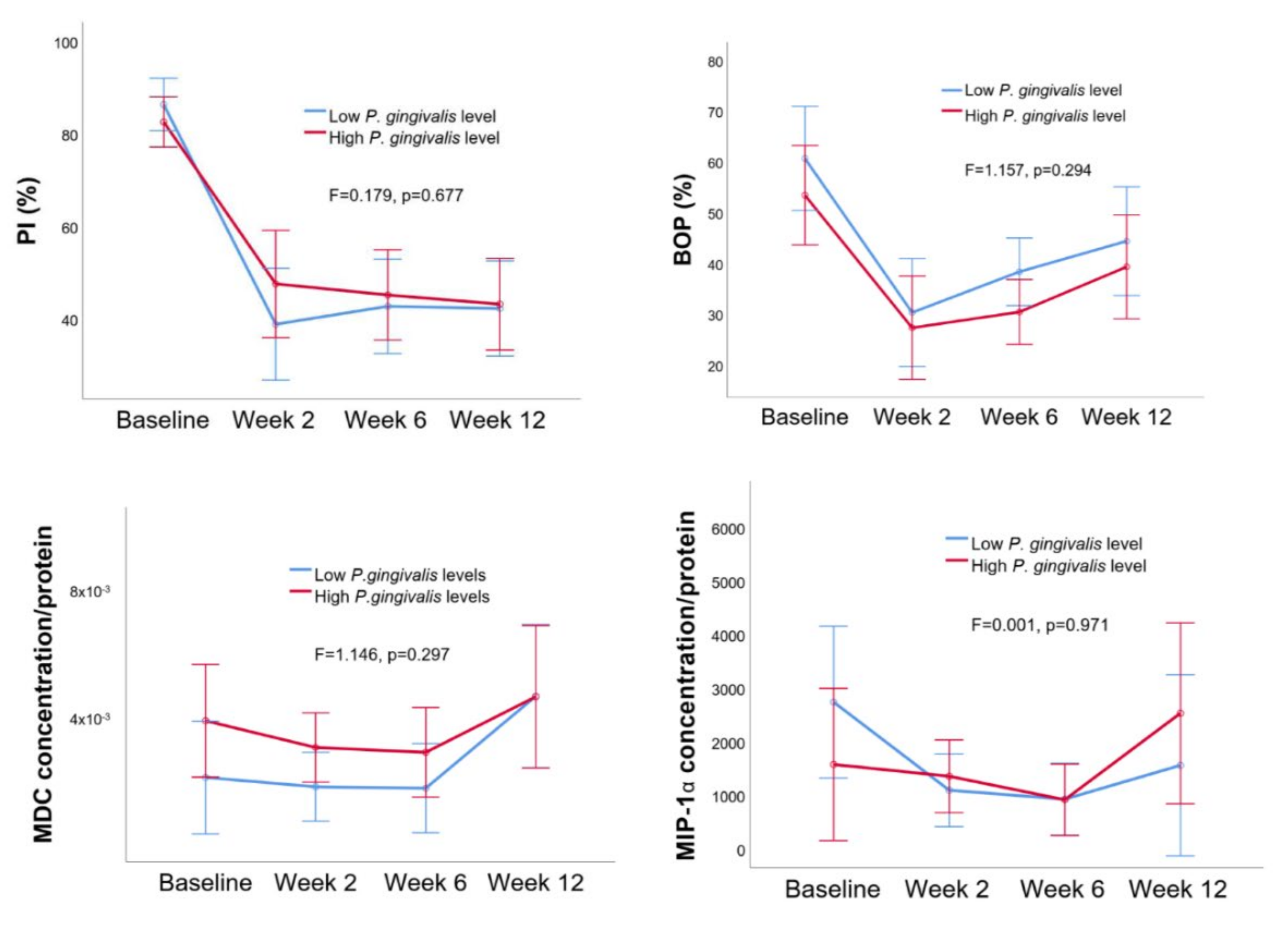
2. Results
3. Discussion
4. Materials and Methods
4.1. Study Population
4.2. Clinical Examination and Periodontal Treatment
4.3. Saliva Collection
4.4. Analyses of P. gingivalis Gingipain, Total Protease, and Neutrophil Elastase Activities
4.5. Analyses of Salivary P. gingivalis Relative Abundance and MIP-1α and MDC Concentrations
4.6. Analysis of Salivary Protein Levels
4.7. Statistical Analysis
Author Contributions
Funding
Conflicts of Interest
Ethical Statement
References
- Andrian, E.; Grenier, D.; Rouabhia, M. Porphyromonas gingivalis-epithelial cell interactions in periodontitis. J. Dent. Res. 2006, 85, 392–403. [Google Scholar] [CrossRef] [PubMed]
- Potempa, J.; Pike, R.N. Corruption of innate immunity by bacterial proteases. J. Innate. Immun. 2009, 1, 70–87. [Google Scholar] [CrossRef]
- Grande, M.; Belstrøm, D.; Damgaard, C.; Holmstrup, P.; Thangaraj, S.S.; Nielsen, C.H.; Palarasah, Y. Complement split product C3c in saliva as biomarker for periodontitis and response to periodontal treatment. J. Periodontal. Res. 2020, 18. [Google Scholar] [CrossRef] [PubMed]
- Chang, A.M.; Liu, Q.; Hajjar, A.M.; Greer, A.; McLean, J.S.; Darveau, R.P. Toll-like receptor-2 and -4 responses regulate neutrophil infiltration into the junctional epithelium and significantly contribute to the composition of the oral microbiota. J. Periodontol. 2019, 90, 1202–1212. [Google Scholar] [CrossRef]
- Könönen, E.; Gursoy, M.; Gursoy, U.K. Periodontitis: A Multifaceted Disease of Tooth-Supporting Tissues. J. Clin. Med. 2019, 8, 1135. [Google Scholar] [CrossRef] [PubMed]
- Aukhil, I. Biology of Wound Healing. Periodontology 2000 2000, 22, 44–50. [Google Scholar] [CrossRef]
- Davies, L.C.; Jenkins, S.J.; Allen, J.E.; Taylor, P.R. Tissue-resident macrophages. Nat. Immunol. 2013, 14, 986–995. [Google Scholar] [CrossRef]
- Gemmell, E.; Seymour, G.J. Cytokine profiles of cells extracted from humans with periodontal diseases. J. Dent. Res. 1998, 77, 16–26. [Google Scholar] [CrossRef]
- Gemmell, E.; Carter, C.L.; Seymour, G.J. Chemokines in human periodontal disease tissues. Clin. Exp. Immunol. 2001, 125, 134–141. [Google Scholar] [CrossRef]
- Pike, R.; McGraw, W.; Potempa, J.; Travis, J. Lysine- and arginine-specific proteinases from Porphyromonas gingivalis. Isolation, characterization, and evidence for the existence of complexes with hemagglutinins. J. Biol. Chem. 1994, 269, 406–411. [Google Scholar]
- Yamada, M.; Ikegami, A.; Kuramitsu, H.K. Synergistic biofilm formation by Treponema denticola and Porphyromonas gingivalis. FEMS. Microbiol. Lett. 2005, 250, 271–277. [Google Scholar] [CrossRef] [PubMed]
- Guo, S.; DiPietro, L.A. Factors Affecting Wound Healing. J. Dent. Res. 2010, 89, 219–229. [Google Scholar] [CrossRef] [PubMed]
- Maisetta, G.; Brancatisano, F.L.; Esin, S.; Campa, M.; Batoni, G. Gingipains produced by Porphyromonas gingivalis ATCC49417 degrade human-β-defensin 3 and affect peptide’s antibacterial activity in vitro. Peptides 2011, 32, 1073–1077. [Google Scholar] [CrossRef] [PubMed]
- Laheij, A.M.; van Loveren, C.; Deng, D.; de Soet, J.J. The impact of virulence factors of Porphyromonas gingivalis on wound healing in vitro. J. Oral. Microbiol. 2015, 7, 27543. [Google Scholar] [CrossRef] [PubMed]
- DeCarlo, A.A.; Grenett, H.E.; Harber, G.J.; Windsor, L.J.; Bodden, M.K.; Birkedal-Hansen, B.; Birkedal-Hansen, H. Induction of matrix metalloproteinases and a collagen-degrading phenotype in fibroblasts and epithelial cells by secreted Porphyromonas gingivalis proteinase. J. Periodontal. Res. 1998, 33, 408–420. [Google Scholar] [CrossRef]
- Gürsoy, U.K.; Pussinen, P.J.; Salomaa, V.; Syrjäläinen, S.; Könönen, E. Cumulative use of salivary markers with an adaptive design improves detection of periodontal disease over fixed biomarker thresholds. Acta. Odontol. Scand. 2018, 76, 493–496. [Google Scholar] [CrossRef]
- Liukkonen, J.; Gürsoy, U.K.; Könönen, E.; Akhi, R.; Salminen, A.; Liljestrand, J.M.; Pradhan-Palikhe, P.; Pietiäinen, M.; Sorsa, T.; Persson, G.R.; et al. Immunological and Microbiological Profiling of Cumulative Risk Score for Periodontitis. Diagnostics (Basel) 2020, 10, 560. [Google Scholar] [CrossRef]
- Bikker, F.J.; Nascimento, G.G.; Nazmi, K.; Silbereisen, A.; Belibasakis, G.N.; Kaman, W.E.; Lopez, R.; Bostanci, N. Salivary Total Protease Activity Based on a Broad-Spectrum Fluorescence Resonance Energy Transfer Approach to Monitor Induction and Resolution of Gingival Inflammation. Mol. Diagn. Ther. 2019, 23, 667–676. [Google Scholar] [CrossRef]
- Özdemir, M.; Caglayan, F.; Bikker, F.J.; Pussinen, P.; Könönen, E.; Yamalik, N.; Gürsoy, M.; Fteita, D.; Nazmi, K.; Güncü, G.N.; et al. Gingival tissue human beta-defensin levels in relation to infection and inflammation. J. Clin. Periodontol. 2020, 47, 309–318. [Google Scholar] [CrossRef]
- Grande, M.A.; Belstrøm, D.; Damgaard, C.; Holmstrup, P.; Könönen, E.; Gursoy, M.; Gursoy, U.K. Salivary concentrations of macrophage activation-related chemokines are influenced by non-surgical periodontal treatment: A 12-week follow-up study. J. Oral. Microbiol. 2019, 12, 1694383. [Google Scholar] [CrossRef]
- Nieminen, A.; Norlund, L.; Uitto, V.J. The effect of treatment on the activity of salivary proteases and glycosidases in adults with advanced periodontitis. J. Periodontol. 1993, 64, 297–301. [Google Scholar] [CrossRef] [PubMed]
- Belstrøm, D.; Grande, M.A.; Sembler-Møller, M.L.; Kirkby, N.; Cotton, S.L.; Paster, B.J.; Holmstrup, P. Influence of periodontal treatment on subgingival and salivary microbiotas. J. Periodontol. 2018, 89, 531–539. [Google Scholar] [CrossRef] [PubMed]
- Memmert, S.; Nokhbehsaim, M.; Damanaki, A.; Nogueira, A.V.B.; Papadopoulou, A.K.; Piperi, C.; Basdra, E.K.; Rath-Deschner, B.; Götz, W.; Cirelli, J.A.; et al. Role of cathepsin S In periodontal wound healing-an in vitro study on human PDL cells. BMC. Oral Health 2018, 18, 60. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Lim, J.; Jeon, H.H.; Xu, F.; Tian, C.; Miao, F.; Hameedaldeen, A.; Graves, D.T. FOXO1 deletion in keratinocytes improves diabetic wound healing through MMP9 regulation. Sci. Rep. 2017, 7, 10565. [Google Scholar] [CrossRef]
- Jha, A.; George, J.P.; Chandrashekhar, G. Estimation and Correlation of MMP-8 Levels in GCF and Serum with Wound Healing and Clinical Outcomes of Coronally Advanced Flap and Sub-Epithelial Connective Tissue Graft for Root Coverage—A Controlled Clinical Trial. J. Int. Acad. Periodontol. 2019, 21, 11–19. [Google Scholar]
- Gul, S.S.; Zardawi, F.M.; Sha, A.M.; Rauf, A.M. Assessment of Creeping Attachment after Free Gingival Graft in Treatment of Isolated Gingival Recession. J. Int. Acad. Periodontol. 2019, 21, 125–131. [Google Scholar]
- Galli, G.; Chantry, D.; Annunziato, F.; Romagnani, P.; Cosmi, L.; Lazzeri, E.; Manetti, R.; Maggi, E.; Gray, P.W.; Romagnani, S. Macrophage-derived chemokine production by activated human T cells in vitro and in vivo: Preferential association with the production of type 2 cytokines. Eur. J. Immunol. 2000, 30, 204–210. [Google Scholar] [CrossRef]
- Kabashima, H.; Yoneda, M.; Nagata, K.; Hirofuji, T.; Maeda, K. The presence of chemokine (MCP-1, MIP-1alpha, MIP-1beta, IP-10, RANTES)-positive cells and chemokine receptor (CCR5, CXCR3)-positive cells in inflamed human gingival tissues. Cytokine 2002, 20, 70–77. [Google Scholar] [CrossRef]
- Ryu, O.H.; Choi, S.J.; Linares, A.M.; Song, I.S.; Kim, Y.J.; Jang, K.T.; Hart, T.C. Gingival epithelial cell expression of macrophage inflammatory protein-1alpha induced by interleukin-1beta and lipopolysaccharide. J. Periodontol. 2007, 78, 1627–1634. [Google Scholar] [CrossRef]
- Sexton, W.M.; Lin, Y.; Kryscio, R.J.; Dolphus, R.; Dawson, D.M.D.; Jeffrey, L.; Miller, C.S. Salivary biomarkers of periodontal disease in response to treatment. J. Clin. Periodontol. 2011, 38, 434–441. [Google Scholar] [CrossRef]
- Stathopoulou, P.G.; Benakanakere, M.R.; Galicia, J.C.; Kinane, D.F. The host cytokine response to Porphyromonas gingivalis is modified by gingipains. Oral. Microbiol. Immunol. 2009, 24, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Wolf, M.; Clark-Lewis, I.; Buri, C.; Langen, H.; Lis, M.; Mazzucchelli, L. Cathepsin D specifically cleaves the chemokines macrophage inflammatory protein-1 alpha, macrophage inflammatory protein-1 beta, and SLC that are expressed in human breast cancer. Am. J. Pathol. 2003, 162, 1183–1190. [Google Scholar] [CrossRef]
- American Academy of Periodontology Task Force Report on the Update to the 1999 Classification of Periodontal Diseases and Conditions. J. Periodontol. 2015, 86, 835–838. [CrossRef] [PubMed]
- Galassi, F.; Kaman, W.E.; Anssari, M.D.; van der Horst, J.; Wismeijer, D.; Crielaard, W.; Laine, M.L.; Veerman, E.C.; Bikker, F.J.; Loos, B.G. Comparing culture, real-time PCR and fluorescence resonance energy transfer technology for detection of Porphyromonas gingivalis in patients with or without peri-implant infections. J. Periodontal. Res. 2012, 47, 616–625. [Google Scholar] [CrossRef] [PubMed]
- Kaman, W.E.; Galassi, F.; de Soet, J.J.; Bizzarro, S.; Loos, B.G.; Veerman, E.C.I.; Belkum, A.V.; Hays, J.P.; Floris, J.B. Highly specific protease-based approach for detection of Porphyromonas gingivalis in diagnosis of periodontitis. J. Clin. Microbiol. 2012, 50, 104–112. [Google Scholar] [CrossRef]
- Janus, M.M.; Keijser, B.J.; Bikker, F.J.; Exterkate, R.A.; Crielaard, W.; Krom, B.P. In vitro phenotypic differentiation towards commensal and pathogenic oral biofilms. Biofouling 2015, 31, 503–510. [Google Scholar] [CrossRef]
- Hammond, J.B.; Kruger, N.J. The Bradford method for protein quantitation. Methods. Mol. Biol. 1988, 3, 25–32. [Google Scholar] [CrossRef]




© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gürsoy, U.K.; Fteita, D.; Bikker, F.J.; Grande, M.A.; Nazmi, K.; Gürsoy, M.; Könönen, E.; Belstrøm, D. Elevated Baseline Salivary Protease Activity May Predict the Steadiness of Gingival Inflammation During Periodontal Healing: A 12-Week Follow-Up Study on Adults. Pathogens 2020, 9, 751. https://doi.org/10.3390/pathogens9090751
Gürsoy UK, Fteita D, Bikker FJ, Grande MA, Nazmi K, Gürsoy M, Könönen E, Belstrøm D. Elevated Baseline Salivary Protease Activity May Predict the Steadiness of Gingival Inflammation During Periodontal Healing: A 12-Week Follow-Up Study on Adults. Pathogens. 2020; 9(9):751. https://doi.org/10.3390/pathogens9090751
Chicago/Turabian StyleGürsoy, Ulvi Kahraman, Dareen Fteita, Floris J. Bikker, Maria Anastasia Grande, Kamran Nazmi, Mervi Gürsoy, Eija Könönen, and Daniel Belstrøm. 2020. "Elevated Baseline Salivary Protease Activity May Predict the Steadiness of Gingival Inflammation During Periodontal Healing: A 12-Week Follow-Up Study on Adults" Pathogens 9, no. 9: 751. https://doi.org/10.3390/pathogens9090751
APA StyleGürsoy, U. K., Fteita, D., Bikker, F. J., Grande, M. A., Nazmi, K., Gürsoy, M., Könönen, E., & Belstrøm, D. (2020). Elevated Baseline Salivary Protease Activity May Predict the Steadiness of Gingival Inflammation During Periodontal Healing: A 12-Week Follow-Up Study on Adults. Pathogens, 9(9), 751. https://doi.org/10.3390/pathogens9090751