
A Bibliometric Analysis of HPV-Positive Oropharyngeal Squamous Cell Carcinoma from 2000 to 2023

Abstract
1. Introduction
2. Methods
2.1. Data Collection
2.2. Data Analysis
3. Results
3.1. Main Information
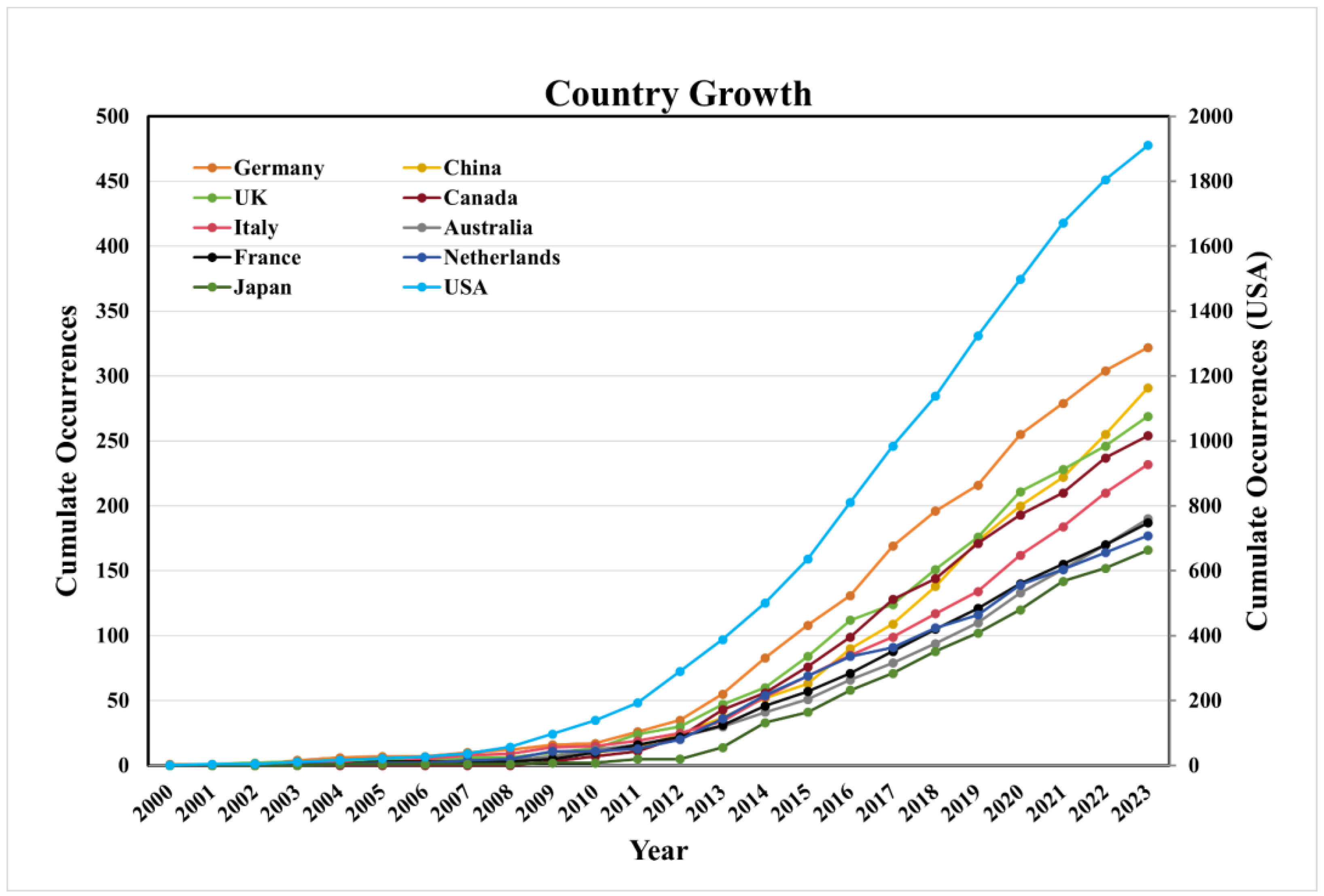
3.2. Analysis of HPV-Positive OPSCC Research at the National Level
3.3. Institution Analysis
3.4. Author Analysis
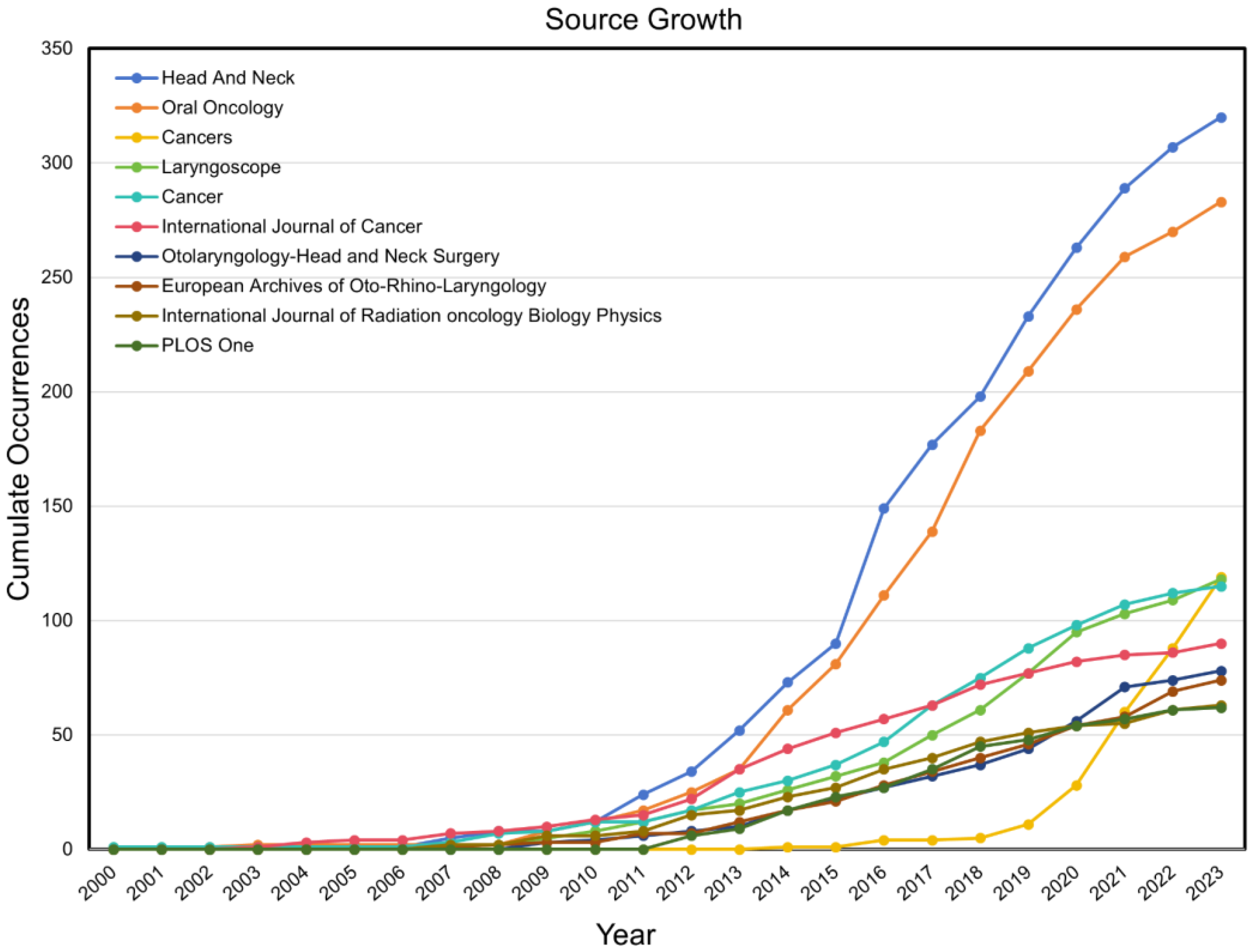
3.5. Journal Analysis
3.6. Top 10 Publications
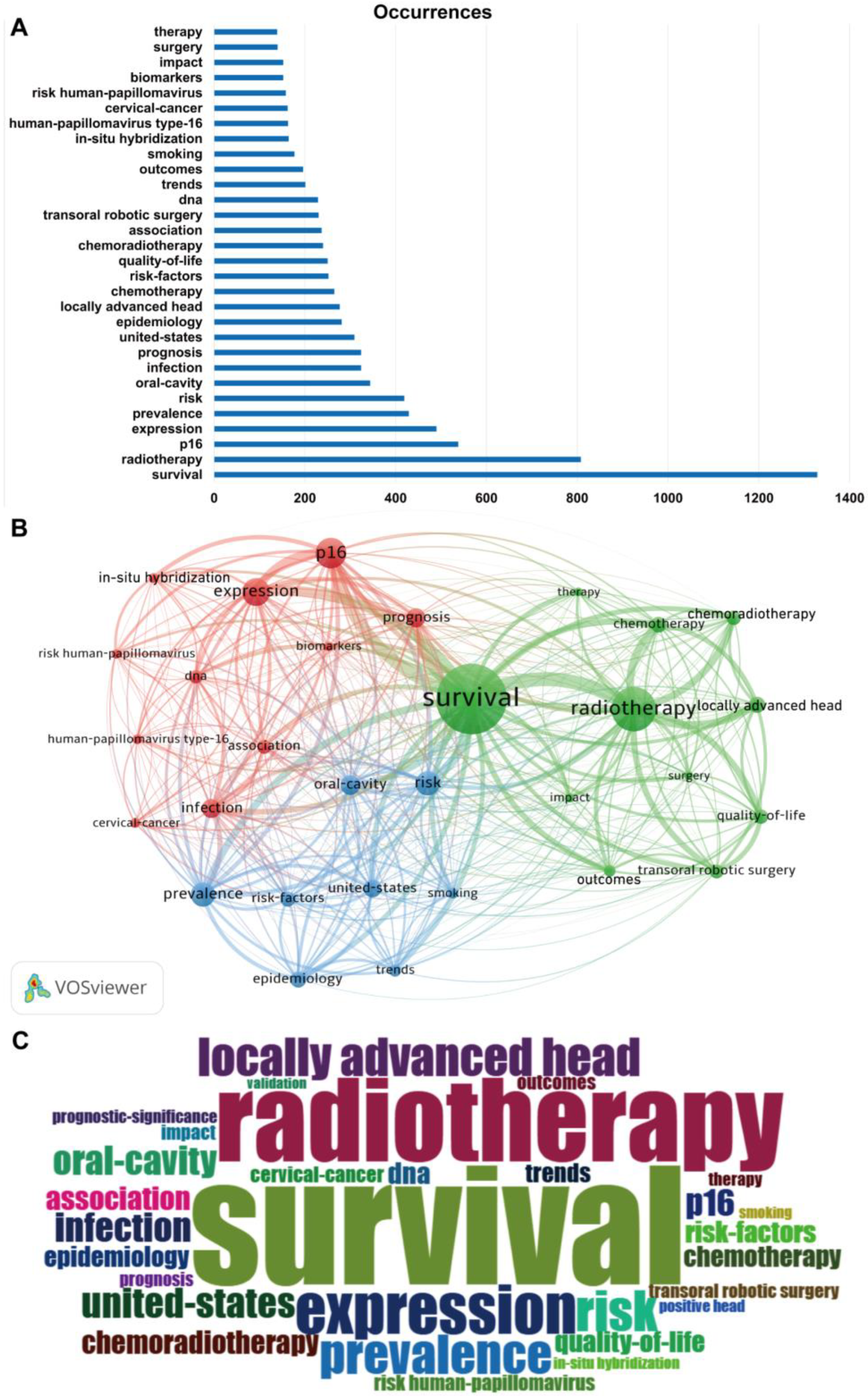
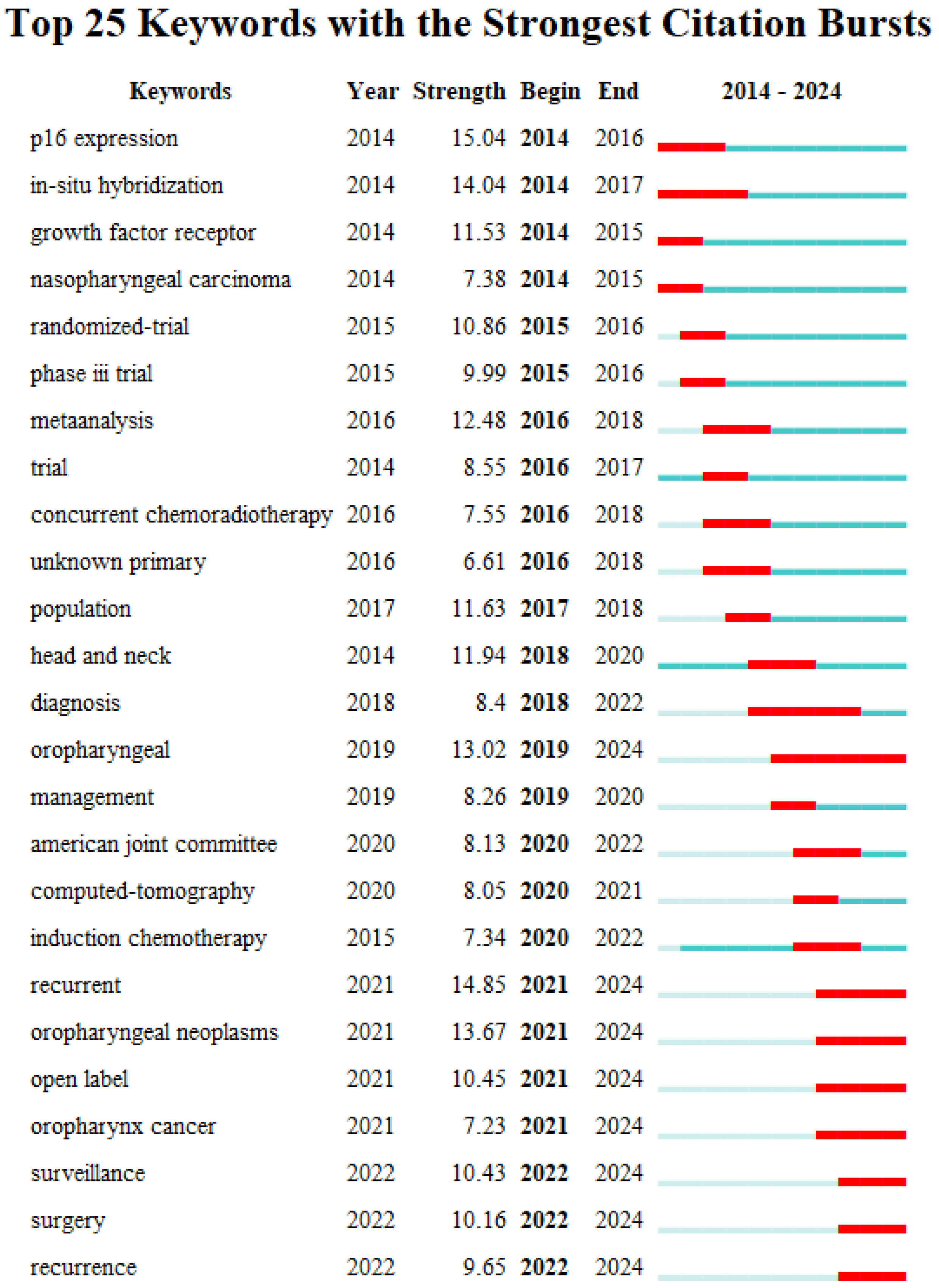
3.7. High-Frequency Keyword Analysis
4. Discussion
4.1. General Information
4.2. Hotspots and Frontiers
4.2.1. Epidemiology
4.2.2. HPV Status Detection Methods
4.2.3. Treatment Strategy
4.2.4. Prevention
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| HPV | human papillomavirus |
| OPSCC HPV-positive OPSCC | oropharyngeal squamous cell carcinoma human-papillomavirus-positive oropharyngeal squamous cell carcinoma |
| pRb | retinoblastoma protein |
| RT CRT WoSCC AJCC8 IHC ISH TORS | radiation chemoradiation Web of Science Core Collection the 8th edition of the American Joint Commission on Cancer immunohistology in situ hybridization transoral robotic surgery |
References
- Gillison, M.L.; Lowy, D.R. A causal role for human papillomavirus in head and neck cancer. Lancet 2004, 363, 1488–1489. [Google Scholar] [CrossRef]
- Lechner, M.; Liu, J.; Masterson, L.; Fenton, T.R. HPV-associated oropharyngeal cancer: Epidemiology, molecular biology and clinical management. Nat. Rev. Clin. Oncol. 2022, 19, 306–327. [Google Scholar] [CrossRef] [PubMed]
- Damgacioglu, H.; Sonawane, K.; Zhu, Y.; Li, R.; Balasubramanian, B.A.; Lairson, D.R.; Giuliano, A.R.; Deshmukh, A.A. Oropharyngeal cancer incidence and mortality trends in all 50 states in the US, 2001–2017. JAMA Otolaryngol.–Head Neck Surg. 2022, 148, 155–165. [Google Scholar] [CrossRef] [PubMed]
- Panwar, A.; Batra, R.; Lydiatt, W.M.; Ganti, A.K. Human papilloma virus positive oropharyngeal squamous cell carcinoma: A growing epidemic. Cancer Treat. Rev. 2014, 40, 215–219. [Google Scholar] [CrossRef]
- Zamani, M.; Gronhoj, C.; Jensen, D.H.; Carlander, A.F.; Agander, T.; Kiss, K.; Olsen, C.; Baandrup, L.; Nielsen, F.C.; Andersen, E.; et al. The current epidemic of HPV-associated oropharyngeal cancer: An 18-year Danish population-based study with 2,169 patients. Eur. J. Cancer 2020, 134, 52–59. [Google Scholar] [CrossRef] [PubMed]
- Schache, A.G.; Powell, N.G.; Cuschieri, K.S.; Robinson, M.; Leary, S.; Mehanna, H.; Rapozo, D.; Long, A.; Cubie, H.; Junor, E.; et al. HPV-related oropharynx cancer in the United Kingdom: An evolution in the understanding of disease etiology. Cancer Res. 2016, 76, 6598–6606. [Google Scholar] [CrossRef]
- Argirion, I.; Zarins, K.R.; McHugh, J.; Cantley, R.L.; Teeramatwanich, W.; Laohasiriwong, S.; Kasemsiri, P.; Naruikon, J.; Srimanta, P.; Chinn, S.B.; et al. Increasing prevalence of HPV in oropharyngeal carcinoma suggests adaptation of p16 screening in Southeast Asia. J. Clin. Virol. 2020, 132, 104637. [Google Scholar] [CrossRef]
- Lowy, D.R.; Munger, K. Prognostic implications of HPV in oropharyngeal cancer. N. Engl. J. Med. 2010, 363, 82–84. [Google Scholar] [CrossRef]
- Rampias, T.; Sasaki, C.; Weinberger, P.; Psyrri, A. E6 and e7 gene silencing and transformed phenotype of human papillomavirus 16-positive oropharyngeal cancer cells. J. Natl. Cancer Inst. 2009, 101, 412–423. [Google Scholar] [CrossRef]
- Zhang, H.S.; Postigo, A.A.; Dean, D.C. Active transcriptional repression by the Rb–E2F complex mediates G1 arrest triggered by p16INK4a, TGFβ, and contact inhibition. Cell 1999, 97, 53–61. [Google Scholar] [CrossRef]
- Gronhoj Larsen, C.; Gyldenlove, M.; Jensen, D.H.; Therkildsen, M.H.; Kiss, K.; Norrild, B.; Konge, L.; von Buchwald, C. Correlation between human papillomavirus and p16 overexpression in oropharyngeal tumours: A systematic review. Br. J. Cancer 2014, 110, 1587–1594. [Google Scholar] [CrossRef] [PubMed]
- Ndiaye, C.; Mena, M.; Alemany, L.; Arbyn, M.; Castellsague, X.; Laporte, L.; Bosch, F.X.; de Sanjose, S.; Trottier, H. HPV DNA, E6/E7 mRNA, and p16INK4a detection in head and neck cancers: A systematic review and meta-analysis. Lancet Oncol. 2014, 15, 1319–1331. [Google Scholar] [CrossRef] [PubMed]
- Ang, K.K.; Harris, J.; Wheeler, R.; Weber, R.; Rosenthal, D.I.; Nguyen-Tân, P.F.; Westra, W.H.; Chung, C.H.; Jordan, R.C.; Lu, C.; et al. Human papillomavirus and survival of patients with oropharyngeal cancer. N. Engl. J. Med. 2010, 363, 24–35. [Google Scholar] [CrossRef] [PubMed]
- O’Rorke, M.A.; Ellison, M.V.; Murray, L.J.; Moran, M.; James, J.; Anderson, L.A. Human papillomavirus related head and neck cancer survival: A systematic review and meta-analysis. Oral Oncol. 2012, 48, 1191–1201. [Google Scholar] [CrossRef]
- Chera, B.S.; Amdur, R.J. Current status and future directions of treatment deintensification in human papilloma virus-associated oropharyngeal squamous cell carcinoma. Semin. Radiat. Oncol. 2018, 28, 27–34. [Google Scholar] [CrossRef]
- Quon, H.; Forastiere, A.A. Controversies in Treatment Deintensification of Human Papillomavirus–Associated Oropharyngeal Carcinomas: Should We, How Should We, and for Whom? J. Clin. Oncol. 2013, 31, 520–522. [Google Scholar] [CrossRef]
- Sinha, P.; Pipkorn, P.; Thorstad, W.L.; Gay, H.A.; Haughey, B.H. Does elimination of planned postoperative radiation to the primary bed in p16-positive, transorally-resected oropharyngeal carcinoma associate with poorer outcomes? Oral Oncol. 2016, 61, 127–134. [Google Scholar] [CrossRef]
- Cramer, J.D.; Ferris, R.L.; Kim, S.; Duvvuri, U. Primary surgery for human papillomavirus-associated oropharyngeal cancer: Survival outcomes with or without adjuvant treatment. Oral Oncol. 2018, 87, 170–176. [Google Scholar] [CrossRef]
- Urban, D.; Corry, J.; Rischin, D. What is the best treatment for patients with human papillomavirus-positive and -negative oropharyngeal cancer? Cancer 2014, 120, 1462–1470. [Google Scholar] [CrossRef]
- Yom, S.S.; Torres-Saavedra, P.; Caudell, J.J.; Waldron, J.N.; Gillison, M.L.; Xia, P.; Truong, M.T.; Kong, C.; Jordan, R.; Subramaniam, R.M.; et al. Reduced-Dose Radiation Therapy for HPV-Associated Oropharyngeal Carcinoma (NRG Oncology HN002). J. Clin. Oncol. 2021, 39, 956–965. [Google Scholar] [CrossRef]
- Gillison, M.L.; Trotti, A.M.; Harris, J.; Eisbruch, A.; Harari, P.M.; Adelstein, D.J.; Jordan, R.C.K.; Zhao, W.; Sturgis, E.M.; Burtness, B.; et al. Radiotherapy plus cetuximab or cisplatin in human papillomavirus-positive oropharyngeal cancer (NRG Oncology RTOG 1016): A randomised, multicentre, non-inferiority trial. Lancet 2019, 393, 40–50. [Google Scholar] [CrossRef]
- Hicks, D.; Wouters, P.; Waltman, L.; de Rijcke, S.; Rafols, I. Bibliometrics: The Leiden Manifesto for research metrics. Nature 2015, 520, 429–431. [Google Scholar] [CrossRef] [PubMed]
- Cai, X.-J.; Zhang, H.-Y.; Zhang, J.-Y.; Li, T.-J. Bibliometric analysis of immunotherapy for head and neck squamous cell carcinoma. J. Dent. Sci. 2023, 18, 872–882. [Google Scholar] [CrossRef] [PubMed]
- de Winter, J.C.F.; Zadpoor, A.A.; Dodou, D. The expansion of Google Scholar versus Web of Science: A longitudinal study. Scientometrics 2013, 98, 1547–1565. [Google Scholar] [CrossRef]
- Pei, Z.; Chen, S.; Ding, L.; Liu, J.; Cui, X.; Li, F.; Qiu, F. Current perspectives and trend of nanomedicine in cancer: A review and bibliometric analysis. J. Control. Release 2022, 352, 211–241. [Google Scholar] [CrossRef]
- Ye, L.; Liang, R.; Liu, X.; Li, J.; Yue, J.; Zhang, X. Frailty and sarcopenia: A bibliometric analysis of their association and potential targets for intervention. Ageing Res. Rev. 2023, 92, 102111. [Google Scholar] [CrossRef]
- Zeng, N.; Sun, J.-X.; Liu, C.-Q.; Xu, J.-Z.; An, Y.; Xu, M.-Y.; Zhang, S.-H.; Zhong, X.-Y.; Ma, S.-Y.; He, H.-D.; et al. Knowledge mapping of application of image-guided surgery in prostate cancer: A bibliometric analysis (2013–2023). Int. J. Surg. 2024, 110, 2992–3007. [Google Scholar] [CrossRef]
- Dahlstrom, K.R.; Adler-Storthz, K.; Etzel, C.J.; Liu, Z.; Dillon, L.; El-Naggar, A.K.; Spitz, M.R.; Schiller, J.T.; Wei, Q.; Sturgis, E.M. Human papillomavirus type 16 infection and squamous cell carcinoma of the head and neck in never-smokers: A matched pair analysis. Clin. Cancer Res. 2003, 9, 2620–2626. [Google Scholar]
- Lydiatt, W.M.; Patel, S.G.; O’Sullivan, B.; Brandwein, M.S.; Ridge, J.A.; Migliacci, J.C.; Loomis, A.M.; Shah, J.P. Head and neck cancers—Major changes in the American Joint Committee on cancer eighth edition cancer staging manual. CA A Cancer J. Clin. 2017, 67, 122–137. [Google Scholar] [CrossRef]
- Klasen, C.; Wuerdemann, N.; Rothbart, P.; Prinz, J.; Eckel, H.N.C.; Suchan, M.; Kopp, C.; Johannsen, J.; Ziogas, M.; Charpentier, A.; et al. Sex-specific aspects in patients with oropharyngeal squamous cell carcinoma: A bicentric cohort study. BMC Cancer 2023, 23, 1054. [Google Scholar] [CrossRef]
- da Costa, A.A.; Guieiro, R.S.; Oliveira, I.G.; Tavares, T.S.; Meirelles, D.P.; Silva, E.V.; Silva, A.T.; León, J.E.; Aguiar, M.C.; Caldeira, P.C. HPV-related oropharyngeal carcinoma remains infrequent over 25 years in a Brazilian Oral Pathology Center: A cross-sectional study with literature review. Med. Oral Patol. Oral Cirugía Bucal 2020, 29, e498–e508. [Google Scholar] [CrossRef] [PubMed]
- Cleere, E.F.; Murphy, J.; Crotty, T.J.; Hintze, J.M.; Timon, C.V.I.; Kinsella, J.; Fitzgerald, C.W.R.; Lennon, P. HPV overtakes smoking as the leading cause of oropharyngeal cancer in Ireland: Experience of a head and neck surgery tertiary referral centre. Ir. J. Med. Sci. (1971-) 2024, 193, 2161–2169. [Google Scholar] [CrossRef] [PubMed]
- Carlander, A.-L.F.; Bendtsen, S.K.; Rasmussen, J.H.; Jakobsen, K.K.; Garset-Zamani, M.; Grønhøj, C.; Friborg, J.; Hutcheson, K.; Johnson, F.M.; Fuller, C.D.; et al. Clinical and prognostic differences in oropharyngeal squamous cell carcinoma in USA and Denmark, two HPV high-prevalence areas. Eur. J. Cancer 2024, 202, 113983. [Google Scholar] [CrossRef]
- Boscolo-Rizzo, P.; Polesel, J.; Del Mistro, A.; Fratta, E.; Lazzarin, C.; Menegaldo, A.; Lupato, V.; Fanetti, G.; Zanconati, F.; Guido, M.; et al. Rising trend in the prevalence of HPV-driven oropharyngeal squamous cell carcinoma during 2000–2022 in Northeastern Italy: Implication for using p16INK4a as a surrogate marker for HPV-driven carcinogenesis. Cancers 2023, 15, 2643. [Google Scholar] [CrossRef] [PubMed]
- Jamieson, L.M.; Antonsson, A.; Garvey, G.; Ju, X.; Smith, M.; Logan, R.M.; Johnson, N.W.; Hedges, J.; Sethi, S.; Dunbar, T.; et al. Prevalence of oral human papillomavirus infection among australian indigenous adults. JAMA Netw. Open 2020, 3, e204951. [Google Scholar] [CrossRef]
- Hauck, F.; Oliveira-Silva, M.; Dreyer, J.H.; Perrusi, V.J.F.; Arcuri, R.A.; Hassan, R.; Bonvicino, C.R.; Barros, M.H.M.; Niedobitek, G. Prevalence of HPV infection in head and neck carcinomas shows geographical variability: A comparative study from Brazil and Germany. Virchows Arch. 2015, 466, 685–693. [Google Scholar] [CrossRef]
- Reyes-Hernández, D.O.; Morán-Torres, A.; Jimenez-Lima, R.; Cano-Valdez, A.M.; Cortés-González, C.C.; Castro-Muñoz, L.J.; Olmedo-Nieva, L.; Maldonado-Frías, S.; Pazos-Salazar, N.G.; de Jesús Marín-Aquíno, J.; et al. HPV Prevalence and Predictive Biomarkers for Oropharyngeal Squamous Cell Carcinoma in Mexican Patients. Pathogens 2022, 11, 1527. [Google Scholar] [CrossRef]
- Chaturvedi, A.K.; Engels, E.A.; Pfeiffer, R.M.; Hernandez, B.Y.; Xiao, W.; Kim, E.; Jiang, B.; Goodman, M.T.; Sibug-Saber, M.; Cozen, W.; et al. Human papillomavirus and rising oropharyngeal cancer incidence in the United States. J. Clin. Oncol. 2011, 29, 4294–4301. [Google Scholar] [CrossRef]
- Scott-Wittenborn, N.; D’Souza, G.; Tewari, S.; Rooper, L.; Troy, T.; Drake, V.; Bigelow, E.O.; Windon, M.J.; Ryan, W.R.; Ha, P.K.; et al. Prevalence of human papillomavirus in head and neck cancers at tertiary care centers in the United States over time. Cancer 2022, 128, 1767–1774. [Google Scholar] [CrossRef]
- Sonawane, K.; Suk, R.; Chiao, E.Y.; Chhatwal, J.; Qiu, P.; Wilkin, T.; Nyitray, A.G.; Sikora, A.G.; Deshmukh, A.A. Oral Human Papillomavirus Infection: Differences in Prevalence Between Sexes and Concordance With Genital Human Papillomavirus Infection, NHANES 2011 to 2014. Ann. Intern. Med. 2017, 167, 714–724. [Google Scholar] [CrossRef]
- Mourad, M.; Jetmore, T.; Jategaonkar, A.A.; Moubayed, S.; Moshier, E.; Urken, M.L. Epidemiological Trends of Head and Neck Cancer in the United States: A SEER Population Study. J. Oral Maxillofac. Surg. 2017, 75, 2562–2572. [Google Scholar] [CrossRef] [PubMed]
- Taberna, M.; Mena, M.; Pavón, M.A.; Alemany, L.; Gillison, M.L.; Mesía, R. Human papillomavirus-related oropharyngeal cancer. Ann. Oncol. 2017, 28, 2386–2398. [Google Scholar] [CrossRef] [PubMed]
- Wichmann, G.; Rudolph, J.; Henger, S.; Engel, C.; Wirkner, K.; Wenning, J.R.; Zeynalova, S.; Wiegand, S.; Loeffler, M.; Wald, T.; et al. Is High-Risk Sexual Behavior a Risk Factor for Oropharyngeal Cancer? Cancers 2023, 15, 3356. [Google Scholar] [CrossRef] [PubMed]
- Sathasivam, H.P.; Davan, S.P.; Chua, S.M.; Rohaizat, R.F.; Japar, R.; Zakaria, Z.; Ahmad, A.R.; Hashim, H.; Marimuthu, S.G.; Liew, Y.T.; et al. Findings from a Malaysian multicentre study on oropharyngeal squamous cell carcinoma. Infect. Agents Cancer 2023, 18, 74. [Google Scholar] [CrossRef]
- Saiya, P.; Jantharapattana, K.; Dechaphunkul, A.; Jirapongsak, J.; Thongsuksai, P. HPV-Related Oropharyngeal Cancer in Southern Thailand: Proportion Trend and Survival Outcome. Asian Pac. J. Cancer Prev. 2024, 25, 57–64. [Google Scholar] [CrossRef]
- Ukpo, O.C.; Flanagan, J.J.; Ma, X.J.; Luo, Y.; Thorstad, W.L.; Lewis, J.S., Jr. High-risk human papillomavirus E6/E7 mRNA detection by a novel in situ hybridization assay strongly correlates with p16 expression and patient outcomes in oropharyngeal squamous cell carcinoma. Am. J. Surg. Pathol. 2011, 35, 1343–1350. [Google Scholar] [CrossRef]
- Randén-Brady, R.; Carpén, T.; Jouhi, L.; Syrjänen, S.; Haglund, C.; Tarkkanen, J.; Remes, S.; Mäkitie, A.; Mattila, P.S.; Silén, S.; et al. In situ hybridization for high-risk HPV E6/E7 mRNA is a superior method for detecting transcriptionally active HPV in oropharyngeal cancer. Hum. Pathol. 2019, 90, 97–105. [Google Scholar] [CrossRef]
- El-Naggar, A.K.; Westra, W.H. p16 expression as a surrogate marker for HPV-related oropharyngeal carcinoma: A guide for interpretative relevance and consistency. Head Neck 2011, 34, 459–461. [Google Scholar] [CrossRef]
- Gallus, R.; Nauta, I.H.; Marklund, L.; Rizzo, D.; Crescio, C.; Mureddu, L.; Tropiano, P.; Delogu, G.; Bussu, F. Accuracy of p16 IHC in classifying HPV-driven OPSCC in different populations. Cancers 2023, 15, 656. [Google Scholar] [CrossRef]
- Biron, V.L.; O’Connell, D.A.; Barber, B.; Clark, J.M.; Andrews, C.; Jeffery, C.C.; Côté, D.W.J.; Harris, J.; Seikaly, H. Transoral robotic surgery with radial forearm free flap reconstruction: Case control analysis. J. Otolaryngol.–Head Neck Surg. 2017, 46, 20. [Google Scholar] [CrossRef]
- Weinstein, G.S.; O’Malley, B.W., Jr.; Snyder, W.; Sherman, E.; Quon, H. Transoral robotic surgery: Radical tonsillectomy. Arch. Otolaryngol.–Head Neck Surg. 2007, 133, 1220–1226. [Google Scholar] [CrossRef] [PubMed]
- Duvvuri, U.; Myers, J.N. Contemporary management of oropharyngeal cancer. Curr. Probl. Surg. 2009, 46, 119–184. [Google Scholar] [CrossRef] [PubMed]
- O’Malley, B.W., Jr.; Weinstein, G.S.; Snyder, W.; Hockstein, N.G. Transoral robotic surgery (TORS) for base of tongue neoplasms. Laryngoscope 2006, 116, 1465–1472. [Google Scholar] [CrossRef] [PubMed]
- Kang, J.J.; Yu, Y.; Chen, L.; Zakeri, K.; Gelblum, D.Y.; McBride, S.M.; Riaz, N.; Tsai, C.J.; Kriplani, A.; Hung, T.K.W.; et al. Consensuses, controversies, and future directions in treatment deintensification for human papillomavirus-associated oropharyngeal cancer. CA A Cancer J. Clin. 2022, 73, 164–197. [Google Scholar] [CrossRef]
- Tan, W.; Bui, R.; Ranasinghe, V.J.; Coblens, O.; Shabani, S. Transoral Robotic Surgery for Oropharyngeal and Hypopharyngeal Squamous Cell Carcinoma. Cureus 2024, 16, e57186. [Google Scholar] [CrossRef]
- Williamson, A.; Moen, C.M.; Slim, M.A.M.; Warner, L.; O’Leary, B.; Paleri, V. Transoral robotic surgery without adjuvant therapy: A systematic review and meta-analysis of the association between surgical margins and local recurrence. Oral Oncol. 2023, 147, 106610. [Google Scholar] [CrossRef]
- O’Sullivan, B.; Huang, S.H.; Siu, L.L.; Waldron, J.; Zhao, H.; Perez-Ordonez, B.; Weinreb, I.; Kim, J.; Ringash, J.; Bayley, A.; et al. Deintensification candidate subgroups in human papillomavirus–related oropharyngeal cancer according to minimal risk of distant metastasis. J. Clin. Oncol. 2013, 31, 543–550. [Google Scholar] [CrossRef]
- Langendijk, J.A.; Doornaert, P.; Verdonck-de Leeuw, I.M.; Leemans, C.R.; Aaronson, N.K.; Slotman, B.J. Impact of late treatment-related toxicity on quality of life among patients with head and neck cancer treated with radiotherapy. J. Clin. Oncol. 2008, 26, 3770–3776. [Google Scholar] [CrossRef]
- Chera, B.S.; Amdur, R.J.; Tepper, J.E.; Tan, X.; Weiss, J.; Grilley-Olson, J.E.; Hayes, D.N.; Zanation, A.; Hackman, T.G.; Patel, S.; et al. Mature results of a prospective study of deintensified chemoradiotherapy for low-risk human papillomavirus-associated oropharyngeal squamous cell carcinoma. Cancer 2018, 124, 2347–2354. [Google Scholar] [CrossRef]
- Chera, B.S.; Amdur, R.J.; Green, R.; Shen, C.; Gupta, G.; Tan, X.; Knowles, M.; Fried, D.; Hayes, N.; Weiss, J.; et al. Phase II trial of de-Intensified chemoradiotherapy for human papillomavirus-associated oropharyngeal squamous cell carcinoma. J. Clin. Oncol. 2019, 37, 2661–2669. [Google Scholar] [CrossRef]
- Adams, A.K.; Wise-Draper, T.M.; Wells, S.I. Human papillomavirus induced transformation in cervical and head and neck cancers. Cancers 2014, 6, 1793–1820. [Google Scholar] [CrossRef] [PubMed]
- Qi, L.; Luo, Q.; Zhang, Y.; Jia, F.; Zhao, Y.; Wang, F. Advances in Toxicological Research of the Anticancer Drug Cisplatin. Chem. Res. Toxicol. 2019, 32, 1469–1486. [Google Scholar] [CrossRef] [PubMed]
- Mirghani, H.; Amen, F.; Blanchard, P.; Moreau, F.; Guigay, J.; Hartl, D.M.; Lacau St Guily, J. Treatment de-escalation in HPV-positive oropharyngeal carcinoma: Ongoing trials, critical issues and perspectives. Int. J. Cancer 2014, 136, 1494–1503. [Google Scholar] [CrossRef] [PubMed]
- Mehanna, H.; Robinson, M.; Hartley, A.; Kong, A.; Foran, B.; Fulton-Lieuw, T.; Dalby, M.; Mistry, P.; Sen, M.; O’Toole, L.; et al. Radiotherapy plus cisplatin or cetuximab in low-risk human papillomavirus-positive oropharyngeal cancer (De-ESCALaTE HPV): An open-label randomised controlled phase 3 trial. Lancet 2019, 393, 51–60. [Google Scholar] [CrossRef]
- Galvis, M.M.; Borges, G.A.; Oliveira, T.B.d.; Toledo, I.P.d.; Castilho, R.M.; Guerra, E.N.S.; Kowalski, L.P.; Squarize, C.H. Immunotherapy improves efficacy and safety of patients with HPV positive and negative head and neck cancer: A systematic review and meta-analysis. Crit. Rev. Oncol. /Hematol. 2020, 150, 102966. [Google Scholar] [CrossRef]
- Shen, X.; Zhao, B. Efficacy of PD-1 or PD-L1 inhibitors and PD-L1 expression status in cancer: Meta-analysis. BMJ 2018, 362, k3529. [Google Scholar] [CrossRef]
- Cohen, E.E.W.; Soulières, D.; Le Tourneau, C.; Dinis, J.; Licitra, L.; Ahn, M.-J.; Soria, A.; Machiels, J.-P.; Mach, N.; Mehra, R.; et al. Pembrolizumab versus methotrexate, docetaxel, or cetuximab for recurrent or metastatic head-and-neck squamous cell carcinoma (KEYNOTE-040): A randomised, open-label, phase 3 study. Lancet 2019, 393, 156–167. [Google Scholar] [CrossRef]
- Shinomiya, H.; Nibu, K.-i. Etiology, diagnosis, treatment, and prevention of human papilloma virus-associated oropharyngeal squamous cell carcinoma. Int. J. Clin. Oncol. 2023, 28, 975–981. [Google Scholar] [CrossRef]
- Whang, S.; Filippova, M.; Duerksen-Hughes, P. Recent Progress in Therapeutic Treatments and Screening Strategies for the Prevention and Treatment of HPV-Associated Head and Neck Cancer. Viruses 2015, 7, 5040–5065. [Google Scholar] [CrossRef]
- Macilwraith, P.; Malsem, E.; Dushyanthen, S. The effectiveness of HPV vaccination on the incidence of oropharyngeal cancers in men: A review. Infect. Agents Cancer 2023, 18, 24. [Google Scholar] [CrossRef]
- Alsharif, M.T.; Alsahafi, E. Assessing the Knowledge of HPV-Associated Oropharyngeal Squamous Cell Carcinoma, HPV Vaccination, and Practice Scope among Saudi Dental Students in the Western Region. Healthcare 2024, 12, 905. [Google Scholar] [CrossRef] [PubMed]
- Lehtinen, T.; Elfström, K.M.; Mäkitie, A.; Nygård, M.; Vänskä, S.; Pawlita, M.; Dillner, J.; Waterboer, T.; Lehtinen, M. Elimination of HPV–associated oropharyngeal cancers in Nordic countries. Prev. Med. 2021, 144, 106445. [Google Scholar] [CrossRef] [PubMed]
- Massarelli, E.; William, W.; Johnson, F.; Kies, M.; Ferrarotto, R.; Guo, M.; Feng, L.; Lee, J.J.; Tran, H.; Kim, Y.U.; et al. Combining Immune Checkpoint Blockade and Tumor-Specific Vaccine for Patients With Incurable Human Papillomavirus 16–Related Cancer. JAMA Oncol. 2019, 5, 67–73. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Rank | Country | Documents | Citations | SCPs 1 | MCPs 2 | MCP Ratio 3 | Rank based on Citations |
|---|---|---|---|---|---|---|---|
| 1 | USA | 1908 | 91,042 | 1427 | 481 | 0.252 | 1 |
| 2 | Germany | 322 | 12,710 | 146 | 176 | 0.547 | 3 |
| 3 | China | 291 | 5260 | 149 | 142 | 0.488 | 10 |
| 4 | UK | 269 | 11,130 | 111 | 158 | 0.587 | 4 |
| 5 | Canada | 254 | 18,372 | 120 | 134 | 0.528 | 2 |
| 6 | Italy | 231 | 6791 | 124 | 107 | 0.463 | 7 |
| 7 | Australia | 190 | 5532 | 103 | 87 | 0.458 | 9 |
| 8 | France | 187 | 9836 | 73 | 114 | 0.61 | 5 |
| 9 | Netherlands | 177 | 9632 | 78 | 99 | 0.559 | 6 |
| 10 | Japan | 166 | 2631 | 121 | 45 | 0.271 | 15 |
| Rank | Institution | Documents | Total Citations | Country | Average Citations per Document |
|---|---|---|---|---|---|
| 1 | Johns Hopkins University | 310 | 36,106 | USA | 116.47 |
| 2 | The University of Texas MD Anderson Cancer Center | 207 | 16,003 | USA | 77.31 |
| 3 | Washington University | 129 | 7226 | USA | 56.02 |
| 4 | Harvard University | 126 | 4615 | USA | 36.63 |
| 5 | University Of Michigan | 107 | 5271 | USA | 49.26 |
| 6 | University of Pittsburgh | 101 | 5103 | USA | 50.52 |
| 7 | Mayo Clinic | 99 | 2867 | USA | 28.96 |
| 8 | Karolinska Institutet | 98 | 3786 | Sweden | 38.63 |
| 9 | German Cancer Consortium (DKTK) | 96 | 5758 | Germany | 59.98 |
| 10 | University of Toronto | 87 | 6716 | Canada | 77.20 |
| Rank | Author | Documents | Citations | H-Index | Affiliation |
|---|---|---|---|---|---|
| 1 | Erich M. Sturgis | 94 | 5317 | 74 | Baylor College of Medicine |
| 2 | Carole Fakhry | 87 | 7139 | 48 | Johns Hopkins University School of Medicine |
| 3 | Tina Dalianis | 59 | 2550 | 49 | Karolinska Institutet |
| 4 | Guojun Li | 59 | 1428 | 39 | University of Texas School of Public Health |
| 5 | James S. Lewis Jr | 57 | 3382 | 54 | Vanderbilt University Medical Center |
| 6 | Robert L. Ferris | 51 | 2366 | 94 | University of Pittsburgh Medical Center |
| 7 | William H. Westra | 51 | 12,779 | 114 | Icahn School of Medicine at Mount Sinai |
| 8 | Brian O’Sullivan | 48 | 4967 | 99 | University of Toronto Faculty of Medicine |
| 9 | Qingyi Wei | 48 | 1278 | 83 | Duke University School of Medicine |
| 10 | Gypsyamber D’Souza | 46 | 5808 | 56 | Johns Hopkins Bloomberg School of Public Health |
| Rank | Journal | Documents | Citations | IF (2022) | CiteScore | Publisher |
|---|---|---|---|---|---|---|
| 1 | Head and Neck | 320 | 7585 | 2.9 | 6.9 | Wiley |
| 2 | Oral Oncology | 283 | 9317 | 4.8 | 8.6 | Elsevier |
| 3 | Cancers | 119 | 1172 | 5.2 | 7.4 | MDPI |
| 4 | Laryngoscope | 118 | 2692 | 2.6 | 5.7 | Wiley |
| 5 | Cancer | 115 | 6419 | 6.2 | 12.2 | Wiley |
| 6 | International Journal of Cancer | 90 | 6838 | 6.4 | 15.2 | Wiley |
| 7 | Otolaryngology-Head and Neck Surgery | 78 | 1293 | 3.4 | 7.2 | Sage |
| 8 | European Archives of Oto-Rhino-Laryngology | 74 | 985 | 2.6 | 5.0 | Springer |
| 9 | International Journal of Radiation oncology Biology Physics | 63 | 2605 | 7.0 | 11.0 | Elsevier |
| 10 | PLOS ONE | 62 | 1329 | 3.7 | 6.0 | PLOS |
| 15 | Journal of Clinical Oncology | 47 | 12,705 | 45.3 | 39.6 | ASCO |
| Rank | Title | Journal | First Author | Total Citations | Year |
|---|---|---|---|---|---|
| 1 | Human Papillomavirus and Survival of Patients with Oropharyngeal Cancer | The New England Journal of Medicine | K. Kian Ang | 4714 | 2010 |
| 2 | Evidence for a Causal Association Between Human Papillomavirus and a Subset of Head and Neck Cancers | Journal of the National Cancer Institute | Maura L. Gillison | 2262 | 2000 |
| 3 | Case–Control Study of Human Papillomavirus and Oropharyngeal Cancer | The New England Journal of Medicine | Gypsyamber D’Souza | 1913 | 2007 |
| 4 | Human Papillomavirus Types in Head and Neck Squamous Cell Carcinomas Worldwide: A Systematic Review | Cancer Epidemiology, Biomarkers & Prevention | Aimee R. Kreimer | 1520 | 2005 |
| 5 | HPV-associated head and neck cancer: a virus-related cancer epidemic | The Lancet Oncology | Shanthi Marur | 1314 | 2010 |
| 6 | Incidence Trends for Human Papillomavirus–Related and –Unrelated Oral Squamous Cell Carcinomas in the United States | Journal of Clinical Oncology | Anil K. Chaturvedi | 1203 | 2008 |
| 7 | Head and Neck Cancers—Major Changes in the American Joint Committee on Cancer Eighth Edition Cancer Staging Manual | CA-A Cancer Journal for Clinicians | William M. Lydiatt | 976 | 2017 |
| 8 | Worldwide Trends in Incidence Rates for Oral Cavity and Oropharyngeal Cancers | Journal of Clinical Oncology | Anil K. Chaturvedi | 916 | 2013 |
| 9 | The molecular landscape of head and neck cancer | Nature Reviews Cancer | C. René Leemans | 784 | 2018 |
| 10 | Epidemiology of Human Papillomavirus–Positive Head and Neck Squamous Cell Carcinoma | Journal of Clinical Oncology | Maura L. Gillison | 769 | 2015 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cui, Y.; Li, W.; Li, B. A Bibliometric Analysis of HPV-Positive Oropharyngeal Squamous Cell Carcinoma from 2000 to 2023. Pathogens 2025, 14, 289. https://doi.org/10.3390/pathogens14030289
Cui Y, Li W, Li B. A Bibliometric Analysis of HPV-Positive Oropharyngeal Squamous Cell Carcinoma from 2000 to 2023. Pathogens. 2025; 14(3):289. https://doi.org/10.3390/pathogens14030289
Chicago/Turabian StyleCui, Yingying, Wei Li, and Binbin Li. 2025. "A Bibliometric Analysis of HPV-Positive Oropharyngeal Squamous Cell Carcinoma from 2000 to 2023" Pathogens 14, no. 3: 289. https://doi.org/10.3390/pathogens14030289
APA StyleCui, Y., Li, W., & Li, B. (2025). A Bibliometric Analysis of HPV-Positive Oropharyngeal Squamous Cell Carcinoma from 2000 to 2023. Pathogens, 14(3), 289. https://doi.org/10.3390/pathogens14030289