
Sex, Age, and Previous Herpes Zoster Infection Role on Adverse Events Following Immunization with Adjuvanted Recombinant Vaccine
 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Demographic and AEFI Data Collection
2.3. Statistical Analysis
3. Results
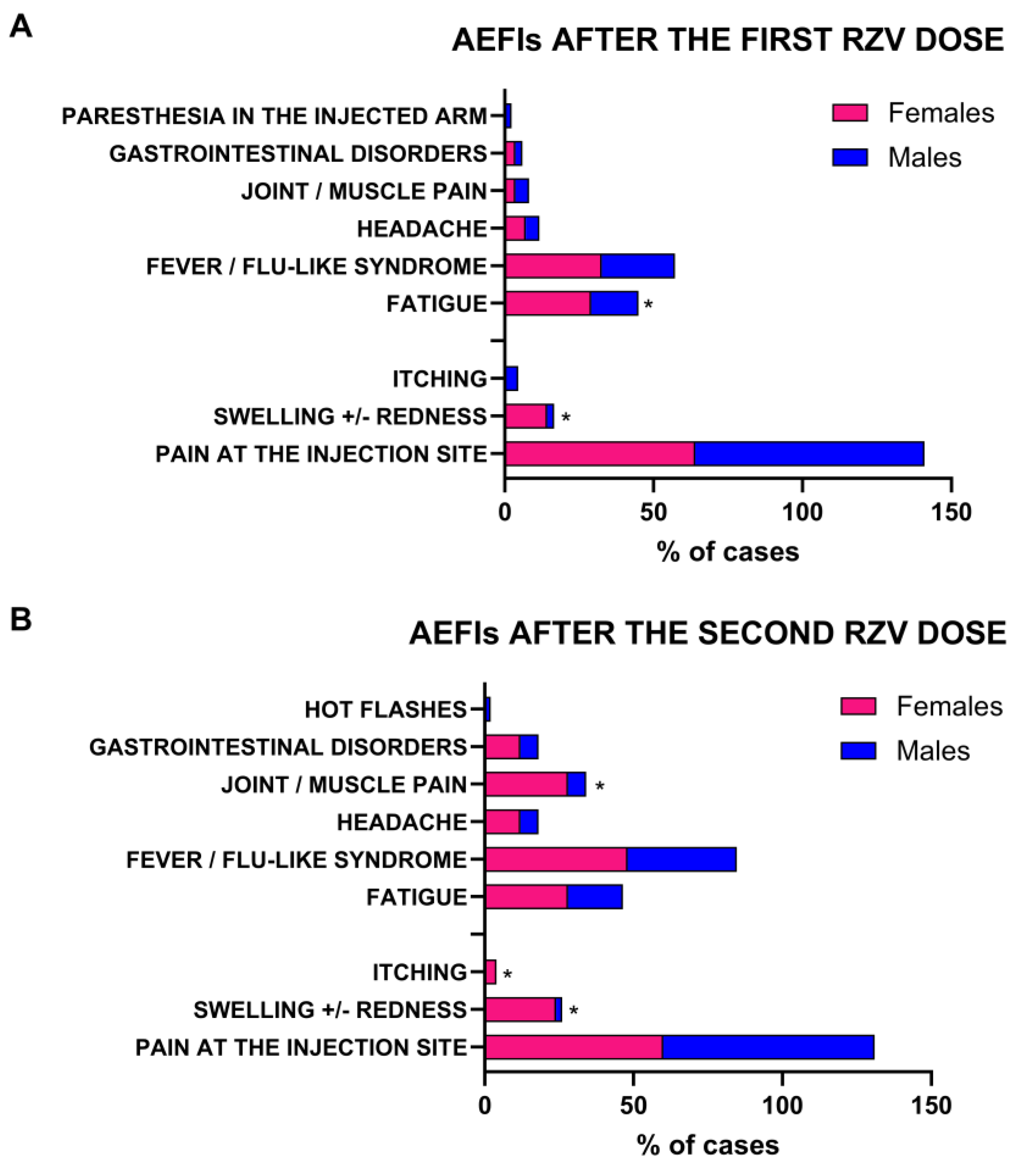
3.1. Females More Frequently Report Mild/Moderate AEFIs After First RZV Dose
3.2. Young Adults More Frequently Report Local and Systemic AEFIs
3.3. Previous AEFI Occurrence Does Not Increase Severity and Incidence of Adverse Events After Second RZV Dose
3.4. Impact of Previous Herpes Zoster Infection on Prevalence and Duration of AEFI
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Costanzo, V.; Roviello, G.N. The Potential Role of Vaccines in Preventing Antimicrobial Resistance (AMR): An Update and Future Perspectives. Vaccines 2023, 11, 333. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Rappuoli, R.; Pizza, M.; Del Giudice, G.; De Gregorio, E. Vaccines, new opportunities for a new society. Proc. Natl. Acad. Sci. USA 2014, 111, 12288–12293. [Google Scholar] [CrossRef] [PubMed]
- Kwong, J.C.; Maaten, S.; Upshur, R.E.G.; Patrick, D.M.; Marra, F. The Effect of Universal Influenza Immunization on Antibiotic Prescriptions: An Ecological Study. Clin. Infect. Dis. 2009, 49, 750–756. [Google Scholar] [CrossRef]
- Ozgur, S.K.; Beyazova, U.; Kemaloglu, Y.K.; Maral, I.; Sahin, F.; Camurdan, A.D.; Kizil, Y.; Dinc, E.; Tuzun, H. Effectiveness of Inactivated Influenza Vaccine for Prevention of Otitis Media in Children. Pediatr. Infect. Dis. J. 2006, 25, 401–404. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.iss.it/vaccini/-/asset_publisher/EqhqPGnWTDJo/content/differenze-di-genere-in-risposta-alle-vaccinazioni (accessed on 19 November 2024).
- Poland, G.A.; Ovsyannikova, I.G.; Jacobson, R.M. Vaccine immunogenetics: Bedside to bench to population. Vaccine 2008, 26, 6183–6188. [Google Scholar] [CrossRef] [PubMed]
- Poland, G.A.; Ovsyannikova, I.G.; Jacobson, R.M. Application of pharmacogenomics to vaccines. Pharmacogenomics 2009, 10, 837–852. [Google Scholar] [CrossRef] [PubMed]
- Klein, S.L.; Jedlicka, A.; Pekosz, A. The Xs and Y of immune responses to viral vaccines. Lancet Infect. Dis. 2010, 10, 338–349. [Google Scholar] [CrossRef] [PubMed]
- Ruggieri, A.; Anticoli, S.; D’Ambrosio, A.; Giordani, L.; Viora, M. The influence of sex and gender on immunity, infection and vaccination. Ann. Dell’istituto Super. Sanita 2016, 52, 198–204. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.aifa.gov.it/en/-/aifa-pubblica-il-rapporto-vaccini (accessed on 2 January 2025).
- Global Manual on Surveillance of Adverse Events Following Immunization. Available online: https://www.who.int/publications/i/item/9789241507769 (accessed on 24 November 2024).
- Sciarra, F.; Campolo, F.; Franceschini, E.; Carlomagno, F.; Venneri, M.A. Gender-Specific Impact of Sex Hormones on the Immune System. Int. J. Mol. Sci. 2023, 24, 6302. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Mittal, S.; Rawat, C.; Gupta, A.; Solanki, H.K.; Singh, R.K. Adverse Events Following Immunization Among Children Under Two Years of Age: A Prospective Observational Study from North India. Cureus 2023, 15, e38356. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Klein, S.L. Immune cells have sex and so should journal articles. Endocrinology 2012, 153, 2544–2550. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Roved, J.; Westerdahl, H.; Hasselquist, D. Sex differences in immune responses: Hormonal effects, antagonistic selection, and evolutionary consequences. Horm. Behav. 2017, 88, 95–105. [Google Scholar] [CrossRef] [PubMed]
- Weinberg, A.; Kroehl, M.E.; Johnson, M.J.; Hammes, A.; Reinhold, D.; Lang, N.; Levin, M.J. Comparative Immune Responses to Licensed Herpes Zoster Vaccines. J. Infect. Dis. 2018, 218 (Suppl. S2), S81–S87. [Google Scholar] [CrossRef]
- Hou, Y.; Chen, M.; Bian, Y.; Hu, Y.; Chuan, J.; Zhong, L.; Zhu, Y.; Tong, R. Insights into vaccines for elderly individuals: From the impacts of immunosenescence to delivery strategies. Npj Vaccines 2024, 9, 77. [Google Scholar] [CrossRef] [PubMed]
- Nair, P.A.; Patel, B.C. Herpes Zoster. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar] [PubMed]
- Johnson, R.W. Herpes zoster and postherpetic neuralgia. Expert Rev. Vaccines 2010, 9 (Suppl. S3), 21–26. [Google Scholar] [CrossRef] [PubMed]
- Loubet, P.; Roustand, L.; Schmidt, A.; Jacquemet, P.; de Wazières, B.; Vabre, C.; Nishimwe, M.; Faure, E. Clinical profile of herpes zoster-related hospitalizations and complications: A French population-based database study. J. Infect. 2024, 89, 106330. [Google Scholar] [CrossRef] [PubMed]
- Giorda, C.B.; Picariello, R.; Tartaglino, B.; Nada, E.; Romeo, F.; Costa, G.; Gnavi, R. Hospitalisation for herpes zoster in people with and without diabetes: A 10-year-observational study. Diabetes Res. Clin. Pract. 2024, 210, 111603. [Google Scholar] [CrossRef] [PubMed]
- Costantino, M.; Giudice, V.; Moccia, G.; Longanella, W.; Caruccio, S.; Tremiterra, G.; Sinopoli, P.; Benvenuto, D.; Serio, B.; Malatesta, F.; et al. Safety of Adjuvanted Recombinant Herpes Zoster Virus Vaccination in Fragile Populations: An Observational Real-Life Study. Vaccines 2024, 12, 990. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Adverse Event Following Immunization. Available online: https://www.who.int/groups/global-advisory-committee-on-vaccine-safety/topics/aefi/serious-aefi (accessed on 30 November 2024).
- Hartwig, S.; Siegel, J.; Schneider, P.J. Preventability and severity assessment in reporting adverse drug reactions. Am. J. Hosp. Pharm. 1992, 49, 2229–2232. [Google Scholar] [CrossRef]
- Available online: https://www.who.int/health-topics/vaccines-and-immunization?utm_#tab=tab_1 (accessed on 3 January 2025).
- Depledge, D.P.; Sadaoka, T.; Ouwendijk, W.J.D. Molecular Aspects of Varicella-Zoster Virus Latency. Viruses 2018, 10, 349. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Bricout, H.; Haugh, M.; Olatunde, O.; Prieto, R.G. Herpes zoster-associated mortality in Europe: A systematic review. BMC Public Health 2015, 15, 466. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Schutzer-Weissmann, J.; Farquhar-Smith, P. Post-herpetic neuralgia—A review of current management and future directions. Expert Opin. Pharmacother. 2017, 18, 1739–1750. [Google Scholar] [CrossRef] [PubMed]
- Schmader, K. Herpes zoster in older adults. Clin. Infect. Dis. 2001, 32, 1481–1486. [Google Scholar] [CrossRef] [PubMed]
- Pinchinat, S.; Cebrián-Cuenca, A.M.; Bricout, H.; Johnson, R.W. Similar herpes zoster incidence across Europe: Results from a systematic literature review. BMC Infect. Dis. 2013, 13, 170. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Mullane, K.M.; Morrison, V.A.; Camacho, L.H.; Arvin, A.; McNeil, S.A.; Durrand, J.; Campbell, B.; Su, S.C.; Chan, I.S.F.; Parrino, J.; et al. Safety and efficacy of inactivated varicella zoster virus vaccine in immunocompromised patients with malignancies: A two-arm, randomised, double-blind, phase 3 trial. Lancet Infect. Dis. 2019, 19, 1001–1012. [Google Scholar] [CrossRef]
- Stefanizzi, P.; Moscara, L.; Palmieri, C.; Martinelli, A.; Di Lorenzo, A.; Venerito, V.; Germinario, C.A.; Tafuri, S. Safety profile of recombinant adjuvanted anti-herpes zoster vaccine (RZV) in high-risk groups: Data from active surveillance program. Puglia (Italy), 2021–2023. Vaccine 2024, 42, 2966–2974. [Google Scholar] [CrossRef] [PubMed]
- Zeevaert, R.; Thiry, N.; Maertens de Noordhout, C.; Roberfroid, D. Efficacy and safety of the recombinant zoster vaccine: A systematic review and meta-analysis. Vaccine X 2023, 15, 100397. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.cdc.gov/vaccine-safety-systems/monitoring/covid-19.html (accessed on 3 January 2025).
- Su, J.R.; Moro, P.L.; Ng, C.S.; Lewis, P.W.; Said, M.A.; Cano, M.V. Anaphylaxis after vaccination reported to the Vaccine Adverse Event Reporting System, 1990–2016. J. Allergy Clin. Immunol. 2019, 143, 1465–1473. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Flanagan, K.L.; Fink, A.L.; Plebanski, M.; Klein, S.L. Sex and gender differences in the outcomes of vaccination over the life course. Annu. Rev. Cell Dev. Biol. 2017, 33, 577–599. [Google Scholar] [CrossRef] [PubMed]
- Kiely, M.; Tadount, F.; Lo, E.; Sadarangani, M.; Wei, S.Q.; Rafferty, E.; Quach, C.; MacDonald, S.E. Sex differences in adverse events following seasonal influenza vaccines: A meta-analysis of randomized controlled trials. J. Epidemiol Community Health 2023, 77, 791–801. [Google Scholar] [CrossRef] [PubMed]
- Jensen, A.; Stromme, M.; Moyassari, S.; Chadha, A.S.; Tartaglia, M.C.; Szoeke, C.; Ferretti, M.T. COVID-19 vaccines: Considering sex differences in efficacy and safety. Contemp. Clin. Trials 2022, 115, 106700. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Sampath, V.; Rabinowitz, G.; Shah, M.; Jain, S.; Diamant, Z.; Jesenak, M.; Rabin, R.; Vieths, S.; Agache, I.; Akdis, M.; et al. Vaccines and allergic reactions: The past, the current COVID-19 pandemic, and future perspectives. Allergy 2021, 76, 1640–1660. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Halsey, N.A.; Griffioen, M.; Dreskin, S.C.; Dekker, C.L.; Wood, R.; Sharma, D.; Jones, J.F.; LaRussa, P.S.; Garner, J.; Berger, M.; et al. Immediate hypersensitivity reactions following monovalent 2009 pandemic influenza A (H1N1) vaccines: Reports to VAERS. Vaccine 2013, 31, 6107–6112. [Google Scholar] [CrossRef]
- Tran, V.N.; Nguyen, H.A.; Le, T.T.A.; Truong, T.T.; Nguyen, P.T.; Nguyen, T.T.H. Factors influencing adverse events following immunization with AZD1222 in Vietnamese adults during first half of 2021. Vaccine 2021, 39, 6485–6491. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Rosato, E.; Sciarra, F.; Anastasiadou, E.; Lenzi, A.; Venneri, M.A. Revisiting the physiological role of androgens in women. Expert Rev. Endocrinol. Metab. 2022, 17, 547–561. [Google Scholar] [CrossRef]
- Sciarra, F.; Franceschini, E.; Campolo, F.; Gianfrilli, D.; Pallotti, F.; Paoli, D.; Isidori, A.M.; Venneri, M.A. Disruption of Circadian Rhythms: A Crucial Factor in the Etiology of Infertility. Int. J. Mol. Sci. 2020, 21, 3943. [Google Scholar] [CrossRef]
- Calabrò, A.; Accardi, G.; Aiello, A.; Caruso, C.; Candore, G. Sex and gender affect immune aging. Front. Aging 2023, 4, 1272118. [Google Scholar] [CrossRef] [PubMed]
- Engler, R.J.; Nelson, M.R.; Klote, M.M.; VanRaden, M.J.; Huang, C.Y.; Cox, N.J.; Klimov, A.; Keitel, W.A.; Nichol, K.L.; Carr, W.W.; et al. Half- vs full-dose trivalent inactivated influenza vaccine (2004–2005): Age, dose, and sex effects on immune responses. Arch. Intern. Med. 2008, 168, 2405–2414. [Google Scholar] [CrossRef] [PubMed]
- Spini, A.; Giudice, V.; Brancaleone, V.; Morgese, M.G.; De Francia, S.; Filippelli, A.; Ruggieri, A.; Ziche, M.; Ortona, E.; Cignarella, A.; et al. Sex-tailored pharmacology and COVID-19: Next steps towards appropriateness and health equity. Pharmacol. Res. 2021, 173, 105848. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Hesse, E.M. Postlicensure Safety Surveillance of Recombinant Zoster Vaccine (Shingrix)—United States, October 2017–June 2018. MMWR. Morb. Mortal. Wkly. Rep. 2019, 68, 91–94. [Google Scholar] [CrossRef] [PubMed]
- Venerito, V.; Stefanizzi, P.; Cantarini, L.; Lavista, M.; Galeone, M.G.; Di Lorenzo, A.; Iannone, F.; Tafuri, S.; Lopalco, G. Immunogenicity and Safety of Adjuvanted Recombinant Zoster Vaccine in Rheumatoid Arthritis Patients on Anti-Cellular Biologic Agents or JAK Inhibitors: A Prospective Observational Study. Int. J. Mol. Sci. 2023, 24, 6967. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Jackson, L.A.; Gurtman, A.; van Cleeff, M.; Jansen, K.U.; Jayawardene, D.; Devlin, C.; Scott, D.A.; Emini, E.A.; Gruber, W.C.; Schmoele-Thoma, B. Immunogenicity and safety of a 13-valent pneumococcal conjugate vaccine compared to a 23-valent pneumococcal polysaccharide vaccine in pneumococcal vaccine-naive adults. Vaccine 2013, 31, 3577–3584. [Google Scholar] [CrossRef] [PubMed]
- Xiong, X.; Yuan, J.; Li, M.; Jiang, B.; Lu, Z.K. Age and Gender Disparities in Adverse Events Following COVID-19 Vaccination: Real-World Evidence Based on Big Data for Risk Management. Front. Med. 2021, 8, 700014. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]

{kind=link}
| Characteristics | Total Cohort |
|---|---|
| N = 174 | |
| Age, years | |
| Mean ± SD | 57 ± 11.8 |
| Median [range] | 57 [28–84] |
| M/F | 123 (71%)/51 (29%) |
| Comorbidities, n (%) | |
| Kidney transplant | 126 (72) |
| Liver transplant | 14 (8.0) |
| HIV infection | 13 (7.5) |
| Ulcerative colitis | 4 (2.3) |
| Dialysis | 4 (2.3) |
| Obesity | 2 (1.1) |
| Autoimmune rheumatic diseases | 3 (1.7) |
| Type 2 diabetes | 1 (1) |
| Hematological malignancies | 2 (1.1) |
| Geriatric frailty (age ≥ 65 years), n (%) | 5 (3.0) |
| Characteristics | Females | Males | p Value |
|---|---|---|---|
| N = 51 | N = 123 | ||
| Age, years | 1.0 | ||
| Mean ± SD | 57.0 ± 12.5 | 56.9 ± 11.5 | |
| Median [range] | 58 [28–78] | 57 [33–84] | |
| Comorbidities, n (%) | |||
| Kidney transplant | 39 (76) | 87 (70.7) | 0.4 |
| Liver transplant | 3 (6) | 11 (9) | 0.3 |
| HIV infection | 0 (0) | 13 (10.6) | 0.02 |
| Ulcerative colitis | 3 (6) | 1 (0.8) | 0.04 |
| Dialysis | 2 (4) | 2 (1.6) | 0.4 |
| Obesity | 1 (2) | 1 (0.8) | 0.5 |
| Autoimmune rheumatic diseases | 2 (4) | 1 (0.8) | 0.2 |
| Type 2 diabetes | 1 (2) | 0 (0) | 0.1 |
| Hematological malignancies | 0 (0) | 2 (1.6) | 0.4 |
| Geriatric frailty (Age ≥ 65 years) | 0 (0) | 5 (4.1) | 0.1 |
| AEFIs after the first dose, n (%) | 28 (55) | 44 (35.8) | 0.02 |
| Total duration (h), mean ± SD | 75 ± 74.8 | 66 ± 114.8 | 0.7 |
| Local symptom duration (h), mean ± SD (n) | 93 ± 81.1 (20) | 76 ± 126.7 (35) | 0.6 |
| Systemic symptom duration (h), mean ± SD (n) | 62 ± 91.7 (14) | 50 ± 66.5 (19) | 0.7 |
| Medications, n (%) | 6 (21.4) | 4 (9.1) | 0.1 |
| AEFIs after the second dose, n (%) | 28 (55) | 50 (41) | 0.09 |
| Total duration (h), mean ± SD | 51 ± 40.4 | 48 ± 42.7 | 0.8 |
| Local symptom duration (h), mean ± SD (n) | 60 ± 43.8 (19) | 47 ± 35.7 (37) | 0.2 |
| Systemic symptom duration (h), mean ± SD (n) | 41 ± 35.6 (19) | 45 ± 47.4 (26) | 0.6 |
| Medications, n (%) | 8 (29) | 13 (26) | 0.8 |
| Characteristics | Young Adults | Adults | Older Adults | p Value |
|---|---|---|---|---|
| 28–39 yo | 40–65 yo | >65 yo | ||
| N = 13 | N = 115 | N = 46 | ||
| AEFIs after the first dose, n (%) | 7 (54) | 51 (44) | 14 (30) | >0.05 |
| Total duration (h), mean ± SD | 84 ± 46.5 | 67 ± 111 | 70 ± 84.4 | |
| Local symptom duration (h), mean ± SD (n) | 88 ± 49.6 (6) | 82 ± 125 (38) | 78 ± 92.9 (11) | |
| Systemic symptom duration (h), mean ± SD (n) | 84 ± 31.7 (3) | 42 ± 69 (25) | 95 ± 106 (6) | |
| Medications, n (%) | 1 (14) | 8 (16) | 1 (7) | |
| Local AEFIs, n (%) | 7 (54) | 40 (35) | 12 (26) | 0.11 |
| Pain at the injection site | 4 (57) | 38 (75) | 10 (71) | 0.35 |
| Swelling +/− redness | 3 (23) | 1 (1) | 1 (2) | 0.004 |
| Itching | 0 (0) | 1 (1) | 1 (2) | 0.56 |
| Systemic AEFIs, n (%) | 5 (38) | 31 (27) | 8 (17) | 0.21 |
| Fever/Flu-like syndrome | 2 (29) | 15 (30) | 2 (14) | 0.23 |
| Joint/muscle pain | 1 (14) | 1 (2) | 1 (7) | 0.13 |
| Fatigue | 1 (14) | 11 (22) | 3 (21) | 0.91 |
| Headache | 1 (14) | 2 (4) | 1 (7) | 0.32 |
| Gastrointestinal disorders | 0 (0) | 2 (4) | 0 (0) | 1.0 |
| Paresthesia in the injected arm | 0 (0) | 0 (0) | 1 (7) | 0.34 |
| AEFIs after the second dose, n (%) | 9 (69) | 52 (45) | 17 (37) | 0.04 # |
| Total duration (h), mean ± SD | 61 ± 48.7 | 43 ± 34.1 | 60 ± 55.7 | all |
| Local symptom duration (h), mean ± SD (n) | 70 ± 33.5 (7) | 46 ± 38.3 (37) | 48 ± 19.6 (10) | p > 0.05 |
| Systemic symptom duration (h), mean ± SD (n) | 47 ± 60.7 (6) | 39 ± 29.8 (29) | 54 ± 61.5 (10) | |
| Medications, n (%) | 3 (33) | 17 (33) | 2 (12) | |
| Local AEFIs, n (%) | 7 (54) | 42 (37) | 12 (26) | 0.11 |
| Pain at the injection site | 6 (67) | 36 (69) | 11 (65) | 0.27 |
| Swelling +/− redness | 1 (11) | 5 (10) | 1 (6) | 0.43 |
| Itching | 0 (0) | 1 (2) | 0 (0) | 1.0 |
| Edema | 1 (11) | 0 (0) | 0 (0) | 0.07 |
| Systemic AEFIs, n (%) | 9 (69) | 48 (42) | 17 (37) | 0.04 # |
| Fever/Flu-like syndrome | 5 (55) | 22 (42) | 5 (30) | 0.04 |
| Joint/muscle pain | 0 (0) | 8 (15) | 3 (18) | 1.0 |
| Fatigue | 1 (11) | 9 (17) | 7 (41) | 0.3 |
| Headache | 1 (11) | 5 (10) | 0 (0) | 0.2 |
| Gastrointestinal disorders | 1 (11) | 4 (8) | 1 (6) | 0.6 |
| Hot flashes | 0 (0) | 0 (0) | 1 (6) | 0.34 |
| Characteristics | I/II AEFI | II AEFI | p Value |
|---|---|---|---|
| N = 49 | N = 31 | ||
| Age, years | 0.5 | ||
| Mean ± SD | 56 ± 12.1 | 54 ± 13.3 | |
| Median [range] | 56 [28–81] | 50 [33–82] | |
| M/F | 18 (37)/31 (63) | 11 (35)/20 (65) | 0.9 |
| Local AEFIs, n (%) | 34 (69) | 27 (87) | 0.07 |
| Pain at the injection site | 30 (61) | 24 (77) | 0.1 |
| Swelling +/− redness | 4 (8) | 2 (6) | 1.0 |
| Itching | 0 (0) | 1 (3) | 0.2 |
| Systemic AEFIs, n (%) | 47 (96) | 26 (84) | 0.06 |
| Fever/Flu-like syndrome | 20 (41) | 12 (38) | 1.0 |
| Joint/muscle pain | 7 (14) | 4 (13) | 1.0 |
| Fatigue | 13 (27) | 4 (13) | 0.1 |
| Headache | 4 (8) | 2 (6) | 0.8 |
| Gastrointestinal disorders | 3 (6) | 3 (10) | 0.6 |
| Hot flashes | 0 (0) | 1 (3) | 0.2 |
| Total duration (h), mean ± SD | 44 ± 35.2 | 57 ± 48.7 | 0.2 |
| Local symptom duration (h), mean ± SD (n) | 47 ± 35.4 (32) | 56 ± 41.5 (26) | 0.4 |
| Systemic symptom duration (h), mean ± SD (n) | 38 ± 32.7 (30) | 53 ± 57.4 (15) | 0.3 |
| Medications, n (%) | 17 (35) | 5 (16) | 0.07 |
| Characteristics | No Previous HZ | Previous HZ | p Value |
|---|---|---|---|
| N = 136 | N = 38 | ||
| AEFIs after the first dose, n (%) | 55 (40) | 17 (45) | 0.6 |
| Total duration (h), mean ± SD | 78 ± 111.9 | 42 ± 38.1 | 0.2 |
| Local symptom duration (h), mean ± SD (n) | 90 ± 122.1 (44) | 52 ± 43.5 (11) | 0.3 |
| Systemic symptom duration (h), mean ± SD (n) | 66 ± 85.6 (25) | 26 ± 18.6 (9) | 0.2 |
| Medications, n (%) | 7 (13) | 3 (18) | 0.6 |
| Local AEFIs, n (%) | 45 (82) | 13 (76) | 0.6 |
| Pain at the injection site | 40 (73) | 11 (65) | 0.5 |
| Swelling +/− redness | 4 (8) | 1 (6) | 1.0 |
| Itching | 1 (2) | 1 (6) | 0.4 |
| Systemic AEFIs, n (%) | 31 (56) | 14 (82) | 0.05 |
| Fever/Flu-like syndrome | 14 (26) | 6 (25) | 0.4 |
| Joint/muscle pain | 2 (4) | 1 (6) | 0.5 |
| Fatigue | 11 (20) | 4 (24) | 0.8 |
| Headache | 2 (4) | 2 (12) | 0.2 |
| Gastrointestinal disorders | 1 (2) | 1 (6) | 0.4 |
| Paresthesia in the injected arm | 1 (2) | 0 (0) | 0.6 |
| AEFIs after the second dose, n (%) | 52 (38) | 26 (68) | 0.001 |
| Total duration (h), mean ± SD | 43 ± 34.8 | 61 ± 51.1 | 0.07 |
| Local symptom duration (h), mean ± SD (n) | 46 ± 34.0 (36) | 62 ± 44.9 (20) | 0.1 |
| Systemic symptom duration (h), mean ± SD (n) | 42 ± 42.1 (28) | 45 ± 44.1 (17) | 0.8 |
| Medications, n (%) | 16 (31) | 6 (23) | 0.5 |
| Local AEFIs, n (%) | 38 (73) | 23 (88) | 0.1 |
| Pain at the injection site | 33 (63) | 20 (77) | 0.2 |
| Swelling +/− Redness | 5 (10) | 2 (8) | 0.6 |
| Itching | 0 (0) | 1 (4) | 0.2 |
| Systemic AEFIs, n (%) | 48 (92) | 26 (100) | 0.1 |
| Fever/Flu-like syndrome | 21 (40) | 12 (46) | 1.0 |
| Joint/muscle pain | 7 (14) | 4 (16) | 0.3 |
| Fatigue | 12 (23) | 5 (19) | 0.5 |
| Headache | 4 (8) | 2 (8) | 0.7 |
| Gastrointestinal disorders | 4 (8) | 2 (8) | 1.0 |
| Hot flashes | 0 (0) | 1 (4) | 0.2 |
| Dependent Variable = AEFI After First Dose | ||||
| Variable | Odds Ratio | SE | 95%CI | p Value |
| Intercept | 1.192 | 0.8156 | −1.428 to 1.785 | 0.8299 |
| Age (years) | 0.983 | 0.01435 | −0.0456 to 0.011 | 0.2381 |
| Sex [F] | 2.163 | 0.3784 | 0.0334 to 1.524 | 0.0415 |
| Comorbidities [Others] | 4.375 | 0.6313 | 0.3014 to 2.835 | 0.0194 |
| Comorbidities [HIV infection] | 1.530 | 0.6096 | −0.8093 to 1.625 | 0.4851 |
| Comorbidities [Age > 65 years] | 0.716 | 1.170 | −3.361 to 1.703 | 0.7754 |
| History of HZ infection | 0.844 | 0.5211 | −1.224 to 0.8369 | 0.7454 |
| Number of previous HZ infections | 1.881 | 0.5231 | −0.3712 to 1.713 | 0.2273 |
| Dependent Variable = AEFI After Second Dose | ||||
| Variable | Odds Ratio | SE | 95%CI | p Value |
| Intercept | 2.022 | 0.9145 | −1.082 to 2.522 | 0.4412 |
| Age (years) | 0.966 | 0.0161 | −0.0673 to −0.004 | 0.0300 |
| Sex [F] | 1.399 | 0.4239 | −0.5017 to 1.169 | 0.4279 |
| Comorbidities [Others] | 0.866 | 0.6381 | −1.419 to 1.108 | 0.8223 |
| Comorbidities [HIV infection] | 1.898 | 0.7087 | −0.7481 to 2.073 | 0.3660 |
| Comorbidities [Age > 65 years] | 0.935 | 1.247 | −3.190 to 2.119 | 0.9570 |
| History of HZ infection | 3.304 | 0.5755 | 0.0873 to 2.364 | 0.0378 |
| Number of previous HZ infections | 1.501 | 0.6167 | −0.7537 to 1.705 | 0.5100 |
| AEFI after first dose | 4.302 | 0.4317 | 0.6228 to 2.323 | 0.0007 |
| Systemic AEFI after first dose (h) | 1.015 | 0.0103 | 0.001 to 0.042 | 0.1354 |
| Local AEFI after first dose (h) | 0.998 | 0.0033 | −0.011 to 0.003 | 0.4735 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Costantino, M.; Giudice, V.; Moccia, G.; Ragozzino, M.; Calabrese, S.; Caiazzo, F.; Beatrice, M.; Longanella, W.; Caruccio, S.; Iacuzzo, C.; et al. Sex, Age, and Previous Herpes Zoster Infection Role on Adverse Events Following Immunization with Adjuvanted Recombinant Vaccine. Pathogens 2025, 14, 195. https://doi.org/10.3390/pathogens14020195
Costantino M, Giudice V, Moccia G, Ragozzino M, Calabrese S, Caiazzo F, Beatrice M, Longanella W, Caruccio S, Iacuzzo C, et al. Sex, Age, and Previous Herpes Zoster Infection Role on Adverse Events Following Immunization with Adjuvanted Recombinant Vaccine. Pathogens. 2025; 14(2):195. https://doi.org/10.3390/pathogens14020195
Chicago/Turabian StyleCostantino, Maria, Valentina Giudice, Giuseppina Moccia, Monica Ragozzino, Salvatore Calabrese, Francesco Caiazzo, Massimo Beatrice, Walter Longanella, Simona Caruccio, Candida Iacuzzo, and et al. 2025. "Sex, Age, and Previous Herpes Zoster Infection Role on Adverse Events Following Immunization with Adjuvanted Recombinant Vaccine" Pathogens 14, no. 2: 195. https://doi.org/10.3390/pathogens14020195
APA StyleCostantino, M., Giudice, V., Moccia, G., Ragozzino, M., Calabrese, S., Caiazzo, F., Beatrice, M., Longanella, W., Caruccio, S., Iacuzzo, C., Giugliano, C., Marongiu, M. B., Genovese, G., Serio, B., Vozzella, E. A., Filippelli, A., & De Caro, F. (2025). Sex, Age, and Previous Herpes Zoster Infection Role on Adverse Events Following Immunization with Adjuvanted Recombinant Vaccine. Pathogens, 14(2), 195. https://doi.org/10.3390/pathogens14020195