
Force of Infection (FOI) and Multiplicity of Infection (MOI) in Plasmodium falciparum Infected Children Aged 1.5–12 Years Living in the Malaria Endemic Area of Banfora, Burkina Faso

 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
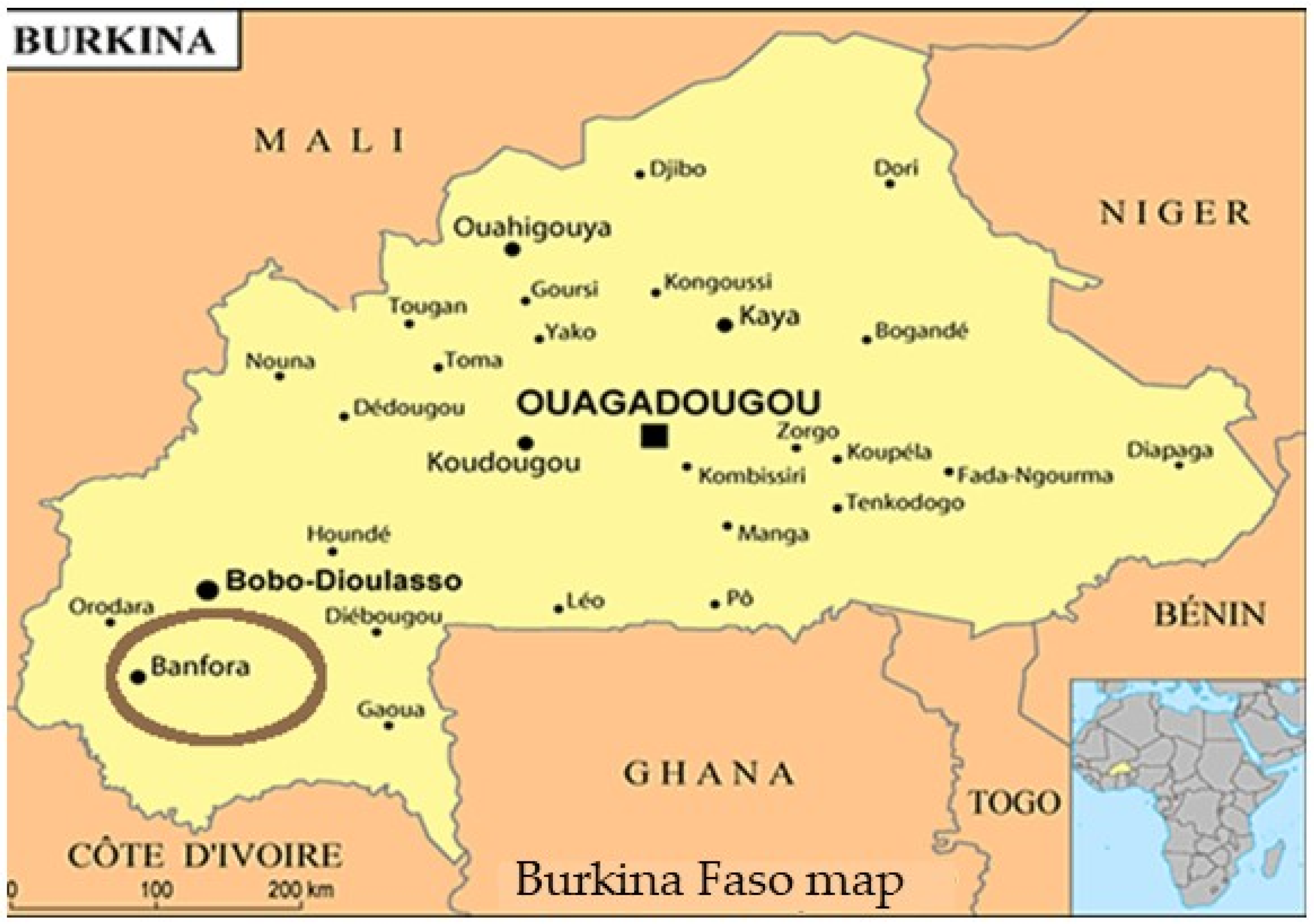
2.1. Study Site
2.2. Study Population, Design and Period
2.3. Sample Collection
2.4. Malaria Parasites Density by Microscopy
2.5. DNA Extraction by Methanol Method
2.6. Molecular Analysis
2.7. Data Management and Statistical Analysis
3. Results
3.1. Baseline Characteristics of Participants
3.2. Incidence of P. falciparum Infection by PCR during the Study
3.3. FOI and MOI in Study Participants
3.4. Risks Factors of Clinical Episode
3.5. Predictive Factors of MOI and FOI
3.5.1. Predictive Factors of MOI
3.5.2. Predictive Factors of New Clones’ Acquisition (FOI)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO (World Health Organization). World Malaria Report. 2023. Available online: https://www.who.int/teams/global-malaria-programme/reports/world-malaria-report-2023 (accessed on 12 December 2023).
- EIPBF, Enquête sur les Indicateurs du Paludisme. 2017–2018. Available online: https://dhsprogram.com/pubs/pdf/MIS32/MIS32.pdf (accessed on 12 December 2023).
- WHO (World Health Organization). World Malaria Report 2011. Available online: https://www.who.int/publications/i/item/9789241564403 (accessed on 12 December 2023).
- Sermé, L.; Bicaba, A.; Ly, A.; Bila, A.; Druetz, T.; Haddad, S. Comprendre le Succès de L’implantation et L’expansion de la Chimioprophylaxie Saisonnière du Paludisme au Burkina Faso. 2018. IDRC Research Results/Innovating for Maternal and Child Health in Africa (IMCHA). Available online: http://hdl.handle.net/10625/57545 (accessed on 12 December 2023).
- Sakihama, N.; Nakamura, M.; Palanca, A.A.; Argubano, R.A.; Realon, E.P.; Larracas, A.L.; Espina, R.L.; Tanabe, K. Allelic diversity in the merozoite surface protein 1 gene of Plasmodium falciparum on Palawan Island, the Philippines. Parasitol. Int. 2007, 56, 185–194. [Google Scholar] [CrossRef]
- Sondo, P. Etude de la Relation Entre le Polymorphisme Génétique de Plasmodium falciparum et les Signes du Paludisme à Nanoro, Burkina Faso 2014. Available online: https://beep.ird.fr/collect/upb/index/assoc/INSSA-2014-SON-ETU/INSSA-2014-SON-ETU.pdf (accessed on 12 December 2023).
- Eisen, D.; Billman-Jacobe, H.; Marshall, V.F.; Fryauff, D.; Coppel, R.L. Temporal Variation of the Merozoite Surface Protein-2 Gene of Plasmodium falciparum. Infect. Immun. 1998, 66, 239–246. [Google Scholar] [CrossRef] [PubMed]
- Kemp, D.J.; Cowman, A.F.; Walliker, D. Genetic Diversity in Plasmodium falciparum. Adv. Parasitol. 1990, 29, 75–149. [Google Scholar] [CrossRef] [PubMed]
- Viriyakosol, S.; Siripoon, N.; Petcharapirat, C.; Petcharapirat, P.; Jarra, W.; Thaithong, S.; Brown, K.N.; Snounou, G. Genotyping of Plasmodium falciparum isolates by the polymerase chain reaction and potential uses in epidemiological studies. Bull. World Health Organ. 1995, 73, 85–95. [Google Scholar]
- Felger, I.; Tavul, L.; Kabintik, S.; Marshall, V.; Genton, B.; Alpers, M.; Beck, H. Plasmodium falciparum: Extensive Polymorphism in Merozoite Surface Antigen 2 Alleles in an Area with Endemic Malaria in Papua New Guinea. Exp. Parasitol. 1994, 79, 106–116. [Google Scholar] [CrossRef]
- Premji, Z.; Ndayanga, P.; Shiff, C.; Minjas, J.; Lubega, P.; MacLeod, J. Community based studies on childhood mortality in a malaria holoendemic area on the Tanzanian coast. Acta Trop. 1997, 63, 101–109. [Google Scholar] [CrossRef]
- Bolad, A.; Berzins, K. Antigenic Diversity of Plasmodium falciparum and Antibody-Mediated Parasite Neutralization. Scand. J. Immunol. 2000, 52, 233–239. [Google Scholar] [CrossRef]
- Mueller, I.; Schoepflin, S.; Smith, T.A.; Benton, K.L.; Bretscher, M.T.; Lin, E.; Kiniboro, B.; Zimmerman, P.A.; Speed, T.P.; Siba, P.; et al. Force of infection is key to understanding the epidemiology of Plasmodium falciparum malaria in Papua New Guinean children. Proc. Natl. Acad. Sci. USA 2012, 109, 10030–10035. [Google Scholar] [CrossRef]
- Arnot, D. Clone multiplicity of Plasmodium falciparum infections in individuals exposed to variable levels of disease transmission. Trans. R. Soc. Trop. Med. Hyg. 1998, 92, 580–585. [Google Scholar] [CrossRef]
- INSD (Institut National de la Statistique et de la Démographie). Résultats Cinquième Recensement Général de la Population et de L’habitation: Monographie de la Région des Cascades; Institut National de la Statistique et de la Démographie: Ouagadougou, Burkina Faso, 2022; 192p, Available online: http://www.cns.bf/IMG/pdf/monographie_des_cascades_5e_rgph.pdf (accessed on 12 December 2023).
- Tiono, A.B.; Kangoye, D.T.; Rehman, A.M.; Kargougou, D.G.; Kaboré, Y.; Diarra, A.; Ouedraogo, E.; Nébié, I.; Ouédraogo, A.; Okech, B.; et al. Malaria Incidence in Children in South-West Burkina Faso: Comparison of Active and Passive Case Detection Methods. PLoS ONE 2014, 9, e86936. [Google Scholar] [CrossRef]
- WHO (World Health Organization). WHO Policy Recommendation: Seasonal Malaria Chemoprevention (SMC) for Plasmodium falciparum Malaria Control in Highly Seasonal Transmission Areas of the Sahel Sub-Region in Africa; World Health Organization: Geneva, Switzerland, 2012; 4p, Available online: https://iris.who.int/bitstream/handle/10665/337978/WHO-HTM-GMP-2012.02-eng.pdf (accessed on 12 December 2023).
- Snounou, G.; Viriyakosol, S.; Zhu, X.P.; Jarra, W.; Pinheiro, L.; Rosario, V.E.D.; Thaithong, S.; Brown, K. High sensitivity of detection of human malaria parasites by the use of nested polymerase chain reaction. Mol. Biochem. Parasitol. 1993, 61, 315–320. [Google Scholar] [CrossRef]
- WHO (World Health Organization). Methods and Techniques for Clinical Trials on Antimalarial Drug Efficacy: Genotyping to Identify Parasite Populations. In Amsterdam The Netherlands Geneva: Medicines for Malaria Venture Informal consultation.; World Health Organization: Geneva, Switzerland, 2007; 54p, Available online: https://iris.who.int/handle/10665/43824 (accessed on 12 December 2023).
- Snounou, G.; Zhu, X.; Siripoon, N.; Jarra, W.; Thaithong, S.; Brown, K.N.; Viriyakosol, S. Biased distribution of msp1 and msp2 allelic variants in Plasmodium falciparum populations in Thailand. Trans. R. Soc. Trop. Med. Hyg. 1999, 93, 369–374. [Google Scholar] [CrossRef] [PubMed]
- Smythe, J.A.; Peterson, M.; Coppel, R.L.; Saul, A.J.; Kemp, D.J.; Anders, R.F. Structural diversity in the 45-kilodalton merozoite surface antigen of Plasmodium falciparum. Mol. Biochem. Parasitol. 1990, 39, 227–234. [Google Scholar] [CrossRef]
- Tanabe, K.; Mackay, M.; Goman, M.; Scaife, J.G. Allelic dimorphism in a surface antigen gene of the malaria parasite Plasmodium falciparum. J. Mol. Biol. 1987, 195, 273–287. [Google Scholar] [CrossRef]
- Ntoumi, F.; Contamin, H.; Rogier, C.; Bonnefoy, S.; Trape, J.-F.; Mercereau-Puijalon, O. Age-Dependent Carriage of Multiple Plasmodium falciparum Merozoite Surface Antigen-2 Alleles in Asymptomatic Malaria Infections. Am. J. Trop. Med. Hyg. 1995, 52, 81–88. [Google Scholar] [CrossRef]
- Felger, I.; Irion, A.; Steiger, S.; Beck, H.-P. 2. Genotypes of merozoite surface protein 2 of Plasmodium falciparum in Tanzania. Trans. R. Soc. Trop. Med. Hyg. 1999, 93, 3–9. [Google Scholar] [CrossRef]
- Ojurongbe, O.; Fagbenro-Beyioku, A.F.; A Adeyeba, O.; Kun, J.F. Allelic diversity of merozoite surface protein 2 gene of P falciparum among children in Osogbo, Nigeria. West Indian Med. J. 2011, 60, 19–23. [Google Scholar]
- Walldorf, J.A.; Cohee, L.M.; Coalson, J.E.; Bauleni, A.; Nkanaunena, K.; Kapito-Tembo, A.; Seydel, K.B.; Ali, D.; Mathanga, D.; Taylor, T.E.; et al. School-Age Children Are a Reservoir of Malaria Infection in Malawi. PLoS ONE 2015, 10, e0134061. [Google Scholar] [CrossRef]
- Cohee, L.M.; Opondo, C.; E Clarke, S.; E Halliday, K.; Cano, J.; Shipper, A.G.; Barger-Kamate, B.; Djimde, A.; Diarra, S.; Dokras, A.; et al. Preventive malaria treatment among school-aged children in sub-Saharan Africa: A systematic review and meta-analyses. Lancet Glob. Health 2020, 8, e1499–e1511. [Google Scholar] [CrossRef]
- Nankabirwa, J.; Brooker, S.J.; Clarke, S.E.; Fernando, D.; Gitonga, C.W.; Schellenberg, D.; Greenwood, B. Malaria in school-age children in Africa: An increasingly important challenge. Trop. Med. Int. Health 2014, 19, 1294–1309. [Google Scholar] [CrossRef]
- Sondo, P.; Derra, K.; Rouamba, T.; Diallo, S.N.; Taconet, P.; Kazienga, A.; Ilboudo, H.; Tahita, M.C.; Valéa, I.; Sorgho, H.; et al. Determinants of Plasmodium falciparum multiplicity of infection and genetic diversity in Burkina Faso. Parasites Vectors 2020, 13, 427. [Google Scholar] [CrossRef] [PubMed]
- Badoum, E.S.; Bougouma, E.C.; Sombie, S.; Sermé, S.S.; Yaro, J.B.; Diarra, A.; Nébié, I.; Ouedraogo, A.; Tiono, A.B.; Soulama, I.; et al. Relationship between human genetic factors and Plasmodium falciparum genetic diversity of msp1, msp2 and glurp in a malaria endemic area of Burkina Faso. Biomed. Genet. Genom. 2019, 4, 10-15761. [Google Scholar] [CrossRef]
- Soulama, I.; Nébié, I.; Ouédraogo, A.; Gansane, A.; Diarra, A.; Tiono, A.B.; Bougouma, E.C.; Konaté, A.T.; Kabré, G.B.; Taylor, W.R.; et al. Plasmodium falciparum genotypes diversity in symptomatic malaria of children living in an urban and a rural setting in Burkina Faso. Malar. J. 2009, 8, 135. [Google Scholar] [CrossRef] [PubMed]
- Somé, A.F.; Bazié, T.; Zongo, I.; Yerbanga, R.S.; Nikiéma, F.; Neya, C.; Taho, L.K.; Ouédraogo, J.-B. Plasmodium falciparum msp1 and msp2 genetic diversity and allele frequencies in parasites isolated from symptomatic malaria patients in Bobo-Dioulasso, Burkina Faso. Parasites Vectors 2018, 11, 328. [Google Scholar] [CrossRef]
- Tadele, G.; Jaiteh, F.K.; Oboh, M.; Oriero, E.; Dugassa, S.; Amambua-Ngwa, A.; Golassa, L. Low genetic diversity of Plasmodium falciparum merozoite surface protein 1 and 2 and multiplicity of infections in western Ethiopia following effective malaria interventions. Malar. J. 2022, 21, 383. [Google Scholar] [CrossRef]
- Konaté, L.; Zwetyenga, J.; Rogier, C.; Bischoff, E.; Fontenille, D.; Tall, A.; Spiegel, A.; Trape, J.-F.; Mercereau-Puijalon, O. 5. Variation of Plasmodium falciparum msp1 block 2 and msp2 allele prevalence and of infection complexity in two neighbouring Senegalese villages with different transmission conditions. Trans. R. Soc. Trop. Med. Hyg. 1999, 93, 21–28. [Google Scholar] [CrossRef]
- Zwetyenga, J.; Rogier, C.; Trape, J.F.; Snounou, G.; Fontenille, D.; Tall, A.; Mercereau-Puijalon, O. No influence of age on infection complexity and allelic distribution in Plasmodium falciparum infections in Ndiop, a Senegalese village with seasonal, mesoendemic malaria. Am. J. Trop. Med. Hyg. 1998, 59, 726–735. [Google Scholar] [CrossRef]
- Arzika, I.; Lamine, M.M.; Mahamadou, A.; Zamanka, H.; Laminou, I.M. Etude du polymorphisme genetique des souches de Plasmodium falciparum au Niger. Rev. CAMES SANTE 5 2017, 7, 42–48. [Google Scholar]
- Miles, A.; Iqbal, Z.; Vauterin, P.; Pearson, R.; Campino, S.; Theron, M.; Gould, K.; Mead, D.; Drury, E.; O’Brien, J.; et al. Indels, structural variation, and recombination drive genomic diversity in Plasmodium falciparum. Genome Res. 2016, 26, 1288–1299. [Google Scholar] [CrossRef]
- Funwei, R.I.; Thomas, B.N.; Falade, C.O.; Ojurongbe, O. Extensive diversity in the allelic frequency of Plasmodium falciparum merozoite surface proteins and glutamate-rich protein in rural and urban settings of southwestern Nigeria. Malar. J. 2018, 17, 1. [Google Scholar] [CrossRef]
- Chang, H.-H.; Childs, L.M.; Buckee, C.O. Variation in infection length and superinfection enhance selection efficiency in the human malaria parasite. Sci. Rep. 2016, 6, 26370. [Google Scholar] [CrossRef]
- Vafa, M.; Troye-Blomberg, M.; Anchang, J.; Garcia, A.; Migot-Nabias, F. Multiplicity of Plasmodium falciparum infection in asymptomatic children in Senegal: Relation to transmission, age and erythrocyte variants. Malar. J. 2008, 7, 17. [Google Scholar] [CrossRef] [PubMed]
- Ranford-Cartwright, L.C.; Balfe, P.; Carter, R.; Walliker, D. Frequency of cross-fertilization in the human malaria parasite Plasmodium falciparum. Parasitology 1993, 107, 11–18. [Google Scholar] [CrossRef]
- Hastings, I.M.; Watkins, W.M. Intensity of malaria transmission and the evolution of drug resistance. Acta Trop. 2005, 94, 218–229. [Google Scholar] [CrossRef]
- Patgiri, S.J.; Sarma, K.; Sarmah, N.; Bhattacharyya, N.; Sarma, D.K.; Nirmolia, T.; Bhattacharyya, D.R.; Mohapatra, P.K.; Bansal, D.; Bharti, P.K.; et al. Characterization of drug resistance and genetic diversity of Plasmodium falciparum parasites from Tripura, Northeast India. Sci. Rep. 2019, 9, 13704. [Google Scholar] [CrossRef]
- Port, G.R.; Boreham, P.F.L.; Bryan, J.H. The relationship of host size to feeding by mosquitoes of the Anopheles gambiae Giles complex (Diptera: Culicidae). Bull. Entomol. Res. 1980, 70, 133–144. [Google Scholar] [CrossRef]
- Smith, T.; Killeen, G.F.; Maire, N.; Dietz, K.; Molineaux, L.; Vounatsou, P.; Tanner, M. Relationship between the entomologic inoculation rate and the force of infection for Plasmodium falciparum malaria. Am. J. Trop. Med. Hyg. 2006, 75, 11–18. [Google Scholar] [CrossRef]
- Yaro, J.B.; Ouedraogo, A.; Ouedraogo, Z.A.; Diarra, A.; Lankouande, M.; Agboraw, E.; Worrall, E.; Toe, K.H.; Sanou, A.; Guelbeogo, W.M.; et al. A cohort study to identify risk factors for Plasmodium falciparum infection in Burkinabe children: Implications for other high burden high impact countries. Malar. J. 2020, 19, 371. [Google Scholar] [CrossRef]
- Rogier, C.; Henry, M.C.; Spiegel, A. Diagnostic des accès palustres en zone d’endémie: Bases théoriques et implications pratiques. Med. Trop. 2001, 61, 27–46. Available online: https://www.jle.com/en/MedSanteTrop/2001/61.1/027-046 Diagnostic des accès palustres en zone d’endémie bases théoriques et implications pratiques (Rogier).pdf (accessed on 12 December 2023).
- Ullah, I.; Khan, A.; Israr, M.; Shah, M.; Shams, S.; Khan, W.; Shah, M.; Siraj, M.; Akbar, K.; Naz, T.; et al. Genomic miscellany and allelic frequencies of Plasmodium falciparum msp-1, msp-2 and glurp in parasite isolates. PLoS ONE 2022, 17, e0264654. [Google Scholar] [CrossRef]
- Boyce, R.M.; Hathaway, N.; Fulton, T.; Reyes, R.; Matte, M.; Ntaro, M.; Mulogo, E.; Waltmann, A.; Bailey, J.A.; Siedner, M.J.; et al. Reuse of malaria rapid diagnostic tests for amplicon deep sequencing to estimate Plasmodium falciparum transmission intensity in western Uganda. Sci. Rep. 2018, 8, 10159. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.T.; Hathaway, N.J.; Saunders, D.L.; Lon, C.; Balasubramanian, S.; Kharabora, O.; Gosi, P.; Sriwichai, S.; Kartchner, L.; Chuor, C.M.; et al. Using Amplicon Deep Sequencing to Detect Genetic Signatures of Plasmodium vivax Relapse. J. Infect. Dis. 2015, 212, 999–1008. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Characteristic | n (%) |
|---|---|
| Age | |
| ˂5years | 191 (41.16) |
| ≥5years | 273 (58.84) |
| Sex | |
| Male | 229 (49.35) |
| Female | 235 (50.65) |
| Protection tools against mosquitoes’ bites | |
| ITN | 94 (20.30) |
| Insecticide only | 3 (0.65) |
| ITN + Insecticide | 358 (77.32) |
| None | 8 (1.73) |
| Unadjusted Model | Adjusted Model | |||||
|---|---|---|---|---|---|---|
| IRR | 95% CI | p Value | IRR | 95% CI | p Value | |
| Age | 0.78 | [0.67–0.91] | 0.002 | 0.74 | [0.61–0.90] | 0.002 |
| Gender | 0.74 | [0.33–1.69] | 0.482 | 0.41 | [0.16–1.08] | 0.997 |
| Polyclonality | 0.75 | [0.18–3.08] | 0.687 | 0.49 | [0.11–2.22] | 0.354 |
| MOI | 1.30 | [1.03–1.64] | 0.025 | 1.43 | [1.04–1.99] | 0.029 |
| FOI | - | - | - | 0.99 | [0.70–1.43] | 0.997 |
| Log likelihood | −90.85 | −66.43 | ||||
| AIC | 191.69 | 144.85 | ||||
| Univariate Analysis | Multivariate Analysis | Adjusted Model | |||||||
|---|---|---|---|---|---|---|---|---|---|
| IRR | 95% CI | p Value | IRR | 95% CI | p Value | IRR | 95% CI | p Value | |
| Age Group | |||||||||
| ˂5years | 1 (base) | 1 (base) | |||||||
| ≥5years | 0.87 | [0.75–0.99] | 0.042 | 0.87 | [0.73–1.046] | 0.144 | |||
| Gender | |||||||||
| Male | 1 (base) | 1 (base) | |||||||
| Female | 1.08 | [0.96–1.22] | 0.217 | 1.026 | [0.88–1.19] | 0.719 | |||
| Polyclonality | |||||||||
| No | 1 (base) | 1 (base) | |||||||
| Yes | 4.001 | [3.10–5.15] | ˂0.001 | 2.90 | [2.13–3.96] | ˂0.001 | 2.962 | [2.17–4.03] | ˂0.001 |
| Treated (treatment administrated during follow-up) | |||||||||
| No | 1 (base) | 1 (base) | |||||||
| Yes | 0.69 | [0.61–0.78] | ˂0.001 | 0.88 | [0.73–1.08] | 0.504 | |||
| Fever | |||||||||
| No | 1 (base) | 1 (base) | |||||||
| Yes | 1.34 | [1.13–1.59] | 0.001 | 1.23 | [0.97–1.54] | 0.084 | |||
| Study site | |||||||||
| Bounouna | 1 (base) | 1 (base) | |||||||
| Nafona | 1.24 | [1.10–1.40] | ˂0.001 | 1.12 | [0.95–1.31] | 0.172 | |||
| FOI | 1.27 | [1.03–1.64] | ˂0.001 | 1.17 | [1.12–1.23] | ˂0.001 | 1.168 | [1.12–1.22] | ˂0.001 |
| Parasitemia | 1.46 | [1.28–1.66] | ˂0.001 | 1.17 | [0.99–1.39] | 0.072 | 1.239 | [1.06–1.45] | 0.006 |
| Season of sample collection | |||||||||
| Dry months | 1 (base) | 1 (base) | 1 (base) | ||||||
| Rainy months | 1.51 | [1.32–1.72] | ˂0.001 | 1.62 | [1.31–1.99] | ˂0.001 | 1.680 | [1.38–2.04] | ˂0.001 |
| Univariate Analysis | Multivariate Analysis | Adjusted Model | |||||||
|---|---|---|---|---|---|---|---|---|---|
| IRR | 95% CI | p Value | IRR | 95% CI | p Value | IRR | 95% CI | p Value | |
| Age Group | |||||||||
| ˂5years | 1 (base) | 1 (base) | |||||||
| ≥5years | 0.80 | [0.66–0.98] | 0.032 | 0.81 | [0.65–1.00] | 0.060 | |||
| Gender | |||||||||
| Male | 1 (base) | 1 (base) | |||||||
| Female | 1.12 | [0.94–1.34] | 0.187 | 1.09 | [0.91–1.31] | 0.327 | |||
| Polyclonality | |||||||||
| No | 1 (base) | 1 (base) | 1 (base) | ||||||
| Yes | 4.98 | [3.36–7.39] | ˂0.001 | 2.47 | [1.62–3.77] | ˂0.001 | 2.46 | [1.62–3.76] | ˂0.001 |
| Treated (treatment administrated during follow-up) | |||||||||
| No | 1 (base) | 1 (base) | |||||||
| Yes | 1.45 | [1.20–1.76] | ˂0.001 | 1.07 | [0.85–1.36] | 0.542 | |||
| Fever | |||||||||
| No | 1 (base) | 1 (base) | |||||||
| Yes | 1.45 | [1.13–1.84] | 0.003 | 0.89 | [0.66–1.19] | 0.435 | |||
| Study site | |||||||||
| Bounouna | 1 (base) | 1 (base) | |||||||
| Nafona | 1.31 | [1.10–1.55] | 0.002 | 1.13 | [0.92–1.39] | 0.235 | |||
| MOI | 1.0004 | [0.92–1.08] | 0.993 | 1.26 | [1.20–1.33] | ˂0.001 | 1.27 | [1.22–1.34] | ˂0.001 |
| Parasitemia | 1.55 | [1.28–1.86] | ˂0.001 | 1.07 | [0.86–1.33] | 0.530 | |||
| Season of sample collection | |||||||||
| Dry months | 1 (base) | 1 (base) | |||||||
| Rainy months | 2.08 | [1.65–2.61] | ˂0.001 | 2.02 | [1.57–2.60] | ˂0.001 | 2.09 | [1.67–2.63] | ˂0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Badoum, E.S.; Kouraogo, L.; Diarra, A.; Ouattara, D.; Nebie, I.; Ouedraogo, A.; Tiono, A.B.; Sirima, S.B. Force of Infection (FOI) and Multiplicity of Infection (MOI) in Plasmodium falciparum Infected Children Aged 1.5–12 Years Living in the Malaria Endemic Area of Banfora, Burkina Faso. Pathogens 2024, 13, 883. https://doi.org/10.3390/pathogens13100883
Badoum ES, Kouraogo L, Diarra A, Ouattara D, Nebie I, Ouedraogo A, Tiono AB, Sirima SB. Force of Infection (FOI) and Multiplicity of Infection (MOI) in Plasmodium falciparum Infected Children Aged 1.5–12 Years Living in the Malaria Endemic Area of Banfora, Burkina Faso. Pathogens. 2024; 13(10):883. https://doi.org/10.3390/pathogens13100883
Chicago/Turabian StyleBadoum, Emilie S., Ludovic Kouraogo, Amidou Diarra, Daouda Ouattara, Issa Nebie, Alphonse Ouedraogo, Alfred B. Tiono, and Sodiomon B. Sirima. 2024. "Force of Infection (FOI) and Multiplicity of Infection (MOI) in Plasmodium falciparum Infected Children Aged 1.5–12 Years Living in the Malaria Endemic Area of Banfora, Burkina Faso" Pathogens 13, no. 10: 883. https://doi.org/10.3390/pathogens13100883
APA StyleBadoum, E. S., Kouraogo, L., Diarra, A., Ouattara, D., Nebie, I., Ouedraogo, A., Tiono, A. B., & Sirima, S. B. (2024). Force of Infection (FOI) and Multiplicity of Infection (MOI) in Plasmodium falciparum Infected Children Aged 1.5–12 Years Living in the Malaria Endemic Area of Banfora, Burkina Faso. Pathogens, 13(10), 883. https://doi.org/10.3390/pathogens13100883