Abstract
Toxoplasma (T.) gondii is an obligate intracellular parasite with felids, including domestic cats, as definitive hosts. In immunocompetent individuals, T. gondii infection is usually asymptomatic. However, under immunosuppression, it may have severe pathological impacts, which often result from the reactivation of a chronic infection. In this case study, a 21-month-old female domestic shorthair cat—diagnosed with primary immune-mediated hemolytic anemia three months prior and treated with cyclosporine and prednisolone—presented with acute tachypnea, dyspnea, diarrhea, and anorexia. Thoracic radiography suggested severe pneumonia. Testing for Mycoplasma spp., Anaplasma spp., Ehrlichia spp., and lungworm infection was negative. Serology for T. gondii revealed seroconversion of IgG, but not of IgM, indicating previous exposure to T. gondii. The cat remained stable but tachypneic for three days, followed by an acute onset of dyspnea and clinical deterioration, after which euthanasia was elected. Numerous protozoa were present in a postmortem transtracheal bronchoalveolar lavage and fine-needle aspiration of the lung. Microsatellite typing classified the extracted DNA as T. gondii type II variant TgM-A. This case demonstrates that T. gondii reactivation, leading to fulminant pneumonia, can be a sequela of immunosuppressive treatment in cats and should, therefore, be considered as a differential diagnosis in immunosuppressed cats with acute-onset respiratory signs. Rapid diagnosis may prevent fatal consequences.
1. Introduction
Autoimmune conditions are common in companion animals, including cats, and can either involve several different organ systems or present a multicentric condition such as systemic lupus erythematosus [1]. Differences in the frequency of occurrence, underlying etiologies, and pathomechanisms vary between dogs and cats, and species-specific differences in the immune response—particularly the T-helper-cell balance—might contribute to some differences between both species [2]. Immune-mediated hemolytic anemia (IMHA) is also common in cats [3], requiring the exclusion of non-immune-mediated causes [4,5,6,7,8,9] as well as infectious (e.g., hemotrophic Mycoplasma species) and neoplastic etiologies (e.g., lymphoma) for a diagnosis of primary autoimmune hemolytic anemia (AIHA) [10]. The mainstay of AIHA treatment is immunosuppression and the prevention of complications such as thrombosis and thromboembolism [3,11,12]. Secondary infections are also a concern in any natural or iatrogenic immunosuppressed patient [13,14], and this can include infectious bacterial or protozoal pneumonia and the development of septicemia with potentially fatal outcomes [15].
Toxoplasma (T.) gondii is an obligate intracellular protozoan parasite with the cat as its definitive host and all warm-blooded animals as intermediate hosts [16]. It is globally distributed and causes the zoonosis toxoplasmosis. Two recent systematic analyses found that its global seroprevalence is estimated at 26% in humans [17] and 35% in domestic cats [18]. T. gondii is the only species in the genus Toxoplasma. In Europe, most genotypes observed belong to three clonal lineages (types I, II, and III), with type II representing the genotype of the vast majority of isolates. T. gondii has several developmental stages during its life cycle [19]. Sexual reproduction of the parasite occurs in the intestine of the definitive host, with the resulting oocysts being exclusively excreted in the feces. Oral infection results in rapid asexual multiplication of the acute (tachyzoite) stage, followed by the infection of all tissues via the blood, lymph and peritoneal fluid [20]. In chronic stages of the disease, intracellular tissue cysts with bradyzoites are formed, which have a reduced metabolism and may persist throughout the host’s lifetime [21]. In adult healthy and immunocompetent individuals, T. gondii infection is usually asymptomatic. However, in people who are immunosuppressed due to autoimmune disease treatment or underlying disease (e.g., with human immunodeficiency virus), T. gondii infection may have severe pathological impacts, which most often result from the reactivation of a chronic T. gondii infection [22,23,24,25]. Similarly, localized or disseminated toxoplasmosis in cats has been associated with immunodeficient states following treatment with immunosuppressant medication [26,27,28,29] or retrovirus infection [30,31]. Corresponding clinical signs include fever, loss of appetite, weight loss, lethargy, neurological signs (e.g., tremors or seizures), pneumonia, uveitis, retinitis, and hepatitis. Given the broad spectrum of clinical manifestations, diagnosis of feline toxoplasmosis is often challenging and contributes to fatal outcomes if cases remain undiagnosed.
This case report documents the reactivation of latent toxoplasmosis and its clinical manifestation in the respiratory system following immunosuppressive treatment in a cat.
2. Case Report
A 21-month-old female domestic shorthair cat (3.3 kg) presented with acute onset of tachypnea and dyspnea at home. The cat also had acute diarrhea and anorexia in the two days prior to presentation and was progressively lethargic. The pertinent patient history included a primary IMHA (AIHA) that was diagnosed three months earlier. To treat the AIHA, the cat received cyclosporin (Atopica®, Elanco, Bad Homburg, Germany; at 5 mg/kg PO q12h) monotherapy after combination therapy with prednisolone (started at 1.4 mg/kg PO q12h) was tapered (dose reduction by 25% every 2–3 weeks) and discontinued two weeks before presentation. The cat was strictly housed indoors, had no obvious concurrent conditions, and received no other medications or supplements. Vaccinations were not current, but the cat had been regularly dewormed. Retrovirus testing (feline leukemia virus and feline immunodeficiency virus) was negative at the time of IMHA diagnosis.
Upon physical examination, the cat was quiet, alert, and responsive but experienced distress with handling. The heart rate was 160/min (no pulse deficit), and the respiratory rate was 68/min (forceful breathing with abdominal push); the rectal body temperature could not be measured. Oral mucous membranes were pale, with a capillary refill time of <2 s. Sneezing, nasal discharge, or spontaneous coughing were not noted. Palpation of the abdomen and peripheral lymph nodes was unremarkable.
Abdominal ultrasonography revealed no abnormalities of the liver, spleen, kidneys, adrenal glands, pancreas, liver, gall bladder, stomach, and intestines, but mild mesenteric lymphadenopathy likely reflected a reactive change. A laterolateral thoracic radiograph was performed and showed a generally reduced opacity of the lung fields with a mixed bronchointerstitial to alveolar lung pattern, a poorly delineated cardiac silhouette and a mildly increased vertebral heart size (VHS) of 9.4 (normal right lateral VHS: <8.1) (Figure 1).
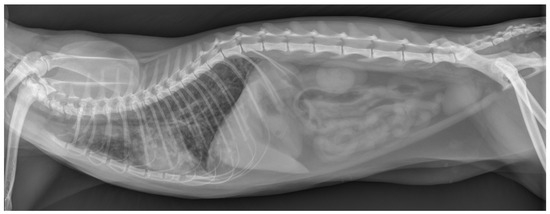
Figure 1.
Thoracic radiograph at the time of presentation. This laterolateral view shows a generalized mixed bronchointerstitial to alveolar lung pattern, resulting in a decreased delineation of the cardiac silhouette.
Hematology revealed normal erythrogram findings (hematocrit: 37.3%, reference interval (RI): 30.3–52.3%; mean corpuscular volume: 38.0 fL, RI: 35.9–53.1 fL; mean corpuscular hemoglobin: 13.4 pg, RI: 11.8–17.3 pg; reticulocyte count: 13.7 × 109/L, RI: <50 × 109/L). In addition, there was a marked leukopenia (0.81 × 109/L, RI: 2.87–17.02 × 109/L) characterized by mature neutropenia (0.13 × 109/L, RI: 1.48–10.29 × 109/L) and mild thrombocytopenia (automated count: 137 × 109/L, manual count: 118 × 109/L; RI: 151–600 × 109/L). The serum biochemistry profile showed a high-normal blood glucose concentration (8.2 mmol/L, RI: 3.9–8.2 mmol/L), low-normal potassium concentration (3.5 mmol/L, RI: 3.4–4.6 mmol/L), and minimal hyperchloremia (sodium-corrected chloride: 120.2 mmol/L, RI: 107–120 mmol/L), while all other parameters were within the corresponding normal reference intervals. The patient-side NT-proBNP (N-terminal pro-brain natriuretic peptide) test (feline proBNP SNAP®, Idexx Laboratories, Kornwestheim, Germany) was normal. Fecal flotation/sedimentation and the Baerman technique for lungworm detection were negative. Moreover, polymerase chain reaction (PCR)-based testing for feline hemotrophic mycoplasmosis (M. hemofelis, Cand. M. hemominutum, and Cand. M. turicensis) and serology for Anaplasma spp. and Ehrlichia canis were all negative. Serological testing for T. gondii using an indirect immunofluorescence assay (IDEXX Laboratories, Kornwestheim, Germany) was negative for immunoglobulin M (IgM) but positive for IgG at dilutions >1:1024.
More invasive diagnostics comprising a tracheobronchoscopy with bronchoalveolar lavage (for cytology and clinical microbiology) under general anesthesia were considered to evaluate important differential diagnoses further. However, these could not be performed given the overall clinical condition of the cat.
The cat was hospitalized in the intensive care unit and received supplemental oxygen (oxygen cage, 40% O2), intravenous crystalloid fluid support (Ringer’s Acetate solution), bronchodilation with theophylline (Euphylong® Injectable solution, Altana Pharma, Konstanz, Germany), amoxicillin/clavulanate (AmoxiClav®, Hikma, Munich, Germany) antimicrobial treatment, and empirical deworming with fenbendazole (Panacur®, MSD-Intervet, Unterschleißheim, Germany), and was closely monitored for any changes in its respiratory rate and effort or other complications. Carefully weighing the benefits of the current treatment strategy against the risks of AIHA relapse and the working diagnosis of secondary infectious pneumonia, cyclosporine treatment was decided to be continued. Given the severe neutropenia and lack of significant clinical improvement within 24 h, clindamycin (Cleorobe®, Zoetis, Berlin, Germany) was added to the treatment plan. The cat remained stable but tachypneic for three days, followed by an acute onset of dyspnea on day four of hospitalization. Repeat thoracic radiographs (only one image plane due to the clinical instability of the cat) revealed mildly progressive changes (Figure 2). The cat acutely decompensated, and humane euthanasia was elected by the owner.
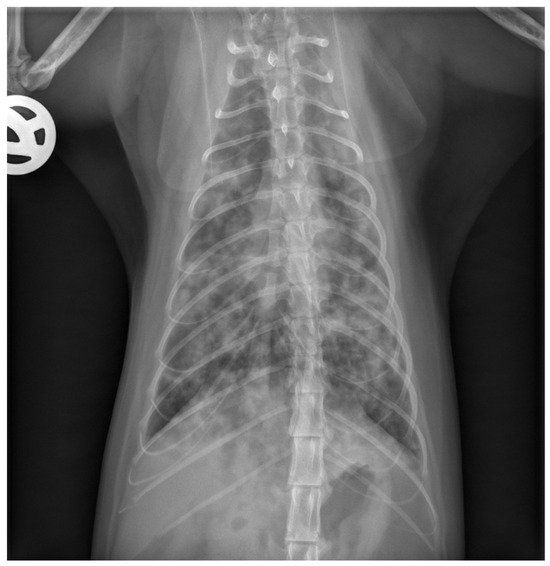
Figure 2.
Repeat thoracic radiograph after 3 days of hospitalization. This ventrodorsal view shows a progressive bronchointerstitial to alveolar lung pattern compared to the initial radiographs obtained at the time of presentation.
A postmortem transtracheal bronchoalveolar lavage (BAL) and fine-needle aspiration (FNA) of the lung were performed. Cytology of the BAL fluid and FNA samples, stained with Diff-Quik, revealed numerous protozoal structures that were distributed extracellularly as well as within alveolar macrophages (Figure 3). Microsatellite typing of the protozoal DNA extracted from BAL fluid and lung FNA samples classified the isolate as T. gondii type II variant TgM-A (Table 1).
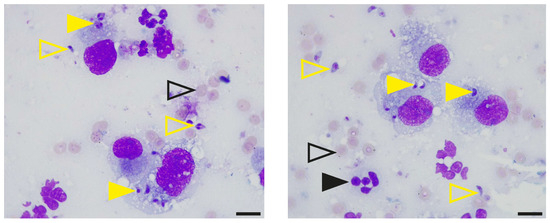
Figure 3.
Identification of protozoal structures in the feline bronchoalveolar lavage fluid. Samples of bronchoalveolar lavage fluid and fine-needle aspiration of the lung were centrifuged onto glass slides, stained with Diff-Quik and examined using a Leica DM 750 light microscope equipped with a 100× oil objective (NA 1.25) and a Leica ICC50W camera (Leica, Wetzlar, Germany). Open yellow arrowheads indicate extracellular protozoa, and closed arrowheads in yellow point to protozoa within alveolar macrophages. Open black arrowheads show erythrocytes, and closed arrowheads in black indicate neutrophils. Scale bars, 10 µm.

Table 1.
Microsatellite (MS) analysis of bronchoalveolar lavage fluid samples and fine-needle aspirates of the lung. DNA was extracted from cells and tissue using a NucleoSpin Tissue Mini kit for DNA (Machery-Nagel, Germany) and was analyzed via microsatellite typing. DNA was amplified using a multiplex PCR [25] including 15 unlinked MS markers, eight typing markers (TUB2, W35, TgM-A, B18, B17, M33, IV.1, XI.1) and seven fingerprinting markers (M48, M102, N83, N82, AA, N61, N60). Fingerprinting markers display a high level of polymorphism within the clonal lineages type I, type II, and type III [32]. Primers were used at a concentration of 0.2 pmol/µL. The only divergence from the original method was that in the case of M102, AA, and N60, and the fluorophore Atto 550 was used instead of NED to label amplicons during multiplex PCR. Samples were applied as duplicates. Water was used as a negative control, and T. gondii RH, Me49, and NED—corresponding to type I, II, and III strains, respectively—served as positive controls. Typing followed recently published guidelines, and the results were numerically corrected as recommended [33].
3. Discussion
We report a feline case of fulminant pneumonia, presumably due to the reactivation of latent T. gondii infection.
Based on a complete clinical evaluation and diagnostic work-up three months prior to presentation at the clinic with acute-onset respiratory signs, the cat was diagnosed with primary IMHA (AIHA). Treatment for primary IMHA consisted of immunosuppressant medications, using a combination of cyclosporine and prednisolone in a top-down treatment approach. Hematology revealed normal erythrogram findings (i.e., hematocrit, mean corpuscular volume, mean corpuscular hemoglobin, reticulocyte count), indicating that the primary IMHA was well controlled. However, the cat was in an immunosuppressed state given the treatment of the underlying disease and the development of marked hematologic abnormalities (marked leukopenia, mature neutropenia, and mild to moderate thrombocytopenia).
Diagnostic imaging revealed a normal appearance of abdominal organs (i.e., liver, spleen, kidneys, adrenal glands, pancreas, liver, gall bladder, stomach, and intestines) but marked alterations of the intrathoracic respiratory system (i.e., all lung fields). Specifically, thoracic radiographs at the time of presentation showed a mild generalized alveolar lung pattern with air-bronchograms superimposed on the cardiac silhouette and a mildly increased vertebral heart size, suggesting either pulmonary edema (cardiogenic vs. non-cardiogenic) or pneumonia (bacterial, parasitic, or other etiologies), but less likely diffuse infiltrative neoplasia (e.g., lymphoma, mast cell tumor). The NT-proBNP test was normal, supporting the suggestion that a non-cardiogenic etiology was more likely.
Vector-borne pathogens (M. hemofelis, Cand. M. hemominutum, and Cand. M. turicensis; Anaplasma spp. and Ehrlichia canis) and lungworm infection were ruled out as possible causes based on negative testing. However, serology revealed a high T. gondii-specific IgG titer (>1:1024) but no IgM titer, indicating a previous exposure to T. gondii that resulted in latent toxoplasmosis. Two similar cases with predominantly or exclusively IgG positivity were described in Australia [34], whereas a newly acquired infection was presumed in a cyclosporine-treated cat with fatal toxoplasmosis reported in South Africa [35]. The cat reported here was not given a raw meat-based diet (RMBD) for months prior to presentation, which could have been the source of an acute T. gondii infection. However, as it had been reported to have dug in the soil and licked stones on the owner’s patio when first presented for IMHA (presumably as a physiological compensatory response to the marked anemia), a recent infection via T. gondii-contaminated soil cannot be entirely excluded. While this would be expected to concur with a positive IgM titer, the antibody response may have been delayed in the face of iatrogenic immunosuppression. At the time of primary IMHA diagnosis, the cat had received blood products as an emergency stabilization measure. However, blood transfusion (A-type donor used based on blood typing) is an unlikely cause of T. gondii infection.
Direct tests (i.e., cytology and microsatellite genotyping) were utilized to confirm the suspicion of toxoplasmosis, specifically its manifestation in the respiratory system. Microscopic examination of Diff-Quik-stained BAL fluid and FNA cytology sections revealed the presence of numerous protozoal structures, substantiating the suspicion of respiratory toxoplasmosis. Microsatellite analysis confirmed the presence of T. gondii in BAL fluid material and FNA cytology sections and further classified the isolate as T. gondii type II strain, which is the predominating strain in humans and domestic animals in Europe and North America [36]. Altogether, these results confirmed the diagnosis of infectious pneumonia in this cat and identified the protozoal organism T. gondii as the primary pathogen. In immunocompromised people, reactivation of T. gondii most often manifests as encephalitis and, less frequently, as pneumonia, retinochoroiditis, or disseminated systemic disease [15,25,37]. Given the isolation of a common T. gondii strain in the geographic location of the reported feline case, an impaired clearance of this pathogen by the infected yet immunocompromised host more likely explains the fulminant disease course and fatal outcome than an increased pathogenicity of the organism. Our findings confirm previous reports in cats, in which reactive or acute toxoplasmosis was diagnosed following treatment with immunosuppressant medication, e.g., prednisolone and cyclosporine therapy [26,27,28,29,34,35].
4. Conclusions
T. gondii infection has a broad spectrum of clinical manifestations. This case report shows that T. gondii reactivation, leading to fulminant pneumonia, can be a sequela of immunosuppressive treatment in cats. Hence, T. gondii infection and its manifestation in the respiratory system should be considered in the differential diagnosis list for cats showing acute-onset respiratory signs following treatment with immunosuppressants or retrovirus infection. A rapid diagnosis of this complication can potentially decrease the risk of fatal outcomes.
Author Contributions
Conceptualization, S.A.F. and R.M.H.; methodology, S.A.F., T.G., G.S., T.T. and R.M.H.; software, S.A.F.; validation, S.A.F. and G.S.; formal analysis, G.S., T.T. and R.M.H.; investigation, S.A.F., T.G., G.S. and T.T.; resources, S.A.F., G.S. and R.M.H.; data curation, S.A.F., G.S. and R.M.H.; writing—original draft preparation, S.A.F., T.G. and T.T.; writing—review and editing, G.S. and R.M.H.; visualization, S.A.F., T.G. and T.T.; supervision, R.M.H.; project administration, S.A.F. and R.M.H.; funding acquisition, S.A.F. and R.M.H. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding. Open Access Publication supported by the Leipzig University Open Access Fund.
Institutional Review Board Statement
Ethical review and approval were waived for this study due to permission (owner consent) for using anonymized data, images, and surplus sampling material for research and teaching purposes being given by the owners upon signing the standard hospital admission form of the Department for Small Animals at Leipzig University.
Informed Consent Statement
Written owner consent for the use and publication of the anonymized data, images, and surplus materials has been obtained.
Data Availability Statement
Data and information about this case are available from the corresponding author upon reasonable request.
Acknowledgments
We thank Sandra Gawlowska and Maike Joeres for their technical support and Zaida Rentería-Solís for her conceptual advice.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Gershwin, L.J. Current and Newly Emerging Autoimmune Diseases. Vet. Clin. N. Am. Small Anim. Pract. 2018, 48, 323–338. [Google Scholar] [CrossRef] [PubMed]
- Day, M.J. Cats are not small dogs: Is there an immunological explanation for why cats are less affected by arthropod-borne disease than dogs? Parasites Vectors 2016, 9, 507. [Google Scholar] [CrossRef] [PubMed]
- Kohn, B.; Weingart, C.; Eckmann, V.; Ottenjann, M.; Leibold, W. Primary immune-mediated hemolytic anemia in 19 cats: Diagnosis, therapy, and outcome (1998–2004). J. Vet. Intern. Med. 2006, 20, 159–166. [Google Scholar] [CrossRef] [PubMed]
- Kohn, B.; Goldschmidt, M.H.; Hohenhaus, A.E.; Giger, U. Anemia, splenomegaly, and increased osmotic fragility of erythrocytes in Abyssinian and Somali cats. J. Am. Vet. Med. Assoc. 2000, 217, 1483–1491. [Google Scholar] [CrossRef] [PubMed]
- Grahn, R.A.; Grahn, J.C.; Penedo, M.C.; Helps, C.R.; Lyons, L.A. Erythrocyte pyruvate kinase deficiency mutation identified in multiple breeds of domestic cats. BMC Vet. Res. 2012, 8, 207. [Google Scholar] [CrossRef] [PubMed]
- Hurwitz, B.M.; Center, S.A.; Randolph, J.F.; McDonough, S.P.; Warner, K.L.; Hazelwood, K.S.; Chiapella, A.M.; Mazzei, M.J.; Leavey, K.; Acquaviva, A.E.; et al. Presumed primary and secondary hepatic copper accumulation in cats. J. Am. Vet. Med. Assoc. 2014, 244, 68–77. [Google Scholar] [CrossRef]
- Kushida, K.; Giger, U.; Tsutsui, T.; Inaba, M.; Konno, Y.; Hayashi, K.; Noguchi, K.; Yabuki, A.; Mizukami, K.; Kohyama, M.; et al. Real-time PCR genotyping assay for feline erythrocyte pyruvate kinase deficiency and mutant allele frequency in purebred cats in Japan. J. Vet. Med. Sci. 2015, 77, 743–746. [Google Scholar] [CrossRef]
- DeAvilla, M.D.; Leech, E.B. Hypoglycemia associated with refeeding syndrome in a cat. J. Vet. Emerg. Crit. Care 2016, 26, 798–803. [Google Scholar] [CrossRef]
- Yu, J.; Jenkins, E.; Podadera, J.M.; Proschogo, N.; Chan, R.; Boland, L. Zinc toxicosis in a cat associated with ingestion of a metal screw nut. JFMS Open Rep. 2022, 8, 20551169221136464. [Google Scholar] [CrossRef]
- Garden, O.A.; Kidd, L.; Mexas, A.M.; Chang, Y.M.; Jeffery, U.; Blois, S.L.; Fogle, J.E.; MacNeill, A.L.; Lubas, G.; Birkenheuer, A.; et al. ACVIM consensus statement on the diagnosis of immune-mediated hemolytic anemia in dogs and cats. J. Vet. Intern. Med. 2019, 33, 313–334. [Google Scholar] [CrossRef]
- Yoshida, T.; Mandour, A.S.; Sato, M.; Hirose, M.; Kikuchi, R.; Komiyama, N.; Hendawy, H.A.; Hamabe, L.; Tanaka, R.; Matsuura, K.; et al. Pulmonary thromboembolism due to immune-mediated hemolytic anemia in a cat: A serial study of hematology and echocardiographic findings. Front. Vet. Sci. 2022, 9, 930210. [Google Scholar] [CrossRef] [PubMed]
- DeLaforcade, A.; Bacek, L.; Blais, M.C.; Boyd, C.; Brainard, B.M.; Chan, D.L.; Cortellini, S.; Goggs, R.; Hoareau, G.L.; Koenigshof, A.; et al. 2022 Update of the Consensus on the Rational Use of Antithrombotics and Thrombolytics in Veterinary Critical Care (CURATIVE) Domain 1-Defining populations at risk. J. Vet. Emerg. Crit. Care 2022, 32, 289–314. [Google Scholar] [CrossRef] [PubMed]
- Schmiedt, C.W.; Holzman, G.; Schwarz, T.; McAnulty, J.F. Survival, complications, and analysis of risk factors after renal transplantation in cats. Vet. Surg. 2008, 37, 683–695. [Google Scholar] [CrossRef]
- Swann, J.W.; Szladovits, B.; Glanemann, B. Demographic Characteristics, Survival and Prognostic Factors for Mortality in Cats with Primary Immune-Mediated Hemolytic Anemia. J. Vet. Intern. Med. 2016, 30, 147–156. [Google Scholar] [CrossRef]
- Mariuz, P.; Bosler, E.M.; Luft, B.L. Toxoplasma pneumonia. Semin. Respir. Infect. 1997, 12, 40–43. [Google Scholar] [PubMed]
- Tenter, A.M.; Heckeroth, A.R.; Weiss, L.M. Toxoplasma gondii: From animals to humans. Int. J. Parasitol. 2000, 30, 1217–1258. [Google Scholar] [CrossRef] [PubMed]
- Molan, A.; Nosaka, K.; Hunter, M.; Wang, W. Global status of Toxoplasma gondii infection: Systematic review and prevalence snapshots. Trop. Biomed. 2019, 36, 898–925. [Google Scholar] [PubMed]
- Montazeri, M.; Mikaeili Galeh, T.; Moosazadeh, M.; Sarvi, S.; Dodangeh, S.; Javidnia, J.; Sharif, M.; Daryani, A. The global serological prevalence of Toxoplasma gondii in felids during the last five decades (1967–2017): A systematic review and meta-analysis. Parasites Vectors 2020, 13, 82. [Google Scholar] [CrossRef]
- Dubey, J.P.; Lindsay, D.S.; Speer, C.A. Structures of Toxoplasma gondii tachyzoites, bradyzoites, and sporozoites and biology and development of tissue cysts. Clin. Microbiol. Rev. 1998, 11, 267–299. [Google Scholar] [CrossRef]
- Halonen, S.K.; Weiss, L.M. Toxoplasmosis. Handb. Clin. Neurol. 2013, 114, 125–145. [Google Scholar] [CrossRef]
- Weiss, L.M.; Kim, K. The development and biology of bradyzoites of Toxoplasma gondii. Front. Biosci. 2000, 5, 391–405. [Google Scholar] [CrossRef] [PubMed]
- Montoya, J.G.; Liesenfeld, O. Toxoplasmosis. Lancet 2004, 363, 1965–1976. [Google Scholar] [CrossRef] [PubMed]
- Robert-Gangneux, F.; Belaz, S. Molecular diagnosis of toxoplasmosis in immunocompromised patients. Curr. Opin. Infect. Dis. 2016, 29, 330–339. [Google Scholar] [CrossRef]
- Dunay, I.R.; Gajurel, K.; Dhakal, R.; Liesenfeld, O.; Montoya, J.G. Treatment of Toxoplasmosis: Historical Perspective, Animal Models, and Current Clinical Practice. Clin. Microbiol. Rev. 2018, 31, e00057-17. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.D.; Liu, H.H.; Ma, Z.X.; Ma, H.Y.; Li, Z.Y.; Yang, Z.B.; Zhu, X.Q.; Xu, B.; Wei, F.; Liu, Q. Infection in Immunocompromised Patients: A Systematic Review and Meta-Analysis. Front. Microbiol. 2017, 8, 389. [Google Scholar] [CrossRef]
- Lo Piccolo, F.; Busch, K.; Palic, J.; Geisen, V.; Hartmann, K.; Unterer, S. Toxoplasma gondii-associated cholecystitis in a cat receiving immunosuppressive treatment. Tierärztliche Prax. Ausg. K Kleintiere/Heim. 2019, 47, 453–457. [Google Scholar] [CrossRef]
- Salant, H.; Klainbart, S.; Kelmer, E.; Mazuz, M.L.; Baneth, G.; Aroch, I. Systemic toxoplasmosis in a cat under cyclosporine therapy. Vet. Parasitol. Reg. Stud. Rep. 2021, 23, 100542. [Google Scholar] [CrossRef]
- Pena, H.F.D.; Evangelista, C.M.; Casagrande, R.A.; Biezus, G.; Wisser, C.S.; Ferian, P.E.; de Moura, A.B.; Rolim, V.M.; Driemeier, D.; Oliveira, S.; et al. Fatal toxoplasmosis in an immunosuppressed domestic cat from Brazil caused by clonal type I. Rev. Bras. Parasitol. Vet. 2017, 26, 177–184. [Google Scholar] [CrossRef]
- Ludwig, H.C.; Schlicksup, M.D.; Beale, L.M.; Aronson, L.R. Toxoplasma gondii infection in feline renal transplant recipients: 24 cases (1998–2018). J. Am. Vet. Med. Assoc. 2021, 258, 870–876. [Google Scholar] [CrossRef]
- Moore, A.; Burrows, A.K.; Malik, R.; Ghubash, R.M.; Last, R.D.; Remaj, B. Fatal disseminated toxoplasmosis in a feline immunodeficiency virus-positive cat receiving oclacitinib for feline atopic skin syndrome. Vet. Dermatol. 2022, 33, 435–439. [Google Scholar] [CrossRef]
- Davidson, M.G.; Rottman, J.B.; English, R.V.; Lappin, M.R.; Tompkins, M.B. Feline Immunodeficiency Virus Predisposes Cats to Acute Generalized Toxoplasmosis. Am. J. Pathol. 1993, 143, 1486–1497. [Google Scholar] [PubMed]
- Ajzenberg, D.; Collinet, F.; Mercier, A.; Vignoles, P.; Darde, M.L. Genotyping of Toxoplasma gondii isolates with 15 microsatellite markers in a single multiplex PCR assay. J. Clin. Microbiol. 2010, 48, 4641–4645. [Google Scholar] [CrossRef] [PubMed]
- Joeres, M.; Cardron, G.; Passebosc-Faure, K.; Plault, N.; Fernandez-Escobar, M.; Hamilton, C.M.; O’Brien-Anderson, L.; Calero-Bernal, R.; Galal, L.; Luttermann, C.; et al. A ring trial to harmonize Toxoplasma gondii microsatellite typing: Comparative analysis of results and recommendations for optimization. Eur. J. Clin. Microbiol. Infect. Dis. 2023, 42, 803–818. [Google Scholar] [CrossRef] [PubMed]
- Barrs, V.R.; Martin, P.; Beatty, J.A. Antemortem diagnosis and treatment of toxoplasmosis in two cats on cyclosporin therapy. Aust. Vet. J. 2006, 84, 30–35. [Google Scholar] [CrossRef] [PubMed]
- Last, R.D.; Suzuki, Y.; Manning, T.; Lindsay, D.; Galipeau, L.; Whitbread, T.J. A case of fatal systemic toxoplasmosis in a cat being treated with cyclosporin A for feline atopy. Vet. Dermatol. 2004, 15, 194–198. [Google Scholar] [CrossRef]
- Szabo, E.K.; Finney, C.A. Toxoplasma gondii: One Organism, Multiple Models. Trends Parasitol. 2017, 33, 113–127. [Google Scholar] [CrossRef]
- Walker, M.; Zunt, J.R. Parasitic central nervous system infections in immunocompromised hosts. Clin. Infect. Dis. 2005, 40, 1005–1015. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).