
High Predictive Value of the Soluble ZEBRA Antigen (Epstein-Barr Virus Trans-Activator Zta) in Transplant Patients with PTLD

Abstract
1. Introduction
2. Results
2.1. Patients
2.2. Characterization of EBV Markers in Patients with or without PTLD
2.2.1. Quantification of EBV Viral Load and Detection of sZEBRA (Soluble ZEBRA)
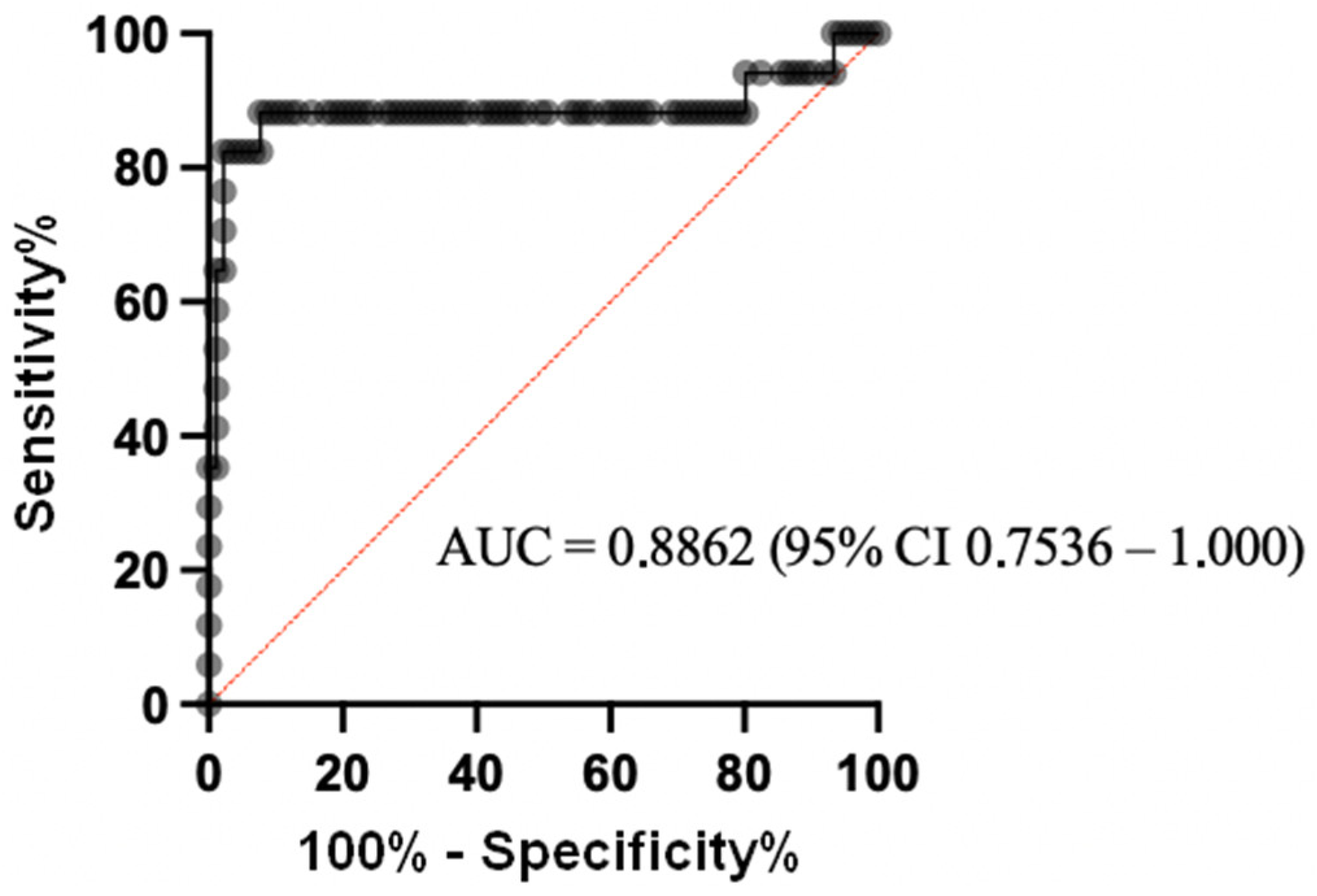
2.2.2. Diagnostic Value of sZEBRA Antigen
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. Quantification of EBV DNA in Whole Blood
4.3. Detection of Soluble ZEBRA (sZEBRA) Protein in Plasma Samples
4.4. Statistical Analysis
4.5. Ethical Considerations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Longnecker, R.M.; Kieff, E.D.; Cohen, J.I. Epstein-Barr virus. In Fields Virology; Knipe, D.M., Howley, P.M., Eds.; Wolters Kluwer Health/Lippincott Williams and Wilkins: Philadelphia, PA, USA, 2013; pp. 1898–1960. ISBN 978-1-4511-0563-6. [Google Scholar]
- Bjornevik, K.; Cortese, M.; Healy, B.C.; Kuhle, J.; Mina, M.J.; Leng, Y.; Elledge, S.J.; Niebuhr, D.W.; Scher, A.I.; Munger, K.L.; et al. Longitudinal Analysis Reveals High Prevalence of Epstein-Barr Virus Associated with Multiple Sclerosis. Science 2022, 375, 296–301. [Google Scholar] [CrossRef] [PubMed]
- Chiu, Y.-F.; Sugden, B. Epstein-Barr Virus: The Path from Latent to Productive Infection. Annu. Rev. Virol. 2016, 3, 359–372. [Google Scholar] [CrossRef] [PubMed]
- Tarbouriech, N.; Buisson, M.; Géoui, T.; Daenke, S.; Cusack, S.; Burmeister, W.P. Structural Genomics of the Epstein–Barr Virus. Acta Crystallogr. Sect. D Biol. Crystallogr. 2006, 62, 1276–1285. [Google Scholar] [CrossRef]
- Manners, O.; Murphy, J.C.; Coleman, A.; Hughes, D.J.; Whitehouse, A. Contribution of the KSHV and EBV Lytic Cycles to Tumourigenesis. Curr. Opin. Virol. 2018, 32, 60–70. [Google Scholar] [CrossRef]
- Germini, D.; Sall, F.B.; Shmakova, A.; Wiels, J.; Dokudovskaya, S.; Drouet, E.; Vassetzky, Y. Oncogenic Properties of the EBV ZEBRA Protein. Cancers 2020, 12, 1479. [Google Scholar] [CrossRef] [PubMed]
- Price, A.M.; Luftig, M.A. Dynamic Epstein-Barr Virus Gene Expression on the Path to B-Cell Transformation. Adv. Virus Res. 2014, 88, 279–313. [Google Scholar] [CrossRef] [PubMed]
- Rosemarie, Q.; Sugden, B. Epstein–Barr Virus: How Its Lytic Phase Contributes to Oncogenesis. Microorganisms 2020, 8, 1824. [Google Scholar] [CrossRef]
- Dierickx, D.; Habermann, T.M. Post-Transplantation Lymphoproliferative Disorders in Adults. N. Engl. J. Med. 2018, 378, 549–562. [Google Scholar] [CrossRef]
- Styczynski, J.; Gil, L.; Tridello, G.; Ljungman, P.; Donnelly, J.P.; van der Velden, W.; Omar, H.; Martino, R.; Halkes, C.; Faraci, M.; et al. Response to Rituximab-Based Therapy and Risk Factor Analysis in Epstein Barr Virus–Related Lymphoproliferative Disorder after Hematopoietic Stem Cell Transplant in Children and Adults: A Study from the Infectious Diseases Working Party of the European Group for Blood and Marrow Transplantation. Clin. Infect. Dis. 2013, 57, 794–802. [Google Scholar] [CrossRef]
- Heslop, H.E. How I Treat EBV Lymphoproliferation. Blood 2009, 114, 4002–4008. [Google Scholar] [CrossRef]
- Morales-Sánchez, A.; Fuentes-Panana, E.M. The Immunomodulatory Capacity of an Epstein-Barr Virus Abortive Lytic Cycle: Potential Contribution to Viral Tumorigenesis. Cancers 2018, 10, 98. [Google Scholar] [CrossRef] [PubMed]
- Stanfield, B.A.; Luftig, M.A. Recent Advances in Understanding Epstein-Barr Virus. F1000Research 2017, 6, 386. [Google Scholar] [CrossRef] [PubMed]
- Hong, G.K.; Gulley, M.L.; Feng, W.-H.; Delecluse, H.-J.; Holley-Guthrie, E.; Kenney, S.C. Epstein-Barr Virus Lytic Infection Contributes to Lymphoproliferative Disease in a SCID Mouse Model. J. Virol. 2005, 79, 13993–14003. [Google Scholar] [CrossRef] [PubMed]
- Ma, S.-D.; Hegde, S.; Young, K.H.; Sullivan, R.; Rajesh, D.; Zhou, Y.; Jankowska-Gan, E.; Burlingham, W.J.; Sun, X.; Gulley, M.L.; et al. A New Model of Epstein-Barr Virus Infection Reveals an Important Role for Early Lytic Viral Protein Expression in the Development of Lymphomas. J. Virol. 2011, 85, 165–177. [Google Scholar] [CrossRef] [PubMed]
- Ma, S.-D.; Yu, X.; Mertz, J.E.; Gumperz, J.E.; Reinheim, E.; Zhou, Y.; Tang, W.; Burlingham, W.J.; Gulley, M.L.; Kenney, S.C. An Epstein-Barr Virus (EBV) Mutant with Enhanced BZLF1 Expression Causes Lymphomas with Abortive Lytic EBV Infection in a Humanized Mouse Model. J. Virol. 2012, 86, 7976–7987. [Google Scholar] [CrossRef] [PubMed]
- Feederle, R.; Kost, M.; Baumann, M.; Janz, A.; Drouet, E.; Hammerschmidt, W.; Delecluse, H.J. The Epstein-Barr Virus Lytic Program Is Controlled by the Co-Operative Functions of Two Transactivators. EMBO J. 2000, 19, 3080–3089. [Google Scholar] [CrossRef]
- Bhende, P.M.; Seaman, W.T.; Delecluse, H.-J.; Kenney, S.C. The EBV Lytic Switch Protein, Z, Preferentially Binds to and Activates the Methylated Viral Genome. Nat. Genet. 2004, 36, 1099–1104. [Google Scholar] [CrossRef]
- Niller, H.-H.; Bauer, G. Epstein-Barr Virus: Clinical Diagnostics. Methods Mol. Biol. 2017, 1532, 33–55. [Google Scholar] [CrossRef]
- Zhang, G.; Li, Z.; Zhou, Q. Utility of Serum EB Virus Zta Antibody in the Diagnostic of Nasopharyngeal Carcinoma: Evidences from 2126 Cases and 15,644 Controls. Front. Oncol. 2019, 9, 1391. [Google Scholar] [CrossRef]
- Gulley, M.L.; Tang, W. Using Epstein-Barr Viral Load Assays to Diagnose, Monitor, and Prevent Posttransplant Lymphoproliferative Disorder. Clin. Microbiol. Rev. 2010, 23, 350–366. [Google Scholar] [CrossRef]
- Bakker, N.A.; van Imhoff, G.W.; Verschuuren, E.A.M.; van Son, W.J. Presentation and Early Detection of Post-Transplant Lymphoproliferative Disorder after Solid Organ Transplantation. Transpl. Int. 2007, 20, 207–218. [Google Scholar] [CrossRef] [PubMed]
- Baldanti, F.; Rognoni, V.; Cascina, A.; Oggionni, T.; Tinelli, C.; Meloni, F. Post-Transplant Lymphoproliferative Disorders and Epstein-Barr Virus DNAemia in a Cohort of Lung Transplant Recipients. Virol. J. 2011, 8, 421. [Google Scholar] [CrossRef] [PubMed]
- Neuringer, I.P. Posttransplant Lymphoproliferative Disease after Lung Transplantation. Clin. Dev. Immunol. 2013, 2013, 430209. [Google Scholar] [CrossRef] [PubMed]
- Oertel, S.; Trappe, R.U.; Zeidler, K.; Babel, N.; Reinke, P.; Hummel, M.; Jonas, S.; Papp-Vary, M.; Subklewe, M.; Dörken, B.; et al. Epstein-Barr Viral Load in Whole Blood of Adults with Posttransplant Lymphoproliferative Disorder after Solid Organ Transplantation Does Not Correlate with Clinical Course. Ann. Hematol. 2006, 85, 478–484. [Google Scholar] [CrossRef] [PubMed]
- Axelrod, D.A.; Holmes, R.; Thomas, S.E.; Magee, J.C. Limitations of EBV-PCR Monitoring to Detect EBV Associated Post-Transplant Lymphoproliferative Disorder. Pediatr. Transpl. 2003, 7, 223–227. [Google Scholar] [CrossRef] [PubMed]
- Gandhi, M.K.; Lambley, E.; Burrows, J.; Dua, U.; Elliott, S.; Shaw, P.J.; Prince, H.M.; Wolf, M.; Clarke, K.; Underhill, C.; et al. Plasma Epstein-Barr Virus (EBV) DNA Is a Biomarker for EBV-Positive Hodgkin’s Lymphoma. Clin. Cancer Res. 2006, 12, 460–464. [Google Scholar] [CrossRef]
- World Health Organization (WHO). The United Network for Organ Sharing (UNOS), 2017; Global Observatory on Donation and Transplantation; WHO: Geneva, Switzerland, 2016. [Google Scholar]
- EBMT Annual Report 2018; European Society for Blood and Marrow Transplantation; EBMT: Barcelona, Spain, 2018.
- Styczynski, J.; Reusser, P.; Einsele, H.; de la Camara, R.; Cordonnier, C.; Ward, K.N.; Ljungman, P.; Engelhard, D. Management of HSV, VZV and EBV Infections in Patients with Hematological Malignancies and after SCT: Guidelines from the Second European Conference on Infections in Leukemia. Bone Marrow Transpl. 2009, 43, 757–770. [Google Scholar] [CrossRef]
- Preiksaitis, J.K.; Pang, X.L.; Fox, J.D.; Fenton, J.M.; Caliendo, A.M.; Miller, G.G. American Society of Transplantation Infectious Diseases Community of Practice Interlaboratory Comparison of Epstein-Barr Virus Viral Load Assays. Am. J. Transpl. 2009, 9, 269–279. [Google Scholar] [CrossRef]
- Tsai, D.E.; Douglas, L.; Andreadis, C.; Vogl, D.T.; Arnoldi, S.; Kotloff, R.; Svoboda, J.; Bloom, R.D.; Olthoff, K.M.; Brozena, S.C.; et al. EBV PCR in the Diagnosis and Monitoring of Posttransplant Lymphoproliferative Disorder: Results of a Two-Arm Prospective Trial. Am. J. Transpl. 2008, 8, 1016–1024. [Google Scholar] [CrossRef]
- Green, M.; Michaels, M.G. Epstein-Barr Virus Infection and Posttransplant Lymphoproliferative Disorder. Am. J. Transpl. 2013, 13 (Suppl. 3), 41–54. [Google Scholar] [CrossRef]
- Kotton, C.N.; Kumar, D.; Caliendo, A.M.; Huprikar, S.; Chou, S.; Danziger-Isakov, L.; Humar, A.; on behalf of the The Transplantation Society International CMV Consensus Group. The Third International Consensus Guidelines on the Management of Cytomegalovirus in Solid-Organ Transplantation. Transplantation 2018, 102, 900–931. [Google Scholar] [CrossRef] [PubMed]
- Pavanello, F.; Zucca, E.; Ghielmini, M. Rituximab: 13 Open Questions after 20 years of Clinical Use. Cancer Treat Rev. 2017, 53, 38–46. [Google Scholar] [CrossRef] [PubMed]
- Barmettler, S.; Ong, M.-S.; Farmer, J.R.; Choi, H.; Walter, J. Association of Immunoglobulin Levels, Infectious Risk, and Mortality With Rituximab and Hypogammaglobulinemia. JAMA Netw. Open 2018, 1, e184169. [Google Scholar] [CrossRef]
- Rea, D.; Fourcade, C.; Leblond, V.; Rowe, M.; Joab, I.; Edelman, L.; Bitker, M.O.; Gandjbakhch, I.; Suberbielle, C.; Farcet, J.P. Patterns of Epstein-Barr Virus Latent and Replicative Gene Expression in Epstein-Barr Virus B Cell Lymphoproliferative Disorders after Organ Transplantation. Transplantation 1994, 58, 317–324. [Google Scholar] [CrossRef] [PubMed]
- Cohen, M.; Vistarop, A.G.; Huaman, F.; Narbaitz, M.; Metrebian, F.; De Matteo, E.; Preciado, M.V.; Chabay, P.A. Epstein-Barr Virus Lytic Cycle Involvement in Diffuse Large B Cell Lymphoma. Hematol. Oncol. 2018, 36, 98–103. [Google Scholar] [CrossRef]
- Fink, S.E.K.; Gandhi, M.K.; Nourse, J.P.; Keane, C.; Jones, K.; Crooks, P.; Jöhrens, K.; Korfel, A.; Schmidt, H.; Neumann, S.; et al. A Comprehensive Analysis of the Cellular and EBV-Specific MicroRNAome in Primary CNS PTLD Identifies Different Patterns among EBV-Associated Tumors. Am. J. Transpl. 2014, 14, 2577–2587. [Google Scholar] [CrossRef]
- Vajro, P.; Lucariello, S.; Migliaro, F.; Sokal, E.; Gridelli, B.; Vegnente, A.; Iorio, R.; Smets, F.; Quinto, I.; Scala, G. Predictive Value of Epstein-Barr Virus Genome Copy Number and BZLF1 Expression in Blood Lymphocytes of Transplant Recipients at Risk for Lymphoproliferative Disease. J. Infect. Dis. 2000, 181, 2050–2054. [Google Scholar] [CrossRef][Green Version]
- Habib, M.; Buisson, M.; Lupo, J.; Agbalika, F.; Socié, G.; Germi, R.; Baccard, M.; Imbert-Marcille, B.-M.; Dantal, J.; Morand, P.; et al. Lytic EBV Infection Investigated by Detection of Soluble Epstein-Barr Virus ZEBRA in the Serum of Patients with PTLD. Sci. Rep. 2017, 7, 10479. [Google Scholar] [CrossRef]
- Caillard, S.; Porcher, R.; Provot, F.; Dantal, J.; Choquet, S.; Durrbach, A.; Morelon, E.; Moal, V.; Janbon, B.; Alamartine, E.; et al. Post-Transplantation Lymphoproliferative Disorder After Kidney Transplantation: Report of a Nationwide French Registry and the Development of a New Prognostic Score. J. Clin. Oncol. 2013, 31, 1302–1309. [Google Scholar] [CrossRef]
- Dharnidharka, V.R.; Webster, A.C.; Martinez, O.M.; Preiksaitis, J.K.; Leblond, V.; Choquet, S. Post-Transplant Lymphoproliferative Disorders. Nat. Rev. Dis. Prim. 2016, 2, 15088. [Google Scholar] [CrossRef]
- Azarfar, A.; Ravanshad, Y.; Mehrad-Majd, H.; Esmaeeli, M.; Aval, S.B.; Emadzadeh, M.; Salehi, M.; Moradi, A.; Golsorkhi, M.; Khazaei, M.R. Comparison of Tacrolimus and Cyclosporine for Immunosuppression after Renal Transplantation: An Updated Systematic Review and Meta-Analysis. Saudi J. Kidney Dis. Transplant. 2018, 29, 1376–1385. [Google Scholar] [CrossRef]
- Wadowsky, R.M.; Laus, S.; Green, M.; Webber, S.A.; Rowe, D. Measurement of Epstein-Barr Virus DNA Loads in Whole Blood and Plasma by TaqMan PCR and in Peripheral Blood Lymphocytes by Competitive PCR. J. Clin. Microbiol. 2003, 41, 5245–5249. [Google Scholar] [CrossRef] [PubMed]
- Frappier, L. Epstein-Barr Virus: Current Questions and Challenges. Tumour Virus Res. 2021, 12, 200218. [Google Scholar] [CrossRef] [PubMed]
- Harris, N.L.; Ferry, J.A.; Swerdlow, S.H. Posttransplant Lymphoproliferative Disorders: Summary of Society for Hematopathology Workshop. Semin. Diagn. Pathol. 1997, 14, 8–14. [Google Scholar] [PubMed]
- Mucha, K.; Foroncewicz, B.; Ziarkiewicz-Wróblewska, B.; Krawczyk, M.; Lerut, J.; Paczek, L. Post-Transplant Lymphoproliferative Disorder in View of the New WHO Classification: A More Rational Approach to a Protean Disease? Nephrol. Dial. Transplant. 2010, 25, 2089–2098. [Google Scholar] [CrossRef]
- Semenova, T.; Lupo, J.; Alain, S.; Perrin-Confort, G.; Grossi, L.; Dimier, J.; Epaulard, O.; Morand, P.; Germi, R. Multicenter Evaluation of Whole-Blood Epstein-Barr Viral Load Standardization Using the WHO International Standard. J. Clin. Microbiol. 2016, 54, 1746–1750. [Google Scholar] [CrossRef]
- Ye, J.; Gradoville, L.; Miller, G. Cellular Immediate-Early Gene Expression Occurs Kinetically Upstream of Epstein-Barr Virus bzlf1 and brlf1 following Cross-Linking of the B Cell Antigen Receptor in the Akata Burkitt Lymphoma Cell Line. J. Virol. 2010, 84, 12405–12418. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Cases (17 Patients) | Controls (91 Patients) | p-Value | ||||
|---|---|---|---|---|---|---|
| F n (%) | M n (%) | 6/11 (55) | 5/11 (45) | 37/91 (41) | 54/91 (59) | 0.5 |
| Age Q2 (Q1–Q3) | 57 (27.5–64.5) | 57 (40–65) | 0.8 | |||
| Organ n (%) | 0.2 | |||||
| Kidney | 7 (41%) | 20 (22%) | 0.1 | |||
| Lung | 3 (18%) | 33 (36%) | 0.2 | |||
| HSCs | 7 (41%) | 38 (42%) | 1 | |||
| Risk Factor n (%) | ||||||
| Mismatch EBV D/R | 4/9 (44%) | 5/50(10%) | 0.02 | |||
| T-cell depletion | 3/8 (38%) | 12/29 (41%) | 1 | |||
| Mismatch HLA D/R | 9/12 (75%) | 28/33 (85%) | 0.7 | |||
| Anti-CMV n (%) | 4/11 (36%) | 20/32 (63%) | 0.2 | |||
| Anti-Rejection (IS) n (%) | ||||||
| Ciclosporin | 13/16 (81%) | |||||
| Tacrolimus | 2/16 (12.5%) | 56/59 (95%) | <0.0001 | |||
| Everolimus | 1/15 (7%) | 10/53 (17%) | 0.4 | |||
| Mycophenolate mofetil | 9/15 (67%) | 40/53 (75.5%) | 0.3 | |||
| Methotrexate | 3/15 (20%) | |||||
| Azathioprine | 1/15 (7%) | 4/53 (7.5%) | 1 | |||
| Corticosteroids | 11/11 (100%) | 43/44 (98%) | 1 | |||
| Everolimus | 1/44 (2%) | |||||
| Time to PTLD, Month Q2 (Q1–Q3) | ||||||
| HSCs | 4 (3–5.3) | |||||
| Lung | 19 (2–134) | |||||
| Kidney | 98 (37–190) | |||||
| Histology n (%) | ||||||
| Morphology | ||||||
| IM-like | 1/17 (5.9%) | |||||
| DLBCL | 13/17 (76%) | |||||
| Burkitt Lymphoma | 1/17 (5.9%) | |||||
| T Lymphoma | 1/17 (5.9%) | |||||
| Hodgkin disease | 1/17 (5.9%) | |||||
| EBV status in tumor | ||||||
| EBV + | 6/10 (60%) | |||||
| EBV − | 4/10 (40%) | |||||
| PTLD Treatment | ||||||
| Rituximab | 5/12 (42%) | |||||
| Rituximab + Chemotherapy | 5/12 (42%) | |||||
| Chemotherapy | 2/12 (16%) | |||||
| Patient | Gender/Age | Organ | Histology/EBV Status | EBV D/R | Time to PTLD | sZEBRA | EBV DNAemia |
|---|---|---|---|---|---|---|---|
| GACY1004 | 21 | Lung | DLBCL/? | +/− | 2 m (E) | + | − |
| PTLD 2 | F/62 | HSCs | DLBCL/+ | +/+ | 4 m (E) | + | + |
| PTLD 3 | M/21 | Lung | DLBCL/+ | ?/+ | 1.5 y (L) | − | − |
| PTLD 4 | F/70 | Lung | DLBCL/+ | ?/+ | 11 y (L) | + | + |
| PTLD 5 | M/19 | Kidney | DLBCL/+ | −/+ | 8 y (L) | + | + |
| PTLD 6 | F/56 | HSCs | IM-like | +/+ | 3 m (E) | + | + |
| PTLD 7 | F/47 | Kidney | DLBCL/+ | +/− | 3 y (L) | + | + |
| PR1 | M/57 | Kidney | T Ly/− | 16 y (L) | + | − | |
| MS2 | F/69 | Kidney | DLBCL/− | +/+ | 6 m (E) | + | − |
| PV3 | F/64 | Kidney | Burkitt/− | +/+ | 11 y (L) | + | − |
| ZA4 | M/53 | Kidney | Hodgkin/+ | −/+ | 19 y (L) | + | + |
| CA5 | M58 | Kidney | DLBCL/− | +/+ | 8 y (L) | + | − |
| R5934 | M/75 | HSCs | DLBCL/+ | ?/+ | 1 m(E) | − | ND |
| R3338 | M/34 | HSCs | DLBCL/+ | ?/+ | 6 m (E) | + | ND |
| R1192 | M/18 | HSCs | DLBCL/+ | ?/+ | 4 m (E) | + | ND |
| R2530 | F/64 | HSCs | DLBCL/+ | ?/+ | 4.5 m (E) | + | ND |
| R1767 | F/65 | HSCs | DLBCL/+ | ?/+ | 5 m (E) | − | ND |
| EBV Markers | Cases | Controls | p-Value | |
|---|---|---|---|---|
| Positive whole blood EBV DNA load n (%) | 6/12 (50.0%) | 42/91 (46.2%) | 0.22 | |
| EBV DNA in whole blood, UI/mL | Median [IQR] | 0 [0, 1500] | 0 [0, 1246] | |
| Mean (+/− SD) | 1000 (+/− 1000) | 3509 (+/− 1241) | 0.26 | |
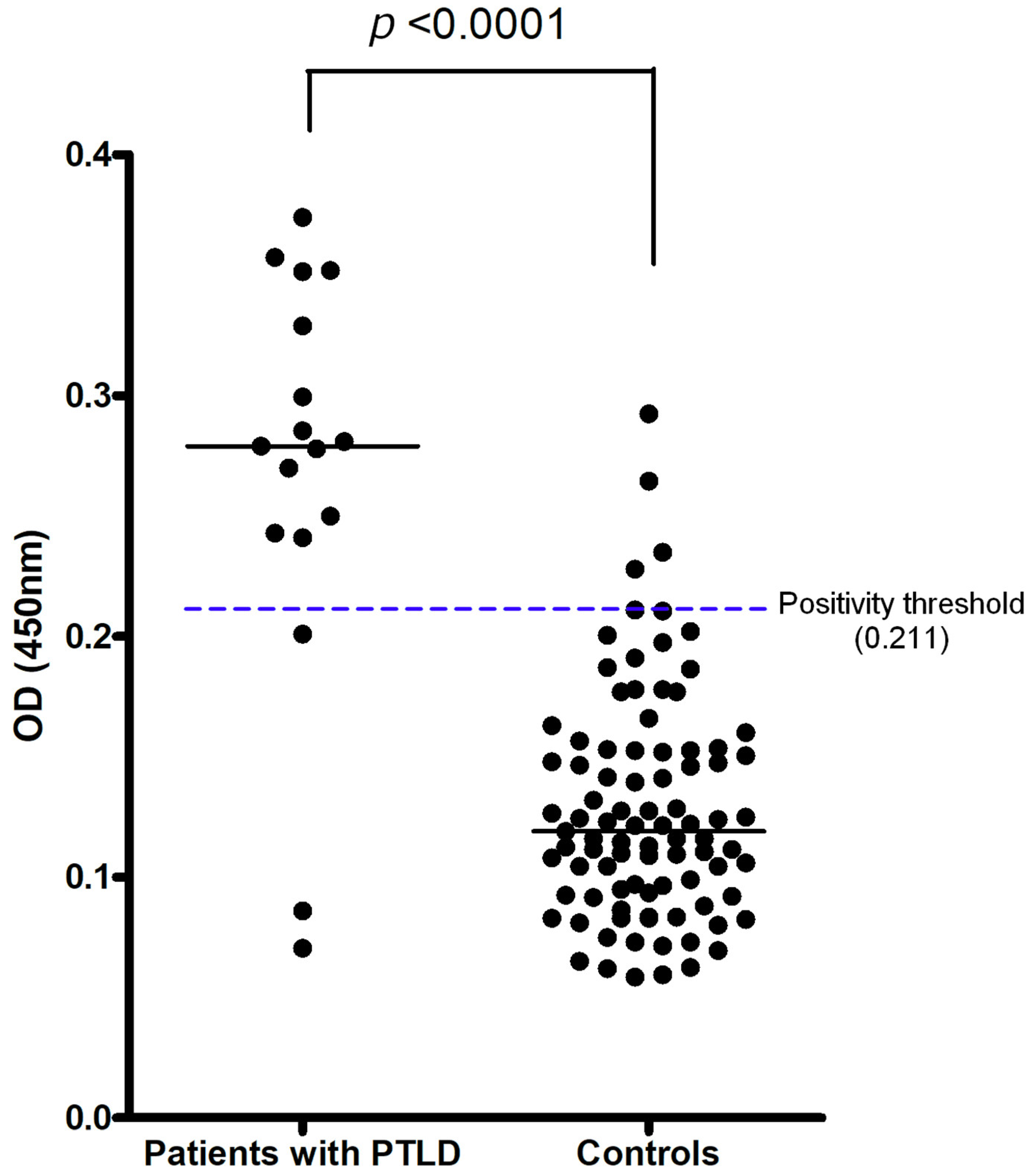
| Detectable sZEBRA antigen n (%) | 14/17 (82.4%) | 5/91 (5.5%) | <0.0001 | |
| sZEBRA, OD450 | Median [IQR] | 0.28 [0.24, 0.34] | 0.12 [0.09, 0.15] | |
| Mean (+/− SD) | 0.27 (+/− 0.02) | 0.13 (+/− 0.01) | <0.0001 | |
| Threshold | Sensitivity % | Specificity % | Relative Prevalence % | PPV % | NPV % |
|---|---|---|---|---|---|
| OD = 0.211 (Mean + 2SD) | 82.35 (95% CI [58.97, 93.81]) | 94.51 (95% CI [87.78, 97.63]) | 1 | 14.2 | 99.8 |
| 16 | 74 | 97 | |||
| OD = 0.259 (Mean + 3SD) | 64.71 (95% CI [41.30, 82.69]) | 97.80 (95% CI [92.34, 99.61]) | 1 | 24.8 | 99.6 |
| 16 | 85 | 94 |
| Center | Transplantation | Number of Samples Cases |
|---|---|---|
| A | Pulmonary | 1 |
| B | Renal | 5 |
| C | HSCs | 5 |
| D | Pulmonary, renal, HSCs | 6 (2, 2, 2) |
| TOTAL: | 17 | |
| E | Number of Samples Controls | |
| HSCs | 38 | |
| Renal | 20 | |
| Pulmonary | 33 | |
| TOTAL: | 91 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lupo, J.; Wielandts, A.-S.; Buisson, M.; Consortium, C.; Habib, M.; Hamoudi, M.; Morand, P.; Verduyn-Lunel, F.; Caillard, S.; Drouet, E. High Predictive Value of the Soluble ZEBRA Antigen (Epstein-Barr Virus Trans-Activator Zta) in Transplant Patients with PTLD. Pathogens 2022, 11, 928. https://doi.org/10.3390/pathogens11080928
Lupo J, Wielandts A-S, Buisson M, Consortium C, Habib M, Hamoudi M, Morand P, Verduyn-Lunel F, Caillard S, Drouet E. High Predictive Value of the Soluble ZEBRA Antigen (Epstein-Barr Virus Trans-Activator Zta) in Transplant Patients with PTLD. Pathogens. 2022; 11(8):928. https://doi.org/10.3390/pathogens11080928
Chicago/Turabian StyleLupo, Julien, Anne-Sophie Wielandts, Marlyse Buisson, CRYOSTEM Consortium, Mohammed Habib, Marwan Hamoudi, Patrice Morand, Frans Verduyn-Lunel, Sophie Caillard, and Emmanuel Drouet. 2022. "High Predictive Value of the Soluble ZEBRA Antigen (Epstein-Barr Virus Trans-Activator Zta) in Transplant Patients with PTLD" Pathogens 11, no. 8: 928. https://doi.org/10.3390/pathogens11080928
APA StyleLupo, J., Wielandts, A.-S., Buisson, M., Consortium, C., Habib, M., Hamoudi, M., Morand, P., Verduyn-Lunel, F., Caillard, S., & Drouet, E. (2022). High Predictive Value of the Soluble ZEBRA Antigen (Epstein-Barr Virus Trans-Activator Zta) in Transplant Patients with PTLD. Pathogens, 11(8), 928. https://doi.org/10.3390/pathogens11080928