
Long-Term Sequelae of COVID-19: A Systematic Review and Meta-Analysis of One-Year Follow-Up Studies on Post-COVID Symptoms


Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion/Exclusion Criteria
2.3. Data Extraction
2.4. Study Quality Assessment
2.5. Statistical Analyses
3. Results
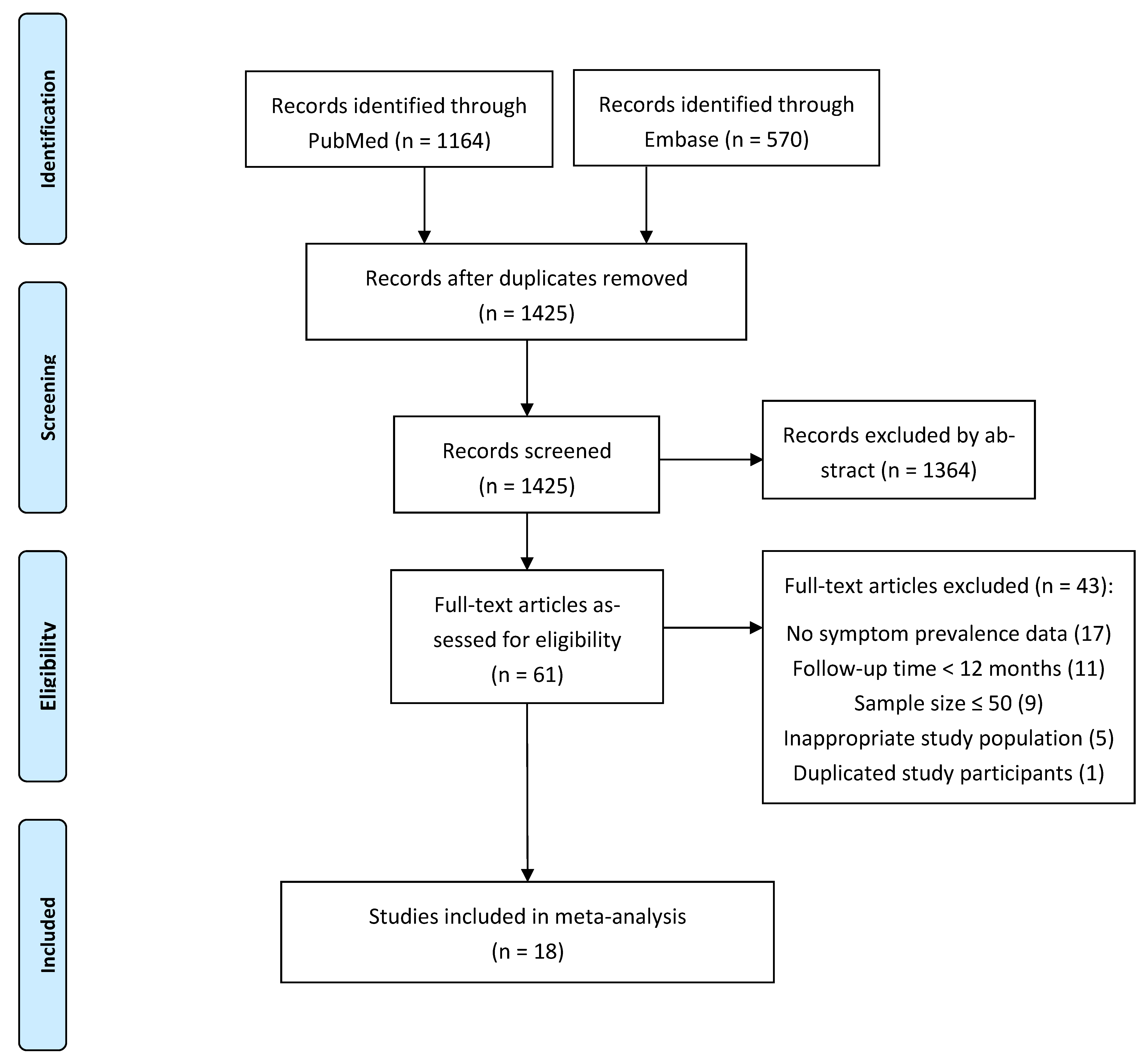
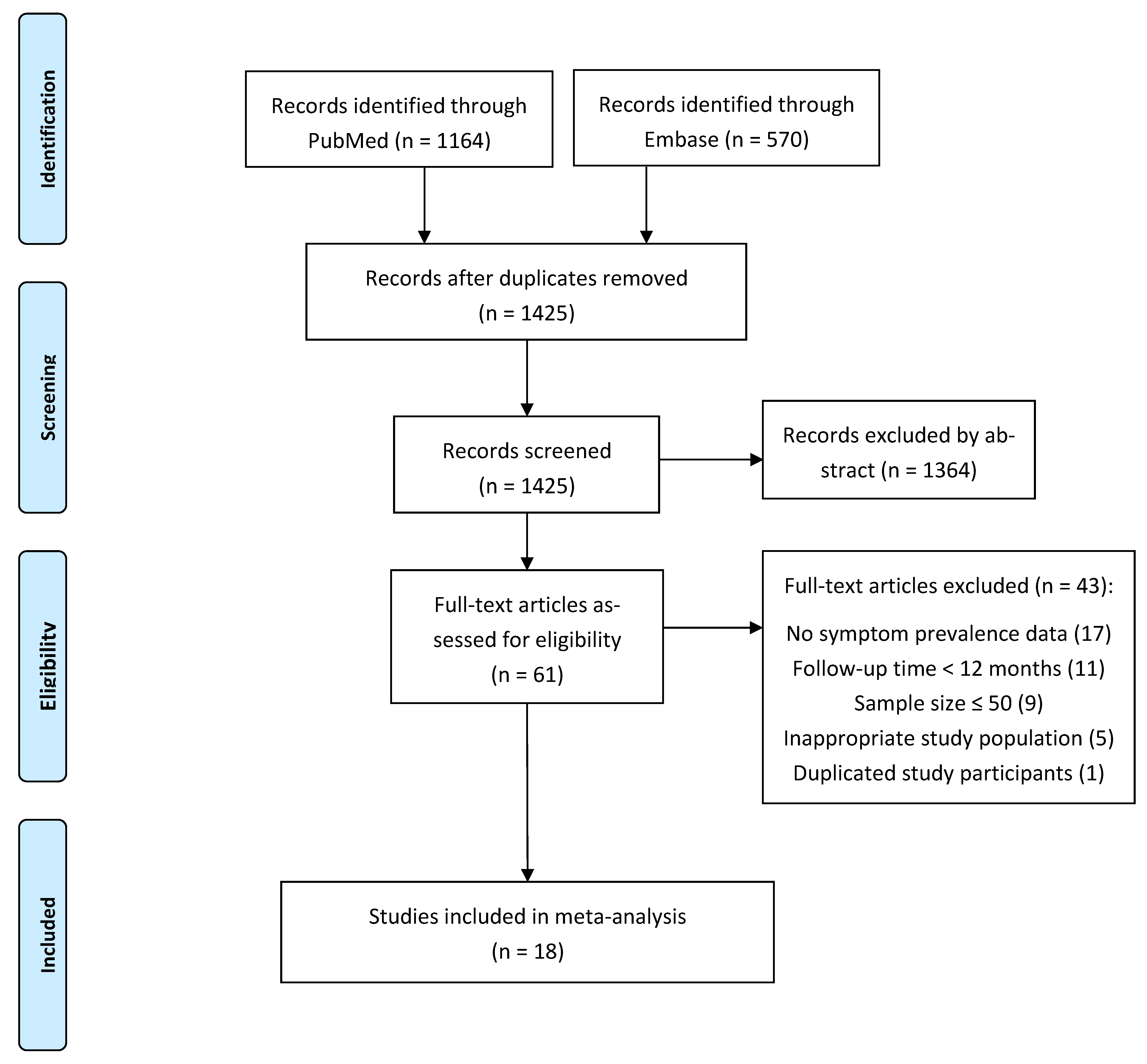
3.1. Search Results and Study Characteristics

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author | Sample Size | Country | Mean/Median Age, Year | Only Adults | Male Proportion | Scale for Symptoms | Single-/Multi-Centre | Hospitalisation | Follow-Up Method | Follow-Up Period |
|---|---|---|---|---|---|---|---|---|---|---|
| Boscolo-Rizzo, P. [20] | 304 | Italy | 47 | Yes | 0.39 | Acute Respiratory Tract Infection Questionnaire | single centre | non-hospitalised | phone | 12 months after symptom onset |
| Boscolo-Rizzo, P. [9] | 100 | Italy | 49 | Yes | 0.61 | 5-item World Health Organization Wellbeing Index, Acute Respiratory Tract Infection Questionnaire | multi-centre | non-hospitalised | in-person visit | median of 401 days from the first SARS-CoV-2 positive swab |
| Catalán, I. P. [21] | 76 | Spain | 64 | Yes | 0.62 | - | single centre | hospitalised | phone | one year after hospital admission |
| Chai, C. [22] | 432 | China | 65 | - | 0.49 | - | multi-centre | hospitalised | in-person visit | median follow-up time from hospital admission was 12.2 (IQR 12.1-12.6) months |
| Fernández-de-las-Peñas, C. [23] | 1950 | Spain | 61 | - | 0.53 | - | multi-centre | hospitalised | phone | one year after hospital discharge |
| Gamberini, L. [24] | 178 | Italy | 64 | - | 0.73 | mMRC | multi-centre | ICU | in-person visit | one year after ICU discharge |
| Huang, L. [25] | 1272 | China | 59 | Yes | 0.53 | mMRC | single centre | hospitalised | in-person visit | 12 months after symptom onset |
| Latronico, N. [26] | 51 | Italy | 60 | Yes | 0.77 | Fatigue Severity Score, Montreal Cognitive Assessment, Hospital Anxiety and Depression Scale subscales, PTSD checklist for DSM-5, Insomnia Severity Index | single centre | ICU | in-person visit | 12 months after ICU discharge |
| Liu, T. [27] | 486 | China | 63 | - | 0.46 | - | single centre | hospitalised | in-person visit | 12 months after discharge |
| Maestre-Muñiz, M. M. [28] | 543 | Spain | 65 | Yes | - | - | single centre | mixed | phone | 12 months after discharge |
| Maestrini, V. [29] | 118 | Italy | 71 | - | 0.57 | - | single centre | hospitalised | phone | mean of 347 ± 10 days from COVID-19 diagnosis |
| Méndez, R. [30] | 171 | Spain | 58 | Yes | 0.58 | a battery of standardised instruments for the cognitive functioning; subjective cognitive complaints; anxiety, depression, and PTSD | single centre | hospitalised | phone | 12 (±1) months after hospital discharge |
| Rank, A. [31] | 83 | Germany | 42 | Yes | 0.76 | - | single centre | mixed | in-person visit | 12 months after onset of COVID-19 |
| Seeßle, J. [32] | 96 | Germany | 57 | Yes | 0.45 | - | single centre | mixed | in-person visit | 12 months after symptom onset |
| Wu, X. [33] | 83 | China | 60 | Yes | 0.57 | mMRC | single centre | hospitalised | in-person visit | 12 months after discharge |
| Zhan, Y. [34] | 121 | China | 49 | Yes | 0.41 | - | single centre | hospitalised | in-person visit | one year after diagnosis |
| Zhang, X. [35] | 2433 | China | 60 | Yes | 0.50 | - | multi-centre | hospitalised | phone | median (IQR) time from discharge to follow-up was 364 (357–371) days |
| Zhao, Y. [36] | 94 | China | 48 | Yes | 0.57 | 14-item Hamilton Anxiety Rating Scale, 24-item Hamilton Depression Rating Scale, mMRC | multi-centre | hospitalised | in-person visit | median duration from symptom onset to follow-up visit was 366 (355, 376) days; median time from hospital discharge to follow-up visit was 345 (333, 349) days. |
3.2. Assessment of Risk of Bias
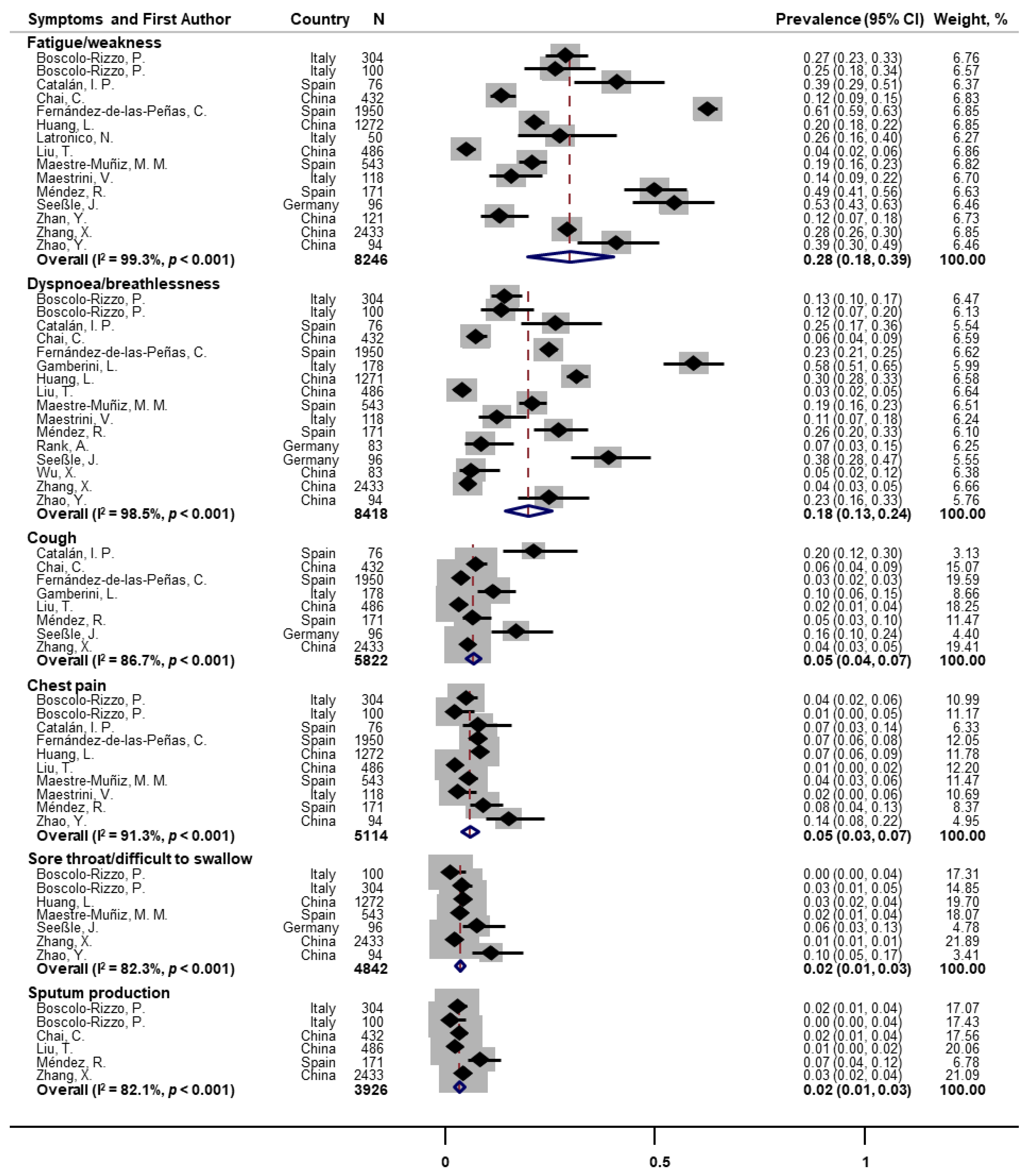
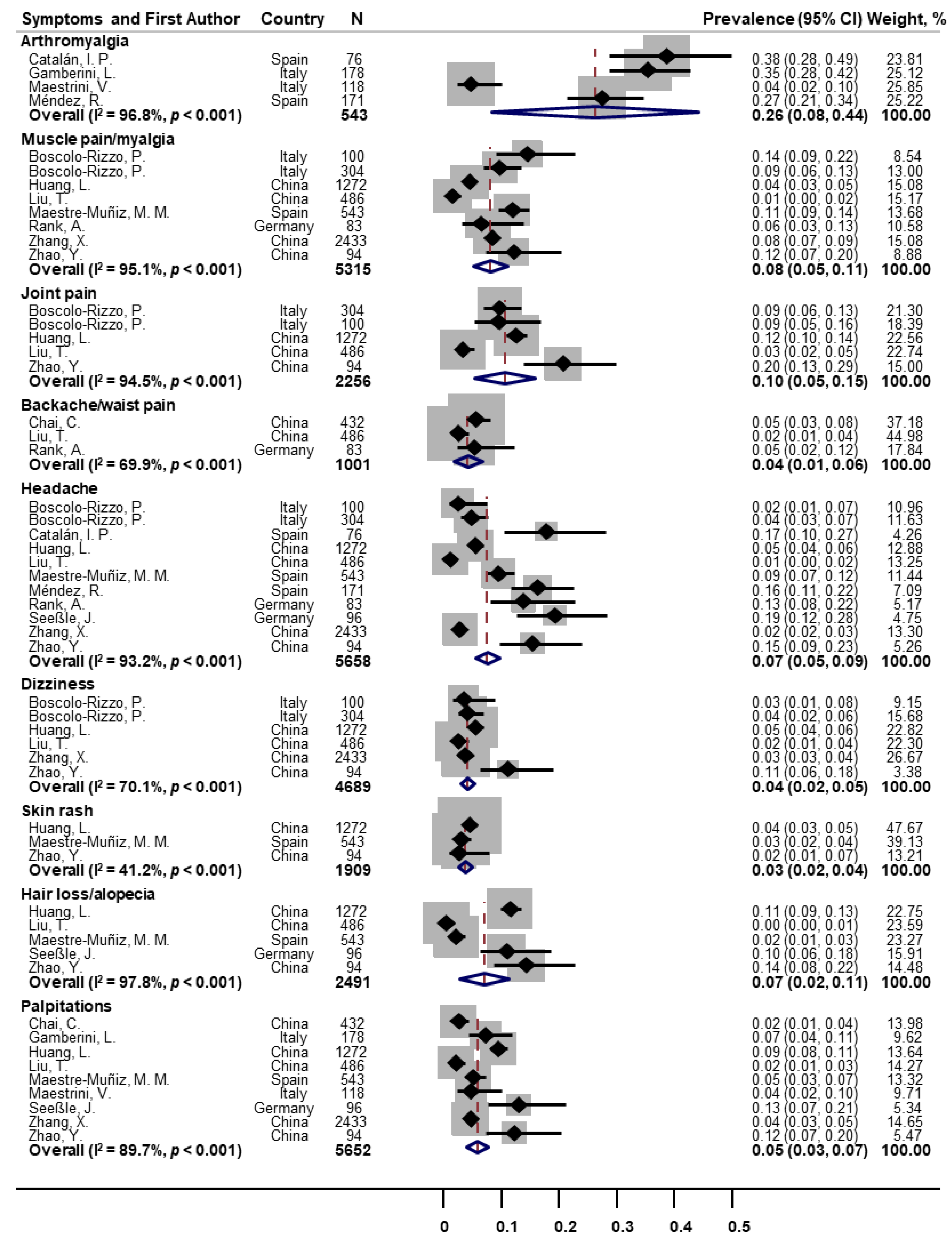
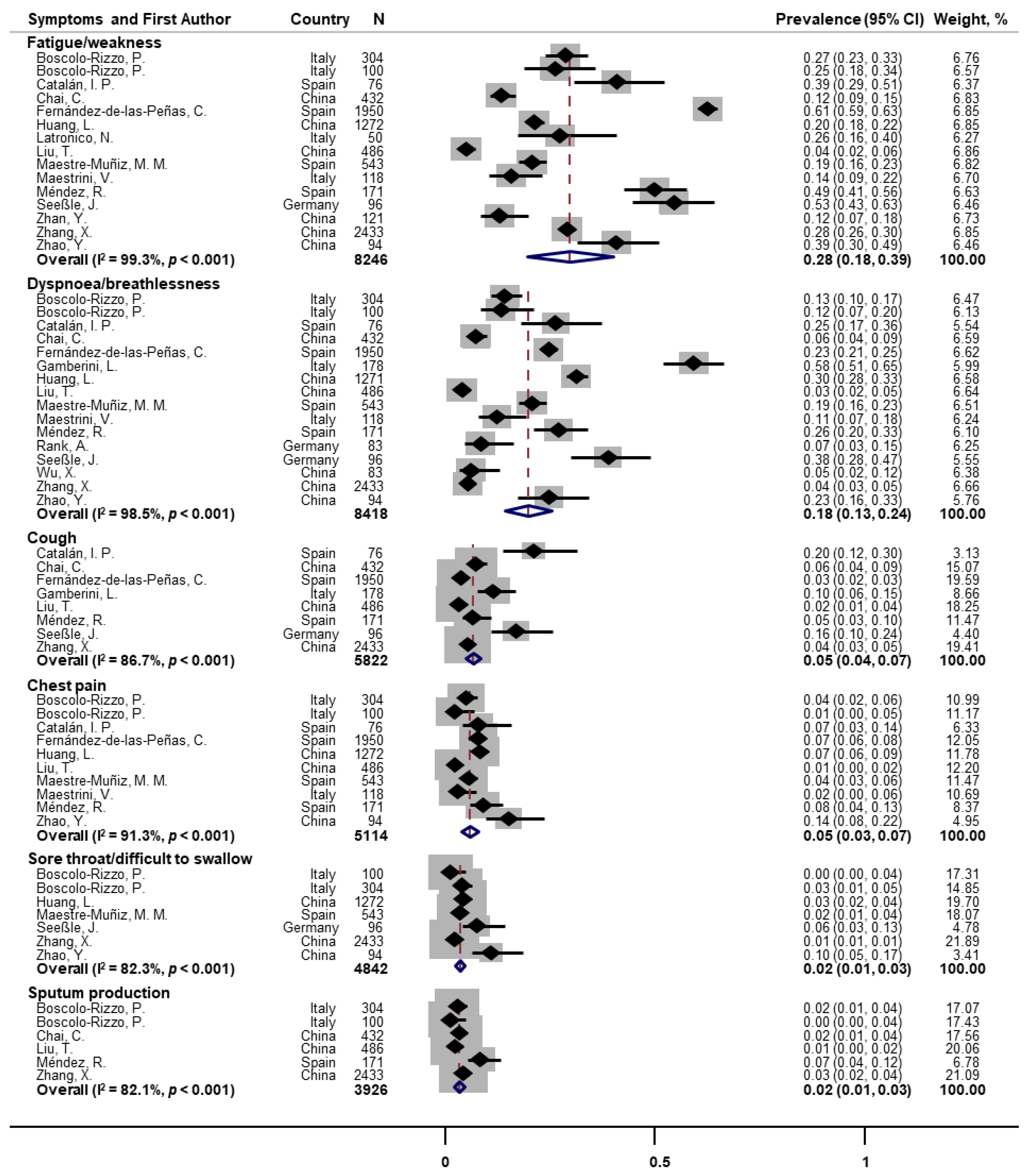
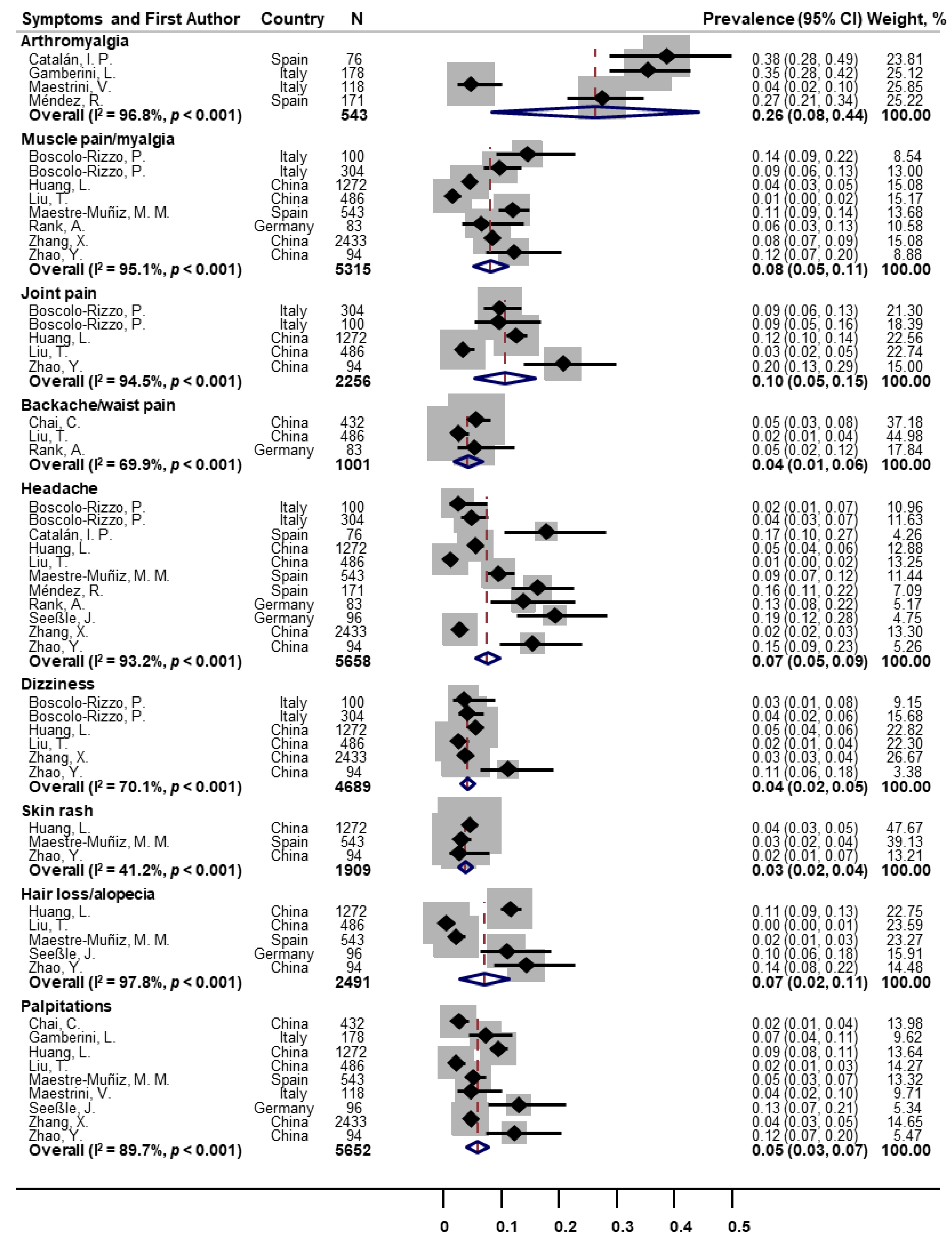
3.3. Prevalence of One-Year Post-COVID Symptoms among COVID-19 Survivors
3.4. Evidence of Risk Factors for One-Year Post-COVID Symptoms
4. Discussion
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization. World Health Organization (WHO) Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 17 January 2022).
- Lopez-Leon, S.; Wegman-Ostrosky, T.; Perelman, C.; Sepulveda, R.; Rebolledo, P.A.; Cuapio, A.; Villapol, S. More than 50 long-term effects of COVID-19: A systematic review and meta-analysis. Sci. Rep. 2021, 11, 16144. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Health and Care Excellence. COVID-19 Rapid Guideline: Managing the Long-Term Effects of COVID-19. Available online: https://www.nice.org.uk/guidance/ng188 (accessed on 17 January 2022).
- Fernandez-de-Las-Penas, C.; Palacios-Cena, D.; Gomez-Mayordomo, V.; Florencio, L.L.; Cuadrado, M.L.; Plaza-Manzano, G.; Navarro-Santana, M. Prevalence of post-COVID-19 symptoms in hospitalized and non-hospitalized COVID-19 survivors: A systematic review and meta-analysis. Eur. J. Intern. Med. 2021, 92, 55–70. [Google Scholar] [CrossRef] [PubMed]
- Michelen, M.; Manoharan, L.; Elkheir, N.; Cheng, V.; Dagens, A.; Hastie, C.; O’Hara, M.; Suett, J.; Dahmash, D.; Bugaeva, P.; et al. Characterising long COVID: A living systematic review. BMJ Glob. Health 2021, 6, e005427. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Munn, Z.; Moola, S.; Lisy, K.; Riitano, D.; Tufanaru, C. Methodological guidance for systematic reviews of observational epidemiological studies reporting prevalence and cumulative incidence data. Int. J. Evid. Based Healthc. 2015, 13, 147–153. [Google Scholar] [CrossRef] [PubMed]
- Nyaga, V.N.; Arbyn, M.; Aerts, M. Metaprop: A Stata command to perform meta-analysis of binomial data. Arch. Public Health 2014, 72, 39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boscolo-Rizzo, P.; Hummel, T.; Hopkins, C.; Dibattista, M.; Menini, A.; Spinato, G.; Fabbris, C.; Emanuelli, E.; D’Alessandro, A.; Marzolino, R.; et al. High prevalence of long-term olfactory, gustatory, and chemesthesis dysfunction in post-COVID-19 patients: A matched case-control study with one-year follow-up using a comprehensive psychophysical evaluation. Rhinology 2021, 59, 517–527. [Google Scholar] [CrossRef]
- Aabenhus, R.; Thorsen, H.; Siersma, V.; Brodersen, J. The development and validation of a multidimensional sum-scaling questionnaire to measure patient-reported outcomes in acute respiratory tract infections in primary care: The acute respiratory tract infection questionnaire. Value Health 2013, 16, 987–992. [Google Scholar] [CrossRef] [Green Version]
- Topp, C.W.; Ostergaard, S.D.; Sondergaard, S.; Bech, P. The WHO-5 Well-Being Index: A systematic review of the literature. Psychother. Psychosom. 2015, 84, 167–176. [Google Scholar] [CrossRef]
- Mahler, D.A.; Wells, C.K. Evaluation of clinical methods for rating dyspnea. Chest 1988, 93, 580–586. [Google Scholar] [CrossRef] [Green Version]
- Krupp, L.B.; LaRocca, N.G.; Muir-Nash, J.; Steinberg, A.D. The fatigue severity scale. Application to patients with multiple sclerosis and systemic lupus erythematosus. Arch. Neurol. 1989, 46, 1121–1123. [Google Scholar] [CrossRef] [PubMed]
- Nasreddine, Z.S.; Phillips, N.A.; Bedirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef] [PubMed]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta. Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamilton, M. The assessment of anxiety states by rating. Br. J. Med. Psychol. 1959, 32, 50–55. [Google Scholar] [CrossRef]
- Hamilton, M. A rating scale for depression. J. Neurol. Neurosurg. Psychiatry 1960, 23, 56–62. [Google Scholar] [CrossRef] [Green Version]
- Blevins, C.A.; Weathers, F.W.; Davis, M.T.; Witte, T.K.; Domino, J.L. The Posttraumatic Stress Disorder Checklist for DSM-5 (PCL-5): Development and Initial Psychometric Evaluation. J. Trauma. Stress 2015, 28, 489–498. [Google Scholar] [CrossRef]
- Bastien, C.H.; Vallieres, A.; Morin, C.M. Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep Med. 2001, 2, 297–307. [Google Scholar] [CrossRef]
- Boscolo-Rizzo, P.; Guida, F.; Marcuzzo, A.V.; D’Alessandro, A.; Zanelli, E.; Marzolino, R.; Lazzarin, C.; Antonucci, P.; Sacchet, E.; Tofanelli, M.; et al. Sequelae in adults at 12 months after mild-to-moderate coronavirus disease 2019 (COVID-19). Int. Forum Allergy Rhinol. 2021, 59, 517–527. [Google Scholar] [CrossRef]
- Catalan, I.P.; Marti, C.R.; Sota, D.P.; Alvarez, A.C.; Gimeno, M.J.E.; Juana, S.F.; Rodriguez, G.H.; Bajo, E.D.; Gaya, N.T.; Blasco, J.U.; et al. Corticosteroids for COVID-19 symptoms and quality of life at 1 year from admission. J. Med. Virol. 2022, 94, 205–210. [Google Scholar] [CrossRef]
- Chai, C.; Feng, X.; Lu, M.; Li, S.; Chen, K.; Wang, H.; Wang, W.; Tang, Z.; Cheng, G.; Wu, X.; et al. One-year mortality and consequences of COVID-19 in cancer patients: A cohort study. IUBMB Life 2021, 73, 1244–1256. [Google Scholar] [CrossRef]
- Fernández-de-Las-Peñas, C.; Guijarro, C.; Plaza-Canteli, S.; Hernández-Barrera, V.; Torres-Macho, J. Prevalence of Post-COVID-19 Cough One Year After SARS-CoV-2 Infection: A Multicenter Study. Lung 2021, 199, 249–253. [Google Scholar] [CrossRef] [PubMed]
- Gamberini, L.; Mazzoli, C.A.; Gordini, G.; Prediletto, I.; Sintonen, H.; Scaramuzzo, G.; Volta, C.A.; Spadaro, S.; Allegri, D.; Colombo, D.; et al. Health-related quality of life profiles, trajectories, persistent symptoms and pulmonary function one year after ICU discharge in invasively ventilated COVID-19 patients, a prospective follow-up study. Respir. Med. 2021, 189, 106665. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.; Yao, Q.; Gu, X.; Wang, Q.; Ren, L.; Wang, Y.; Hu, P.; Guo, L.; Liu, M.; Xu, J.; et al. 1-year outcomes in hospital survivors with COVID-19: A longitudinal cohort study. Lancet 2021, 398, 747–758. [Google Scholar] [CrossRef]
- Latronico, N.; Peli, E.; Calza, S.; Rodella, F.; Novelli, M.P.; Cella, A.; Marshall, J.; Needham, D.M.; Rasulo, F.A.; Piva, S. Physical, cognitive and mental health outcomes in 1-year survivors of COVID-19-associated ARDS. Thorax 2022, 77, 300–303. [Google Scholar] [CrossRef]
- Liu, T.; Wu, D.; Yan, W.; Wang, X.; Zhang, X.; Ma, K.; Chen, H.; Zeng, Z.; Wang, H.; Xing, M.; et al. Twelve-month systemic consequences of COVID-19 in patients discharged from hospital: A prospective cohort study in Wuhan, China. Clin. Infect. Dis. 2021, ciab703. [Google Scholar] [CrossRef]
- Maestre-Muniz, M.M.; Mata-Vazquez, E.; Martin-Toledano, M.; Lopez-Larramona, G.; Ruiz-Chicote, A.M.; Nieto-Sandoval, B.; Arias, A.; Lucendo, A.J. Long-term outcomes of patients with coronavirus disease 2019 at one year after hospital discharge. J. Clin. Med. 2021, 10, 2945. [Google Scholar] [CrossRef]
- Maestrini, V.; Birtolo, L.I.; Francone, M.; Galardo, G.; Galea, N.; Severino, P.; Alessandri, F.; Colaiacomo, M.C.; Cundari, G.; Chimenti, C.; et al. Cardiac involvement in consecutive unselected hospitalized COVID-19 population: In-hospital evaluation and one-year follow-up. Int. J. Cardiol. 2021, 339, 235–242. [Google Scholar] [CrossRef]
- Mendez, R.; Balanza-Martinez, V.; Luperdi, S.C.; Estrada, I.; Latorre, A.; Gonzalez-Jimenez, P.; Bouzas, L.; Yepez, K.; Ferrando, A.; Reyes, S.; et al. Long-term neuropsychiatric outcomes in COVID-19 survivors: A 1-year longitudinal study. J. Intern. Med. 2022, 291, 247–251. [Google Scholar] [CrossRef]
- Rank, A.; Tzortzini, A.; Schmid, C.; Claus, R.; Kling, E.; Loll, E.; Hoffmann, R.; Dennehy, K.M.; Burger, R.; Grutzner, S.; et al. One year after mild covid-19: The majority of patients maintain specific immunity, but one in four still suffer from long-term symptoms. J. Clin. Med. 2021, 10, 3305. [Google Scholar] [CrossRef]
- Seeßle, J.; Hippchen, T.; Lim, A.; Merle, U.; Waterboer, T.; Simon, J.; Kirchner, M.; Muller, B. Persistent symptoms in adult patients one year after COVID-19: A prospective cohort study. Clin. Infect. Dis. 2021, ciab611. [Google Scholar] [CrossRef]
- Wu, X.; Liu, X.; Zhou, Y.; Yu, H.; Li, R.; Zhan, Q.; Ni, F.; Fang, S.; Lu, Y.; Ding, X.; et al. 3-month, 6-month, 9-month, and 12-month respiratory outcomes in patients following COVID-19-related hospitalisation: A prospective study. Lancet Respir. Med. 2021, 9, 747–754. [Google Scholar] [CrossRef]
- Zhan, Y.; Zhu, Y.; Wang, S.; Jia, S.; Gao, Y.; Lu, Y.; Zhou, C.; Liang, R.; Sun, D.; Wang, X.; et al. SARS-CoV-2 immunity and functional recovery of COVID-19 patients 1-year after infection. Signal Transduct. Target. Ther. 2021, 6, 368. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Wang, F.; Shen, Y.; Zhang, X.; Cen, Y.; Wang, B.; Zhao, S.; Zhou, Y.; Hu, B.; Wang, M.; et al. Symptoms and Health Outcomes Among Survivors of COVID-19 Infection 1 Year After Discharge From Hospitals in Wuhan, China. JAMA Netw. Open 2021, 4, e2127403. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Yang, C.; An, X.; Xiong, Y.; Huang, L.; Jia, J.; Xu, Q.; Zhang, L.; Zhao, J.; Xu, A.; et al. Follow-up study on COVID-19 survivors one year after discharge from hospital. Int. J. Infect. Dis. 2021, 112, 173–182. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Symptoms of COVID-19. Available online: https://www.cdc.gov/coronavirus/2019-ncov/symptoms-testing/symptoms.html (accessed on 17 January 2022).
- Yusuf, F.; Fahriani, M.; Mamada, S.S.; Frediansyah, A.; Abubakar, A.; Maghfirah, D.; Fajar, J.K.; Maliga, H.A.; Ilmawan, M.; Emran, T.B.; et al. Global prevalence of prolonged gastrointestinal symptoms in COVID-19 survivors and potential pathogenesis: A systematic review and meta-analysis. F1000Res 2021, 10, 301. [Google Scholar] [CrossRef]
- Wynberg, E.; van Willigen, H.D.G.; Dijkstra, M.; Boyd, A.; Kootstra, N.A.; van den Aardweg, J.G.; van Gils, M.J.; Matser, A.; de Wit, M.R.; Leenstra, T.; et al. Evolution of COVID-19 symptoms during the first 12 months after illness onset. Clin. Infect. Dis. 2021, ciab759. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Han, Q.; Zheng, B.; Daines, L.; Sheikh, A. Long-Term Sequelae of COVID-19: A Systematic Review and Meta-Analysis of One-Year Follow-Up Studies on Post-COVID Symptoms. Pathogens 2022, 11, 269. https://doi.org/10.3390/pathogens11020269
Han Q, Zheng B, Daines L, Sheikh A. Long-Term Sequelae of COVID-19: A Systematic Review and Meta-Analysis of One-Year Follow-Up Studies on Post-COVID Symptoms. Pathogens. 2022; 11(2):269. https://doi.org/10.3390/pathogens11020269
Chicago/Turabian StyleHan, Qing, Bang Zheng, Luke Daines, and Aziz Sheikh. 2022. "Long-Term Sequelae of COVID-19: A Systematic Review and Meta-Analysis of One-Year Follow-Up Studies on Post-COVID Symptoms" Pathogens 11, no. 2: 269. https://doi.org/10.3390/pathogens11020269
APA StyleHan, Q., Zheng, B., Daines, L., & Sheikh, A. (2022). Long-Term Sequelae of COVID-19: A Systematic Review and Meta-Analysis of One-Year Follow-Up Studies on Post-COVID Symptoms. Pathogens, 11(2), 269. https://doi.org/10.3390/pathogens11020269