
Evaluation of Eosinophilic Cationic Protein as a Marker of Alveolar and Cystic Echinococcosis

 , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Inclusion and Exclusion Criteria
2.2. Demographic Data
2.3. Interventions and Imaging
2.4. ECP Measurement
2.5. Statistical Analysis
3. Results
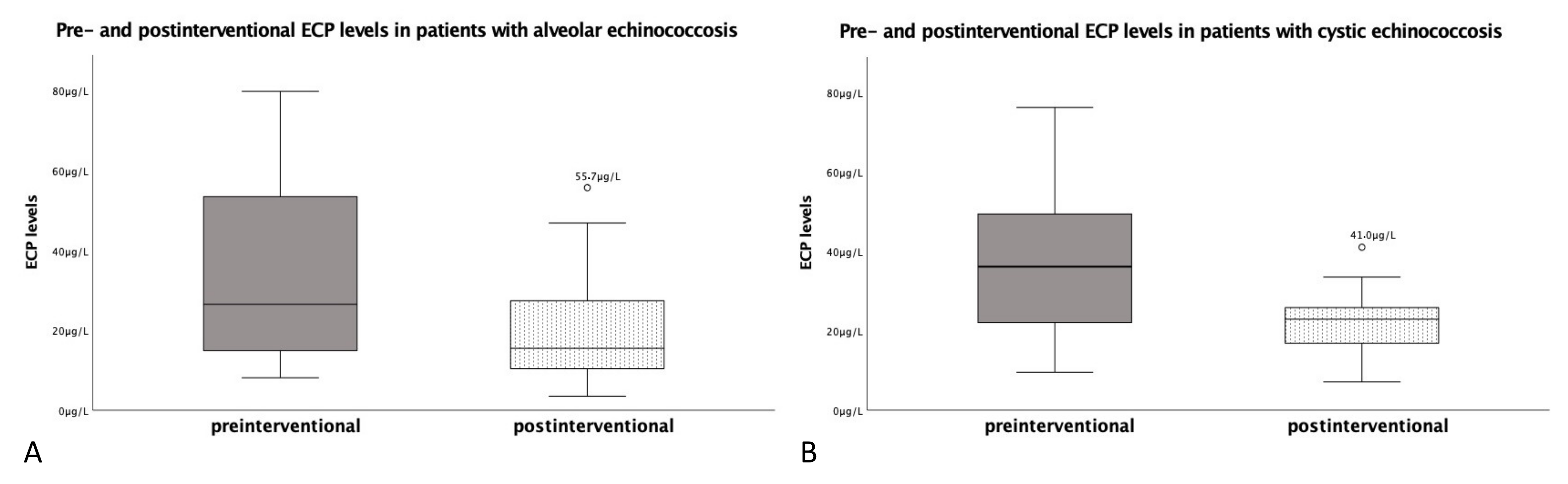
3.1. Eosinophilic Cationic Protein in Patients with Alveolar Echinococcosis
3.2. Eosinophilic Cationic Protein in Patients with Cystic Echinococcosis
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Deplazes, P.; Rinaldi, L.; Alvarez Rojas, C.A.; Torgerson, P.R.; Harandi, M.F.; Romig, T.; Antolova, D.; Schurer, J.M.; Lahmar, S.; Cringoli, G.; et al. Global Distribution of Alveolar and Cystic Echinococcosis. Adv. Parasitol. 2017, 95, 315–493. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kern, P.; Bardonnet, K.; Renner, E.; Auer, H.; Pawlowski, Z.; Ammann, R.W.; Vuitton, D.A.; Kern, P. European echinococcosis registry: Human alveolar echinococcosis, Europe, 1982–2000. Emerg. Infect. Dis. 2003, 9, 343–349. [Google Scholar] [CrossRef] [PubMed]
- Oksanen, A.; Siles-Lucas, M.; Karamon, J.; Possenti, A.; Conraths, F.J.; Romig, T.; Wysocki, P.; Mannocci, A.; Mipatrini, D.; La Torre, G.; et al. The geographical distribution and prevalence of Echinococcus multilocularis in animals in the European Union and adjacent countries: A systematic review and meta-analysis. Parasites Vectors 2016, 9, 519. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chauchet, A.; Grenouillet, F.; Knapp, J.; Richou, C.; Delabrousse, E.; Dentan, C.; Millon, L.; Di Martino, V.; Contreras, R.; Deconinck, E.; et al. Increased incidence and characteristics of alveolar echinococcosis in patients with immunosuppression-associated conditions. Clin. Infect. Dis. 2014, 59, 1095–1104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brunetti, E.; Kern, P.; Vuitton, D.A. Expert consensus for the diagnosis and treatment of cystic and alveolar echinococcosis in humans. Acta Trop. 2010, 114, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Kern, P.; Wen, H.; Sato, N.; Vuitton, D.A.; Gruener, B.; Shao, Y.; Delabrousse, E.; Kratzer, W.; Bresson-Hadni, S. WHO classification of alveolar echinococcosis: Principles and application. Parasitol. Int. 2006, 55, S283–S287. [Google Scholar] [CrossRef] [PubMed]
- Gottstein, B.; Lachenmayer, A.; Beldi, G.; Wang, J.; Merkle, B.; Vu, X.L.; Kurath, U.; Muller, N. Diagnostic and follow-up performance of serological tests for different forms/courses of alveolar echinococcosis. Food Waterborne Parasitol. 2019, 16, e00055. [Google Scholar] [CrossRef]
- Ito, A.; Ma, L.; Schantz, P.M.; Gottstein, B.; Liu, Y.H.; Chai, J.J.; Abdel-Hafez, S.K.; Altintas, N.; Joshi, D.D.; Lightowlers, M.W.; et al. Differential serodiagnosis for cystic and alveolar echinococcosis using fractions of Echinococcus granulosus cyst fluid (antigen B) and E. multilocularis protoscolex (EM18). Am. J. Trop. Med. Hyg. 1999, 60, 188–192. [Google Scholar] [CrossRef] [Green Version]
- Ito, A.; Craig, P.S. Immunodiagnostic and molecular approaches for the detection of taeniid cestode infections. Trends Parasitol. 2003, 19, 377–381. [Google Scholar] [CrossRef]
- Deibel, A.; Stocker, D.; Meyer Zu Schwabedissen, C.; Husmann, L.; Kronenberg, P.A.; Grimm, F.; Deplazes, P.; Reiner, C.S.; Müllhaupt, B. Evaluation of a structured treatment discontinuation in patients with inoperable alveolar echinococcosis on long-term benzimidazole therapy: A retrospective cohort study. PLoS Negl. Trop. Dis. 2022, 16, e0010146. [Google Scholar] [CrossRef]
- Topic, R.Z.; Dodig, S. Eosinophil cationic protein--current concepts and controversies. Biochem. Med. 2011, 21, 111–121. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.; Rosenberg, H.F. Sequence variation at two eosinophil-associated ribonuclease loci in humans. Genetics 2000, 156, 1949–1958. [Google Scholar] [CrossRef] [PubMed]
- Venge, P.; Byström, J. Eosinophil cationic protein (ECP). Int. J. Biochem. Cell Biol. 1998, 30, 433–437. [Google Scholar] [CrossRef]
- Boix, E.; Torrent, M.; Sánchez, D.; Nogués, M.V. The antipathogen activities of eosinophil cationic protein. Curr. Pharm. Biotechnol. 2008, 9, 141–152. [Google Scholar] [CrossRef] [PubMed]
- Munthe-Kaas, M.C.; Gerritsen, J.; Carlsen, K.H.; Undlien, D.; Egeland, T.; Skinningsrud, B.; Tørres, T.; Carlsen, K.L. Eosinophil cationic protein (ECP) polymorphisms and association with asthma, s-ECP levels and related phenotypes. Allergy 2007, 62, 429–436. [Google Scholar] [CrossRef] [PubMed]
- Pereira, M.C.; Oliveira, D.T.; Kowalski, L.P. The role of eosinophils and eosinophil cationic protein in oral cancer: A review. Arch. Oral Biol. 2011, 56, 353–358. [Google Scholar] [CrossRef] [PubMed]
- Kurtzhals, J.A.; Reimert, C.M.; Tette, E.; Dunyo, S.K.; Koram, K.A.; Akanmori, B.D.; Nkrumah, F.K.; Hviid, L. Increased eosinophil activity in acute Plasmodium falciparum infection—Association with cerebral malaria. Clin. Exp. Immunol. 1998, 112, 303–307. [Google Scholar] [CrossRef] [PubMed]
- National Heart, Lung, and Blood Institute. Guidelines for the diagnosis and management of asthma. National Asthma Education Program. Expert Panel Report. J. Allergy Clin. Immunol. 1991, 88, 425–534. [Google Scholar]
- Dal Negro, R.; Tognella, S.; Micheletto, C.; Pomari, C.; Burti, E.; Mauroner, L.; Turco, P. Serum eosinophil cationic protein and bronchial hyperresponsiveness to hypoosmolar challenge in naive atopic asthmatics. J. Investig. Allergol. Clin. Immunol. 1998, 8, 294–299. [Google Scholar]
- Ramos, A.L.; Discipio, R.G.; Ferreira, A.M. Eosinophil cationic protein damages protoscoleces in vitro and is present in the hydatid cyst. Parasite Immunol. 2006, 28, 347–355. [Google Scholar] [CrossRef]
- Cicioglu Aridogan, B.; Kaya, S.; Sesli Cetin, E.; Tas, T.; Demirci, M. Evaluation of eosinophil cationic protein levels with clinical symptoms and laboratory findings of patients with cystic echinococcosis. Mikrobiyol. Bul. 2009, 43, 285–292. [Google Scholar] [PubMed]
- WHO InformalWorking Group. International classification of ultrasound images in cystic echinococcosis for application in clinical and field epidemiological settings. Acta Trop. 2003, 85, 253–261. [Google Scholar] [CrossRef]
- Gharbi, H.A.; Hassine, W.; Brauner, M.W.; Dupuch, K. Ultrasound examination of the hydatic liver. Radiology 1981, 139, 459–463. [Google Scholar] [CrossRef]
- Stojkovic, M.; Rosenberger, K.; Kauczor, H.U.; Junghanss, T.; Hosch, W. Diagnosing and staging of cystic echinococcosis: How do CT and MRI perform in comparison to ultrasound? PLoS Negl. Trop. Dis. 2012, 6, e1880. [Google Scholar] [CrossRef] [PubMed]
- Grüner, B.; Kern, P.; Mayer, B.; Gräter, T.; Hillenbrand, A.; Barth, T.E.F.; Muche, R.; Henne-Bruns, D.; Kratzer, W.; Kern, P. Comprehensive diagnosis and treatment of alveolar echinococcosis: A single-center, long-term observational study of 312 patients in Germany. GMS Infect. Dis. 2017, 5, Doc01. [Google Scholar] [CrossRef]
- Breijo, M.; Anesetti, G.; Martínez, L.; Sim, R.B.; Ferreira, A.M. Echinococcus granulosus: The establishment of the metacestode is associated with control of complement-mediated early inflammation. Exp. Parasitol. 2008, 118, 188–196. [Google Scholar] [CrossRef]
- Siles-Lucas, M.; Casulli, A.; Cirilli, R.; Carmena, D. Progress in the pharmacological treatment of human cystic and alveolar echinococcosis: Compounds and therapeutic targets. PLoS Negl. Trop. Dis. 2018, 12, e0006422. [Google Scholar] [CrossRef] [Green Version]
- Liu, W.; Delabrousse, É.; Blagosklonov, O.; Wang, J.; Zeng, H.; Jiang, Y.; Wang, J.; Qin, Y.; Vuitton, D.A.; Wen, H. Innovation in hepatic alveolar echinococcosis imaging: Best use of old tools, and necessary evaluation of new ones. Parasite 2014, 21, 74. [Google Scholar] [CrossRef]

{kind=link}
| Patients | Gender | Age * | Disease | PNM Classification | Therapy Scheme | Organ Manifestation | ECP Preinterventional | ECP Postinterventional | Lesion Size ** | Traceruptake in PET-CTI |
| Group A | ||||||||||
| patient 1 | female | 80 | AE | P3N0M1 | BMZ | liver, perisplenic | 9.9 μg/L | 4.9 μg/L | 57.6 cm2 | strong |
| patient 2 | female | 27 | AE | P3N0M0 | operative + BMZ | liver | 28.9 μg/L | 10.4 μg/L | 70.3 cm2 | none |
| patient 3 | female | 59 | AE | P2N0M0 | operative + BMZ | liver | 15.2 μg/L | 55.7 μg/L | 23.4 cm2 | none |
| patient 4 | female | 20 | AE | P2N0M0 | operative + BMZ | liver | 38.5 μg/L | 14.1 μg/L | 18.4 cm2 | weak |
| patient 5 | male | 68 | AE | P2N0M0 | BMZ | liver | 33.7 μg/L | 13.4 μg/L | 26.0 cm2 | weak |
| patient 6 | male | 60 | AE | P1N0M0 | operative + BMZ | liver | 8.1 μg/L | 10.4 μg/L | 4.0 cm2 | none |
| patient 7 | male | 57 | AE | P2N0M0 | BMZ | liver | 8.3 μg/L | 3.5 μg/L | 17.1 cm2 | none |
| patient 8 | female | 21 | AE | P2N1M0 | operative + BMZ | liver, pleura | 14.6 μg/L | 16.6 μg/L | 12.3 cm2 | none |
| patient 9 | female | 36 | AE | P2N0M0 | operative + BMZ | liver | 24.1 μg/L | 16.9 μg/L | 34.3 cm2 | weak |
| patient 10 | male | 72 | AE | P3N0M0 | operative + BMZ | liver | 57.1 μg/L | 24.6 μg/L | 28.2 cm2 | weak |
| patient 11 | male | 71 | AE | P4N0M1 | operative + BMZ | liver, lung, adrenal | 72.0 μg/L | 28.1 μg/L | 45.5 cm2 | - |
| patient 12 | male | 66 | AE | P3N0M0 | operative + BMZ | liver | 24.0 μg/L | 31.8 μg/L | 23.2 cm2 | weak |
| patient 13 | male | 55 | AE | P3N0M0 | operative + BMZ | liver | 56.4 μg/L | 14.4 μg/L | 48.0 cm2 | weak |
| patient 14 | female | 63 | AE | P3N0M0 | operative + BMZ | liver | 50.5 μg/L | 8.7 μg/L | 70.5 cm2 | strong |
| patient 15 | male | 54 | AE | P3N0M0 | operative + BMZ | liver | 79.8 μg/L | 46.9 μg/L | 24.5 cm2 | strong |
| patient 16 | female | 53 | AE | P4N0M1 | operative + BMZ | liver, lung | 22.6 μg/L | 22.7 μg/L | 64.0 cm2 | weak |
| Patients | Gender | Age * | Disease | CE Cyst Classification *** | Therapy Scheme | Organ Manifestation | ECP Preinterventional | ECP Postinterventional | Lesion Size | |
| Group B | ||||||||||
| patient 17 | male | 48 | CE | CE2 | operative + BMZ | liver, lung | 58.7 μg/L | 24.9 μg/L | 70.5 cm2 | |
| patient 18 | female | 34 | CE | CE2 | operative + BMZ | liver | 76.2 μg/L | 41.0 μg/L | 36.3 cm2 | |
| patient 19 | male | 45 | CE | CE5, CE1 | BMZ | liver | 44.8 μg/L | 14.9 μg/L | 60.9 cm2 | |
| patient 20 | female | 32 | CE | CE1 | operative + BMZ | liver | 28.3 μg/L | 24.7 μg/L | 127.8 cm2 | |
| patient 21 | male | 40 | CE | CE3a | operative + BMZ | right thigh | 48.5 μg/L | 26.7 μg/L | 40.1 cm2 | |
| patient 22 | male | 51 | CE | CE2 | BMZ | liver | 33.0 μg/L | 7.1 μg/L | 25.4 cm2 | |
| patient 23 | male | 27 | CE | CE1 | operative + BMZ | liver | 17.1 μg/L | 31.0 μg/L | 63.2 cm2 | |
| patient 24 | male | 30 | CE | CE3a | operative + BMZ | lung | 50.2 μg/L | 33.5 μg/L | 5.9 cm2 | |
| patient 25 | female | 62 | CE | CE1 | operative + BMZ | liver, lung | 36.2 μg/L | 18.8 μg/L | 108.2 cm2 | |
| patient 26 | male | 20 | CE | CE3a | operative + BMZ | liver | 41.7 μg/L | 16.1 μg/L | 16.4 cm2 | |
| patient 27 | male | 54 | CE | CE3a | BMZ | liver, lung, spleen | 75.5 μg/L | 22.7 μg/L | 116.5 cm2 | |
| patient 28 | female | 42 | CE | CE2, CE3b | operative + BMZ | uterus, adnexa | 23.9 μg/L | 17.5 μg/L | 71.5 cm2 | |
| patient 29 | male | 58 | CE | CE3a | BMZ | liver | 36.0 μg/L | 23.5 μg/L | 34.0 cm2 | |
| patient 30 | female | 18 | CE | CE4, CE5 | BMZ | liver, kidney | 9.5 μg/L | 13.3 μg/L | 13.7 cm2 | |
| patient 31 | female | 30 | CE | CE3b, CE1 | operative + BMZ | liver, lung | 20.2 μg/L | 19.9 μg/L | 25.8 cm2 | |
| patient 32 | female | 54 | CE | CE1 | BMZ | liver | 17.2 μg/L | 23.1 μg/L | 33.2 cm2 |
| PNM Classification | Tracer Uptake in PET–CTI | Lesion Size | |||
|---|---|---|---|---|---|
| Spearman Rho | Alveolar Echinococcosis | ||||
| ECP * | k ** | 0.23 | 0.56 | 0.40 | |
| p | 0.39 | p < 0.05 | 0.12 | ||
| n | 16 | 15 | 16 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hotz, J.F.; Kaczirek, K.; Stremitzer, S.; Waneck, F.; Auer, H.; Perkmann, T.; Kussmann, M.; Bauer, P.K.; Chen, R.-Y.; Kriz, R.; et al. Evaluation of Eosinophilic Cationic Protein as a Marker of Alveolar and Cystic Echinococcosis. Pathogens 2022, 11, 261. https://doi.org/10.3390/pathogens11020261
Hotz JF, Kaczirek K, Stremitzer S, Waneck F, Auer H, Perkmann T, Kussmann M, Bauer PK, Chen R-Y, Kriz R, et al. Evaluation of Eosinophilic Cationic Protein as a Marker of Alveolar and Cystic Echinococcosis. Pathogens. 2022; 11(2):261. https://doi.org/10.3390/pathogens11020261
Chicago/Turabian StyleHotz, Julian Frederic, Klaus Kaczirek, Stefan Stremitzer, Fredrik Waneck, Herbert Auer, Thomas Perkmann, Manuel Kussmann, Philipp Karl Bauer, Rui-Yang Chen, Richard Kriz, and et al. 2022. "Evaluation of Eosinophilic Cationic Protein as a Marker of Alveolar and Cystic Echinococcosis" Pathogens 11, no. 2: 261. https://doi.org/10.3390/pathogens11020261
APA StyleHotz, J. F., Kaczirek, K., Stremitzer, S., Waneck, F., Auer, H., Perkmann, T., Kussmann, M., Bauer, P. K., Chen, R.-Y., Kriz, R., Burgmann, H., Ramharter, M., & Lagler, H. (2022). Evaluation of Eosinophilic Cationic Protein as a Marker of Alveolar and Cystic Echinococcosis. Pathogens, 11(2), 261. https://doi.org/10.3390/pathogens11020261