

Matrix Metalloproteinase 9 (MMP-9) and Interleukin-8 (IL-8) in Gingival Crevicular Fluid after Regenerative Therapy in Periodontal Intrabony Defects with and without Systemic Antibiotics—Randomized Clinical Trial
 ,
, 
 and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population and Experimental Design
2.2. Surgical Procedures
2.3. Clinical Examinations and Postoperative Care
2.4. GCF Sampling
2.5. GCF IL-8 and MMP-9 Analysis
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Page, R.C. The role of inflammatory mediators in the pathogenesis of periodontal disease. J. Periodontal Res. 1991, 26, 230–242. [Google Scholar] [CrossRef] [PubMed]
- Golub, L.M.; Lee, H.M.; Greenwald, R.A.; Ryan, M.E.; Sorsa, T.; Salo, T.; Giannobile, W.V. A matrix metalloproteinase inhibitor reduces bone-type collagen degradation fragments and specific collagenases in gingival crevicular fluid during adult periodontitis. Inflamm. Res. 1997, 46, 310–319. [Google Scholar] [CrossRef] [PubMed]
- Ryan, M.E.; Golub, L.M. Modulation of matrix metalloproteinase activities in periodontitis as a treatment strategy. Periodontology 2000 2000, 24, 226–238. [Google Scholar] [CrossRef] [PubMed]
- Uitto, V.J.; Overall, C.M.; McCulloch, C. Proteolytic host cell enzymes in gingival crevice fluid. Periodontology 2000 2003, 31, 77–104. [Google Scholar] [CrossRef]
- Pozo, P.; Valenzuela, M.A.; Melej, C.; Zaldivar, M.; Puente, J.; Martinez, B.; Gamonal, J. Longitudinal analysis of metalloproteinases, tissue inhibitors of metalloproteinases and clinical parameters in gingival crevicular fluid from periodontitis-affected patients. J. Periodont. Res. 2005, 40, 199–207. [Google Scholar] [CrossRef]
- Soder, B.; AirilaMansson, S.; Soder, P.O.; Kari, K.; Meurman, J. Levels of matrix metalloproteinases-8 and -9 with simultaneous presence of periodontal pathogens in gingival crevicular fluid as well as matrix metalloproteinase-9 and cholesterol in blood. J. Periodont. Res. 2008, 41, 411–417. [Google Scholar] [CrossRef]
- Marcaccini, A.M.; Meschiari, C.A.; Zuardi, L.R.; de Sousa, T.S.; Taba, M.; Teofilo, J.M.; Jacob-Ferreira, A.L.B.; Tanus-Santos, J.E.; Novaes, A.B.; Gerlach, R.F. Gingival crevicular fluid levels of MMP-8, MMP-9, TIMP-2, and MPO decrease after periodontal therapy. J. Clin.Periodontol. 2010, 37, 180–190. [Google Scholar] [CrossRef]
- Balli, U.; Keles, G.C.; Cetinkaya, B.O.; Mercan, U.; Ayas, B.; Erdogan, D. Assessment of vascular endothelial growth factor and matrix metalloproteinase-9 in the periodontium of rats treated with atorvastatin. J. Periodontol. 2014, 85, 178–187. [Google Scholar] [CrossRef]
- Hill, P.A.; Docherty, A.J.; Bottomley, K.M.; O’Connell, J.P.; Morphy, J.R.; Reynolds, J.J.; Meikle, M.C. Inhibition of bone resorption in vitro by selective inhibitors of gelatinase and collagenase. Biochem. J. 1995, 308 Pt 1, 167–175. [Google Scholar] [CrossRef]
- Hernández Ríos, M.; Sorsa, T.; Obregón, F.; Tervahartiala, T.; Valenzuela, M.A.; Pozo, P.; Dutzan, N.; Lesaffre, E.; Molas, M.; Gamonal, J. Proteolytic roles of matrix metalloproteinase (MMP)-13 during progression of chronic periodontitis: Initial evidence for MMP-13/MMP-9 activation cascade. J. Clin. Periodontol. 2009, 36, 1011–1017. [Google Scholar] [CrossRef]
- Baggiolini, M.; Walz, A.; Kunkel, S.L. Neutrophil-activating peptide-1/interleukin 8, a novel cytokine that activates neutrophils. J. Clin. Investig. 1989, 84, 1045–1049. [Google Scholar] [CrossRef] [PubMed]
- Yoshimura, A.; Hara, Y.; Kaneko, T.; Kato, I. Secretion of IL-1β, TNF-α, IL-8 and IL-1ra by human polymorphonuclear leukocytes in response to lipopolysaccharides from periodontopathic bacteria. J. Periodont. Res. 1997, 32, 279–286. [Google Scholar] [CrossRef] [PubMed]
- Schluger, N.W.; Rom, W.N. Early responses to infection: Chemokines as mediators of inflammation. Curr. Opin. Immunol. 1997, 9, 504–508. [Google Scholar] [CrossRef]
- Bickel, M. The role of interleukin-8 in inflammation and mechanisms of regulation. J. Periodontol. 1993, 64 (5 Suppl.), 456–460. [Google Scholar]
- Herrera, D.; Alonso, B.; Leon, R.; Roldan, S.; Sanz, M. Antimicrobial therapy in periodontitis: The use of systemic antimicrobials against the subgingival biofilm. J. Clin. Periodontol. 2008, 35 (Suppl. 8), 45–66. [Google Scholar] [CrossRef]
- Nowzari, H.; Matian, F.; Slots, J. Periodontal pathogens on polytetrafluoroethylene membrane for guided tissue regeneration inhibit healing. J. Clin. Periodontol. 1995, 22, 469–474. [Google Scholar] [CrossRef]
- Mombelli, A.; Zappa, U.; Bragger, U.; Lang, N.P. Systemic antimicrobial treatment and guided tissue regeneration. Clinical and microbiological effects in furcation defects. J. Clin. Periodontol. 1996, 23, 386–396. [Google Scholar] [CrossRef]
- Powell, C.A.; Mealey, B.L.; Deas, D.E.; McDonnell, H.T.; Moritz, A.J. Post-surgical infections: Prevalence associated with various periodontal surgical procedures. J. Periodontol. 2005, 76, 329–333. [Google Scholar] [CrossRef]
- Van Winkelhoff, A.J.; Winkel, E.G. Antibiotics in periodontics: Right or wrong? J. Periodontol. 2009, 80, 1555–1558. [Google Scholar] [CrossRef]
- Addy, M.; Martin, M.V. Systemic antimicrobials in the treatment of chronic periodontal diseases: A dilemma. Oral Dis. 2003, 9 (Suppl. 1), 38–44. [Google Scholar] [CrossRef]
- Pietruska, M.; Dolińska, E.; Milewski, R.; Sculean, A. Effect of systemic antibiotics on the outcomes of regenerative periodontal surgery in intrabony defects: A randomized, controlled, clinical study. Clin. Oral Investig. 2021, 25, 2959–2968. [Google Scholar] [CrossRef]
- O’Leary, T.J.; Drake, R.B.; Naylor, J.E. The plaque control record. J. Periodontol. 1972, 43, 38. [Google Scholar] [CrossRef] [PubMed]
- Lamster, I.B.; Oshrain, R.L.; Gordon, J.M. Enzyme activity in human gingival crevicular fluid: Considerations in data reporting based on analysis of individual crevicular sites. J. Clin. Periodontol. 1986, 13, 799–804. [Google Scholar] [CrossRef]
- Wassall, R.R.; Preshaw, P.M. Clinical and technical considerations in the analysis of gingival crevicular fluid. Periodontology 2000 2016, 70, 65–79. [Google Scholar] [CrossRef]
- Lamster, I.B.; Ahlo, J.K. Analysis of gingival crevicular fluid as applied to the diagnosis of oral and systemic diseases. Ann. N. Y. Acad. Sci. 2007, 1098, 216–229. [Google Scholar] [CrossRef] [PubMed]
- Oliver, R.C.; Holm-Pederen, P.; Löe, H. The correlation between clinical scoring, exudate measurements and microscopic evaluation of inflammation in the gingiva. J. Periodontol. 1969, 40, 201–209. [Google Scholar] [CrossRef] [PubMed]
- Ozkavaf, A.; Aras, H.; Huri, C.B.; Mottaghian-Dini, F.; Tözüm, T.F.; Etikan, I.; Yamalik, N.; Caglayan, F. Relationship between the quantity of gingival crevicular fluid and clinical periodontal status. J. Oral Sci. 2000, 42, 231–238. [Google Scholar] [CrossRef]
- Armitage, G.C. Analysis of gingival crevicular fluid and risk of progression of periodontitis. Periodontology 2000 2004, 34, 109–119. [Google Scholar] [CrossRef]
- Griffiths, G. Formation, collection and significance of gingival crevice fluid. Periodontology 2000 2003, 31, 32–42. [Google Scholar] [CrossRef]
- Gamal, A.Y.; El-Shal, O.S.; El-Aasara, M.M.; Fakhry, E.M. Plateletderivedgrowth factor-BB release profile in gingival crevicular fluid after use of marginal periosteal pedicle graft as an autogenous guided tissue membrane to treat localized intrabony defects. J. Periodontol. 2011, 82, 272–280. [Google Scholar] [CrossRef]
- Gamal, A.Y.; Abdel-Ghaffar, K.A.; Iacono, V.J. Gingival crevicular fluid vascular endothelial cell growth factor and plateletderived growth factor-BB release profile following the use of perforated barrier membranes during treatment of intrabony defects: A randomised clinical trial. J. Periodont. Res. 2016, 51, 407–416. [Google Scholar] [CrossRef] [PubMed]
- Rakmanee, T.; Calciolari, E.; Olsen, I.; Darbar, U.; Griffiths, G.S.; Petrie, A.; Donos, N. Expression of growth mediators in the gingival crevicular fluid of patients with aggressive periodontitis undergoing periodontal surgery. Clin. Oral Investig. 2018, 23, 3307–3318. [Google Scholar] [CrossRef] [PubMed]
- Kuru, L.; Griffiths, G.S.; Petrie, A.; Olsen, I. Changes in transforming growth factor-beta1 in gingival crevicular fluid following periodontal surgery. J. Clin. Periodontol. 2004, 31, 527–533. [Google Scholar] [CrossRef] [PubMed]
- Pellegrini, G.; Rasperini, G.; Pagni, G.; Giannobile, W.V.; Milani, S.; Musto, F.; Dellavia, C. Local wound healing biomarkers for real-time assessment of periodontal regeneration: Pilot study. J. Periodont. Res. 2017, 52, 388–396. [Google Scholar] [CrossRef] [PubMed]
- Okuda, K.; Miyazaki, A.; Momose, M.; Murata, M.; Nomura, T.; Kubota, T.; Wolff, L.F.; Yoshie, H. Levels of tissue inhibitor ofmetalloproteinases-1 andmatrix metalloproteinases-1 and -8 in gingival crevicular fluid following treatment with enamel matrix derivative(Emdogain). J. Periodont. Res. 2001, 36, 309–316. [Google Scholar] [CrossRef] [PubMed]
- Mäkelä, M.; Salo, T.; Uitto, V.J.; Larjava, H. Matrix metalloproteinases (MMP-2 and MMP-9) of the oral cavity: Cellular origin and relationship to periodontal status. J. Dent. Res. 1994, 73, 1397–1406. [Google Scholar] [CrossRef] [PubMed]
- Franco, C.; Patricia, H.R.; Timo, S.; Claudia, B.; Marcela, H. Matrix metalloproteinases as regulators of periodontal inflammation. Int. J. Mol. Sci. 2017, 18, 440. [Google Scholar] [CrossRef]
- Sijari, Z.; Romano, F.; Ciardo, G.; Martella, V.; Maggiora, M.; Bottone, M.; Aimetti, M. Effect of two post-surgical cleansing protocols on early periodontal wound healing and cytokine levels following osseous resective surgery: A randomized controlled study. Int. J. Dent. Hyg. 2019, 17, 300–308. [Google Scholar] [CrossRef] [PubMed]
- Opdenakker, G.; Van den Steen, P.E.; Dubois, B.; Nelissen, I.; Van Coillie, E.; Masure, S.; Proost, P.; Van Damme, J. Gelatinase B functions as regulator and effector in leukocyte biology. J. Leukoc. Biol. 2001, 69, 851–859. [Google Scholar] [CrossRef]
- Zariffard, M.R.; Anastos, K.; French, A.L.; Munyazesa, E.; Cohen, M.; Landay, A.L.; Spear, G.T. Cleavage/alteration of interleukin-8 by matrix metalloproteinase-9 in the female lower genital tract. PLoS ONE 2015, 22, e0116911. [Google Scholar] [CrossRef]
- Dias, I.H.; Marshall, L.; Lambert, P.A.; Chapple, I.L.; Matthews, J.B.; Griffiths, H.R. Gingipains from Porphyromonas gingivalis increase the chemotactic and respiratory burst-priming properties of the 77-amino-acid interleukin-8 variant. Infect. Immun. 2008, 76, 317–323. [Google Scholar] [CrossRef] [PubMed]
- Mikolajczyk-Pawlinska, J.; Travis, J.; Potempa, J. Modulation of interleukin-8 activity by gingipains from Porphyromonas gingivalis: Implications for pathogenicity of periodontal disease. FEBS Lett. 1998, 440, 282–286. [Google Scholar] [CrossRef]
- Potempa, J.; Banbula, A.; Travis, J. Role of bacterial proteinases in matrix destruction and modulation of host responses. Periodontology 2000 2000, 24, 153–192. [Google Scholar] [CrossRef]
- Koidou, V.P.; Chatzopoulos, G.S.; Tomas, I.; Nibali, L.; Donos, N. Expression of gingival crevicular fluid markers during early and late healing of intrabony defects after surgical treatment: A systematic review. Clin. Oral Investig. 2020, 24, 487–502. [Google Scholar] [CrossRef] [PubMed]
- Koidou, V.P.; Hagi-Pavli, E.; Cross, S.; Nibali, L.; Donos, N. Molecular profiling of intrabony defects’ gingival crevicular fluid. J. Periodontal Res. 2022, 57, 152–161. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| DBBM/GTR+AB Me (Q1; Q3) | DBBM/GTR Me (Q1; Q3) | p** (Group vs. Group) | |
|---|---|---|---|
| baseline | 20.85 (12.08; 73.16) | 14.76 (6.46; 53.63) | NS |
| 2 weeks | 26.35 (13.34; 55.1) | 13.37 (7.03; 29.67) | NS |
| 4 weeks | 14.7 (8.49; 28.32) | 17.52 (7.32; 29.78) | NS |
| 6 months | 18.14 (9.45; 52.99) | 14.13 (6.92; 23.07) | NS |
| p* (time changes) | NS | NS |
| DBBM/GTR+AB Me (Q1; Q3) | DBBM/GTR Me (Q1; Q3) | p** (Gruop vs. Group) | |
|---|---|---|---|
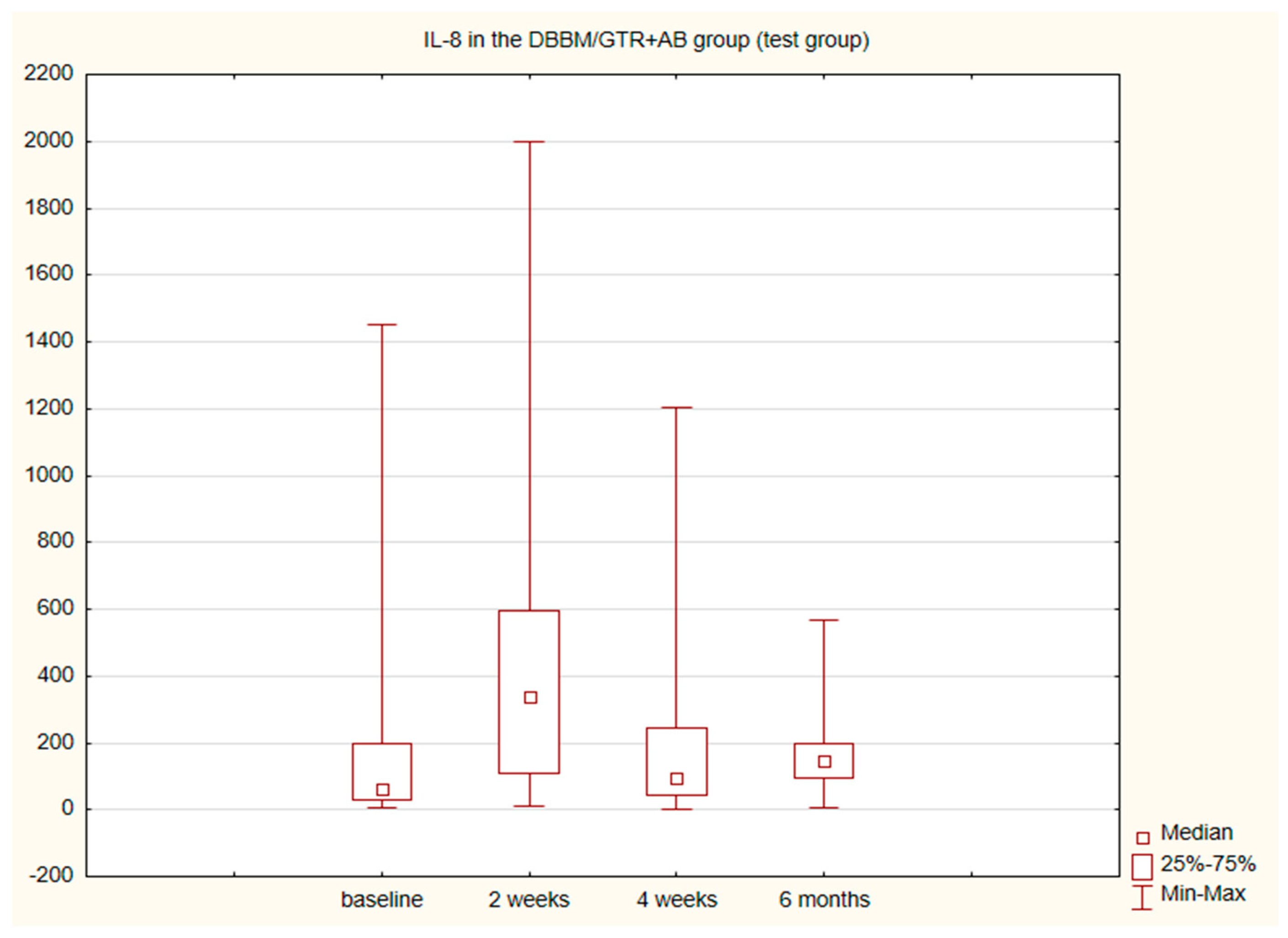
| baseline | 64.42 (28.34; 199.6) | 99.7 (51.76; 208.3) | NS |
| 2 weeks | 337.5 (107.7; 593.8) | 163.9 (42.37; 336.75) | NS |
| 4 weeks | 95.21 (45.35; 246.6) | 98.68 (34.98; 180,5) | NS |
| 6 months | 146.7 (96.32; 198.6) | 95.53 (60.36; 142.7) | NS |
| p* (time changes) | p = 0.01 | NS |
| IL-8 & MMP-9 | DBBM/GTR+AB | DBBM/GTR | ||
|---|---|---|---|---|
| R | p | R | p | |
| baseline | 0.58 | 0.006 | 0.55 | 0.013 |
| 2 weeks | 0.43 | 0.049 | 0.67 | 0.001 |
| 4 weeks | 0.24 | 0.3 (NS) | 0.65 | 0.002 |
| 6 months | 0.86 | 0.000001 | 0.7 | 0.0006 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dolińska, E.; Pietruska, M.; Dymicka-Piekarska, V.; Milewski, R.; Sculean, A. Matrix Metalloproteinase 9 (MMP-9) and Interleukin-8 (IL-8) in Gingival Crevicular Fluid after Regenerative Therapy in Periodontal Intrabony Defects with and without Systemic Antibiotics—Randomized Clinical Trial. Pathogens 2022, 11, 1184. https://doi.org/10.3390/pathogens11101184
Dolińska E, Pietruska M, Dymicka-Piekarska V, Milewski R, Sculean A. Matrix Metalloproteinase 9 (MMP-9) and Interleukin-8 (IL-8) in Gingival Crevicular Fluid after Regenerative Therapy in Periodontal Intrabony Defects with and without Systemic Antibiotics—Randomized Clinical Trial. Pathogens. 2022; 11(10):1184. https://doi.org/10.3390/pathogens11101184
Chicago/Turabian StyleDolińska, Ewa, Małgorzata Pietruska, Violetta Dymicka-Piekarska, Robert Milewski, and Anton Sculean. 2022. "Matrix Metalloproteinase 9 (MMP-9) and Interleukin-8 (IL-8) in Gingival Crevicular Fluid after Regenerative Therapy in Periodontal Intrabony Defects with and without Systemic Antibiotics—Randomized Clinical Trial" Pathogens 11, no. 10: 1184. https://doi.org/10.3390/pathogens11101184
APA StyleDolińska, E., Pietruska, M., Dymicka-Piekarska, V., Milewski, R., & Sculean, A. (2022). Matrix Metalloproteinase 9 (MMP-9) and Interleukin-8 (IL-8) in Gingival Crevicular Fluid after Regenerative Therapy in Periodontal Intrabony Defects with and without Systemic Antibiotics—Randomized Clinical Trial. Pathogens, 11(10), 1184. https://doi.org/10.3390/pathogens11101184