
Clinical Characteristics and Risk Factors for Intra-Abdominal Infection with Chryseobacterium indologenes after Orthotopic Liver Transplantation
Abstract
1. Introduction
2. Materials and Methods
2.1. Bacterial Identification and Antimicrobial Susceptibility Testing
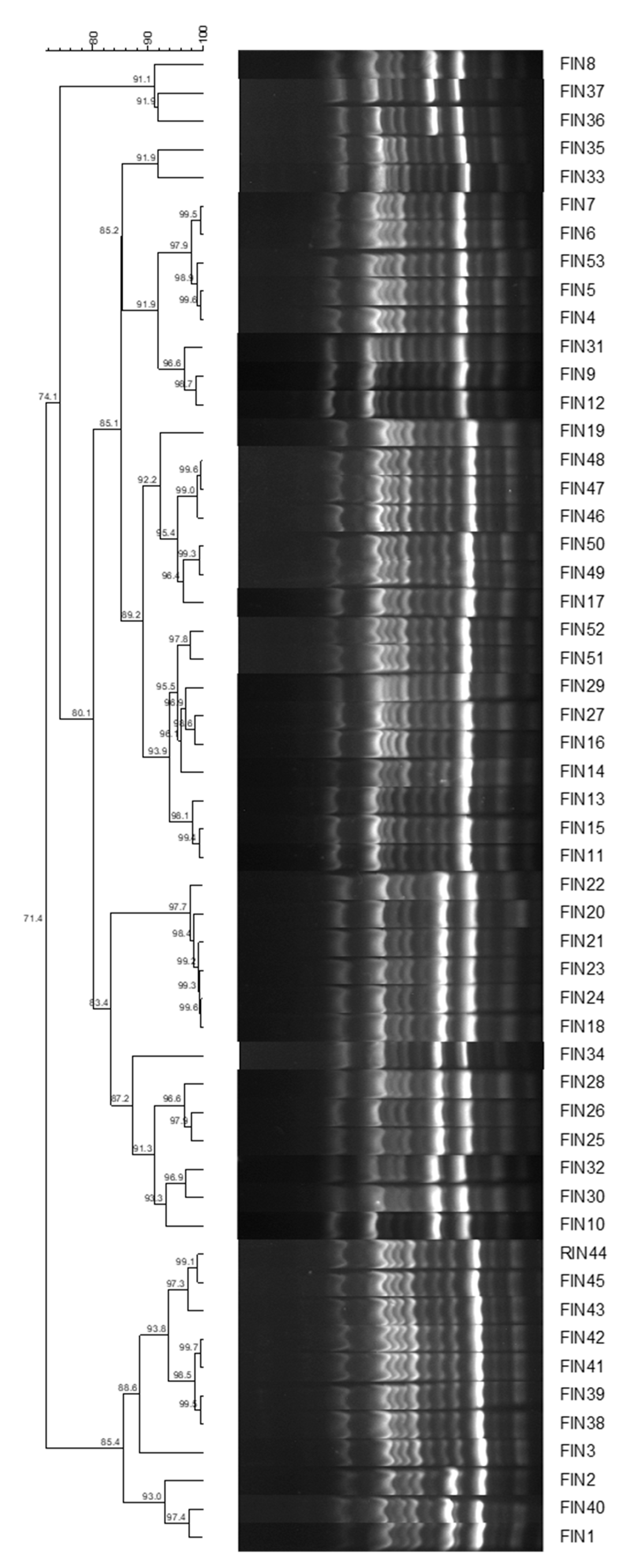
2.2. Homology Analysis
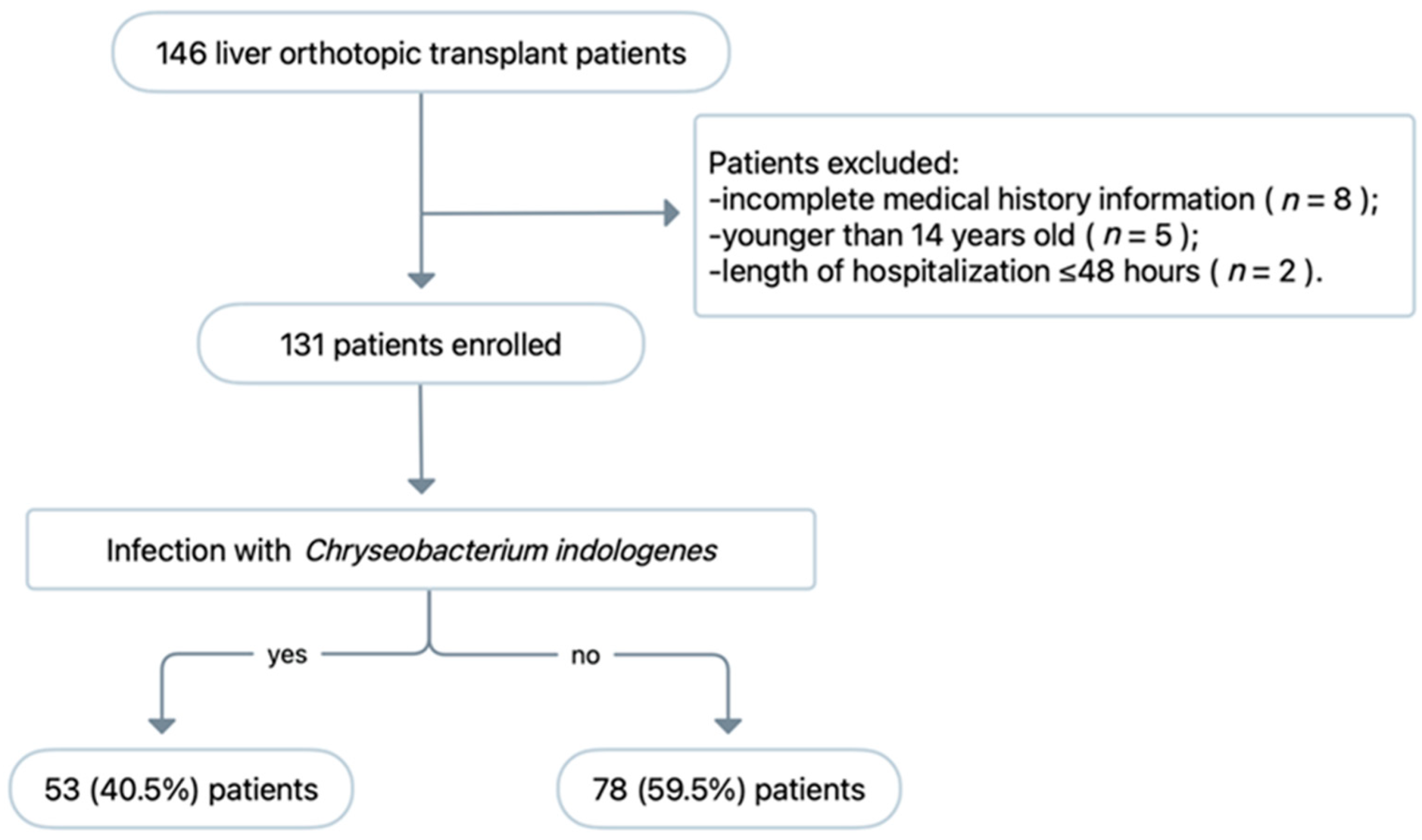
2.3. Case–Control Study
2.4. Assessment
2.5. Statistical Analysis
3. Results
3.1. Antimicrobial Susceptibility Testing
3.2. Homology Analysis
3.3. Patient Characteristics
3.4. Risk Factors for C. indologenes Intra-Abdominal Infection after OLT
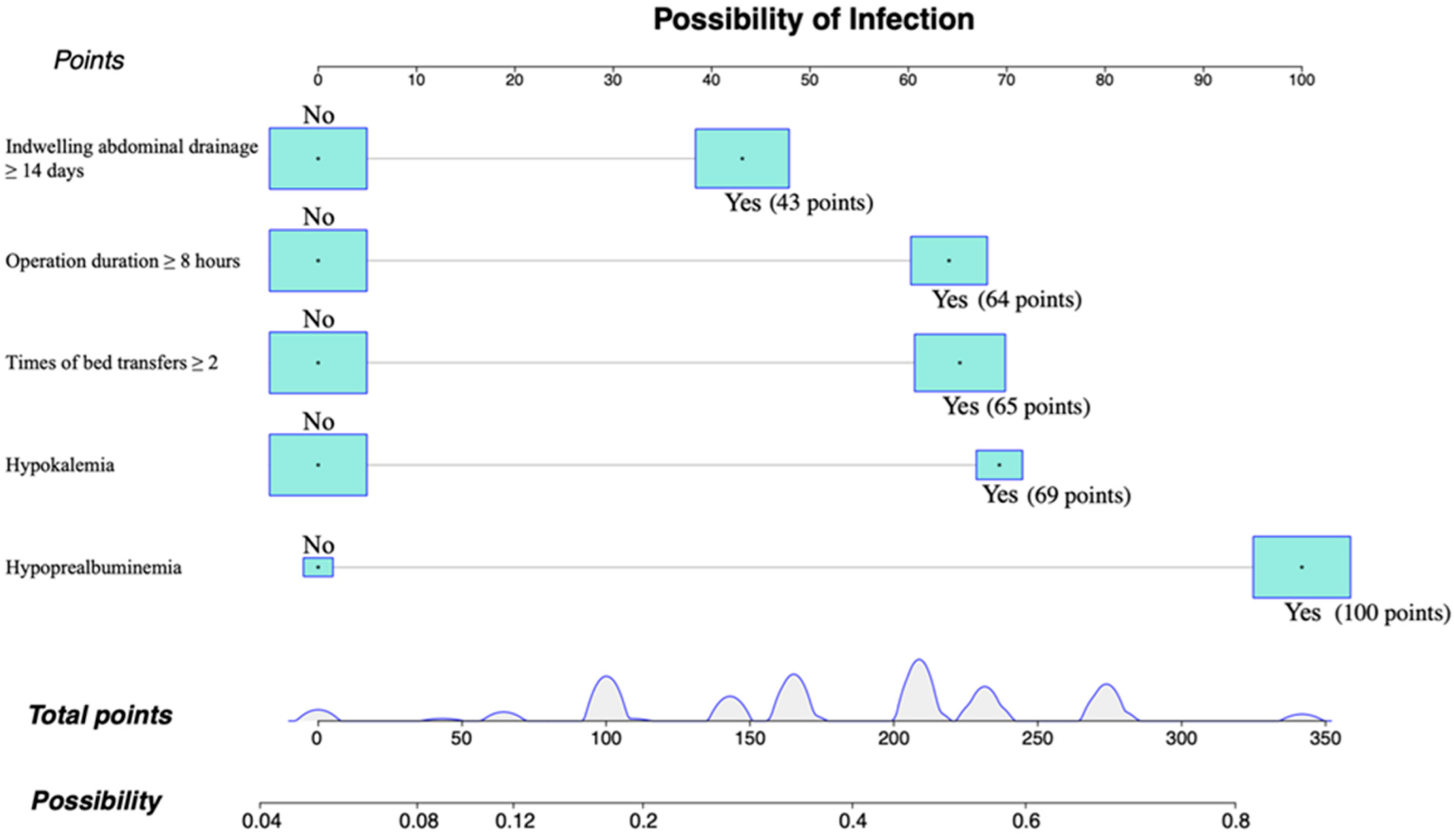
3.5. Nomogram Model of C. indologenes Infection after OLT
3.6. Nomogram Model Verification
3.7. Post-LT Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hsueh, P.R.; Teng, L.J.; Yang, P.C.; Ho, S.W.; Hsieh, W.C.; Luh, K.T. Increasing incidence of nosocomial Chryseobacterium indologenes infections in Taiwan. Eur. J. Clin. Microbiol. Infect. Dis. Off. Publ. Eur. Soc. Clin. Microbiol. 1997, 16, 568–574. [Google Scholar] [CrossRef] [PubMed]
- Esposito, S.; Russo, E.; De Simone, G.; Gioia, R.; Noviello, S.; Vitolo, M.; Rega, M.R.; Massari, A.; Posteraro, L. Transient bacteraemia due to Chryseobacterium indologenes in an immunocompetent patient: A case report and literature review. J. Chemother. 2015, 27, 324–329. [Google Scholar] [CrossRef] [PubMed]
- Chen, F.L.; Wang, G.C.; Teng, S.O.; Ou, T.Y.; Yu, F.L.; Lee, W.S. Clinical and epidemiological features of Chryseobacterium indologenes infections: Analysis of 215 cases. J. Microbiol. Immunol. Infect. 2013, 46, 425–432. [Google Scholar] [CrossRef]
- Cantero, M.; Parra, L.M.; Munez, E.; Iranzo, R.; Sanchez-Romero, M.I.; Oteo, J.; Asensio, A. A cluster of Chryseobacterium indologenes cases related to drainage water in intensive care units. Infect. Control Hosp. Epidemiol. 2018, 39, 997–999. [Google Scholar] [CrossRef]
- Fishman, J.A. Infection in solid-organ transplant recipients. N. Engl. J. Med. 2007, 357, 2601–2614. [Google Scholar] [CrossRef]
- Kim, S.I. Bacterial infection after liver transplantation. World J. Gastroenterol. 2014, 20, 6211–6220. [Google Scholar] [CrossRef] [PubMed]
- Fishman, J.A. Infections in immunocompromised hosts and organ transplant recipients: Essentials. Liver Transpl. 2011, 17 (Suppl. 3), S34–S37. [Google Scholar] [CrossRef]
- Hand, J.; Patel, G. Multidrug-resistant organisms in liver transplant: Mitigating risk and managing infections. Liver Transpl. 2016, 22, 1143–1153. [Google Scholar] [CrossRef]
- Fernández, J.; Prado, V.; Trebicka, J.; Amoros, A.; Gustot, T.; Wiest, R.; Deulofeu, C.; Garcia, E.; Acevedo, J.; Fuhrmann, V.; et al. Multidrug-resistant bacterial infections in patients with decompensated cirrhosis and with acute-on-chronic liver failure in Europe. J. Hepatol. 2019, 70, 398–411. [Google Scholar] [CrossRef]
- Macesic, N.; Gomez-Simmonds, A.; Sullivan, S.B.; Giddins, M.J.; Ferguson, S.A.; Korakavi, G.; Leeds, D.; Park, S.; Shim, K.; Sowash, M.G.; et al. Genomic Surveillance Reveals Diversity of Multidrug-Resistant Organism Colonization and Infection: A Prospective Cohort Study in Liver Transplant Recipients. Clin. Infect. Dis. 2018, 67, 905–912. [Google Scholar] [CrossRef]
- Shah, S.; Sarwar, U.; King, E.A.; Lat, A. Chryseobacterium indologenes subcutaneous port-related bacteremia in a liver transplant patient. Transpl. Infect. Dis. 2012, 14, 398–402. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Li, D.; Yang, Y.; Su, J.; Xu, X.; Wang, M.; Chen, Y.; Li, Y. Clinical and molecular characteristics of Chryseobacterium indologenes isolates at a teaching hospital in Shanghai, China. Ann. Transl. Med. 2021, 9, 668. [Google Scholar] [CrossRef] [PubMed]
- Clinical and Laboratory Standards Institute (CLSI). Performance Standards for Antimicrobial Susceptibility Testing. 29th Informational Supplement; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2019; Volume CLSI, Document M100. [Google Scholar]
- Versalovic, J.; Koeuth, T.; Lupski, J.R. Distribution of repetitive DNA sequences in eubacteria and application to fingerprinting of bacterial genomes. Nucleic Acids Res. 1991, 19, 6823–6831. [Google Scholar] [CrossRef] [PubMed]
- Horan, T.C.; Andrus, M.; Dudeck, M.A. CDC/NHSN surveillance definition of health care-associated infection and criteria for specific types of infections in the acute care setting. Am. J. Infect. Control 2008, 36, 309–332. [Google Scholar] [CrossRef]
- Kamath, P.S.; Kim, W.R. The model for end-stage liver disease (MELD). Hepatology 2007, 45, 797–805. [Google Scholar] [CrossRef]
- Manz, W.; Amann, R.; Ludwig, W.; Vancanneyt, M.; Schleifer, K.H. Application of a suite of 16S rRNA-specific oligonucleotide probes designed to investigate bacteria of the phylum cytophaga-flavobacter-bacteroides in the natural environment. Microbiology 1996, 142 Pt 5, 1097–1106. [Google Scholar] [CrossRef]
- Chang, Y.C.; Lo, H.H.; Hsieh, H.Y.; Chang, S.M. Identification, epidemiological relatedness, and biofilm formation of clinical Chryseobacterium indologenes isolates from central Taiwan. J. Microbiol. Immunol. Infect. 2015, 48, 559–564. [Google Scholar] [CrossRef]
- Deng, L.; Li, M.F.; Li, Y.H.; Yang, J.L.; Zhou, X. Chryseobacterium indologenes in four patients with leukemia. Transpl. Infect. Dis. Off. J. Transplant. Soc. 2015, 17, 583–587. [Google Scholar] [CrossRef]
- Olbrich, P.; Rivero-Garvía, M.; Falcón-Neyra, M.D.; Lepe, J.A.; Cisneros, J.M.; Marquez-Rivas, J.; Neth, O. Chryseobacterium indologenes central nervous system infection in infancy: An emergent pathogen? Infection 2014, 42, 179–183. [Google Scholar] [CrossRef]
- Afshar, M.; Nobakht, E.; Lew, S.Q. Chryseobacterium indologenes peritonitis in peritoneal dialysis. BMJ Case Rep. 2013, 2013, bcr2013009410. [Google Scholar] [CrossRef]
- Ozcan, N.; Dal, T.T.A.; Kelekci, S.; Can, S.; Ezin, O.; Kandemir, I.; Gul, K. Is Chryseobacterium indologenes a shunt-lover bacterium? A case report and review of the literature. Infez. Med. 2013, 21, 312–316. [Google Scholar] [PubMed]
- van Hoek, B.; de Rooij, B.J.; Verspaget, H.W. Risk factors for infection after liver transplantation. Best Pract. Res. Clin. Gastroenterol. 2012, 26, 61–72. [Google Scholar] [CrossRef]
- Santoro-Lopes, G.; de Gouvêa, E.F. Multidrug-resistant bacterial infections after liver transplantation: An ever-growing challenge. World J. Gastroenterol. 2014, 20, 6201–6210. [Google Scholar] [CrossRef] [PubMed]
- Righi, E. Management of bacterial and fungal infections in end stage liver disease and liver transplantation: Current options and future directions. World J. Gastroenterol. 2018, 24, 4311–4329. [Google Scholar] [CrossRef] [PubMed]
- Haque, M.; Sartelli, M.; McKimm, J.; Abu Bakar, M. Health care-associated infections—An overview. Infect. Drug. Resist. 2018, 11, 2321–2333. [Google Scholar] [CrossRef] [PubMed]
- Boncea, E.E.; Expert, P.; Honeyford, K.; Kinderlerer, A.; Mitchell, C.; Cooke, G.S.; Mercuri, L.; Costelloe, C.E. Association between intrahospital transfer and hospital-acquired infection in the elderly: A retrospective case-control study in a UK hospital network. BMJ Qual. Saf. 2021, 30, 457–466. [Google Scholar] [CrossRef]
- Hamel, M.; Zoutman, D.; O’Callaghan, C. Exposure to hospital roommates as a risk factor for health care-associated infection. Am. J. Infect. Control 2010, 38, 173–181. [Google Scholar] [CrossRef]
- Cheng, H.; Chen, B.P.; Soleas, I.M.; Ferko, N.C.; Cameron, C.G.; Hinoul, P. Prolonged Operative Duration Increases Risk of Surgical Site Infections: A Systematic Review. Surg. Infect. 2017, 18, 722–735. [Google Scholar] [CrossRef]
- Wang, J.Z.; Liu, Y.; Wang, J.L.; Lu, L.; Zhang, Y.F.; Lu, H.W.; Li, Y.M. Sequential vs simultaneous revascularization in patients undergoing liver transplantation: A meta-analysis. World J. Gastroenterol. 2015, 21, 7036–7046. [Google Scholar] [CrossRef]
- Nguyen, T.J.; Costa, M.A.; Vidar, E.N.; Shahabi, A.; Peric, M.; Hernandez, A.M.; Chan, L.S.; Sener, S.F.; Wong, A.K. Effect of immediate reconstruction on postmastectomy surgical site infection. Ann. Surg. 2012, 256, 326–333. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Antimicrobial Agent | S (%) | I (%) | R (%) | MIC50 | MIC90 | Susceptibility Breakpoint | MIC Range |
|---|---|---|---|---|---|---|---|
| Cefotaxime | 0.0 | 0.0 | 100.0 | >128 | >128 | ≤8 | 128–>128 |
| Ceftazidime | 0.0 | 0.0 | 100.0 | >128 | >128 | ≤8 | 64–>128 |
| Piperacillin–tazobactam | 56.6 | 7.5 | 35.8 | 8 | >128/4 | ≤16/4 | 2/4–>128/4 |
| Cefoperazone–sulbactam | 0.0 | 0.0 | 100.0 | >128/64 | >128/64 | ≤8/4 | 32/016–>128/64 |
| Imipenem | 0.0 | 0.0 | 100.0 | >64 | >64 | ≤4 | 64–>64 |
| Meropenem | 0.0 | 0.0 | 100.0 | >64 | >64 | ≤4 | 64–>64 |
| Levofloxacin | 1.9 | 0.0 | 98.1 | 8 | >32 | ≤2 | 1–>32 |
| Ciprofloxacin | 1.9 | 0.0 | 98.1 | 32 | >32 | ≤1 | 1–>32 |
| Amikacin | 0.0 | 0.0 | 100.0 | >128 | >128 | ≤16 | >128–>128 |
| Minocycline | 100.0 | 0.0 | 0.0 | 2 | 2 | ≤4 | 1–4 |
| TMP-SMZ | 100.0 | 0.0 | 0.0 | 0.5/9.5 | 0.5/9.5 | ≤2/38 | <0.125/2.375–1/19 |
| Rifampicin | 66.0 | 1.9 | 32.1 | 0.5 | 16 | ≤1 | <0.25–16 |
| Characteristics | Infection (n = 53) | Without Infection (n = 78) | p-Value |
|---|---|---|---|
| Male sex/n (%) | 46 (86.8%) | 72 (92.3%) | 0.300 |
| Age | |||
| Range/years | 25–75 | 19–68 | / |
| Mean ± standard deviation/years | 49.60 ± 1.48 | 48.13 ± 1.31 | 0.463 |
| ≥65 years/n (%) | 4 (7.5%) | 5 (6.4%) | >0.999 |
| BMI/mean ± standard deviation/(kg/m2) | 23.97 ± 0.55 | 23.55 ± 0.44 | 0.548 |
| MELD score | 17.91 ± 1.16 | 16.94 ± 1.03 | 0.535 |
| Diagnosis/n (%) | |||
| Hepatitis B virus | 35 (66.0%) | 61 (78.2%) | 0.122 |
| Hepatocarcinoma | 22 (41.5%) | 41 (52.6%) | 0.214 |
| Drug-induced liver failure | 4 (7.5%) | 0 (0) | 0.025 |
| Autoimmune hepatitis | 3 (5.7%) | 1 (1.3%) | 0.303 |
| Alcoholic hepatitis | 3 (5.7%) | 5 (6.4%) | 1 |
| Hepatitis C virus | 2 (3.8%) | 1 (1.3%) | 0.565 |
| Congenital liver disease | 0 (0) | 2 (2.6%) | 0.515 |
| Fatty liver | 0 (0) | 1 (1.3%) | 1 |
| Comorbidity/n (%) | |||
| Hypertension | 5 (9.4%) | 10 (12.8%) | 0.550 |
| Diabetes mellitus | 6 (11.3%) | 10 (12.8%) | 0.797 |
| Complications/n (%) | |||
| Anemia | 34 (64.2%) | 50 (64.1%) | 0.995 |
| Hypoalbuminemia | 28 (52.3%) | 26 (33.3%) | 0.026 |
| Hypoprealbuminemia | 52 (98.1%) | 68 (87.2%) | 0.028 |
| Hyponatremia | 16 (30.2%) | 16 (20.5%) | 0.206 |
| Hypokalemia | 14 (26.4%) | 10 (12.8%) | 0.048 |
| Risk factors/n (%) | |||
| Hospital history one month before surgery | 30 (56.6%) | 39 (50.0%) | 0.457 |
| Ward transfer | 10 (18.9%) | 4 (5.1%) | 0.012 |
| Number of bed transfers | |||
| One | 18 (34.9%) | 37 (47.4%) | 0.125 |
| Two or more | 33 (62.3%) | 28 (35.9%) | 0.003 |
| General anesthesia abdominal surgery ≥ 2 times/n (%) | 6 (11.3%) | 5 (6.4%) | 0.351 |
| Operation time ≥ 8 h/n (%) | 26 (49.1%) | 24 (30.8%) | 0.034 |
| Intra-operation blood transfusion volume ≥ 400mL/n (%) | 42 (79.2%) | 54 (69.2%) | 0.204 |
| Tracheotomia/n (%) | 3 (5.7%) | 3 (3.8%) | 0.685 |
| Central venous catheter/n (%) | 53 (100.0%) | 78 (100.0%) | 1 |
| Urethral catheter/n (%) | 53 (100.0%) | 78 (100.0%) | 1 |
| Indwelling urethral catheter ≥ 7 days | 21 (39.6%) | 33 (42.3%) | 0.759 |
| Abdominal drainage catheter/n (%) | 46 (86.8%) | 60 (76.9%) | 0.158 |
| Indwelling abdominal drainage ≥ 14 days/n (%) | 32 (60.4%) | 31 (39.7%) | 0.020 |
| Outcomes | |||
| Intensive care/days ± standard deviation | 11.94 ± 1.07 | 9.33 ± 0.77 | 0.045 |
| Hospital stay/days ± standard deviation | 34.47 ± 2.86 | 29.58 ± 1.53 | 0.105 |
| Overall in-hospital mortality/n (%) | 4 (7.5%) | 9 (11.5%) | 0.453 |
| Risk Factors | Multivariate Analysis | ||
|---|---|---|---|
| OR | 95% CI | p-Value | |
| Hypoprealbuminemia | 3.846 | 0.644–73.742 | 0.218 |
| Hypokalemia | 2.542 | 0.976–6.894 | 0.059 |
| Bed transfer ≥2 times | 2.408 | 1.112–5.312 | 0.027 |
| Operation time ≥8 h | 2.373 | 1.088–5.302 | 0.032 |
| Indwelling abdominal drainage ≥14 days | 1.787 | 0.821–3.934 | 0.145 |
| Factor | Points |
|---|---|
| Indwelling abdominal drainage for ≥14 days | 43 |
| Operation duration ≥ 8 h | 64 |
| Times of bed transfers ≥ 2 | 65 |
| Hypokalemia | 69 |
| Hypoprealbuminemia | 100 |
| Total Points | Odds of Infection |
|---|---|
| <53 | <10% |
| 53–113 | 10–20% |
| 113–153 | 20–30% |
| 153–186 | 30–40% |
| 186–216 | 40–50% |
| 216–246 | 50–60% |
| 246–279 | 60–70% |
| 279–319 | 70–80% |
| ≥320 | ≥80% |
| Parameter | Precision | Sensitivity | Specificity | LR+ | LR− |
|---|---|---|---|---|---|
| Value | 0.617 | 0.698 | 0.705 | 2.390 | 0.418 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, Y.; Zhao, X.; Xu, S.; Li, Y. Clinical Characteristics and Risk Factors for Intra-Abdominal Infection with Chryseobacterium indologenes after Orthotopic Liver Transplantation. Pathogens 2022, 11, 1126. https://doi.org/10.3390/pathogens11101126
Zhang Y, Zhao X, Xu S, Li Y. Clinical Characteristics and Risk Factors for Intra-Abdominal Infection with Chryseobacterium indologenes after Orthotopic Liver Transplantation. Pathogens. 2022; 11(10):1126. https://doi.org/10.3390/pathogens11101126
Chicago/Turabian StyleZhang, Yixin, Xiaoyu Zhao, Su Xu, and Ying Li. 2022. "Clinical Characteristics and Risk Factors for Intra-Abdominal Infection with Chryseobacterium indologenes after Orthotopic Liver Transplantation" Pathogens 11, no. 10: 1126. https://doi.org/10.3390/pathogens11101126
APA StyleZhang, Y., Zhao, X., Xu, S., & Li, Y. (2022). Clinical Characteristics and Risk Factors for Intra-Abdominal Infection with Chryseobacterium indologenes after Orthotopic Liver Transplantation. Pathogens, 11(10), 1126. https://doi.org/10.3390/pathogens11101126