
Pattern of Respiratory Viruses among Pilgrims during 2019 Hajj Season Who Sought Healthcare Due to Severe Respiratory Symptoms

 ,
,  , , , , and
, , , , and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Ethical Approval
2.2. Study Design
2.3. RNA Extraction and Molecular Detection of Respiratory Viruses
2.4. Statistical Analysis
3. Results
3.1. Characteristics of the Pilgrims Enrolled in the Study
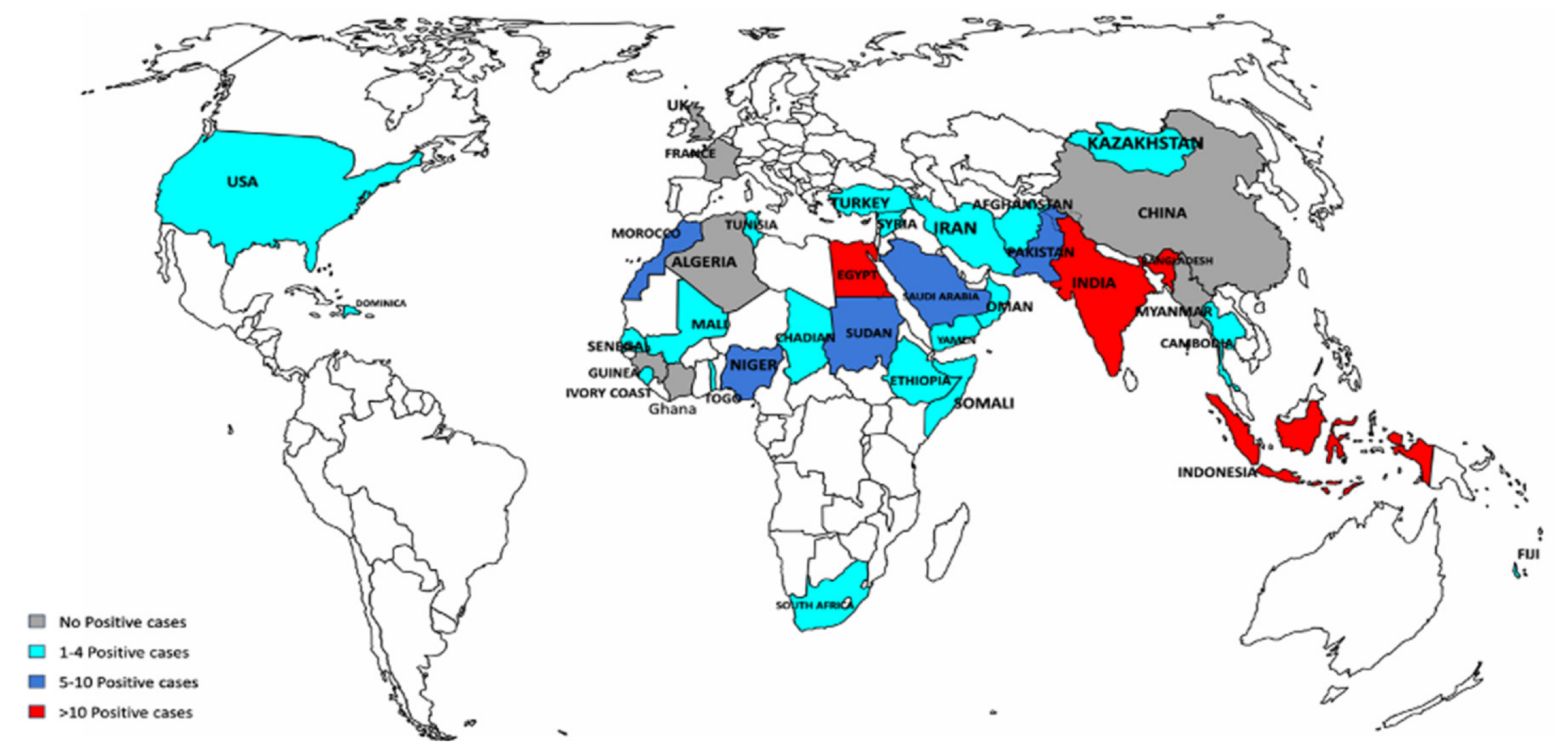
3.2. Detection of Respiratory Viruses by Pligrims’ Country of Origin
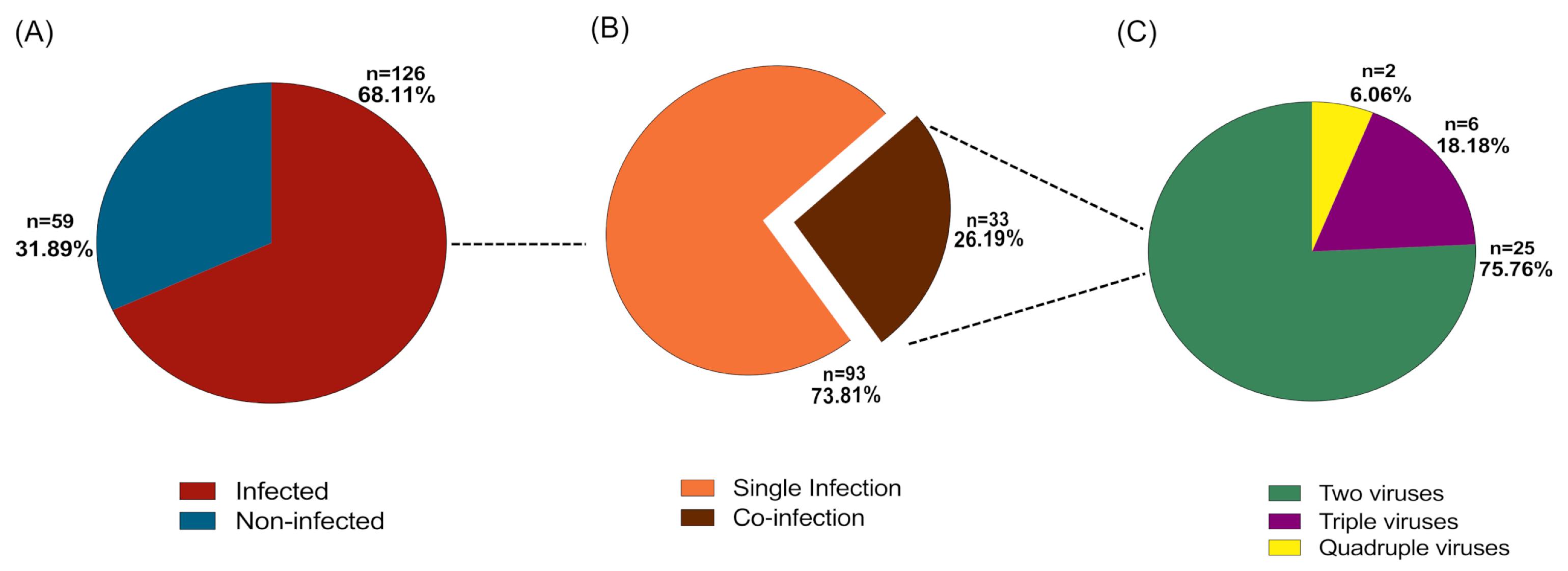
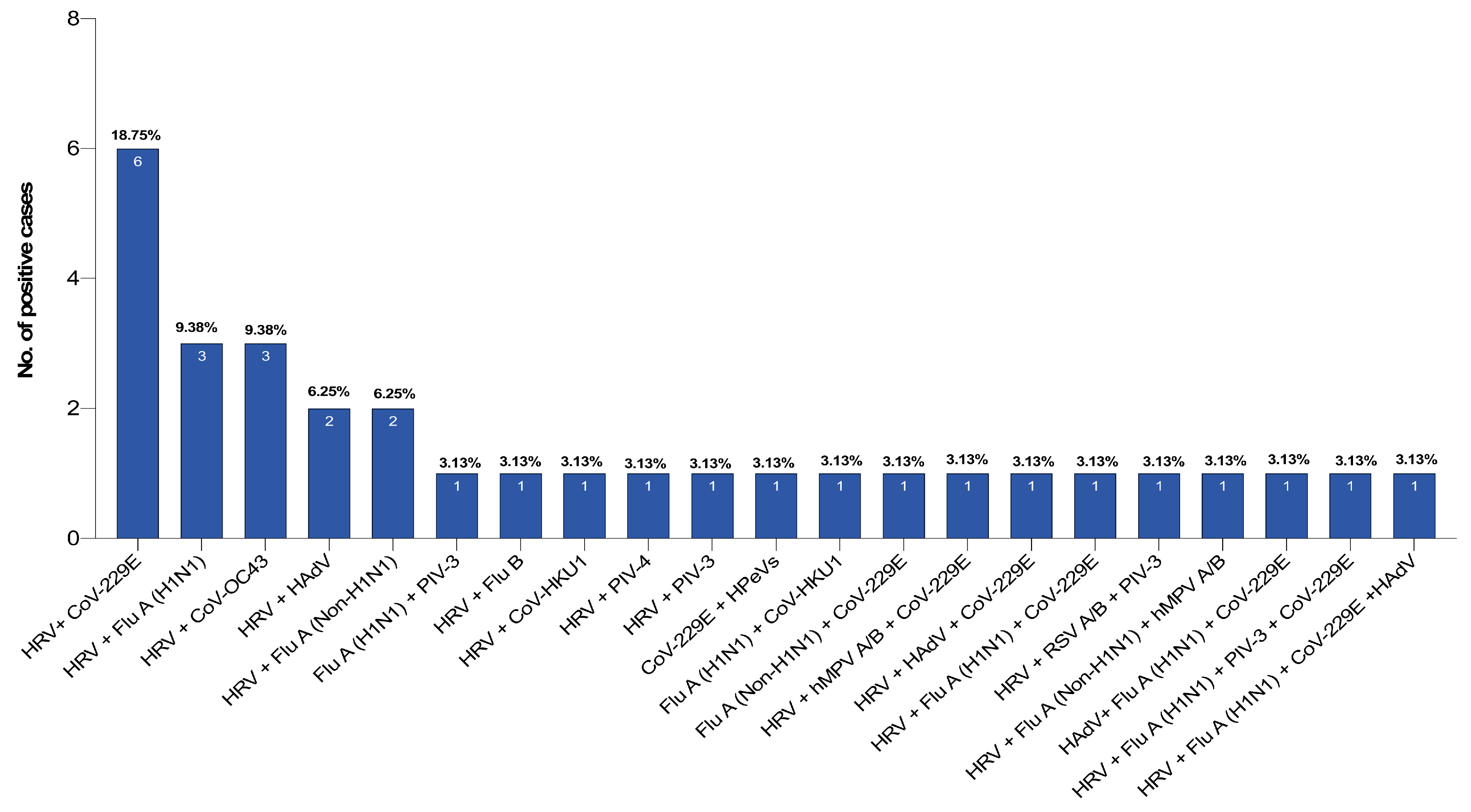
3.3. The Prevalence of Single Infection and Coinfection among the Pilgrims
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Petersen, E.; Memish, Z.A.; Zumla, A.; Maani, A.A. Transmission of respiratory tract infections at mass gathering events. Curr. Opin Pulm. Med. 2020, 26, 197–202. [Google Scholar] [CrossRef]
- Memish, Z.A.; Steffen, R.; White, P.; Dar, O.; Azhar, E.I.; Sharma, A.; Zumla, A. Mass gatherings medicine: Public health issues arising from mass gathering religious and sporting events. Lancet 2019, 393, 2073–2084. [Google Scholar] [CrossRef]
- Al-Tawfiq, J.A.; Benkouiten, S.; Memish, Z.A. A systematic review of emerging respiratory viruses at the Hajj and possible coinfection with Streptococcus pneumoniae. Travel Med. Infect. Dis. 2018, 23, 6–13. [Google Scholar] [CrossRef] [PubMed]
- Tam, J.S.; Barbeschi, M.; Shapovalova, N.; Briand, S.; Memish, Z.A.; Kieny, M.-P. Research agenda for mass gatherings: A call to action. Lancet Infect. Dis. 2012, 12, 231–239. [Google Scholar] [CrossRef]
- Mani, G. Mass Gatherings: Public Health implications and opportunities. Public Health Indones. 2017, 3, 4–6. [Google Scholar] [CrossRef]
- Memish, Z.A.; Zumla, A.; Alhakeem, R.F.; Assiri, A.; Turkestani, A.; Al Harby, K.D.; Alyemni, M.; Dhafar, K.; Gautret, P.; Barbeschi, M. Hajj: Infectious disease surveillance and control. Lancet 2014, 383, 2073–2082. [Google Scholar] [CrossRef]
- Aldossari, M.; Aljoudi, A.; Celentano, D. Health issues in the Hajj pilgrimage: A literature review. East. Mediterr. Health J. 2019, 25, 744–753. [Google Scholar] [CrossRef] [PubMed]
- Hashem, A.M.; Al-Subhi, T.L.; Badroon, N.A.; Hassan, A.M.; Bajrai, L.H.M.; Banassir, T.M.; Alquthami, K.M.; Azhar, E.I. MERS-CoV, influenza and other respiratory viruses among symptomatic pilgrims during 2014 Hajj season. J. Med Virol. 2019, 91, 911–917. [Google Scholar] [CrossRef]
- Barasheed, O.; Rashid, H.; Alfelali, M.; Tashani, M.; Azeem, M.; Bokhary, H.; Kalantan, N.; Samkari, J.; Heron, L.; Kok, J.; et al. Viral respiratory infections among Hajj pilgrims in 2013. Virol. Sin. 2014, 29, 364–371. [Google Scholar] [CrossRef]
- Khamis, N.K. Epidemiological pattern of diseases and risk behaviors of pilgrims attending mina hospitals, hajj 1427 h (2007 g). J. Egypt. Public Health Assoc. 2008, 83, 15–33. [Google Scholar]
- Gautret, P.; Benkouiten, S.; Al-Tawfiq, J.A.; Memish, Z.A. Hajj-associated viral respiratory infections: A systematic review. Travel Med. Infect. Dis. 2016, 14, 92–109. [Google Scholar] [CrossRef] [PubMed]
- Benkouiten, S.; Charrel, R.; Belhouchat, K.; Drali, T.; Nougairede, A.; Salez, N.; Memish, Z.A.; Al Masri, M.; Fournier, P.-E.; Raoult, D. Respiratory viruses and bacteria among pilgrims during the 2013 Hajj. Emerg. Infect. Dis. 2014, 20, 1821. [Google Scholar] [CrossRef] [PubMed]
- Memish, Z.A.; Assiri, A.; Turkestani, A.; Yezli, S.; Al Masri, M.; Charrel, R.; Drali, T.; Gaudart, J.; Edouard, S.; Parola, P.; et al. Mass gathering and globalization of respiratory pathogens during the 2013 Hajj. Clin. Microbiol. Infect. 2015, 21, 571.e1–571.e8. [Google Scholar] [CrossRef]
- Al-Abdallat, M.M.; Rha, B.; Alqasrawi, S.; Payne, D.C.; Iblan, I.; Binder, A.M.; Haddadin, A.; Al Nsour, M.; Alsanouri, T.; Mofleh, J. Acute respiratory infections among returning Hajj pilgrims—Jordan, 2014. J. Clin. Virol. 2017, 89, 34–37. [Google Scholar] [CrossRef]
- Annan, A.; Owusu, M.; Marfo, K.S.; Larbi, R.; Sarpong, F.N.; Adu-Sarkodie, Y.; Amankwa, J.; Fiafemetsi, S.; Drosten, C.; Owusu-Dabo, E. High prevalence of common respiratory viruses and no evidence of Middle East respiratory syndrome coronavirus in Hajj pilgrims returning to Ghana, 2013. Trop. Med. Int. Health 2015, 20, 807–812. [Google Scholar] [CrossRef] [PubMed]
- Imani, R.; Karimi, A.; Habibian, R. Acute respiratory viral infections among Tamattu’Hajj pilgrims in Iran. Life Sci. J. 2013, 10. [Google Scholar]
- Memish, Z.A.; Almasri, M.; Turkestani, A.; Al-Shangiti, A.M.; Yezli, S. Etiology of severe community-acquired pneumonia during the 2013 Hajj—part of the MERS-CoV surveillance program. Int. J. Infect. Dis. 2014, 25, 186–190. [Google Scholar] [CrossRef] [PubMed]
- Choudhry, A.J.; Al-Mudaimegh, K.S.; Turkistani, A.M.; Al-Hamdan, N.A. Hajj-associated acute respiratory infection among hajjis from Riyadh. East. Mediterr. Health J. 2006, 12, 300–309. [Google Scholar]
- Alborzi, A.; Aelami, M.H.; Ziyaeyan, M.; Jamalidoust, M.; Moeini, M.; Pourabbas, B.; Abbasian, A. Viral Etiology of Acute Respiratory Infections Among Iranian Hajj Pilgrims, 2006. J. Travel Med. 2009, 16, 239–242. [Google Scholar] [CrossRef]
- Gautret, P.; Soula, G.; Parola, P.; Brouqui, P. Hajj pilgrims’ knowledge about acute respiratory infections. Emerg. Infect. Dis. 2009, 15, 1861–1862. [Google Scholar] [CrossRef]
- Gautret, P.; Benkouiten, S.; Griffiths, K.; Sridhar, S. The inevitable Hajj cough: Surveillance data in French pilgrims, 2012–2014. Travel Med. Infect. Dis. 2015, 13, 485–489. [Google Scholar] [CrossRef]
- Koul, P.A.; Mir, H.; Saha, S.; Chadha, M.S.; Potdar, V.; Widdowson, M.A.; Lal, R.B.; Krishnan, A. Respiratory viruses in returning Hajj & Umrah pilgrims with acute respiratory illness in 2014-2015. Indian J. Med. Res. 2018, 148, 329–333. [Google Scholar]
- Bakhsh, A.R.; Sindy, A.I.; Baljoon, M.J.; Dhafar, K.O.; Gazzaz, Z.J.; Baig, M.; Deiab, B.A.; Al Hothali, F.T. Diseases pattern among patients attending Holy Mosque (Haram) medical centers during Hajj 1434 (2013). Saudi Med J. 2015, 36, 962. [Google Scholar] [CrossRef]
- Ahmed, Q.A.; Arabi, Y.M.; Memish, Z.A. Health risks at the Hajj. Lancet 2006, 367, 1008–1015. [Google Scholar] [CrossRef]
- Shafi, S.; Dar, O.; Khan, M.; Khan, M.; Azhar, E.I.; McCloskey, B.; Zumla, A.; Petersen, E. The annual Hajj pilgrimage-minimizing the risk of ill health in pilgrims from Europe and opportunity for driving the best prevention and health promotion guidelines. Int. J. Infect. Dis. 2016, 47, 79–82. [Google Scholar] [CrossRef]
- Al-Masud, S.M.R.; Bakar, A.A.; Yussof, S. Determining the types of diseases and emergency issues in Pilgrims during Hajj: A literature review. Stat. Inf. 2016, 5, 7. [Google Scholar]
- Alzeer, A.H. Respiratory tract infection during Hajj. Ann. Thorac. Med. 2009, 4, 50. [Google Scholar] [CrossRef] [PubMed]
- Wilder-Smith, A.; Foo, W.; Earnest, A.; Paton, N.I. High risk of Mycobacterium tuberculosis infection during the Hajj pilgrimage. Trop. Med. Int. Health 2005, 10, 336–339. [Google Scholar] [CrossRef] [PubMed]
- Al-Asmary, S.; Al-Shehri, A.S.; Abou-Zeid, A.; Abdel-Fattah, M.; Hifnawy, T.; El-Said, T. Acute respiratory tract infections among Hajj medical mission personnel, Saudi Arabia. Int. J. Infect. Dis. 2007, 11, 268–272. [Google Scholar] [CrossRef]
- Hoang, V.-T.; Ali-Salem, S.; Belhouchat, K.; Meftah, M.; Sow, D.; Dao, T.-L.; Ly, T.D.A.; Drali, T.; Ninove, L.; Yezli, S.; et al. Respiratory tract infections among French Hajj pilgrims from 2014 to 2017. Sci. Rep. 2019, 9, 17771. [Google Scholar] [CrossRef] [PubMed]
- Al-Tawfiq, J.A.; Gautret, P.; Memish, Z.A. Expected immunizations and health protection for Hajj and Umrah 2018—An overview. Travel Med. Infect. Dis. 2017, 19, 2–7. [Google Scholar] [CrossRef] [PubMed]
- Bokhary, H.; Barasheed, O.; Abd El Ghany, M.; Khatami, A.; Hill-Cawthorne, G.A.; Rashid, H.; Hajj Research, T. Pilot Survey of Knowledge, Attitudes and Perceptions of Hajj Deployed Health Care Workers on Antibiotics and Antibiotic Prescriptions for Upper Respiratory Tract Infections: Results from Two Hajj Seasons. Trop Med. Infect. Dis. 2020, 5, 18. [Google Scholar] [CrossRef] [PubMed]
- Al-Tawfiq, J.A.; Zumla, A.; Memish, Z.A. Respiratory tract infections during the annual Hajj: Potential risks and mitigation strategies. Curr. Opin. Pulm. Med. 2013, 19, 192–197. [Google Scholar] [CrossRef] [PubMed]
- Benkouiten, S.; Al-Tawfiq, J.A.; Memish, Z.A.; Albarrak, A.; Gautret, P. Clinical respiratory infections and pneumonia during the Hajj pilgrimage: A systematic review. Travel Med. Infect. Dis. 2019, 28, 15–26. [Google Scholar] [CrossRef]
- AlMazroa, M.A.; Memish, Z.A.; AlWadey, A.M. Pandemic influenza A (H1N1) in Saudi Arabia: Description of the first one hundred cases. Ann. Saudi Med. 2010, 30, 11–14. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Description | n (%) * | Infected n (%) ** | p Value *** |
|---|---|---|---|---|
| Gender | Male | 122 (65.95%) | 81 (64.29%) | 0.486 |
| Female | 63 (34.05%) | 45 (35.71%) | ||
| Age group | <60 | 71 (39.46%) | 42 (33.33%) | 0.039 |
| ≥60 | 114 (60.54%) | 84 (66.67%) | ||
| Total | 185 | 126 (68.11%) | ||
| Infecting Virus | Total | Gender | Age Groups | ||
|---|---|---|---|---|---|
| Male | Female | <60 | ≥60 | ||
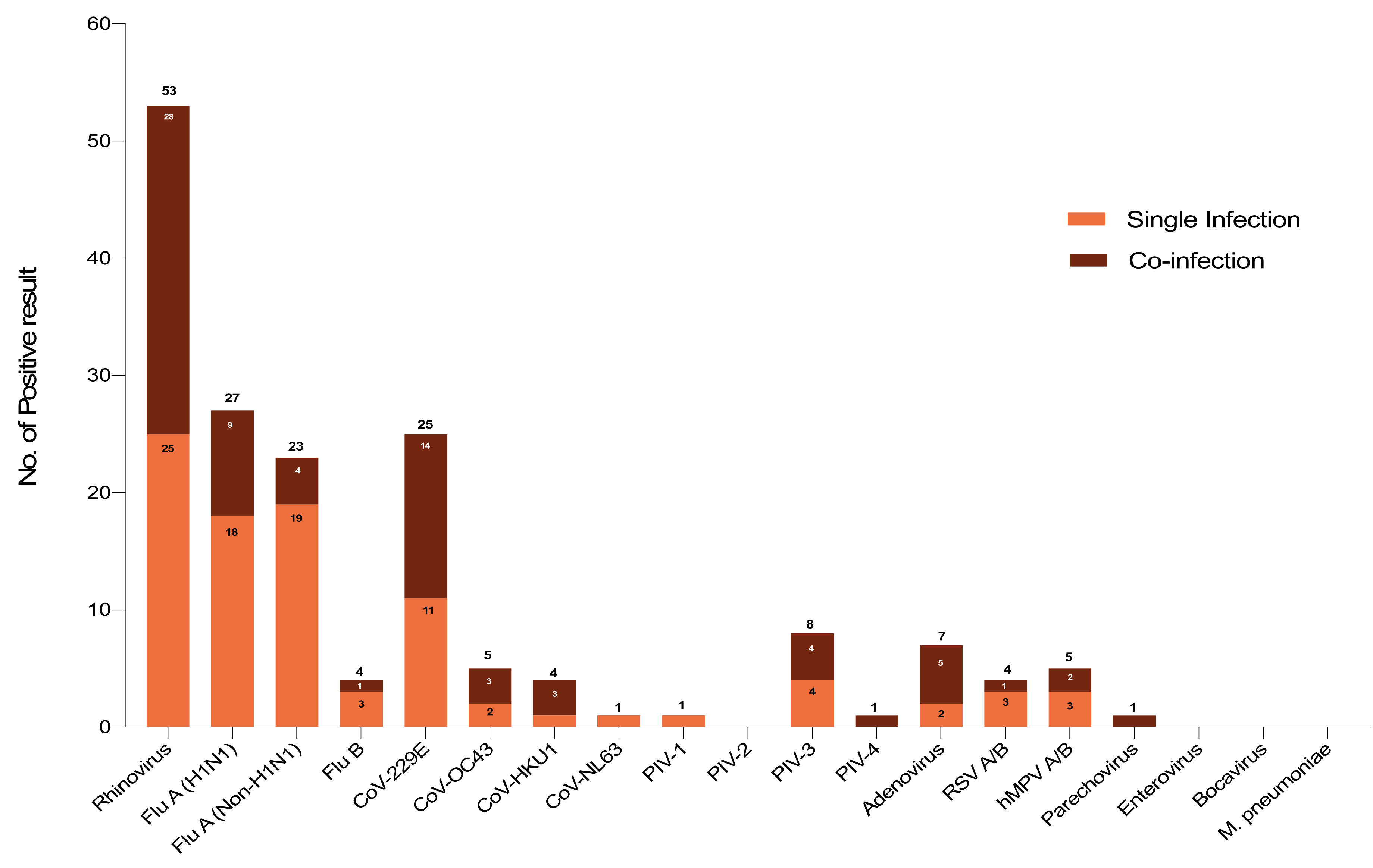
| Rhinovirus | 53 | 38 (71.70%) | 15 (28.30%) | 14 (26.42%) | 39 (73.58%) |
| Influenza A (H1N1) | 27 | 14 (51.85%) | 13 (48.15%) | 7 (25.93%) | 20 (74.07%) |
| Influenza A (Non-H1N1) | 23 | 16 (69.57%) | 7 (30.43%) | 12 (52.17%) | 11 (47.83%) |
| Influenza B | 4 | 1 (25.00%) | 3 (75.00%) | 3 (75.00%) | 1 (25.00%) |
| CoV-229E | 25 | 14 (56.00%) | 11 (44.00%) | 9 (36.00%) | 16 (64.00%) |
| CoV-OC43 | 5 | 2 (40.00%) | 3 (60.00%) | 0 (0.00%) | 5 (100.00%) |
| CoV-HKU1 | 4 | 3 (75.00%) | 1 (25.00%) | 2 (50.00%) | 2 (50.00%) |
| CoV-NL63 | 1 | 0 (0.00%) | 1 (100.00%) | 0 (0.00%) | 1 (100.00%) |
| PIV-1 | 1 | 1 (100.00%) | 0 (0.00%) | 0 (0.00%) | 1 (100.00%) |
| PIV-2 | 0 | 0 (0.00%) | 0 (0.00%) | 0 (0.00%) | 0 (0.00%) |
| PIV-3 | 8 | 8 (100.00%) | 0 (0.00%) | 2 (25.00%) | 6 (75.00%) |
| PIV-4 | 1 | 1 (100.00%) | 0 (0.00%) | 0 (0.00%) | 1 (100.00%) |
| Adenovirus | 7 | 5 (71.43%) | 2 (28.57%) | 1 (14.29%) | 6 (85.71%) |
| RSV A/B | 4 | 4 (100.00%) | 0 (0.00%) | 2 (50.00%) | 2 (50.00%) |
| HMPV A/B | 5 | 4 (80.00%) | 1 (20.00%) | 2 (40.00%) | 3 (60.00%) |
| Parechovirus | 1 | 0 (0.00%) | 1 (100.00%) | 0 (0.00%) | 1 (100.00%) |
| Enterovirus | 0 | 0 (0.00%) | 0 (0.00%) | 0 (0.00%) | 0 (0.00%) |
| Bocavirus | 0 | 0 (0.00%) | 0 (0.00%) | 0 (0.00%) | 0 (0.00%) |
| M. pneumoniae | 0 | 0 (0.00%) | 0 (0.00%) | 0 (0.00%) | 0 (0.00%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alsayed, S.M.; Alandijany, T.A.; El-Kafrawy, S.A.; Hassan, A.M.; Bajrai, L.H.; Faizo, A.A.; Mulla, E.A.; Aljahdali, L.S.; Alquthami, K.M.; Zumla, A.; et al. Pattern of Respiratory Viruses among Pilgrims during 2019 Hajj Season Who Sought Healthcare Due to Severe Respiratory Symptoms. Pathogens 2021, 10, 315. https://doi.org/10.3390/pathogens10030315
Alsayed SM, Alandijany TA, El-Kafrawy SA, Hassan AM, Bajrai LH, Faizo AA, Mulla EA, Aljahdali LS, Alquthami KM, Zumla A, et al. Pattern of Respiratory Viruses among Pilgrims during 2019 Hajj Season Who Sought Healthcare Due to Severe Respiratory Symptoms. Pathogens. 2021; 10(3):315. https://doi.org/10.3390/pathogens10030315
Chicago/Turabian StyleAlsayed, Salma M., Thamir A. Alandijany, Sherif A. El-Kafrawy, Ahmed M. Hassan, Leena H. Bajrai, Arwa A. Faizo, Eman A. Mulla, Lujain S. Aljahdali, Khalid M. Alquthami, Alimuddin Zumla, and et al. 2021. "Pattern of Respiratory Viruses among Pilgrims during 2019 Hajj Season Who Sought Healthcare Due to Severe Respiratory Symptoms" Pathogens 10, no. 3: 315. https://doi.org/10.3390/pathogens10030315
APA StyleAlsayed, S. M., Alandijany, T. A., El-Kafrawy, S. A., Hassan, A. M., Bajrai, L. H., Faizo, A. A., Mulla, E. A., Aljahdali, L. S., Alquthami, K. M., Zumla, A., & Azhar, E. I. (2021). Pattern of Respiratory Viruses among Pilgrims during 2019 Hajj Season Who Sought Healthcare Due to Severe Respiratory Symptoms. Pathogens, 10(3), 315. https://doi.org/10.3390/pathogens10030315