
Whole Genome Sequencing and Antimicrobial Resistance of Staphylococcus aureus from Surgical Site Infections in Ghana

 , , , , ,
, , , , ,
Abstract
1. Introduction
2. Results
2.1. Proportions of Subjects Positive for Staphylococcus aureus and Antimicrobial Resistance
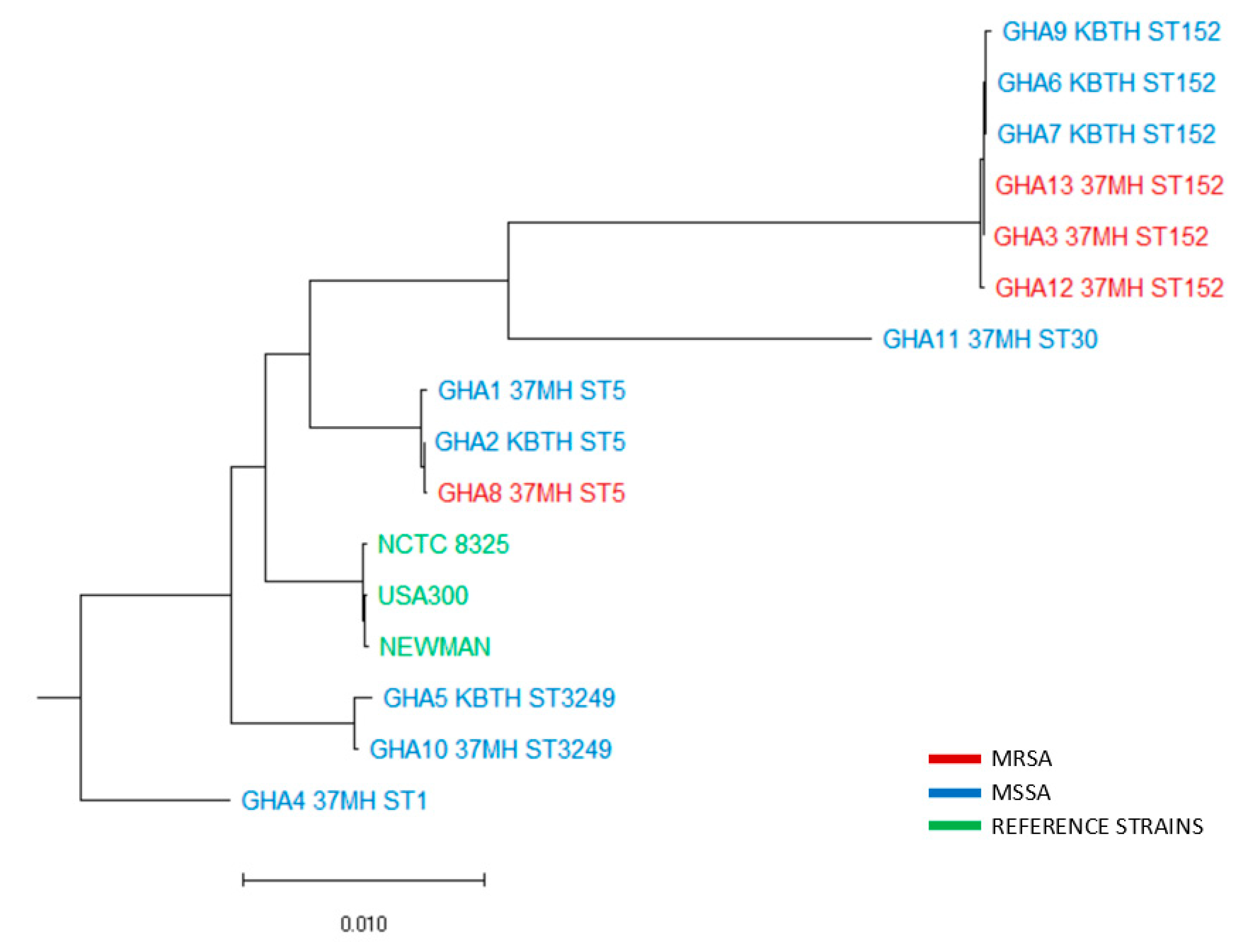
2.2. Whole-Genome Sequence Analysis
3. Discussion
4. Materials and Methods
4.1. Study Design, Site, and Sampling Procedures
4.2. Isolation and Identification of S. aureus
4.3. Antimicrobial Susceptibility Testing
4.4. PCR Detection of spa, pvl, and mecA genes
4.5. Whole-Genome Sequencing
4.6. Data Analysis
5. Conclusions
6. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Centers for Disease Control and Prevention (CDC). National Healthcare Safety Network (NHSN). Surgical Site Infection (SSI) Event. Procedure-Associated Module SSI. January 2015; CDC: Atlanta, GA, USA. Available online: www.cdc.gov/nhsn/PDFs/pscManual/9pscSSI (accessed on 13 March 2019).
- Smyth, E.T.; McIlvenny, G.; Enstone, J.E.; Emmerson, A.M.; Humphreys, H.; Fitzpatrick, F.; Davies, E.; Newcombe, R.G.; Spencer, R.C. Hospital Infection Society Prevalence Survey Steering Group. Four country healthcare associated infection prevalence survey 2006: Overview of the results. J. Hosp. Infect. 2008, 69, 230–248. [Google Scholar] [CrossRef]
- Allegranzi, B.; Nejad, S.B.; Combescure, C.; Graafmans, W.; Attar, H.; Donaldson, L.; Pittet, D. Burden of endemic health-care-associated infection in developing countries: Systematic review and meta-analysis. Lancet 2011, 377, 228–241. [Google Scholar] [CrossRef]
- Klevens, R.M.; Edwards, J.R.; Richards, J.C.L.; Horan, T.C.; Gaynes, R.P.; Pollock, D.A.; Cardo, D.M. Estimating health care-associated infections and deaths in US hospitals, 2002. Public Health Rep. 2007, 122, 160–166. [Google Scholar] [CrossRef] [PubMed]
- Labi, A.K.; Obeng-Nkrumah, N.; Owusu, E.; Bjerrum, S.; Bediako-Bowan, A.; Sunkwa-Mills, G.; Akufo, C.; Fenny, A.P.; Opintan, J.A.; Enweronu-Laryea, C.; et al. Multi-centre point-prevalence survey of hospital-acquired infections in Ghana. J. Hosp. Infect. 2019, 101, 60–68. [Google Scholar] [CrossRef] [PubMed]
- Magill, S.S.; Hellinger, W.; Cohen, J.; Kay, R.; Bailey, C.; Boland, B.; Carey, D.; de Guzman, J.; Dominguez, K.; Edwards, J.; et al. Prevalence of healthcare-associated infections in acute care hospitals in Jacksonville, Florida. Infect. Control Hosp. Epidemiol. 2012, 33, 283–291. [Google Scholar] [CrossRef]
- Awad, S.S. Adherence to surgical care improvement project measures and post-operative surgical site infections. Surg. Infect. 2012, 13, 234–237. [Google Scholar] [CrossRef]
- Grimble, S.A.; Magee, T.R.; Galland, R.B. Methicillin resistant Staphylococcus aureus in patients undergoing major amputation. Eur. J. Vasc. Endovasc. Surg. 2001, 22, 215–218. [Google Scholar] [CrossRef]
- Merkow, R.P.; Ju, M.H.; Chung, J.W.; Hall, B.L.; Cohen, M.E.; Williams, M.V.; Tsai, T.C.; Ko, C.Y.; Bilimoria, K.Y. Underlying reasons associated with hospital readmission following surgery in the United States. JAMA 2015, 313, 483–495. [Google Scholar] [CrossRef]
- Zimlichman, E.; Henderson, D.; Tamir, O.; Franz, C.; Song, P.; Yamin, C.K.; Keohane, C.; Denham, C.R.; Bates, D.W. Health care–associated infections: A meta-analysis of costs and financial impact on the US health care system. JAMA Intern. Med. 2013, 173, 2039–2046. [Google Scholar] [CrossRef]
- Dhar, H.; Al-Busaidi, I.; Rathi, B.; Nimre, E.A.; Sachdeva, V.; Hamdi, I. A study of post-caesarean section wound infections in a regional referral hospital, Oman. Sultan Qaboos Univ. Med. J. 2014, 14, 211. [Google Scholar]
- Lilani, S.P.; Jangale, N.; Chowdhary, A.; Daver, G.B. Surgical site infection in clean and clean-contaminated cases. Indian J. Med. Microbiol. 2005, 23, 249. [Google Scholar] [PubMed]
- Mpogoro, F.J.; Mshana, S.E.; Mirambo, M.M.; Kidenya, B.R.; Gumodoka, B.; Imirzalioglu, C. Incidence and predictors of surgical site infections following caesarean sections at Bugando Medical Centre, Mwanza, Tanzania. Antimicrob. Resist. Infect. Control 2014, 3, 25. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, E.F.; Gad, G.F.; Abdalla, A.M.; Hasaneen, A.M.; Abdelwahab, S.F. Prevalence of methicillin resistant Staphylococcus aureus among Egyptian patients after surgical interventions. Surg. Infect. 2014, 15, 404–411. [Google Scholar] [CrossRef]
- Falagas, M.E.; Karageorgopoulos, D.E.; Leptidis, J.; Korbila, I.P. MRSA in Africa: Filling the global map of antimicrobial resistance. PLoS ONE 2013, 8, e68024. [Google Scholar] [CrossRef]
- Iyamba, J.M.; Wambale, J.M.; Lukukula, C.M. High prevalence of methicillin resistant staphylococci strains isolated from surgical site infections in Kinshasa. Pan Afr. Med. J. 2014, 18, 322. [Google Scholar] [CrossRef]
- Kheder, S.I.; Ali, N.A.; Fathelrahman, A.I. Prevalence and Antimicrobial Susceptibility Pattern of Methicillin Resistance Staphylococcus in a Sudanese Surgical Ward. Pharmacol. Pharm. 2012, 3, 103–108. [Google Scholar] [CrossRef]
- Dessie, W.; Mulugeta, G.; Fentaw, S.; Mihret, A.; Hassen, M.; Abebe, E. Pattern of bacterial pathogens and their susceptibility isolated from surgical site infections at selected referral hospitals, Addis Ababa, Ethiopia. Int. J. Microb. 2016, 2016, 1–8. [Google Scholar] [CrossRef]
- Malik, Z.I.; Nawaz, T.; Abdullah, M.T.; Waqar, S.H.; Zahid, M.A. Surgical site infections in general surgical wards at a tertiary care hospital. Pak. J. Med. Res. 2013, 52, 116. [Google Scholar]
- Feglo, P.; Afriyie-Asante, A. Environmental impact on postoperative wound infections in a privately-owned hospital in Ghana. Afr. J. Microbiol. Res. 2014, 8, 1620–1626. [Google Scholar] [CrossRef]
- Schaumburg, F.; Alabi, A.S.; Peters, G.; Becker, K. New epidemiology of Staphylococcus aureus infection in Africa. Clin. Microbiol. Infect. 2014, 20, 589–596. [Google Scholar] [CrossRef]
- Gu, F.F.; Han, L.Z.; Chen, X.; Wang, Y.C.; Shen, H.; Wang, J.Q.; Tang, J.; Zhang, J.; Ni, Y.X. Molecular characterization of Staphylococcus aureus from surgical site infections in orthopedic patients in an orthopedic trauma clinical medical center in Shanghai. Surg. Infect. 2015, 16, 97–104. [Google Scholar] [CrossRef] [PubMed]
- Gardete, S.; Tomasz, A. Mechanisms of vancomycin resistance in Staphylococcus aureus. J. Clin. Invest. 2014, 124, 2836–2840. [Google Scholar] [CrossRef] [PubMed]
- Egyir, B.; Guardabassi, L.; Nielsen, S.S.; Larsen, J.; Addo, K.K.; Newman, M.J.; Larsen, A.R. Prevalence of nasal carriage and diversity of Staphylococcus aureus among inpatients and hospital staff at Korle Bu Teaching Hospital, Ghana. J. Glob. Antimicrob. Resist. 2013, 1, 189–193. [Google Scholar] [CrossRef] [PubMed]
- Egyir, B.; Guardabassi, L.; Esson, J.; Nielsen, S.S.; Newman, M.J.; Addo, K.K.; Larsen, A.R. Insights into nasal carriage of Staphylococcus aureus in an urban and a rural community in Ghana. PLoS ONE 2014, 9, e96119. [Google Scholar] [CrossRef] [PubMed]
- Egyir, B.; Guardabassi, L.; Sørum, M.; Nielsen, S.S.; Kolekang, A.; Frimpong, E.; Addo, K.K.; Newman, M.J.; Larsen, A.R. Molecular epidemiology and antimicrobial susceptibility of clinical Staphylococcus aureus from healthcare institutions in Ghana. PLoS ONE 2014, 9, e3047. [Google Scholar] [CrossRef]
- Egyir, B.; Guardabassi, L.; Monecke, S.; Addo, K.K.; Newman, M.J.; Larsen, A.R. Methicillin-resistant Staphylococcus aureus strains from Ghana include USA300. J. Glob. Antimicrob. Resist. 2015, 3, 26–30. [Google Scholar] [CrossRef]
- Ahmed, M.I. Prevalence of nosocomial wound infection among postoperative patients and antibiotics patterns at teaching hospital in Sudan. N. Am. J. Med. Sci. 2012, 4, 29. [Google Scholar] [CrossRef]
- Seni, J.; Bwanga, F.; Najjuka, C.F.; Makobore, P.; Okee, M.; Mshana, S.E.; Kidenya, B.R.; Joloba, M.L.; Kateete, D.P. Molecular characterization of Staphylococcus aureus from patients with surgical site infections at Mulago Hospital in Kampala, Uganda. PLoS ONE 2013, 8, e66153. [Google Scholar] [CrossRef] [PubMed]
- Labi, A.K.; Obeng-Nkrumah, N.; Nartey, E.T.; Bjerrum, S.; Adu-Aryee, N.A.; Ofori-Adjei, Y.A.; Yawson, A.E.; Newman, M.J. Antibiotic use in a tertiary healthcare facility in Ghana: A point prevalence survey. Antimicrob. Resist. Infect. Control 2018, 7, 15. [Google Scholar] [CrossRef]
- Breurec, S.; Fall, C.; Pouillot, R.; Boisier, P.; Brisse, S.; Diene-Sarr, F.; Djibo, S.; Etienne, J.; Fonkoua, M.C.; Perrier-Gros-Claude, J.D.; et al. Epidemiology of methicillin-susceptible Staphylococcus aureus lineages in five major African towns: High prevalence of Panton-Valentine leukocidin genes. Clin. Microbiol. Infect. 2011, 17, 633–639. [Google Scholar] [CrossRef] [PubMed]
- Dekker, D.; Wolters, M.; Mertens, E.; Boahen, K.G.; Krumkamp, R.; Eibach, D.; Schwarz, N.; Adu-Sarkodie, Y.; Rohde, H.; Christner, M.; et al. Antibiotic resistance and clonal diversity of invasive Staphylococcus aureus in the rural Ashanti Region, Ghana. BMC Infect. Dis. 2016, 16, 720. [Google Scholar] [CrossRef] [PubMed]
- Donkor, E.S.; Jamrozy, D.; Mills, R.O.; Dankwah, T.; Amoo, P.K.; Egyir, B.; Badoe, E.V.; Twasam, J.; Bentley, S.D. A genomic infection control study for Staphylococcus aureus in two Ghanaian hospitals. Infect. Drug Resist. 2018, 11, 1757. [Google Scholar] [CrossRef] [PubMed]
- Ruimy, R.; Maiga, A.; Armand-Lefevre, L.; Maiga, I.; Diallo, A.; Koumaré, A.K.; Ouattara, K.; Soumaré, S.; Gaillard, K.; Lucet, J.C.; et al. The carriage population of Staphylococcus aureus from Mali is composed of a combination of pandemic clones and the divergent Panton-Valentine leukocidin-positive genotype ST152. J. Bacteriol. 2008, 190, 3962–3968. [Google Scholar] [CrossRef]
- Monecke, S.; Berger-Bächi, B.; Coombs, G.; Holmes, A.; Kay, I.; Kearns, A.; Linde, H.J.; O’Brien, F.; Slickers, P.; Ehricht, R. Comparative genomics and DNA array-based genotyping of pandemic Staphylococcus aureus strains encoding Panton-Valentine leukocidin. Clin. Microbiol. Infect. 2007, 13, 236–249. [Google Scholar] [CrossRef]
- Müller-Premru, M.; Strommenge, B.; Alikadic, N.; Witte, W.; Friedrich, A.W.; Seme, K.; Kucina, N.S.; Smrke, D.; Spik, V.; Gubina, M. New strains of community-acquired methicillin-resistant Staphylococcus aureus with Panton–Valentine leukocidin causing an outbreak of severe soft tissue infection in a football team. Eur. J. Clin. Microbiol. Infect. Dis. 2005, 24, 848–850. [Google Scholar] [CrossRef]
- Linde, H.; Wagenlehner, F.; Strommenger, B.; Drubel, I.; Tanzer, J.; Reischl, U.; Raab, U.; Höller, C.; Naber, K.G.; Witte, W.; et al. Healthcare-associated outbreaks and community-acquired infections due to MRSA carrying the Panton-Valentine leucocidin gene in southeastern Germany. Eur. J. Clin. Microbiol. Infect. Dis. 2005, 24, 419–422. [Google Scholar] [CrossRef]
- Goering, R.V.; Shawar, R.M.; Scangarella, N.E.; O’Hara, F.P.; Amrine-Madsen, H.; West, J.M.; Dalessandro, M.; Becker, J.A.; Walsh, S.L.; Miller, L.A.; et al. Molecular epidemiology of methicillin-resistant and methicillin-susceptible Staphylococcus aureus isolates from global clinical trials. J. Clin. Microbiol. 2008, 46, 2842–2847. [Google Scholar] [CrossRef]
- Amissah, N.A.; Van Dam, L.; Ablordey, A.; Ampomah, O.W.; Prah, I.; Tetteh, C.S.; Van der Werf, T.S.; Friedrich, A.W.; Rossen, J.W.; Van Dijl, J.M.; et al. Epidemiology of Staphylococcus aureus in a burn unit of a tertiary care center in Ghana. PLoS ONE 2017, 12, e0181072. [Google Scholar] [CrossRef]
- Reygaert, W.C. Antimicrobial resistance mechanisms of Staphylococcus aureus. In Microbial Pathogens and Strategies for Combating Them: Science, Technology and Education, 1st ed.; Formatex Research Center: Badajoz, Spain, 2013; pp. 297–310. [Google Scholar]
- Mottola, C.; Semedo-Lemsaddek, T.; Mendes, J.J.; Melo-Cristino, J.; Tavares, L.; Cavaco-Silva, P.; Oliveira, M. Molecular typing, virulence traits and antimicrobial resistance of diabetic foot staphylococci. J. Biomed. Sci. 2016, 23, 33. [Google Scholar] [CrossRef] [PubMed]
- Jarraud, S.; Mougel, C.; Thioulouse, J.; Lina, G.; Meugnier, H.; Forey, F.; Nesme, X.; Etienne, J.; Vandenesch, F. Relationships between Staphylococcus aureus genetic background, virulence factors, agr groups (alleles), and human disease. Infect. Immun. 2002, 70, 631–641. [Google Scholar] [CrossRef]
- CLSI. Performance Standards for Antimicrobial Susceptibility Testing, 28th ed.; CLSI supplement M100; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2018. [Google Scholar]
- Dashti, A.A.; Jadaon, M.M.; Abdulsamad, A.M.; Dashti, H.M. Heat treatment of bacteria: A simple method of DNA extraction for molecular techniques. Kuwait Med. J. 2009, 41, 117–122. [Google Scholar]
- Larsen, A.R.; Stegger, M.; Sørum, M. Spa typing directly from a mecA, spa and pvl multiplex PCR assay—a cost-effective improvement for methicillin-resistant Staphylococcus aureus surveillance. Clin. Microbiol. Infect. 2008, 14, 611–614. [Google Scholar] [CrossRef] [PubMed]
- Darling, A.C.; Mau, B.; Blattner, F.R.; Perna, N.T. Mauve: Multiple alignment of conserved genomic sequence with rearrangements. Genome Res. 2004, 14, 1394–1403. [Google Scholar] [CrossRef]
- Lanave, C.; Preparata, G.; Sacone, C.; Serio, G. A new method for calculating evolutionary substitution rates. J. Mol. Evol. 1984, 20, 86–93. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | 37 Military Hospital N = 56 n%) | Korle Bu Teaching Hospital N = 56 n(%) | Total N = 112 n(%) |
|---|---|---|---|
| Gender | |||
| Male | 28(50.0) | 6(10.7) | 34(30.4) |
| Female | 28(50.0) | 50(89.3) | 78(69.6) |
| Age | |||
| ≤13 years | 1(1.8) | 6(10.7) | 7(6.3) |
| >13 years | 55(98.2) | 50(89.3) | 105(93.8) |
| Department/ward | |||
| General surgery | 20(35.7) | − | |
| Trauma and Surgical emergency unit | 10(17.9) | − | |
| Surgical OPD | 16(28.6) | − | |
| Obstetrics and Gynecology | 10(17.9) | 5(8.9) | |
| Maternity | − | 38(67.9) | |
| Neurosurgery | − | 2(3.6) | |
| Pediatric Unit | − | 6(10.7) | |
| Surgical Unit | − | 3(5.4) | |
| Orthopedic ward | − | 2(3.6) | |
| S. aureus positivity | 8(14.3) | 5(8.9) | 13(11.6) |
| Hospital | Ward | Age | Gender | Operation Type | Antibiotic After Operation | POH | MRSA/MSSA | Antibiotic Resistance | Spa type/ST | SCCmec Type | Resistant Genes | Virulence Genes |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 37-MH | TSE | 25 | Male | Incision and drainage | Amoxicillin clavulanic acid | 6days | MRSA | cef+ tet | t355(ST152) | IVa (2B) | blaZ, tet(K), cat(pC221), mecA | hlgA, hlgB, lukS-PV, lukF-PV |
| 37-MH | GS | 57 | Female | Debridement of right foot | Ciprofloxacin | 9days | MRSA | cef+ cli+ ery | t355(ST152) | IVa (2B) | blaZ, erm(C), mecA | hlgA, hlgB, lukS-PV, lukF-PV, scn |
| 37-MH | GS | 57 | Male | Incision and drainage of Pus | Clindamycin | 12days | MRSA | cef+ery | t355(ST152) | IVa (2B) | cat(pC221), mecA | hlgA, hlgB, lukS-PV, lukF-PV, scn |
| 37-MH | SOPD | 48 | Male | Herniotomy | Ciprofloxacin | 7days | MRSA | cef+tet+cli+ery | t002(ST5) | Vc | blaZ, tet(K), Inu(A), mecA | hlgA, hlgB, hlgC, lukD, sei, sem, sen, seo, sep, scn, sak, aur, splA, splB |
| 37-MH | GS | 49 | Female | Incision and Drainage | Amoxicillin clavulanic acid, Cefuroxime | 6days | MSSA | − | t442(ST5) | N/A | blaZ | hlgA, hlgB, hlgC, lukD, lukE, lukS-PV, lukF-PV sea, seb, sei, sem, sen, seo, scn, sak, aur, splA |
| 37-MH | SOPD | 41 | Female | Open reduction internal fixation | Metronidazole | 30days | MSSA | tet+cli | t127(ST1) | N/A | blaZ, tet(K) | hlgA, hlgB, hlgC, lukE, sea, sek, tst, scn, sak, aur, splA, splB |
| 37-MH | SOPD | 51 | Male | Hernia Repair | No medication | 5days | MSSA | tet+sxt+ery | t084(ST3249) | N/A | blaZ, tet(K), dfrG | hlgA, hlgB, lukS-PV, lukF-PV, scn |
| 37-MH | GS | 68 | Male | Appendectomy | No medication | 1day | MSSA | ery | t3194(ST30) | N/A | blaZ, dfrG | hlgA, hlgB, hlgC, sei, seu, scn, aur, splE |
| KBTH | MT | 30 | Female | Emergency Caesarean section | Amoxicillin clavulanic acid, Metronidazole | 1day | MSSA | tet+ery | t355(ST152) | N/A | blaZ, tet(K), Inu(A), aadD | hlgA, hlgB, lukS-PV, lukF-PV, scn |
| KBTH | MT | 32 | Female | Elective Caesarean section | Gentamicin, Clindamycin | 13 days | MSSA | tet | t355(ST152) | N/A | blaZ, tet(K) | hlgA, hlgB, scn |
| KBTH | MT | 36 | Female | Caesarean section | Amoxicillin clavulanic acid, Metronidazole | 4days | MSSA | − | Unknown spa type (ST3249) | N/A | blaZ | hlgB, lukS-PV, lukF-PV, scn |
| KBTH | MT | 34 | Female | Caesarean section | Clindamycin | 1days | MSSA | − | t4019(ST152) | N/A | blaZ | hlgA, hlgB, lukS-PV, lukF-PV, scn |
| KBTH | GS | 15 | Female | 2nd Stage Debulking | Cefuroxime | 13days | MSSA | − | t002(ST5) | N/A | blaZ | hlgA, hlgB, hlgC, lukD, sei, sem, sen, seo, sep, scn, sak, aur, splA, splB |
| Isolate ID | No. of Reads | G+C Content (%) | Mean Coverage (X) | No. of Predicted Coding Sequences | No. of Predicted RNAs | GenBank Accession No. |
|---|---|---|---|---|---|---|
| GHA1 | 2,512,041 | 32.8 | 441 | 2699 | 82 | CP043923.1 |
| GHA2 | 2,096,320 | 32.9 | 379 | 2683 | 82 | CP043922.1 |
| GHA3 | 1,159,656 | 32.8 | 208 | 2675 | 81 | CP043921.1 |
| GHA4 | 133,790 | 32.9 | 24 | 2694 | 69 | CP043920.1 |
| GHA5 | 95,977 | 33.0 | 17 | 2612 | 77 | CP043919.1 |
| GHA6 | 3,080,479 | 32.8 | 554 | 2649 | 81 | CP043918.1 |
| GHA7 | 2,947,151 | 32.6 | 551 | 2564 | 56 | CP043917.1 |
| GHA8 | 3,412,807 | 32.8 | 612 | 2716 | 64 | CP043916.1 |
| GHA9 | 397,799 | 32.7 | 74 | 2632 | 58 | CP043915.1 |
| GHA10 | 1,274,423 | 32.9 | 233 | 2651 | 82 | CP043914.1 |
| GHA11 | 982,047 | 32.9 | 175 | 2653 | 80 | CP043913.1 |
| GHA12 | 891,432 | 32.9 | 166 | 2534 | 82 | CP043912.1 |
| GHA13 | 1,882,838 | 32.7 | 352 | 2628 | 57 | CP043911.1 |
| Primer | Primer Sequences | Description | References |
|---|---|---|---|
| spa | F: 5′-TAAAGACGATCCTTCGGTGAGC-3′R: 5′-CAGCAGTAGTGCCGTTTGCTT-3′ | To detect the spa gene (S. aureus specific) | [45] |
| pvl | F: 5′-GCTGGACAAAACTTCTTGGAATAT-3′R: 5′-GATAGGACACCAATAAATTCTGGATTG-3′ | To detect Panton-Valentine leukocidin (virulence factor) | [45] |
| mecA | F: 5′-TCCAGATTACA ACTTCACCAGG-3′R: 5′-CCACTTCATATCTTGTAACG-3′ | To detect methicillin resistance due to the mecA gene | [45] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Egyir, B.; Bentum, J.; Attram, N.; Fox, A.; Obeng-Nkrumah, N.; Appiah-Korang, L.; Behene, E.; Kumordjie, S.; Yeboah, C.; Agbodzi, B.; et al. Whole Genome Sequencing and Antimicrobial Resistance of Staphylococcus aureus from Surgical Site Infections in Ghana. Pathogens 2021, 10, 196. https://doi.org/10.3390/pathogens10020196
Egyir B, Bentum J, Attram N, Fox A, Obeng-Nkrumah N, Appiah-Korang L, Behene E, Kumordjie S, Yeboah C, Agbodzi B, et al. Whole Genome Sequencing and Antimicrobial Resistance of Staphylococcus aureus from Surgical Site Infections in Ghana. Pathogens. 2021; 10(2):196. https://doi.org/10.3390/pathogens10020196
Chicago/Turabian StyleEgyir, Beverly, Jeannette Bentum, Naiki Attram, Anne Fox, Noah Obeng-Nkrumah, Labi Appiah-Korang, Eric Behene, Selassie Kumordjie, Clara Yeboah, Bright Agbodzi, and et al. 2021. "Whole Genome Sequencing and Antimicrobial Resistance of Staphylococcus aureus from Surgical Site Infections in Ghana" Pathogens 10, no. 2: 196. https://doi.org/10.3390/pathogens10020196
APA StyleEgyir, B., Bentum, J., Attram, N., Fox, A., Obeng-Nkrumah, N., Appiah-Korang, L., Behene, E., Kumordjie, S., Yeboah, C., Agbodzi, B., Bentil, R. E., Tagoe, R., Kofi Adu Tabi, B., Owusu, F., Dayie, N. T. K. D., Donkor, E. S., Nsaful, J., Asah-Opoku, K., Nyarko, E., ... Letizia, A. G. (2021). Whole Genome Sequencing and Antimicrobial Resistance of Staphylococcus aureus from Surgical Site Infections in Ghana. Pathogens, 10(2), 196. https://doi.org/10.3390/pathogens10020196