
Assessment of Ceragenins in Prevention of Damage to Voice Prostheses Caused by Candida Biofilm Formation

 , ,
, ,  , ,
, ,  , ,
, ,
Abstract
1. Introduction
2. Results
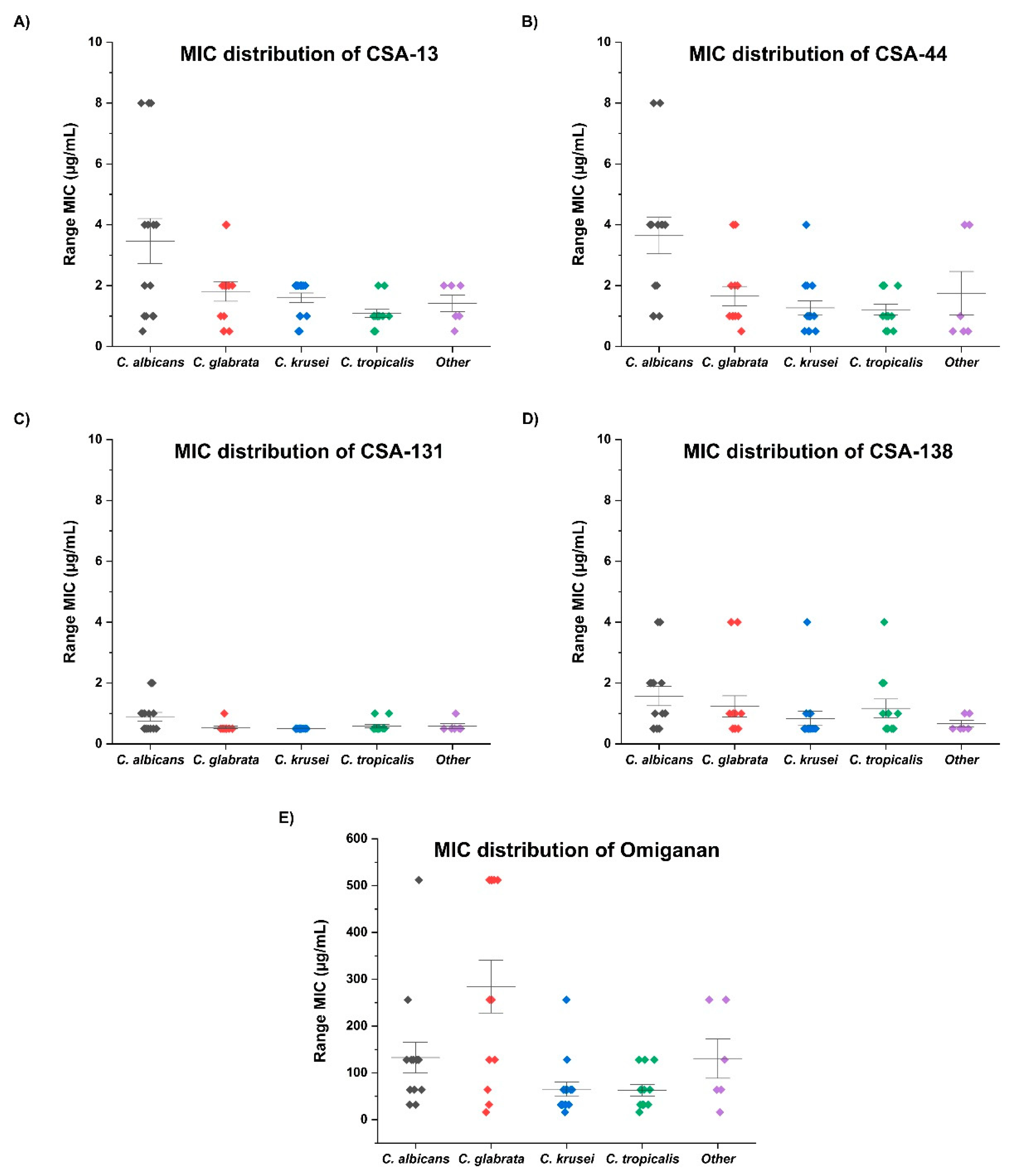
2.1. Ceragenin CSA-131 Displays the Strongest Candidacidal Activity against Tested Candida Strains from Group of Tested Antimicrobial Agents
2.2. Prolongated Incubation of Candida with Ceragenins Did Not Result in Development of Candida Resistance
2.3. The Impregnation of VP in an Ethanolic Solution of Ceragenin Prevents the Development of Candida Biofilm on Their Surface
3. Discussion
4. Materials and Methods
4.1. Collection of Candida Strains
4.2. Antifungals, Ceragenins, and Determination of MIC, MFC, and MBIC
4.3. Subsequential Passages of Selected Candida Strains and the Assessment of Their Susceptibility to Ceragenin
4.4. Voice Prosthesis Incubation in Organic Solution of Ceragenin
4.5. Evaluation of Biofilm Mass
4.6. CSA-131 Quantitation
4.7. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Souza, F.G.R.; Santos, I.C.; Bergmann, A.; Thuler, L.C.S.; Freitas, A.S.; Freitas, E.Q.; Dias, F.L. Quality of life after total laryngectomy: Impact of different vocal rehabilitation methods in a middle income country. Health Qual. Life Outcomes 2020, 18, 1–12. [Google Scholar] [CrossRef]
- Rodrigues, M.E.; Gomes, F.; Rodrigues, C.F. Candida spp./Bacteria Mixed Biofilms. J. Fungi 2019, 6, 5. [Google Scholar] [CrossRef]
- Singer, M.I.B.; Blom, E.D. An endoscopic technique for restoration of voice after laryngectomy. Ann. Otol. Rhinol. Laryngol. 1980, 89, 529–533. [Google Scholar] [CrossRef]
- Douglas, L.J. Candida biofilms and their role in infection. Trends Microbiol. 2003, 11, 30–36. [Google Scholar] [CrossRef]
- Erna, M.; Kojic, R.O.D. Candida Infections of Medical Devices. Clin. Microbiol. Rev. 2004, 17, 255–267. [Google Scholar]
- Galli, J.; Calo, L.; Meucci, D.; Giuliani, M.; Lucidi, D.; Paludetti, G.; Torelli, R.; Sanguinetti, M.; Parrilla, C. Biofilm in voice prosthesis: A prospective cohort study and laboratory tests using sonication and SEM analysis. Clin. Otolaryngol. 2018, 43, 1260–1265. [Google Scholar] [CrossRef]
- Spalek, J.; Deptula, P.; Ciesluk, M.; Strzelecka, A.; Lysik, D.; Mystkowska, J.; Daniluk, T.; Krol, G.; Gozdz, S.; Bucki, R.; et al. Biofilm Growth Causes Damage to Silicone Voice Prostheses in Patients after Surgical Treatment of Locally Advanced Laryngeal Cancer. Pathogens 2020, 9, 793. [Google Scholar] [CrossRef]
- Talpaert, M.J.; Balfour, A.; Stevens, S.; Baker, M.; Muhlschlegel, F.A.; Gourlay, C.W. Candida biofilm formation on voice prostheses. J. Med. Microbiol. 2015, 28, 199–208. [Google Scholar] [CrossRef] [PubMed]
- Laccourreye, O.; Ménard, M.; Crevier-Buchman, L.; Couloigner, V.; Brasnu, D. In Situ Lifetime, Causes for Replacement, and Complications of the ProvoxTM Voice Prosthesis. Laryngoscope 1997, 107, 527–530. [Google Scholar] [CrossRef] [PubMed]
- Kress, P.; Schafer, P.; Schwerdtfeger, F.P.; Rosler, S. Are modern voice prostheses better? A lifetime comparison of 749 voice prostheses. Eur. Arch. Otorhinolaryngol. 2014, 271, 133–140. [Google Scholar] [CrossRef]
- Spałek, J.; Deptuła, P.; Durnaś, B.; Król, G.; Kaliniak, S.; Bucki, R.; Okła, S. Potential colonization of provox voice prosthesis by Candida spp. with no sign of failure for approximately 10 years exploitation time. Acta Oto-Laryngol. Case Rep. 2021, 6, 60–66. [Google Scholar] [CrossRef]
- Ameye, D.; Honraet, K.; Loose, D.; Vermeersch, H.; Nelis, H.; Remon, J.P. Effect of a buccal bioadhesive nystatin tablet on the lifetime of a Provox silicone tracheoesophageal voice prosthesis. Acta Otolaryngol. 2005, 125, 304–306. [Google Scholar] [CrossRef] [PubMed]
- Messing, B.P.; Kim, M.; Hirata, R.; Thompson, C.B.; Gebhart, S.; Sugar, E.A.; Saunders, J.M.; Sciubba, J.; Califano, J.A. Evaluation of prophylaxis treatment of Candida in alaryngeal patients with tracheoesophageal voice prostheses. Laryngoscope 2015, 125, 1118–1123. [Google Scholar] [CrossRef] [PubMed]
- Chin, J.N.; Jones, R.N.; Sader, H.S.; Savage, P.B.; Rybak, M.J. Potential synergy activity of the novel ceragenin, CSA-13, against clinical isolates of Pseudomonas aeruginosa, including multidrug-resistant P. aeruginosa. J. Antimicrob. Chemother. 2008, 61, 365–370. [Google Scholar] [CrossRef]
- Chin, J.N.; Rybak, M.J.; Cheung, C.M.; Savage, P.B. Antimicrobial activities of ceragenins against clinical isolates of resistant Staphylococcus aureus. Antimicrob. Agents Chemother. 2007, 51, 1268–1273. [Google Scholar] [CrossRef]
- Leszczyńska, K.; Namiot, D.; Byfield, F.J.; Cruz, K.; Żendzian-Piotrowska, M.; Fein, D.E.; Savage, P.B.; Diamond, S.; McCulloch, C.A.; Janmey, P.A.; et al. Antibacterial activity of the human host defence peptide LL-37 and selected synthetic cationic lipids against bacteria associated with oral and upper respiratory tract infections. J. Antimicrob. Chemother. 2012, 68, 610–618. [Google Scholar] [CrossRef]
- Lara, D.; Feng, Y.; Bader, J.; Savage, P.B.; Maldonado, R.A. Anti-trypanosomatid activity of ceragenins. J. Parasitol. 2010, 96, 638–642. [Google Scholar] [CrossRef]
- Howell, M.D.; Streib, J.E.; Kim, B.E.; Lesley, L.J.; Dunlap, A.P.; Geng, D.; Feng, Y.; Savage, P.B.; Leung, D.Y. Ceragenins: A class of antiviral compounds to treat orthopox infections. J. Investig. Dermatol. 2009, 129, 2668–2675. [Google Scholar] [CrossRef]
- Durnas, B.; Wnorowska, U.; Pogoda, K.; Deptula, P.; Watek, M.; Piktel, E.; Gluszek, S.; Gu, X.; Savage, P.B.; Niemirowicz, K.; et al. Candidacidal Activity of Selected Ceragenins and Human Cathelicidin LL-37 in Experimental Settings Mimicking Infection Sites. PLoS ONE 2016, 11, e0157242. [Google Scholar] [CrossRef]
- Durnas, B.; Piktel, E.; Watek, M.; Wollny, T.; Gozdz, S.; Smok-Kalwat, J.; Niemirowicz, K.; Savage, P.B.; Bucki, R. Anaerobic bacteria growth in the presence of cathelicidin LL-37 and selected ceragenins delivered as magnetic nanoparticles cargo. BMC Microbiol. 2017, 17, 167. [Google Scholar] [CrossRef]
- Wnorowska, U.; Fiedoruk, K.; Piktel, E.; Prasad, S.V.; Sulik, M.; Janion, M.; Daniluk, T.; Savage, P.B.; Bucki, R. Nanoantibiotics containing membrane-active human cathelicidin LL-37 or synthetic ceragenins attached to the surface of magnetic nanoparticles as novel and innovative therapeutic tools: Current status and potential future applications. J. Nanobiotech. 2020, 18, 3. [Google Scholar] [CrossRef] [PubMed]
- Hacioglu, M.; Haciosmanoglu, E.; Birteksoz-Tan, A.S.; Bozkurt-Guzel, C.; Savage, P.B. Effects of ceragenins and conventional antimicrobials on Candida albicans and Staphylococcus aureus mono and multispecies biofilms. Diagn. Microbiol. Infect. Dis. 2019, 95, 114863. [Google Scholar] [CrossRef] [PubMed]
- Bozkurt-Guzel, C.; Hacioglu, M.; Savage, P.B. Investigation of the in vitro antifungal and antibiofilm activities of ceragenins CSA-8, CSA-13, CSA-44, CSA-131, and CSA-138 against Candida species. Diagn. Microbiol. Infect. Dis. 2018, 91, 324–330. [Google Scholar] [CrossRef] [PubMed]
- Van Weissenbruch, R.; Albers, L.W.J.; Bouckaert, S.; Nelis, H.J.; Criel, G.; Remon, J.P.; Sulter, A.M. Deterioration of the Provox™ silicone tracheoesophageal voice prosthesis: Microbial aspects and structural changes. Acta Oto-Laryngol. 1997, 117, 452–458. [Google Scholar] [CrossRef]
- Percival, S.L.; Suleman, L.; Vuotto, C.; Donelli, G. Healthcare-associated infections, medical devices and biofilms: Risk, tolerance and control. J. Med. Microbiol. 2015, 64, 323–334. [Google Scholar] [CrossRef] [PubMed]
- Leonhard, M.; Schneider-Stickler, B. Voice prostheses, microbial colonization and biofilm formation. Adv. Exp. Med. Biol. 2015, 830, 123–136. [Google Scholar] [CrossRef]
- Rodrigues, L.; Banat, I.M.; Teixeira, J.; Oliveira, R. Strategies for the prevention of microbial biofilm formation on silicone rubber voice prostheses. J. Biomed. Mater. Res. 2007, 81, 358–370. [Google Scholar] [CrossRef] [PubMed]
- Bourdillon, A.T.; Edwards, H.A. Review of probiotic use in otolaryngology. Am. J. Otolaryngol. 2021, 42, 102883. [Google Scholar] [CrossRef]
- Buijssen, K.; Oosterhof, J.J.H.; Basil, L.; Waters, M.; Duits, M.A.; Busscher, H.J.; van der Mei, H.C.; van der Laan, B. Influence of surface roughness on silicone rubber voice prostheses on in vitro biofilm formation and clinical lifetime in laryngectomised patients. Clin. Otolaryngol. 2017, 42, 1235–1240. [Google Scholar] [CrossRef] [PubMed]
- De Prijck, K.; De Smet, N.; Coenye, T.; Schacht, E.; Nelis, H.J. Prevention of Candida albicans biofilm formation by covalently bound dimethylaminoethylmethacrylate and polyethylenimine. Mycopathologia 2010, 170, 213–221. [Google Scholar] [CrossRef]
- Contreras-García, A.; Bucio, E.; Brackman, G.; Coenye, T.; Concheiro, A.; Alvarez-Lorenzo, C. Biofilm inhibition and drug-eluting properties of novel DMAEMA-modified polyethylene and silicone rubber surfaces. Biofouling 2011, 27, 123–135. [Google Scholar] [CrossRef]
- Mendes, R.M.; Francisco, A.P.; Carvalho, F.A.; Dardouri, M.; Costa, B.; Bettencourt, A.F.; Costa, J.; Gonçalves, L.; Costa, F.; Ribeiro, I.A.C. Fighting S. aureus catheter-related infections with sophorolipids: Electing an antiadhesive strategy or a release one? Colloids Surf. B Biointerfaces 2021, 208, 112057. [Google Scholar] [CrossRef] [PubMed]
- Ceresa, C.; Fracchia, L.; Williams, M.; Banat, I.M.; Díaz De Rienzo, M.A. The effect of sophorolipids against microbial biofilms on medical-grade silicone. J. Biotechnol. 2020, 309, 34–43. [Google Scholar] [CrossRef] [PubMed]
- Tsikopoulos, A.; Petinaki, E.; Festas, C.; Tsikopoulos, K.; Meroni, G.; Drago, L.; Skoulakis, C. In vitro Inhibition of Biofilm Formation on Silicon Rubber Voice Prosthesis: A Systematic Review and Meta-Analysis. ORL J. Otorhinolaryngol. Relat. Spec. 2021, 28, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Gu, X.; Jennings, J.D.; Snarr, J.; Chaudhary, V.; Pollard, J.E.; Savage, P.B. Optimization of ceragenins for prevention of bacterial colonization of hydrogel contact lenses. Investig. Ophthalmol. Vis. Sci. 2013, 54, 6217–6223. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Hashemi, M.M.; Rovig, J.; Bateman, J.; Holden, B.S.; Modelzelewski, T.; Gueorguieva, I.; von Dyck, M.; Bracken, R.; Genberg, C.; Deng, S.; et al. Preclinical testing of a broad-spectrum antimicrobial endotracheal tube coated with an innate immune synthetic mimic. J. Antimicrob. Chemother. 2018, 73, 143–150. [Google Scholar] [CrossRef]
- Dao, A.; Mills, R.J.; Kamble, S.; Savage, P.B.; Little, D.G.; Schindeler, A. The application of ceragenins to orthopedic surgery and medicine. J. Orthop. Res. 2020, 38, 1883–1894. [Google Scholar] [CrossRef]
- Mills, R.J.; Boyling, A.; Cheng, T.L.; Peacock, L.; Savage, P.B.; Tägil, M.; Little, D.G.; Schindeler, A. CSA-90 reduces periprosthetic joint infection in a novel rat model challenged with local and systemic Staphylococcus aureus. J. Orthop. Res. 2020, 38, 2065–2073. [Google Scholar] [CrossRef]
- Bozec, A.; Culié, D.; Poissonnet, G.; Dassonville, O. Current Role of Total Laryngectomy in the Era of Organ Preservation. Cancers 2020, 12, 584. [Google Scholar] [CrossRef]
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Mathers, C.; Parkin, D.M.; Piñeros, M.; Znaor, A.; Bray, F. Estimating the global cancer incidence and mortality in 2018: GLOBOCAN sources and methods. Int. J. Cancer 2019, 144, 1941–1953. [Google Scholar] [CrossRef]
- Groome, P.A.; O’Sullivan, B.; Irish, J.C.; Rothwell, D.M.; Schulze, K.; Warde, P.R.; Schneider, K.M.; Mackenzie, R.G.; Hodson, D.I.; Hammond, J.A.; et al. Management and outcome differences in supraglottic cancer between Ontario, Canada, and the Surveillance, Epidemiology, and End Results areas of the United States. J. Clin. Oncol. 2003, 21, 496–505. [Google Scholar] [CrossRef] [PubMed]
- Ding, B.; Taotofa, U.; Orsak, T.; Chadwell, M.; Savage, P.B. Synthesis and Characterization of Peptide−Cationic Steroid Antibiotic Conjugates. Org. Lett. 2004, 6, 3433–3436. [Google Scholar] [CrossRef] [PubMed]
- CLSI. Reference Method for Broth Dilution Antifungal Susceptibility Testing of Yeasts: Approved Standard, 3rd ed.; CLSI Document M27-A3; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2008. [Google Scholar]
- Meletiadis, J.; Mouton, J.W.; Meis, J.F.; Bouman, B.A.; Donnelly, P.J.; Verweij, P.E. Comparison of spectrophotometric and visual readings of NCCLS method and evaluation of a colorimetric method based on reduction of a soluble tetrazolium salt, 2,3-bis [2-methoxy-4-nitro-5-[(sulfenylamino) carbonyl]-2H-tetrazolium-hydroxide], for antifungal susceptibility testing of Aspergillus species. J. Clin. Microbiol. 2001, 39, 4256–4263. [Google Scholar] [CrossRef] [PubMed]
- Pollard, J.E.; Snarr, J.; Chaudhary, V.; Jennings, J.D.; Shaw, H.; Christiansen, B.; Wright, J.; Jia, W.; Bishop, R.E.; Savage, P.B. In vitro evaluation of the potential for resistance development to ceragenin CSA-13. J. Antimicrob. Chemother. 2012, 67, 2665–2672. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Agent | MIC (µg/mL) | MFC (µg/mL) | MBIC (µg/mL) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Range | 50% | 90% | Range | 50% | 90% | Range | 50% | 90% | |
| Candida albicans (n = 14) | |||||||||
| Amphotericin B | 0.5–512 | 0.5 | 1 | 0.5–512 | 0.5 | 1 | 0.5–512 | 1 | 32 |
| Fluconazole | 0.5–512 | 16 | 512 | 1–512 | 128 | 512 | 2–512 | 128 | 512 |
| Omiganan | 32–512 | 128 | 256 | 64–512 | 128 | 256 | 64–512 | 128 | 256 |
| LL-37 | 16–512 | 512 | 512 | 64–512 | 512 | 512 | 64–512 | 512 | 512 |
| CSA-13 | 0.5–8 | 2 | 8 | 1–8 | 4 | 8 | 2–16 | 4 | 8 |
| CSA-131 | 0.5–2 | 0.5 | 2 | 0.5–2 | 0.5 | 2 | 0.5–2 | 1 | 2 |
| CSA-44 | 1–8 | 4 | 8 | 1–8 | 4 | 8 | 1–8 | 4 | 8 |
| CSA-138 | 0.5–4 | 1 | 4 | 0.5–4 | 1 | 4 | 0.5–8 | 1 | 4 |
| Candida krusei (n = 15) * | |||||||||
| Amphotericin B | 0.5–128 | 1 | 4 | 0.5–256 | 2 | 8 | 0.5–256 | 2 | 4 |
| Omiganan | 16–256 | 64 | 128 | 32–512 | 64 | 128 | 32–256 | 128 | 256 |
| LL-37 | 16–512 | 512 | 512 | 16–512 | 512 | 512 | 16–512 | 512 | 512 |
| CSA-13 | 0.5–2 | 2 | 2 | 0.5–2 | 2 | 2 | 0.5–8 | 2 | 4 |
| CSA-131 | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 | 0.5–1 | 0.5 | 1 |
| CSA-44 | 0.5–4 | 1 | 2 | 0.5–4 | 1 | 2 | 0.5–4 | 1 | 4 |
| CSA-138 | 0.5–4 | 0.5 | 1 | 0.5–4 | 0.5 | 2 | 0.5–4 | 1 | 2 |
| Candida tropicalis (n = 12) | |||||||||
| Amphotericin B | 0.5–8 | 1 | 4 | 0.5–16 | 2 | 8 | 0.5–16 | 2 | 4 |
| Fluconazole | 1–512 | 2 | 32 | 2–512 | 4 | 128 | 2–512 | 4 | 128 |
| Omiganan | 16–128 | 32 | 128 | 16–256 | 64 | 128 | 32–256 | 64 | 128 |
| LL-37 | 128–512 | 512 | 512 | 128–512 | 512 | 512 | 512 | 512 | 512 |
| CSA-13 | 0.5–2 | 1 | 2 | 0.5–4 | 1 | 4 | 0.5–4 | 1 | 4 |
| CSA-131 | 0.5–1 | 0.5 | 1 | 0.5–1 | 0.5 | 1 | 0.5–2 | 0.5 | 1 |
| CSA-44 | 0.5–2 | 1 | 2 | 0.5–4 | 1 | 2 | 1–2 | 1 | 2 |
| CSA-138 | 0.5–4 | 0.5 | 2 | 0.5–4 | 1 | 2 | 0.5–4 | 1 | 2 |
| Candida glabrata (n = 13) | |||||||||
| Amphotericin B | 0.5–16 | 1 | 4 | 0.5–16 | 2 | 4 | 0.5–128 | 2 | 16 |
| Fluconazole | 2–512 | 128 | 512 | 4–512 | 256 | 512 | 4–512 | 512 | 512 |
| Omiganan | 16–512 | 256 | 512 | 32–512 | 256 | 512 | 64–512 | 256 | 512 |
| LL-37 | 16–512 | 512 | 512 | 64–512 | 512 | 512 | 64–512 | 512 | 512 |
| CSA-13 | 0.5–4 | 2 | 4 | 0.5–4 | 2 | 4 | 0.5–8 | 2 | 4 |
| CSA-131 | 0.5–1 | 0.5 | 0.5 | 0.5–1 | 0.5 | 0.5 | 0.5–4 | 1 | 2 |
| CSA-44 | 0.5–4 | 1 | 4 | 0.5–4 | 2 | 4 | 1–8 | 2 | 4 |
| CSA-138 | 0.5–4 | 1 | 4 | 0.5–4 | 1 | 4 | 0.5–4 | 1 | 4 |
| Compound | Amphotericin B | Fluconazole | Omiganan | LL-37 | CSA-13 | CSA-131 | CSA-44 | CSA-138 | |
|---|---|---|---|---|---|---|---|---|---|
| Strain | MIC/MFC/MBI | ||||||||
| C. albicans 185 | 256/256/256 | 256/>256/>256 | 128/128/128 | >256/>256/>256 | 1/1/4 | 2/2/2 | 4/4/4 | 2/2/2 | |
| C. albicans 177 | 0.5/0.5/1 | >256/>256/>256 | 64/128/128 | >256/>256/>256 | 2/2/2 | 0.5/0.5/.5 | 1/1/1 | 0.5/0.5/.5 | |
| C. albicans 189 | 0.5/0.5/0.5 | >256/>256/>256 | 128/128/128 | >256/>256/>256 | 1/2/2 | 0.5/0.5/.5 | 2/2/4 | 1/1/1 | |
| C. albicans 138 | >256/>256/>256 | >256/>256/>256 | >256/>256/>256 | >256/>256/>256 | 4/4/4 | 1/1/1 | 4/4/4 | 1/1/1 | |
| C. albicans 160 | 1/2/2 | 128/>256/>256 | 32/64/128 | >256/>256/>256 | 2/2/8 | 0.5/0.5/1 | 1/2/2 | 0.5/0.5/1 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Spałek, J.; Daniluk, T.; Godlewski, A.; Deptuła, P.; Wnorowska, U.; Ziembicka, D.; Cieśluk, M.; Fiedoruk, K.; Ciborowski, M.; Krętowski, A.; et al. Assessment of Ceragenins in Prevention of Damage to Voice Prostheses Caused by Candida Biofilm Formation. Pathogens 2021, 10, 1371. https://doi.org/10.3390/pathogens10111371
Spałek J, Daniluk T, Godlewski A, Deptuła P, Wnorowska U, Ziembicka D, Cieśluk M, Fiedoruk K, Ciborowski M, Krętowski A, et al. Assessment of Ceragenins in Prevention of Damage to Voice Prostheses Caused by Candida Biofilm Formation. Pathogens. 2021; 10(11):1371. https://doi.org/10.3390/pathogens10111371
Chicago/Turabian StyleSpałek, Jakub, Tamara Daniluk, Adrian Godlewski, Piotr Deptuła, Urszula Wnorowska, Dominika Ziembicka, Mateusz Cieśluk, Krzysztof Fiedoruk, Michał Ciborowski, Adam Krętowski, and et al. 2021. "Assessment of Ceragenins in Prevention of Damage to Voice Prostheses Caused by Candida Biofilm Formation" Pathogens 10, no. 11: 1371. https://doi.org/10.3390/pathogens10111371
APA StyleSpałek, J., Daniluk, T., Godlewski, A., Deptuła, P., Wnorowska, U., Ziembicka, D., Cieśluk, M., Fiedoruk, K., Ciborowski, M., Krętowski, A., Góźdź, S., Durnaś, B., Savage, P. B., Okła, S., & Bucki, R. (2021). Assessment of Ceragenins in Prevention of Damage to Voice Prostheses Caused by Candida Biofilm Formation. Pathogens, 10(11), 1371. https://doi.org/10.3390/pathogens10111371