Identifying Autism through Empathizing and Systemizing Abilities

Abstract
1. Introduction
1.1. The Empathizing-Systemizing Model
1.2. The Empathizing-Systemizing Instruments
1.3. Identifying Autism in Children
2. Method
2.1. Participants
2.2. Instruments
2.3. Procedure
2.4. Statistical Analysis
3. Results
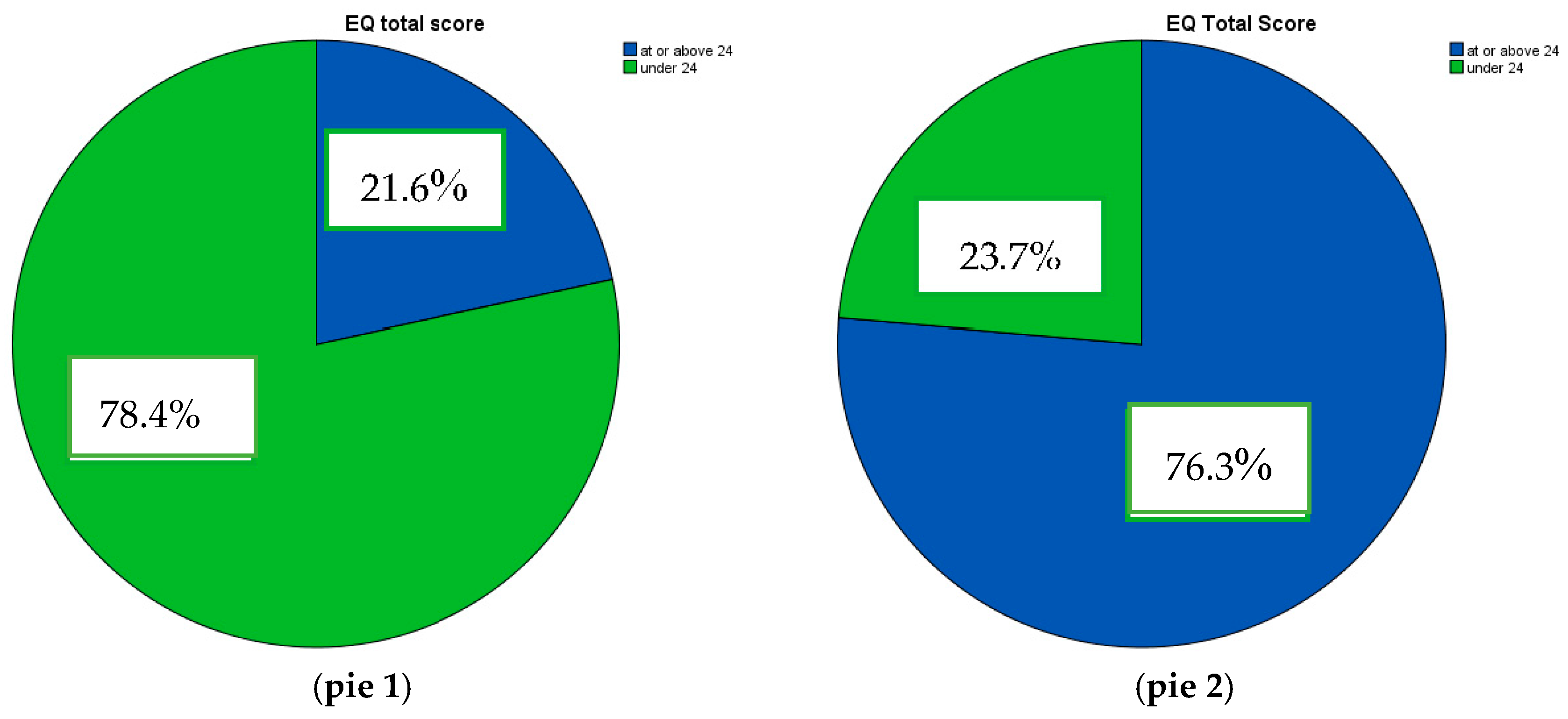
3.1. Psychometric Features and Cut-off Scores of the AQ Child_NL and EQ-SQ Child_NL
3.2. Can Gender Differences be Identified?
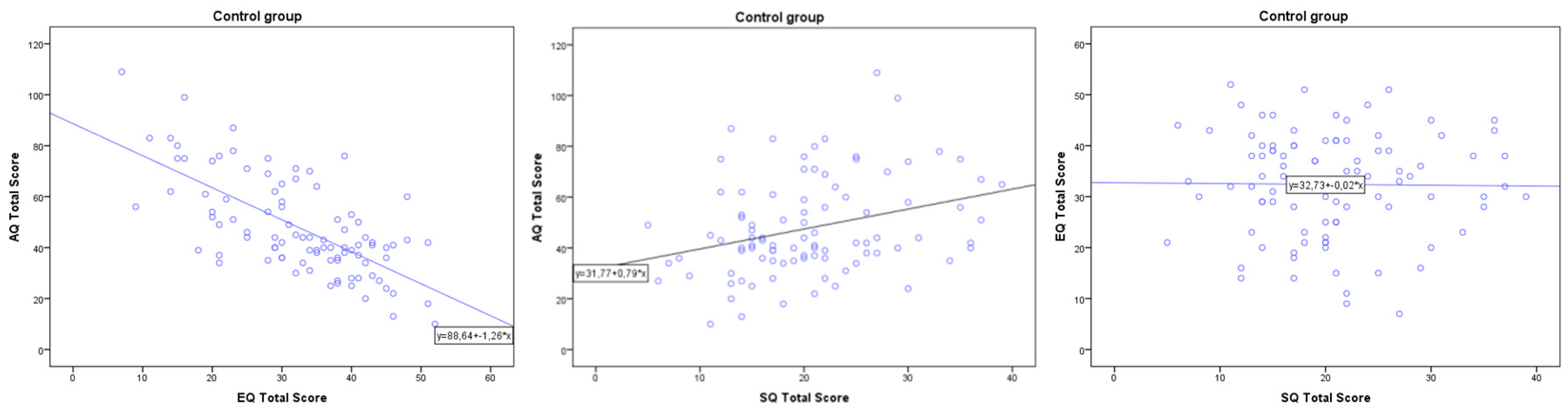
3.3. Can One’s Empathizing and Systemizing Skills Predict One’s AQ Child_NL Score?
3.4. Can Gender and Diagnosis Predict One’s AQ, EQ or SQ Child_NL Score?
4. Discussion
The Discrepancy between an Individual’s Empathizing and Systemizing Abilities are Responsible for Higher Scores on the AQ Child_NL.
5. Conclusions
Limitations and Future Research
Acknowledgments
Author Contributions
Conflicts of Interest
References
- American Psychiatric Association. 1994. DSM-IV Diagnostic and Statistical Manual of Mental Disorders, 4th ed. Arlington: Author. [Google Scholar]
- American Psychiatric Association. 2013. DSM 5 Diagnostic and Statistical Manual of Mental Disorders, 5th ed. Arlington: Author. [Google Scholar]
- Auyeung, Bonnie, Simon Baron-Cohen, Sally Wheelwright, and Carrie Allison. 2007. The Autism Spectrum Quotient: Children’s Version (AQ-Child). Journal of Autism and Developmental Disorders 38: 1230–40. [Google Scholar] [CrossRef] [PubMed]
- Auyeung, Bonnie, Sally Wheelwright, Carrie Allison, Matthew Atkinson, Nelum Samarawickrema, and Simon Baron-Cohen. 2009. The children’s Empathy Quotient and Systemizing Quotient: Sex differences in typical development and in autism spectrum conditions. Journal of Autism and Developmental Disorders 39: 1509. [Google Scholar] [CrossRef] [PubMed]
- Baron-Cohen, Simon. 1995. Mindblindness: An Essay on Autism and Theory of Mind. Cambridge: MIT Press. [Google Scholar]
- Baron-Cohen, Simon. 2002. The extreme male brain theory of autism. Trends in Cognitive Sciences 6: 248–54. [Google Scholar] [CrossRef]
- Baron-Cohen, Simon, and Sally Wheelwright. 2004. The empathy quotient (EQ). An investigation of adults with asperger syndrome or High functioning autism, and normal sex differences. Journal of Autism and Developmental Disorders 34: 163–75. [Google Scholar] [CrossRef] [PubMed]
- Baron-Cohen, Simon, Alan M. Leslie, and Uta Frith. 1985. Does the autistic child have a theory of mind? Cognition 21: 37–46. [Google Scholar] [CrossRef]
- Baron-Cohen, Simon, Sally Wheelwright, Richard Skinner, Joanne Martin, and Emma Clubley. 2001. The autism spectrum quotient (AQ): Evidence from asperger syndrome/high functioning autism, males and females, scientists and mathematicians. Journal of Autism and Developmental Disorders 31: 5–17. [Google Scholar] [CrossRef] [PubMed]
- Baron-Cohen, Simon, Jennifer Richler, Dheraj Bisarya, Nhishanth Gurunathan, and Sally Wheelwright. 2003. The systemizing quotient: An investigation of adults with Asperger syndrome or high functioning autism, and normal sex differences. Philosophical Transactions of the Royal Society 358: 361–74. [Google Scholar] [CrossRef] [PubMed]
- Baron-Cohen, Simon, Rosa A. Hoekstra, Rebecca Knickmeyer, and Sally Wheelwright. 2006. The Autism-Spectrum Quotient (AQ)—Adolescent version. Journal of Autism and Developmental Disorders 36: 343–50. [Google Scholar] [CrossRef] [PubMed]
- Baron-Cohen, Simon, Sarah Cassidy, Bonnie Auyeung, Carrie Allison, Maryam Achoukhi, Sarah Robertson, Alexa Pohl, and Meng-Chuan Lai. 2014. Attenuation of typical sex differences in 800 adults with autism vs. 3900 controls. PLoS ONE 9: e102251. [Google Scholar] [CrossRef] [PubMed]
- Decety, Jean, and Meghan L. Meyer. 2008. From emotion resonance to empathic understanding: A social developmental neuroscience account. Developmental Psychopathology 20: 1053–80. [Google Scholar] [CrossRef] [PubMed]
- Ellis, Hadyn, and Hellen L. Gunter. 1999. Asperger syndrome: A simple matter of white matter? Trends in Cognitive Sciences 3: 192–200. [Google Scholar] [CrossRef]
- Gillberg, Christopher. 1992. Subgroups in autism: Are there behavioral phenotypes typical of underlying medical conditions? Journal of Intellect Disability Research 36: 201–14. [Google Scholar] [CrossRef]
- Happé, Francesca, and Uta Frith. 2006. The weak coherence account: Detail-focused cognitive style in autism spectrum disorders. Journal of Autism and Developmental Disorders 36: 5–25. [Google Scholar] [CrossRef] [PubMed]
- Hoekstra, Rosa A., Meike Bartels, Danielle C. Cath, and Dorret I. Boomsma. 2008. Factor structure of the broader autism phenotype and its diagnostic validity: A study using the Dutch translation of the autism-spectrum quotient (AQ). Journal of Autism and Developmental Disorders 38: 1555–66. [Google Scholar] [CrossRef] [PubMed]
- Klin, Ami, F. Volkmar, Sara S. Sparrow, Domenic Cicchetti, and B. P. Rourke. 1995. Validity and neuropsychological characterization of Asperger Syndrome: Convergence with nonverbal learning disabilities syndrome. Journal of Child Psychology and Psychiatry 36: 1127–40. [Google Scholar] [CrossRef] [PubMed]
- Rutter, Michael L. 1978. Diagnosis and definition of childhood autism. Journal of Autism and Childhood Schizophrenia 8: 139–61. [Google Scholar] [CrossRef] [PubMed]
- Wheelwright, Sally, Simon Baron-Cohen, Nigel Goldenfeld, Joe Delaney, Debra Fine, Richard Smith, Leonora Weil, and Akio Wakabayashi. 2006. Predicting Autism Spectrum Quotient (AQ) from the Systemizing Quotient-Revised (SQ-R) and Empathy Quotient (EQ). Brain Research 1079: 47–56. [Google Scholar] [CrossRef] [PubMed]
- Wing, Lorna, and Judith Gould. 1979. Severe impairments of social interaction and associated abnormalities in children: epidemiology and classification. Journal of Autism and Developmental Disorders 9: 11–29. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Instruments | N | Mean | SD | Min | Max | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Autism | Typical | Autism | Typical | Autism | Typical | Autism | Typical | Autism | Typical | |
| AQ Total Score | 34 * | 93 | 101.06 | 47.92 | 16.749 | 19.153 | 73 | 10 | 132 | 109 |
| AQ Score Boys | 26 | 49 | 101.65 | 53.69 | 17.497 | 20.971 | 73 | 22 | 132 | 109 |
| AQ Score Girls | 8 | 44 | 99.12 | 41.50 | 14.952 | 14.622 | 75 | 10 | 118 | 83 |
| EQ Total Score | 35 ** | 93 | 16.83 | 32.40 | 6.866 | 10.352 | 5 | 7 | 33 | 52 |
| EQ Score Boys | 27 | 49 | 16.41 | 29.76 | 6.541 | 10.995 | 5 | 7 | 33 | 51 |
| EQ Score Girls | 8 | 44 | 18.25 | 35.34 | 8.190 | 8.803 | 6 | 11 | 31 | 52 |
| SQ Total Score | 35 ** | 93 | 25.49 | 20.57 | 7.845 | 7.555 | 11 | 5 | 40 | 39 |
| SQ Score Boys | 27 | 49 | 25.48 | 21.33 | 7.439 | 7.392 | 11 | 6 | 39 | 39 |
| SQ Score Girls | 8 | 44 | 25.50 | 19.73 | 9.666 | 7.729 | 11 | 5 | 40 | 37 |
| AQ Total Score | ||||||
|---|---|---|---|---|---|---|
| Model | Sum of Squares | df | Mean Square | F | Sig. | |
| 1 | Regression | 73,325,840 | 2 | 36,662,920 | 113,728 | 000 b |
| Residual | 39,974,318 | 124 | 322,374 | |||
| Total | 113,300,157 | 126 | ||||
| AQ Total Score | ||||||
|---|---|---|---|---|---|---|
| Model | Unstandardized Coefficients | Standardized Coefficients | t | Sig. | ||
| B | Std. Error | Beta | ||||
| 1 | (Constant) | 164,343 | 7235 | 22,716 | 000 | |
| Diagnosis | −50,714 | 3684 | −752 | −13,767 | 000 | |
| Gender | −10,176 | 3317 | −168 | −3068 | 003 | |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Van der Zee, E.; Derksen, J. Identifying Autism through Empathizing and Systemizing Abilities. Soc. Sci. 2017, 6, 124. https://doi.org/10.3390/socsci6040124
Van der Zee E, Derksen J. Identifying Autism through Empathizing and Systemizing Abilities. Social Sciences. 2017; 6(4):124. https://doi.org/10.3390/socsci6040124
Chicago/Turabian StyleVan der Zee, Evi, and Jan Derksen. 2017. "Identifying Autism through Empathizing and Systemizing Abilities" Social Sciences 6, no. 4: 124. https://doi.org/10.3390/socsci6040124
APA StyleVan der Zee, E., & Derksen, J. (2017). Identifying Autism through Empathizing and Systemizing Abilities. Social Sciences, 6(4), 124. https://doi.org/10.3390/socsci6040124