
Lack of Thermal Comfort Is a Matter of Life and Death: A Systematic Review for Older People



Abstract
1. Introduction
2. Materials and Methods
3. Terminology and Categories
3.1. Terminology
3.2. Age Categories
3.3. Age Range of Vulnerability
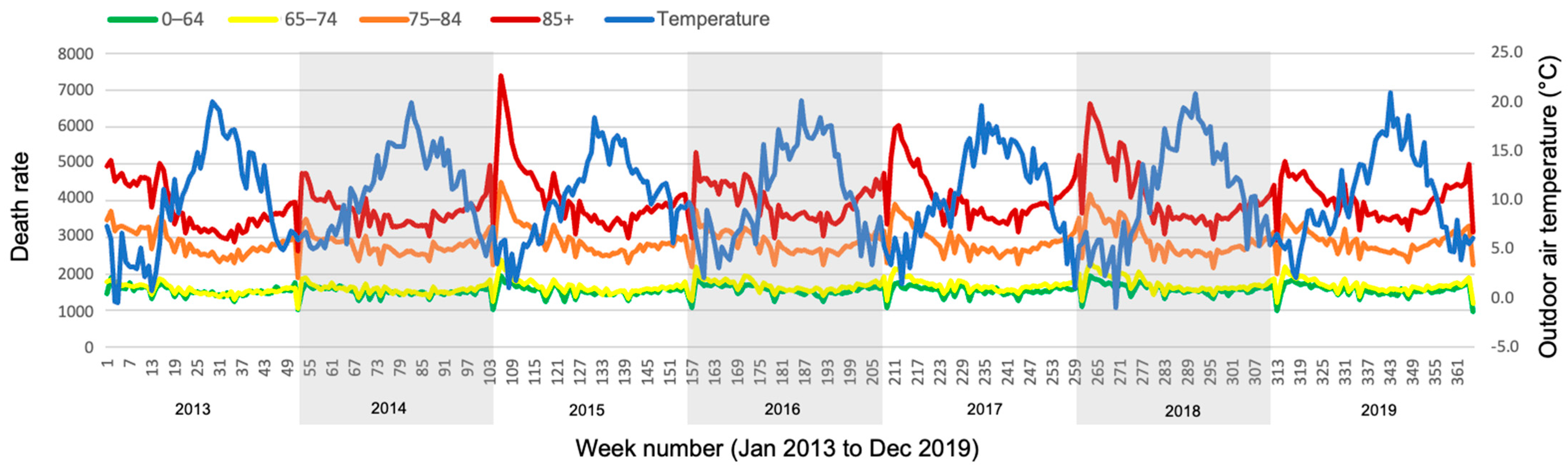
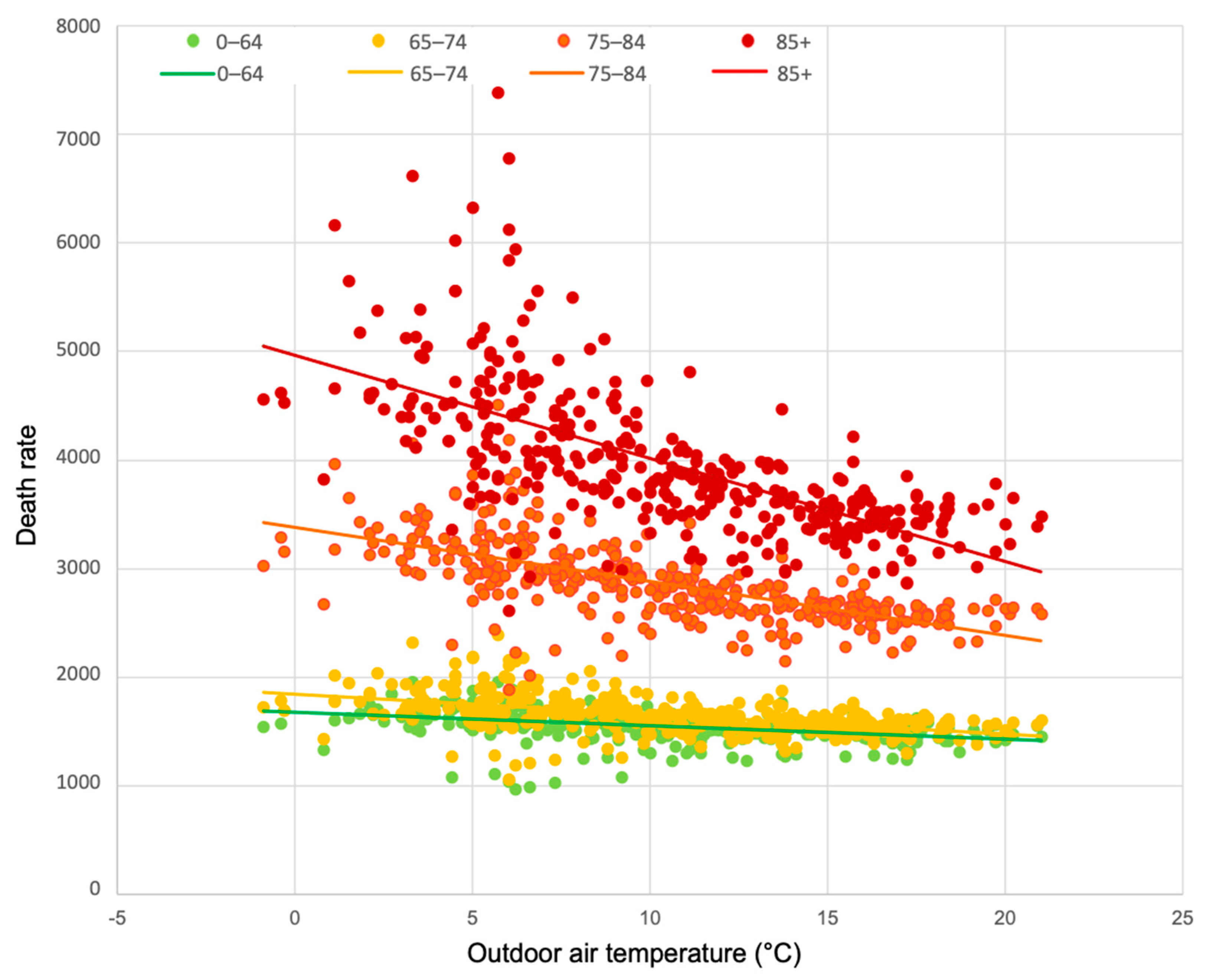
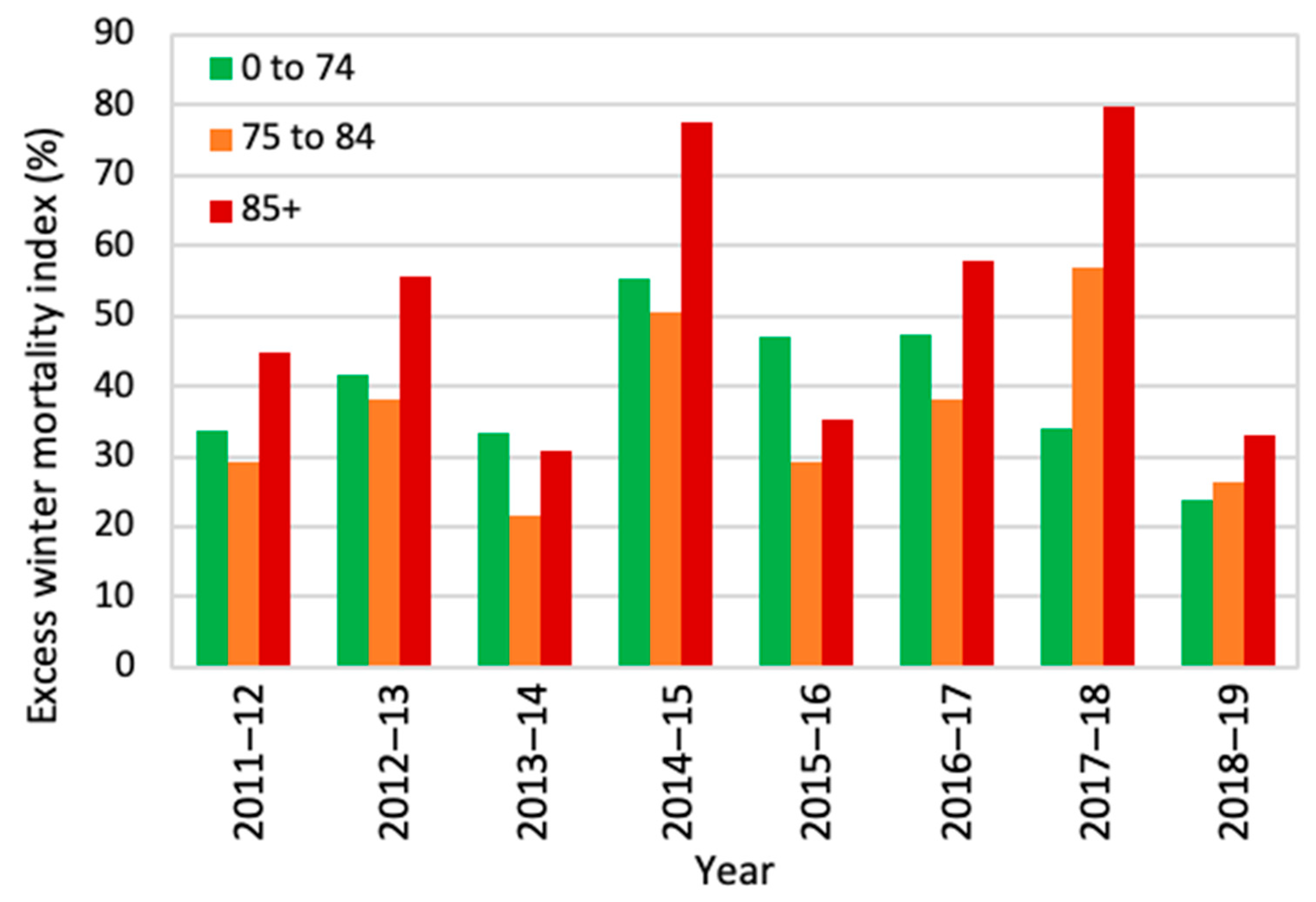
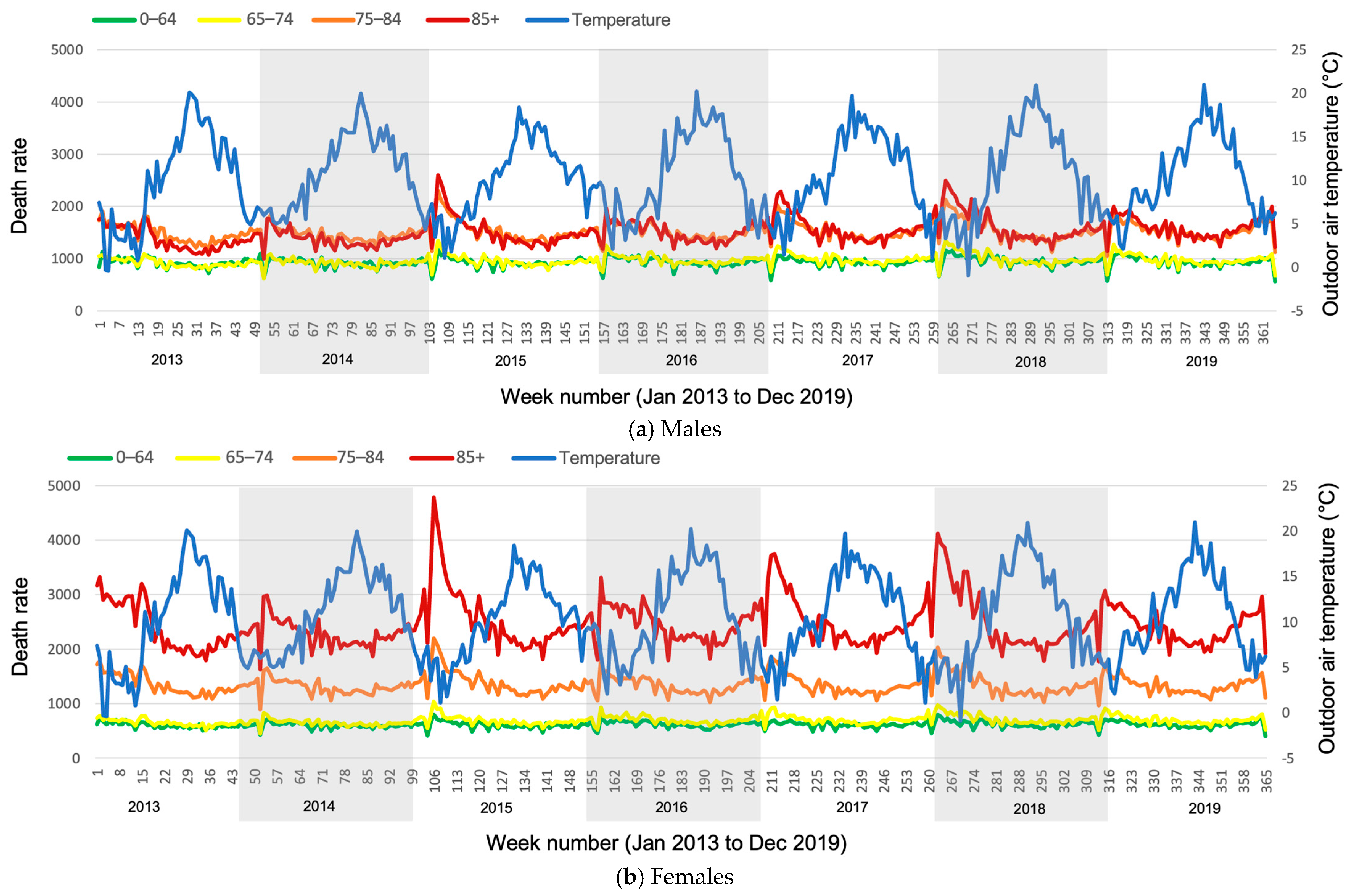
- 85+ years old: high (red line)
- 75–84 years old: medium (orange line)
- 0–74 years old: low (overlapping yellow and green lines)
4. Health and Mortality
4.1. Health and Extreme Temperatures
4.1.1. Hot
4.1.2. Cold
4.2. Thermal Sensitivity and Mobility
4.3. COVID-19 and Energy Crisis
4.4. Mortality
4.4.1. Hot Spells
4.4.2. Cold Spells
5. Gender Differences
5.1. Menopause
5.2. Mortality and Gender
6. Thermal Comfort and Temperature Limit
6.1. Standards and Guidelines
6.2. Thermal Comfort
6.3. Adaptive Behaviour
7. Conclusions
- Older people can be considered as vulnerable and at risk from extremes and changes in the thermal environment.
- Thermal comfort is related to the health of older people. It is a significant risk factor in the morbidity and mortality of older people when they are exposed to extreme weather conditions.
- Thermal comfort researchers consider different starting points for the age of older people, varying between 55 and 70+ years old, as demonstrated in Table 1. However, the thermal requirements of a 55-year-old can be considerably different from that of a 70-year-old.
- The recommendations for the upper limit of indoor air temperature varies between the WHO, CIBSE and ASHRAE. In some cases, no age categories are provided, while the requirements of an 80-year-old person may be significantly different from that of a 20-year-old person. Also, the WHO’s recommendation for older people is quite old and applies worldwide, without taking into account regional climatic considerations. Thermal comfort standards do not suitably apply to older people.
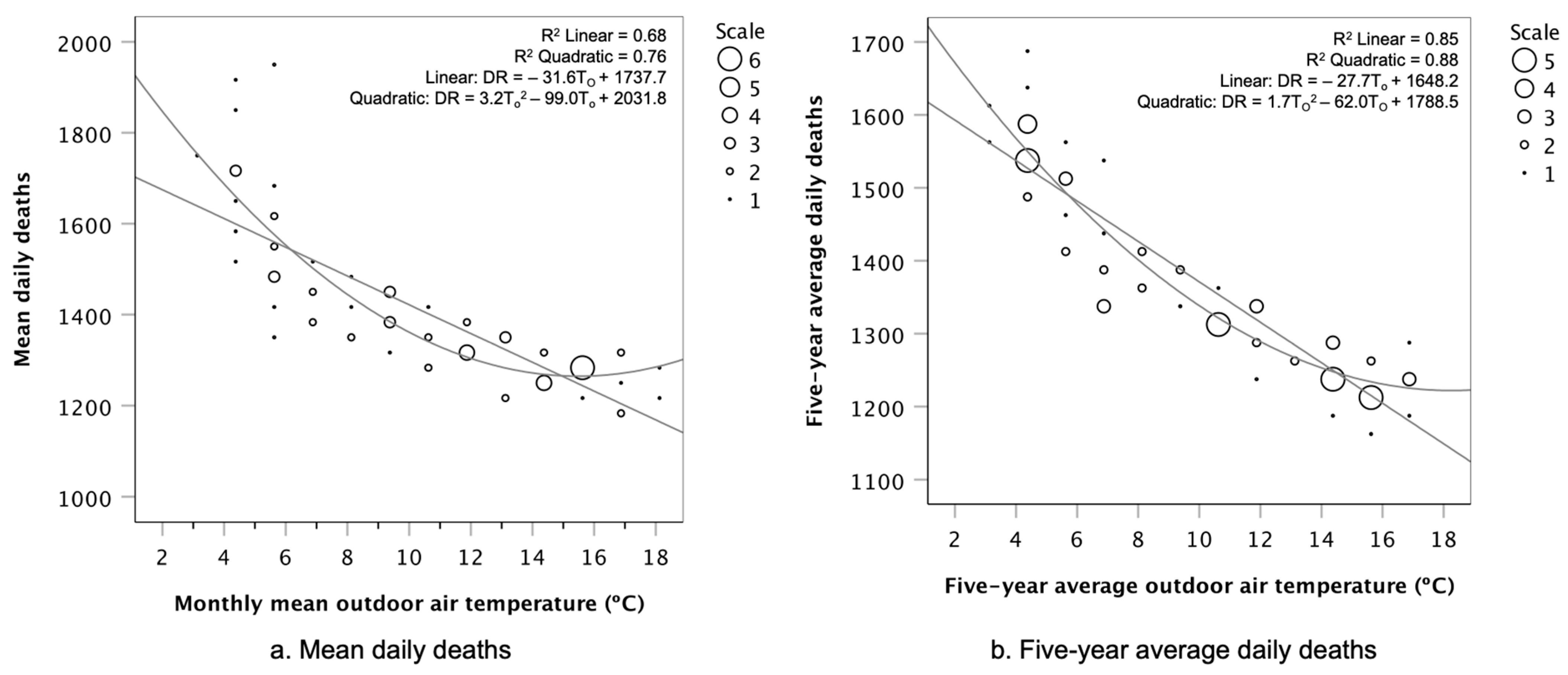
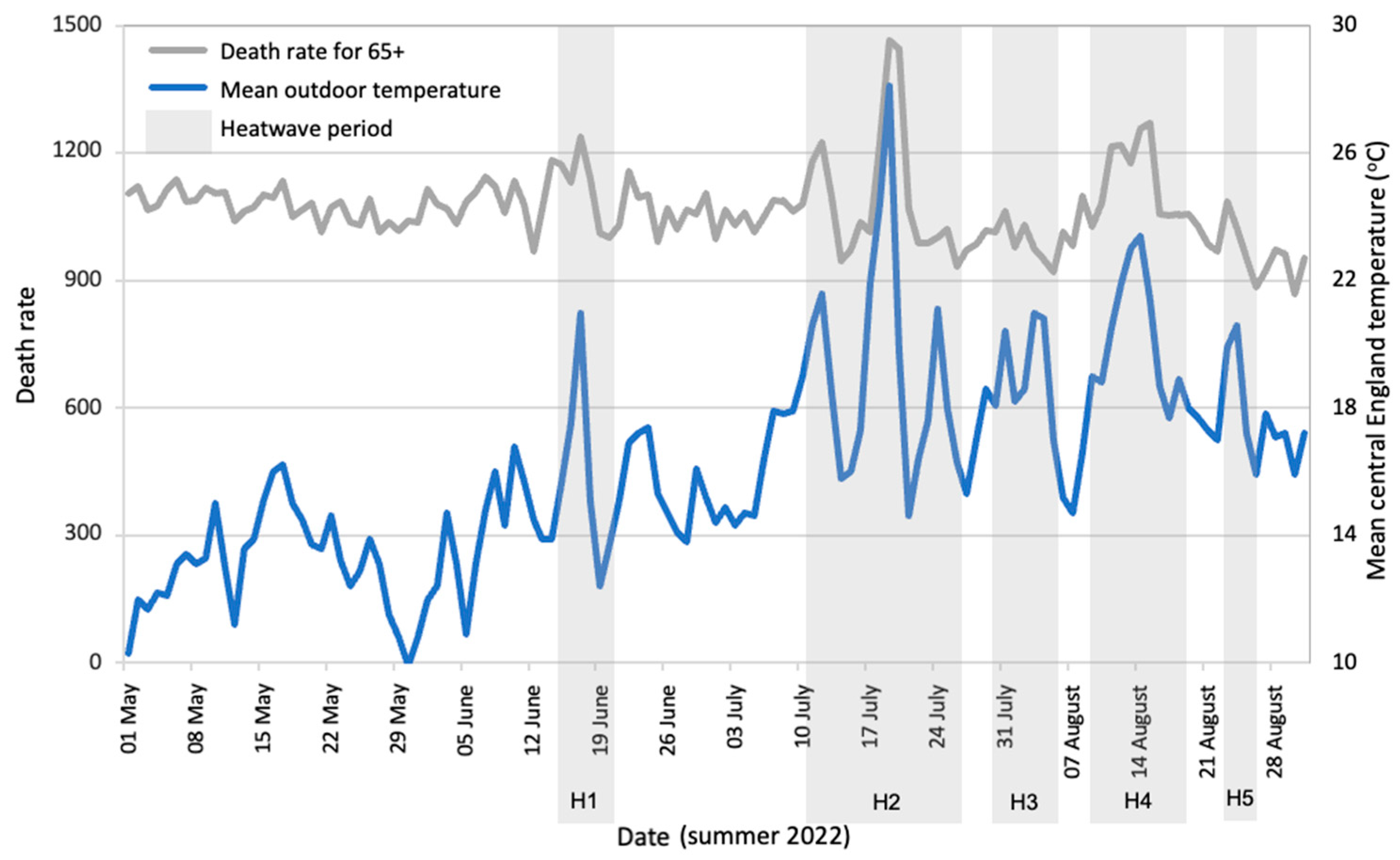
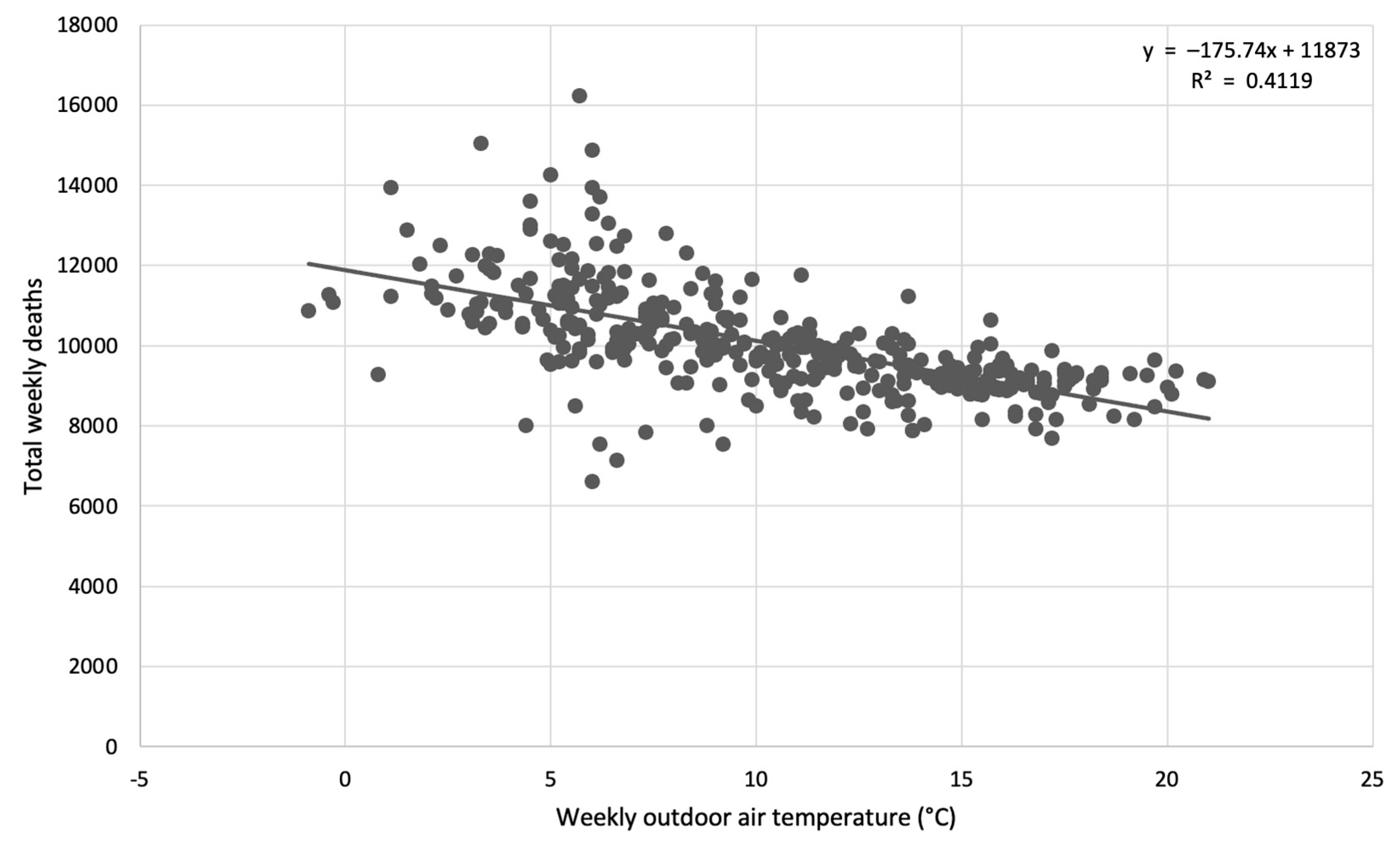
- A significant relationship was found between cold (below 5 °C) outdoor air temperatures and mortality in older people, particularly for those over 85 years old in the UK (based on the analysis of open data). Thermal conditions can be the direct and indirect cause of death up to two weeks after a cold spell or overheating occurs, which leads to up to 175 deaths per degree temperature change.
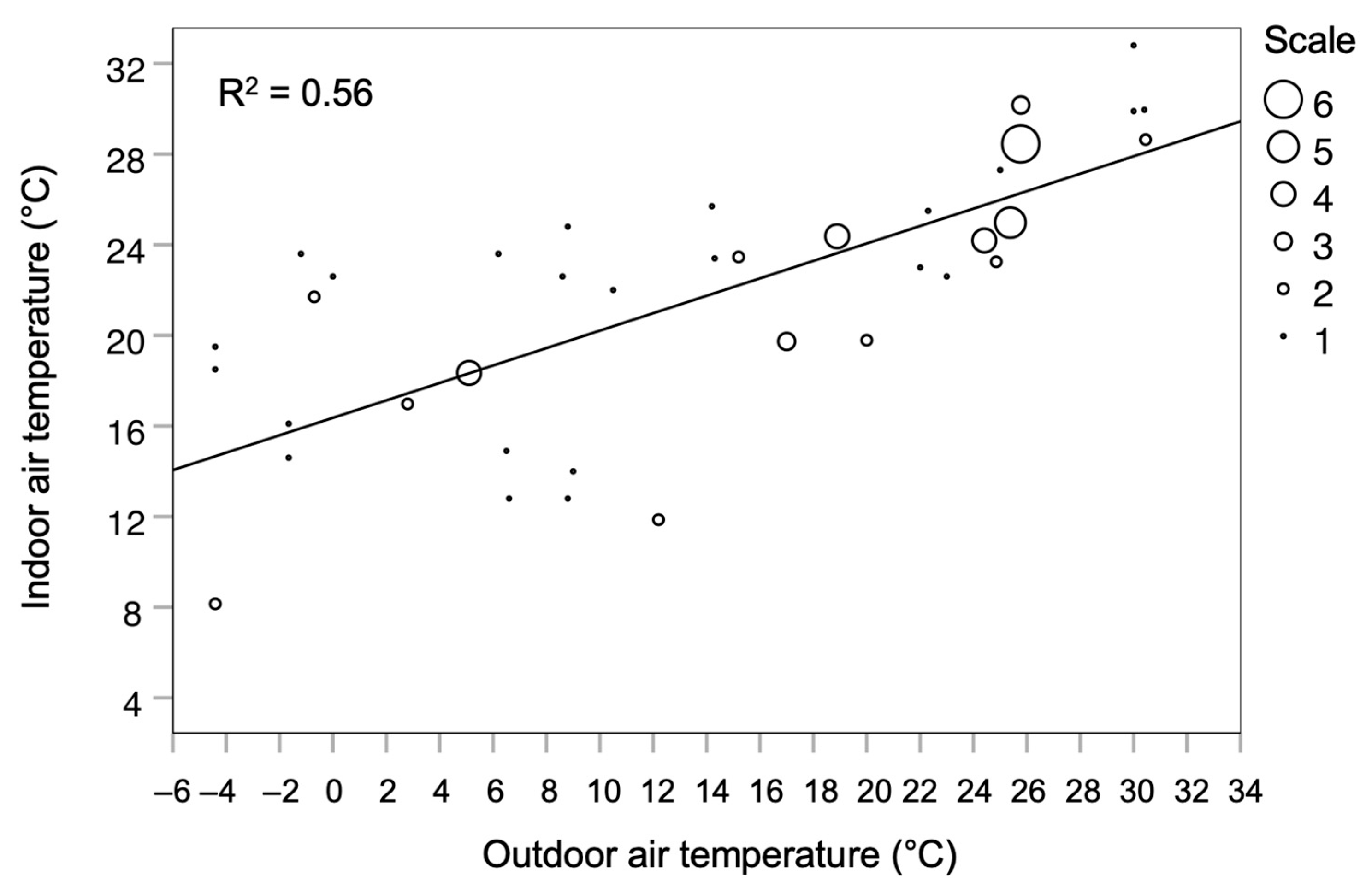
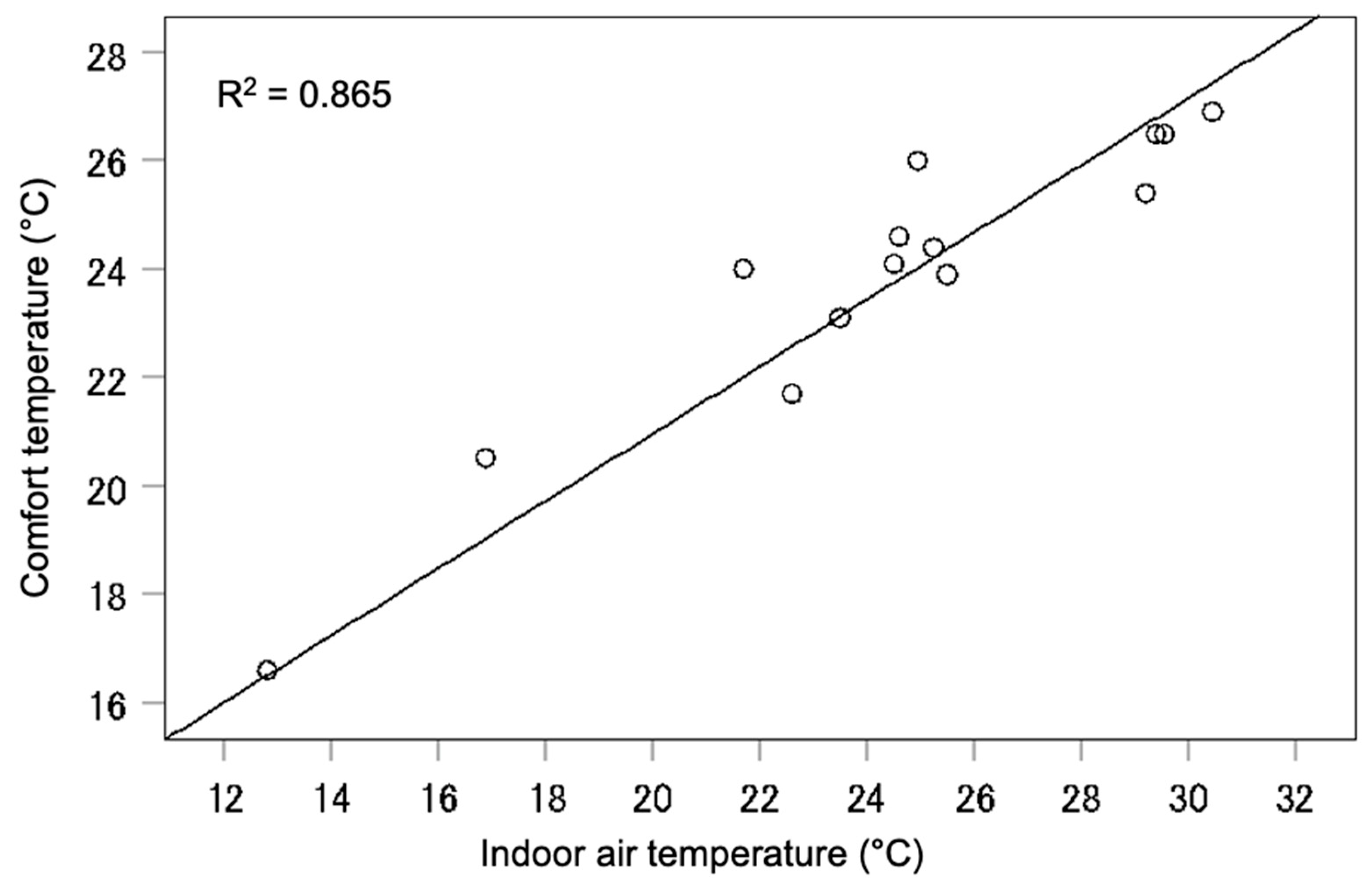
- Indoor and outdoor air temperatures for older people’s residences are significantly related. In low outdoor temperatures, the difference between the two is significant, while at higher outdoor temperatures they match. Similar results are found between comfort temperature and indoor air temperature. Thus, the energy requirement to warm up the space during the cold months is much greater than that for cooling during the warmer months.
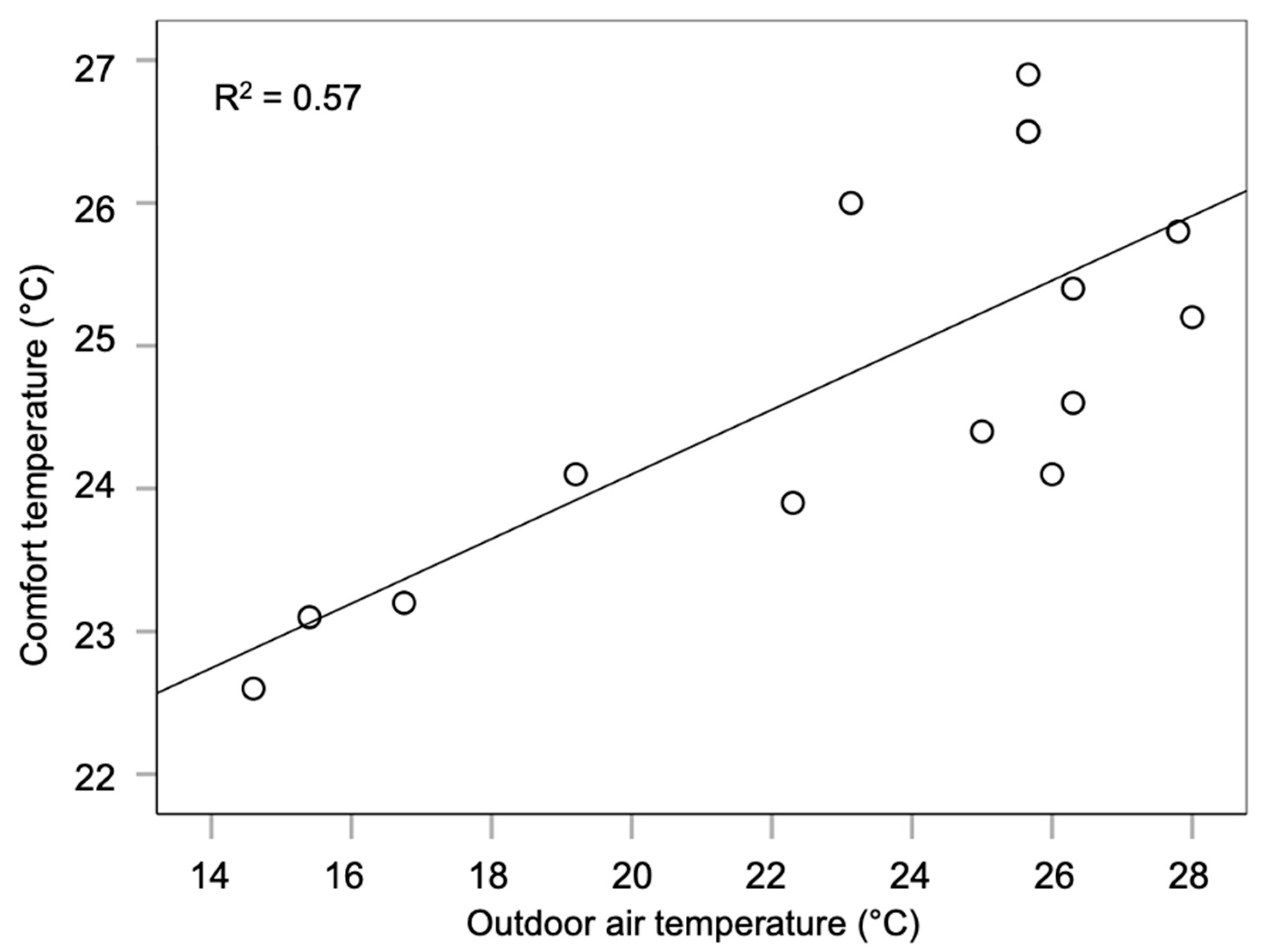
- Analysis of the data provided by limited research suggests the indoor comfort temperature for older people ranges between 22.5 and 27 °C in natural ventilation mode, which is higher than the vague WHO acceptable temperature range of 20 to 21 °C. However, some researchers found 18 °C to be comfortable for older people during the winter, which can lead to energy saving. Every degree of lowering the set point of the indoor air temperature leads to 10% energy saving in the building [151], resulting in a significant energy saving in the building [152].
7.1. Recommendations and Future Research
- “Older people” is the suitable terminology to be used for inclusivity reasons. “Elderly” is commonly used in thermal comfort research, but it is sometimes considered an offensive and exclusive language. Terminologies, such as “aged people” and “senior” are also inappropriate.
- Currently, there is a disparity regarding the starting age at which people are considered to be “older people” among researchers, governmental organisations and others. Physiology, thermal sensitivity, retirement age and other factors indicate different starting ages and, often, altering ones. Thus, further research is needed to determine the starting age or period for people to be considered “older people” particularly in thermal comfort research.
- Further research is needed to examine the thermal vulnerabilities and requirements of older people in different cultures, climatic regions and financial and fuel poverty-related areas, and differences in health, physiology and other factors. This may influence the starting point for the age of older people and age categories.
- In the current thermal comfort research, age categories are not considered for older people, though the thermal needs of people change as they age. Research is needed to define these age categories, such as those defined by Bytheway [51] as young-old (65–74 years old), middle-old (75–84 years old) and old-old (85+ years old).
- There is limited research on the thermal comfort requirements of older people regarding their sleep. The quality and quantity of sleep is significantly related to restoration and regeneration, which is much needed in older age.
- There is a lack of research on gender differences in thermal comfort requirements for older people, particularly related to menopause.
- There is limited research on acceptable, comfortable and preferred thermal ranges for older people.
- There is a lack of research on adaptive thermal behaviours, the availability of environmental control and the development and testing of Personal Comfort Systems for older people.
7.2. Possible Other Concersns
- This paper considers temperature to be the major dependent for thermal comfort and discomfort. Other components such as air movement and humidity can be important, and their effects should be investigated separately or together.
- What are the implications of the findings for the design of buildings for older people?
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lim, C.L.; Byrne, C.; Lee, J.K. Human thermoregulation and measurement of body temperature in exercise and clinical settings. Ann. Acad. Med. Singap. 2008, 37, 347. [Google Scholar]
- Morrison, S.F.; Nakamura, K. Central neural pathways for thermoregulation. Front. Biosci. A J. Virtual Libr. 2011, 16, 74. [Google Scholar] [CrossRef] [PubMed]
- Ohnaka, T.; Tochihara, Y.; Tsuzuki, K.; Nagai, Y.; Tokuda, T.; Kawashima, Y. Preferred temperature of the elderly after cold and heat exposures determined by individual self-selection of air temperature. J. Therm. Biol. 1993, 18, 349–353. [Google Scholar]
- Wong, L.T.; Fong, K.N.K.; Mui, K.W.; Wong, W.W.Y.; Lee, L.W. A field survey of the expected desirable thermal environment for older people. Indoor Built Environ. 2009, 18, 336–345. [Google Scholar]
- Hwang, R.L.; Chen, C.P. Field study on behaviors and adaptation of elderly people and their thermal comfort requirements in residential environments. Indoor Air 2010, 20, 235–245. [Google Scholar]
- Schellen, L.; van Marken Lichtenbelt, W.D.; Loomans, M.G.; Toftum, J.; De Wit, M.H. Differences between young adults and elderly in thermal comfort, productivity, and thermal physiology in response to a moderate temperature drift and a steady-state condition. Indoor Air 2010, 20, 273–283. [Google Scholar]
- Mendes, A.; Pereira, C.; Mendes, D.; Aguiar, L.; Neves, P.; Silva, S.; Batterman, S.; Teixeira, J.P. Indoor air quality and thermal comfort—Results of a pilot study in elderly care centers in Portugal. J. Toxicol. Environ. Health Part A 2013, 76, 333–344. [Google Scholar] [CrossRef]
- Mendes, A.; Bonassi, S.; Aguiar, L.; Pereira, C.; Neves, P.; Silva, S.; Mendes, D.; Guimarães, L.; Moroni, R.; Teixeira, J.P. Indoor air quality and thermal comfort in elderly care centers. Urban Clim. 2015, 14, 486–501. [Google Scholar]
- Bills, R. Cold comfort: Thermal sensation in people over 65 and the consequences for an ageing population. In Proceedings of the 9th International Windsor Conference 2016: Making Comfort Relevant, Windsor, UK, 7–10 April 2016; pp. 156–167. [Google Scholar]
- Bills, R.; Soebarto, V.; Williamson, T. Thermal experiences of older people during hot conditions in Adelaide. Revisiting the role of architectural science in design and practice. In Proceedings of the 50th International Conference of the Architectural Science Association, Adelaide, Australia, 7–9 December 2016; pp. 657–664. [Google Scholar]
- Yang, J.; Nam, I.; Sohn, J.R. The influence of seasonal characteristics in elderly thermal comfort in Korea. Energy Build. 2016, 128, 583–591. [Google Scholar]
- Jiao, Y.; Yu, H.; Wang, T.; An, Y.; Yu, Y. Thermal comfort and adaptation of the elderly in free-running environments in Shanghai, China. Build. Environ. 2017, 118, 259–272. [Google Scholar]
- Fan, G.; Xie, J.; Yoshino, H.; Yanagi, U.; Hasegawa, K.; Wang, C.; Zhang, X.; Liu, J. Investigation of indoor thermal environment in the homes with elderly people during heating season in Beijing, China. Build. Environ. 2017, 126, 288–303. [Google Scholar]
- Vellei, M.; Ramallo-González, A.P.; Coley, D.; Lee, J.; Gabe-Thomas, E.; Lovett, T.; Natarajan, S. Overheating in vulnerable and non-vulnerable households. Build. Res. Inf. 2017, 45, 102–118. [Google Scholar]
- Panraluk, C.; Sreshthaputra, A. Thermal comfort of the elderly in public health service buildings of Thailand. Appl. Mech. Mater. 2018, 878, 173–178. [Google Scholar]
- Hughes, C.; Natarajan, S.; Liu, C.; Chung, W.J.; Herrera, M. Winter thermal comfort and health in the elderly. Energy Policy 2019, 134, 110954. [Google Scholar] [CrossRef]
- Xiong, J.; Ma, T.; Lian, Z.; de Dear, R. Perceptual and physiological responses of elderly subjects to moderate temperatures. Build. Environ. 2019, 156, 117–122. [Google Scholar]
- Lan, L.; Xia, L.; Tang, J.; Zhang, X.; Lin, Y.; Wang, Z. Elevated airflow can maintain sleep quality and thermal comfort of the elderly in a hot environment. Indoor Air 2019, 29, 1040–1049. [Google Scholar]
- Forcada, N.; Gangolells, M.; Casals, M.; Tejedor, B.; Macarulla, M.; Gaspar, K. Summer thermal comfort in nursing homes in the Mediterranean climate. Energy Build. 2020, 229, 110442. [Google Scholar] [CrossRef]
- Yu, J.; Hassan, M.T.; Bai, Y.; An, N.; Tam, V. A pilot study monitoring the thermal comfort of the elderly living in nursing homes in Hefei, China, using wireless sensor networks, site measurements and a survey. Indoor Built Environ. 2020, 29, 449–464. [Google Scholar]
- Forcada, N.; Gangolells, M.; Casals, M.; Tejedor, B.; Macarulla, M.; Gaspar, K. Field study on adaptive thermal comfort models for nursing homes in the Mediterranean climate. Energy Build. 2021, 252, 111475. [Google Scholar]
- Larriva, M.T.B.; Mendes, A.S.; Forcada, N. The effect of climatic conditions on occupants’ thermal comfort in naturally ventilated nursing homes. Build. Environ. 2022, 214, 108930. [Google Scholar]
- Yao, F.; Fang, H.; Han, J.; Zhang, Y. Study on the outdoor thermal comfort evaluation of the elderly in the Tibetan plateau. Sustain. Cities Soc. 2022, 77, 103582. [Google Scholar]
- Yuan, J.; Cong, Y.; Yao, S.; Dai, C.; Li, Y. Research on the thermal comfort of the elderly in rural areas of cold climate, China. Adv. Build. Energy Res. 2022, 16, 612–642. [Google Scholar]
- Li, H.; Xu, G.; Chen, J.; Duan, J. Investigating the adaptive thermal comfort of the elderly in rural mutual aid homes in central Inner Mongolia. Sustainability 2022, 14, 6802. [Google Scholar] [CrossRef]
- Zheng, W.; Shao, T.; Lin, Y.; Wang, Y.; Dong, C.; Liu, J. A field study on seasonal adaptive thermal comfort of the elderly in nursing homes in Xi’an, China. Build. Environ. 2022, 208, 108623. [Google Scholar]
- Kainaga, T.; Sagisaka, K.; Yamada, R.; Nakaya, T. A case study of a nursing home in Nagano, Japan: Field survey on thermal comfort and building energy simulation for future climate change. Energies 2022, 15, 936. [Google Scholar] [CrossRef]
- Zheng, G.; Wei, C.; Li, K. Determining the summer indoor design parameters for pensioners’ buildings based on the thermal requirements of elderly people at different ages. Energy 2022, 258, 124854. [Google Scholar]
- Jiao, Y.; Yu, Y.; Yu, H.; Wang, F. The impact of thermal environment of transition spaces in elderly-care buildings on thermal adaptation and thermal behavior of the elderly. Build. Environ. 2022, 228, 109871. [Google Scholar]
- Zong, H.; Wang, J.; Zhou, T.; Sun, J.; Chen, X. The influence of transient changes in indoor and outdoor thermal comfort on the use of outdoor space by older adults in the nursing home. Buildings 2022, 12, 905. [Google Scholar] [CrossRef]
- Yoon Yi, C.; Childs, C.; Peng, C.; Robinson, D. Thermal comfort modelling of older people living in care homes: An evaluation of heat balance, adaptive comfort, and thermographic methods. Build. Environ. 2022, 207, 108550. [Google Scholar]
- Baquero, M.T.; Forcada, N. Thermal comfort of older people during summer in the continental Mediterranean climate. J. Build. Eng. 2022, 54, 104680. [Google Scholar]
- Walker, M. Why We Sleep: The New Science of Sleep and Dreams; Penguin: London, UK, 2017. [Google Scholar]
- Raymann, R.J.; Van Someren, E.J. Diminished capability to recognize the optimal temperature for sleep initiation may contribute to poor sleep in elderly people. Sleep 2008, 31, 1301–1309. [Google Scholar] [PubMed]
- Okamoto-Mizuno, K.; Tsuzuki, K. Effects of season on sleep and skin temperature in the elderly. Int. J. Biometeorol. 2010, 54, 401–409. [Google Scholar] [PubMed]
- Tsuzuki, K.; Mori, I.; Sakoi, T.; Kurokawa, Y. Effects of seasonal illumination and thermal environments on sleep in elderly men. Build. Environ. 2015, 88, 82–88. [Google Scholar]
- Xia, L.; Lan, L.; Tang, J.; Wan, Y.; Lin, Y.; Wang, Z. Bed heating improves the sleep quality and health of the elderly who adapted to no heating in a cold environment. Energy Build. 2020, 210, 109687. [Google Scholar]
- Tsuzuki, K.; Sakoi, T.; Sakata, Y. Effect of seasonal ambient temperature on sleep and thermal comfort in older people living in public elderly facilities. Buildings 2021, 11, 574. [Google Scholar] [CrossRef]
- Kido, C.; Kubo, H.; Azuma, M.; Sassa, N.; Hoshino, S.; Isoda, N. A field study on the thermal environments of bedrooms and the sleep quality of elderly people in summer in the urban and rural areas of Nara Prefecture. J. Hum. Environ. Syst. 2022, 25, 31–42. [Google Scholar]
- Yan, Y.; Lan, L.; Zhang, H.; Sun, Y.; Fan, X.; Wyon, D.P.; Wargocki, P. Association of bedroom environment with the sleep quality of elderly subjects in summer: A field measurement in Shanghai, China. Build. Environ. 2022, 208, 108572. [Google Scholar]
- Yan, Y.; Zhang, H.; Kang, M.; Lan, L.; Wang, Z.; Lin, Y. Experimental study of the negative effects of raised bedroom temperature and reduced ventilation on the sleep quality of elderly subjects. Indoor Air 2022, 32, e13159. [Google Scholar]
- North Tyneside Age UK. Is ‘Elderly’ Offensive? 2019. Available online: https://www.ageuk.org.uk/northtyneside/about-us/news/articles/2019/offensive-description-of-older-people/ (accessed on 2 February 2023).
- World Health Organization. Quick Guide to Avoid Ageism in Communication. 2021. Available online: https://www.who.int/publications/m/item/quick-guide-to-avoid-ageism-in-communication (accessed on 23 February 2025).
- Centre for Ageing Better. Challenging Ageism: A Guide to Talking About Ageing and Older Age. 2021. Available online: https://ageing-better.org.uk/sites/default/files/2021-12/Challenging-ageism-guide-talking-ageing-older-age.pdf (accessed on 23 February 2025).
- Morrison, S. Don’t Call Me “Old”: Avoiding Ageism When Writing About Aging; National Institute on Aging: Bethesda, MD, USA, 2023. [Google Scholar]
- Chen, M.; Kosonen, R.; Kilpeläinen, S.; Ming, R. A review of thermal comfort modeling of elderly people. In Proceedings of the CLIMA2022: The 14 REHVA World Congress, Rotterdam, The Netherlands, 22–25 May 2022. [Google Scholar]
- Zhou, S.; Li, B.; Du, C.; Liu, H.; Wu, Y.; Hodder, S.; Chen, M.; Kosonen, R.; Ming, R.; Ouyang, L.; et al. Opportunities and challenges of using thermal comfort models for building design and operation for the elderly: A literature review. Renew. Sustain. Energy Rev. 2023, 183, 113504. [Google Scholar]
- Guergova, S.; Dufour, A. Thermal sensitivity in the elderly: A review. Ageing Res. Rev. 2011, 10, 80–92. [Google Scholar] [CrossRef]
- Butler, R.N. Why Survive? Being Old in America; Harper & Row: New York, NY, USA, 1975. [Google Scholar]
- Johnson, J.; Bytheway, B. Ageism: Concept and definition. In Ageing and Later Life; Johnson, J., Slater, R., Eds.; Sage Publications: Thousand Oaks, CA, USA, 1993. [Google Scholar]
- Bytheway, B. Ageism and age categorization. J. Soc. Issues 2005, 61, 361–374. [Google Scholar] [CrossRef]
- Barnes, J.N.; Charkoudian, N. Integrative cardiovascular control in women: Regulation of blood pressure, body temperature and cerebrovascular responsiveness. FASEB J. 2020, 35, e21143. [Google Scholar] [CrossRef] [PubMed]
- ONS. Mortality in England and Wales: Past and Projected Trends in Average Lifespan; Office for National Statistics, UK Government: Newport, UK, 2022.
- UN. Life Expectancy at Birth for Both Sexes Combined (Years). World Population Prospects: The 2024 Revision. UN Data: A World of Information; United Nations Population Division: New York, NY, USA, 2024. [Google Scholar]
- Hobson, F. State Pension age review. In Research Briefing No. 06546; UK Parliament: London, UK, 2022. [Google Scholar]
- Department for Work and Pensions. Autumn Statement Announcement on a Core Principle Underpinning Future State Pension Age Rises: DWP Background Note; UK Government: London, UK, 2013.
- OECD. Pensions at a Glance 2021: OECD and G20 Indicators; Organisation for Economic Co-Operation and Development: Paris, France, 2021. [Google Scholar]
- Healy, J.D. Excess winter mortality in Europe: A cross country analysis identifying key risk factors. J. Epidemiol. Community Health 2003, 57, 784–789. [Google Scholar] [CrossRef] [PubMed]
- Beniston, M.; Stephenson, D.B.; Christensen, O.B.; Ferro, C.A.T.; Frei, C.; Goyette, S.; Halsnaes, K.; Holt, T.; Jylhä, K.; Koffi, B.; et al. Future extreme events in European climate: An exploration of regional climate model projections. Clim. Change 2007, 81, 71–95. [Google Scholar] [CrossRef]
- IPCC. Summary for Policymakers. In Global Warming of 1.5 °C. An IPCC Special Report on the Impacts of Global Warming of 1.5 °C Above Pre-Industrial Levels and Related Global Greenhouse Gas Emission Pathways, in the Context of Strengthening the Global Response to the Threat of Climate Change, Sustainable Development, and Efforts to Eradicate Poverty; Masson-Delmotte, V., Zhai, P., Pörtner, H.O., Roberts, D., Skea, J., Shukla, P.R., Pirani, A., Moufouma-Okia, W., Péan, C., Pidcock, R., et al., Eds.; Cambridge University Press: Cambridge, UK, 2018; pp. 3–24. [Google Scholar]
- Basu, R.; Samet, J.M. Relation between elevated ambient temperature and mortality: A review of the epidemiologic evidence. Epidemiol. Rev. 2002, 24, 190–202. [Google Scholar] [CrossRef]
- Bunker, A.; Wildenhain, J.; Vandenbergh, A.; Henschke, N.; Rocklöv, J.; Hajat, S.; Sauerborn, R. Effects of air temperature on climate-sensitive mortality and morbidity outcomes in the elderly; A systematic review and meta-analysis of epidemiological evidence. EBioMedicine 2016, 6, 258–268. [Google Scholar] [CrossRef]
- Climate Change Committee. Heat and Preventable Deaths in the Health and Social care System. 2019 UK. Available online: https://www.theccc.org.uk/wp-content/uploads/2019/07/Outcomes-Heat-preventable-deaths-case-study.pdf (accessed on 1 March 2024).
- Pallubinsky, H.; van Marken Lichtenbelt, W.; Kramer, R.P. Humans and buildings in times of climate change–A perspective on resilience. In Proceedings of the 3rd International Conference on Comfort at the Extremes: COVID, Climate Change and Ventilation CATE, Edinburgh, UK, 5–6 September 2022; pp. 8–10. [Google Scholar]
- Brunt, V.E.; Howard, M.J.; Francisco, M.A.; Ely, B.R.; Minson, C.T. Passive heat therapy improves endothelial function, arterial stiffness and blood pressure in sedentary humans. J. Physiol. 2016, 594, 5329–5342. [Google Scholar] [CrossRef]
- Hoekstra, S.P.; Bishop, N.C.; Faulkner, S.H.; Bailey, S.J.; Leicht, C.A. Acute and chronic effects of hot water immersion on inflammation and metabolism in sedentary, overweight adults. J. Appl. Physiol. 2018, 125, 2008–2018. [Google Scholar] [CrossRef]
- Pallubinsky, H.; Phielix, E.; Dautzenberg, B.; Schaart, G.; Connell, N.J.; de Wit-Verheggen, V.; Havekes, B.; van Baak, M.A.; Schrauwen, P.; Lichtenbelt, W.D.v.M. Passive exposure to heat improves glucose metabolism in overweight humans. Acta Physiol. 2020, 229, e13488. [Google Scholar] [CrossRef]
- Wongsurawat, N.; Davis, B.B.; Morley, J.E. Thermoregulatory failure in the elderly: St. Louis University geriatric grand rounds. J. Am. Geriatr. Soc. 1990, 38, 899–906. [Google Scholar] [CrossRef]
- ONS. Overview of the UK Population: An Overview of the UK Population Incorporating Data Related to 2020, How It Has Changed, Why It Has Changed and How It Is Projected to Change in the Future; Office for National Statistics, UK Government: Newport, UK, 2020.
- Havenith, G. Temperature regulation and technology. Gerontech J. 2001, 1, 41–49. [Google Scholar] [CrossRef]
- Wilson, M.M.G.; Morley, J.E. Invited review: Aging and energy balance. J. Appl. Physiol. 2003, 95, 1728–1736. [Google Scholar] [CrossRef] [PubMed]
- Shibasaki, M.; Okazaki, K.; Inoue, Y. Aging and thermoregulation. J. Phys. Fit. Sports Med. 2013, 2, 37–47. [Google Scholar] [CrossRef]
- Kenney, W.L.; Chiu, P. Influence of age on thirst and fluid intake. Med. Sci. Sports Exerc. 2001, 33, 1524–1532. [Google Scholar] [CrossRef]
- Ferry, M. Strategies for ensuring good hydration in the elderly. Nutr. Rev. 2005, 63, 22–29. [Google Scholar] [CrossRef]
- Blatteis, C.M. Age-dependent changes in temperature regulation—A mini review. Gerontology 2012, 58, 289–295. [Google Scholar] [CrossRef]
- WHO. Heat and Health. Newsroom Fact Sheet; World Health Organisation: Geneva, Switzerland, 2024. [Google Scholar]
- Turk, E.E. Hypothermia. Forensic Sci. Med. Pathol. 2010, 6, 106–115. [Google Scholar] [CrossRef]
- Hirvonen, J.K. Handbuch Gerichtliche Medizin; Brinkmann, B., Madea, B., Eds.; Springer: Berlin/Heidelberg, Germany, 2003. [Google Scholar]
- Krzyżewska, A.; Dobek, M.; Domżał-Drzewicka, R.; Rząca, M. Emergency interventions due to weather-related hypothermia. Weather 2017, 72, 8–12. [Google Scholar] [CrossRef]
- Collins, K.J.; Exton-Smith, A.N.; Dore, C. Urban hypothermia: Preferred temperature and thermal perception in old age. Br. Med. J. (Clin. Res. Ed.) 1981, 282, 175–177. [Google Scholar] [CrossRef]
- Fox, R.H.; MacGibbon, R.; Davies, L.; Woodward, P.M. Problem of the old and the cold. Br. Med. J. 1973, 1, 21–24. [Google Scholar] [CrossRef]
- Foxman, E.F.; Storer, J.A.; Fitzgerald, M.E.; Wasik, B.R.; Hou, L.; Zhao, H.; Turner, P.E.; Pyle, A.M.; Iwasaki, A. Temperature-dependent innate defense against the common cold virus limits viral replication at warm temperature in mouse airway cells. Proc. Natl. Acad. Sci. USA 2015, 112, 827–832. [Google Scholar] [CrossRef] [PubMed]
- Rijal, H.B.; Yoshida, H.; Umemiya, N. Seasonal and regional differences in neutral temperatures in Nepalese traditional vernacular houses. Build. Environ. 2010, 45, 2743–2753. [Google Scholar] [CrossRef]
- Woodhouse, P.R.; Khaw, K.T.; Plummer, M. Seasonal variation of blood pressure and its relationship to ambient temperature in an elderly population. J. Hypertens. 1993, 11, 1267–1274. [Google Scholar] [CrossRef]
- Lloyd, E.L.; McCormack, C.; McKeever, M.; Syme, M. The effect of improving the thermal quality of cold housing on blood pressure and general health: A research note. J. Epidemiol. Community Health 2008, 62, 793–797. [Google Scholar] [CrossRef] [PubMed]
- Shortt, N.; Rugkåsa, J. “The walls were so damp and cold” fuel poverty and ill health in Northern Ireland: Results from a housing intervention. Health Place 2007, 13, 99–110. [Google Scholar] [CrossRef]
- Lomas, K.J.; Porritt, S.M. Overheating in buildings: Lessons from research. Build. Res. Inf. 2017, 45, 1–18. [Google Scholar]
- Aspvik, N.P.; Viken, H.; Ingebrigtsen, J.E.; Zisko, N.; Mehus, I.; Wisløff, U.; Stensvold, D. Do weather changes influence physical activity level among older adults?–The Generation 100 study. PLoS ONE 2018, 13, e0199463. [Google Scholar]
- Lindemann, U.; Oksa, J.; Skelton, D.A.; Beyer, N.; Klenk, J.; Zscheile, J.; Becker, C. Effect of cold indoor environment on physical performance of older women living in the community. Age Ageing 2014, 43, 571–575. [Google Scholar] [CrossRef]
- Paynter, S. Humidity and respiratory virus transmission in tropical and temperate settings. Epidemiol. Infect. 2015, 143, 1110–1118. [Google Scholar]
- Calderón-Larrañaga, A.; Dekhtyar, S.; Vetrano, D.L.; Bellander, T.; Fratiglioni, L. COVID-19: Risk accumulation among biologically and socially vulnerable older populations. Ageing Res. Rev. 2020, 63, 101149. [Google Scholar]
- ONS. Deaths Involving COVID-19 in the Care Sector, England and Wales: Deaths Occurring up to 12 June 2020 and Registered up to 20 June 2020 (Provisional); Office for National Statistics, UK Government: Newport, UK, 2020.
- West, E.; Moore, K.; Kupeli, N.; Sampson, E.L.; Nair, P.; Aker, N.; Davies, N. Rapid review of decision-making for place of care and death in older people: Lessons for COVID-19. Age Ageing 2021, 50, 294–306. [Google Scholar] [CrossRef] [PubMed]
- Almeida-Silva, M.; Wolterbeek, H.T.; Almeida, S.M. Elderly exposure to indoor air pollutants. Atmos. Environ. 2014, 85, 54–63. [Google Scholar] [CrossRef]
- Abdelbasset, W.K. Stay Home: Role of physical exercise training in elderly individuals’ ability to face the COVID-19 infection. J. Immunol. Res. 2020, 1, 8375096. [Google Scholar] [CrossRef] [PubMed]
- Age UK. Winter Warmth Services—Impact Report 2011–2014. UK, 2014. Available online: https://www.ageuk.org.uk/siteassets/documents/reports-and-publications/evaluation-reports/winter_warmth_impact_report.pdf (accessed on 1 March 2024).
- Age UK. Number of Older People Worried About Heating Their Homes Jumps to Nearly Eight Million as Energy Crisis Deepens. UK. 2022. Available online: https://www.ageuk.org.uk/latest-press/articles/2022/number-of-older-people-worried-about-heating-their-homes-jumps-to-nearly-eight-million-as-energy-crisis-deepens/ (accessed on 1 March 2024).
- Shaw, V. Over-65s May Go Without Food or Heat to Cope with Energy Bill Rises, Says Age UK. The Independent. 2022. Available online: https://www.independent.co.uk/money/over65s-may-go-without-food-or-heat-to-cope-with-energy-bill-rises-says-age-uk-b2003268.html (accessed on 1 March 2024).
- Age UK. Energy Crisis Is Still Causing Misery for the Poorest Pensioners, Says Age UK. 2024. Available online: https://www.ageuk.org.uk/latest-press/articles/2024/energy-crisis-is-still-causing-misery-for-the-poorest-pensioners-says-age-uk/ (accessed on 23 February 2025).
- Roys, M.; Nicol, S.; Garrett, H.; Margoles, S. The Full Cost of Poor Housing; IHS BRE Press: Watford, UK, 2016. [Google Scholar]
- Nicol, S.; Roys, M.; Garett, H. The Cost of Poor Housing to the NHS: Briefing Paper; Building Research Establishment BRE: Garston, UK, 2011. [Google Scholar]
- Age UK. Poverty in Later Life; Age UK Love After Life; Age UK: London, UK, 2022. [Google Scholar]
- ONS. Climate-Related Mortality, England and Wales: 1988 to 2022. Relative Risk of Death Associated with Temperature for England and Wales from 1988 to 2022; Office for National Statistics, UK Government: Newport, UK, 2022.
- ONS. Excess Mortality During Heat-Periods: 1 June to 31 August 2022. Joint Analytical Article Between the Office for National Statistics (ONS) and UK Health Security Agency (UKHSA) on Deaths During Heat-Periods in 2022; Office for National Statistics, UK Government: Newport, UK, 2022.
- ONS. Excess Winter Mortality in England and Wales: 2017 to 2018 (Provisional) and 2016 to 2017 (Final). More People Die in the Winter Than the Summer. We Present Data by Sex, Age, Region and Cause of Death; Office for National Statistics, UK Government: Newport, UK, 2018.
- Kalkstein, L.S.; Greene, J.S. An evaluation of climate/mortality relationships in large US cities and the possible impacts of a climate change. Environ. Health Perspect. 1997, 105, 84–93. [Google Scholar] [CrossRef]
- Donaldson, G.C.; Kovats, R.S.; Keatinge, W.R.; McMichael, A.J. Heat-and cold-related mortality and morbidity and climate change. Health Eff. Clim. Change UK 2001, 70–80. [Google Scholar]
- Koppe, C.; Kovats, S.; Jendritzky, G.; Menne, B. Heat-Waves: Risks and Responses; Health and Global Environmental Change No. 2; WHO: Geneva, Switzerland, 2004. [Google Scholar]
- Perkins-Kirkpatrick, S.E.; Lewis, S.C. Increasing trends in regional heatwaves. Nat. Commun. 2020, 11, 3357. [Google Scholar] [CrossRef]
- ONS. Do Summer Heatwaves Lead to an Increase in Deaths? When the UK’s Hottest Day on Record Was Recorded This Summer, an Increase in Deaths Followed. We Look at How Hot Weather Affects the Number of Deaths That Occur; Office for National Statistics, UK Government: Newport, UK, 2019.
- Bobb, J.F.; Peng, R.D.; Bell, M.L.; Dominici, F. Heat-related mortality and adaptation to heat in the United States. Environ. Health Perspect. 2014, 122, 811–816. [Google Scholar] [CrossRef]
- Robine, J.M.; Cheung, S.L.K.; Le Roy, S.; Van Oyen, H.; Griffiths, C.; Michel, J.-P.; Herrmann, F.R. Death toll exceeded 70,000 in Europe during the summer of 2003. Comptes Rendus Biol. 2008, 331, 171–178. [Google Scholar] [CrossRef]
- Bobb, J.F.; Obermeyer ZWang, Y.; Dominici, F. Cause-specific risk of hospital admission related to extreme heat in older adults. JAMA 2014, 312, 2659–2667. [Google Scholar] [CrossRef]
- Hopp, S.; Dominici, F.; Bobb, J.F. Medical diagnoses of heat wave-related hospital admissions in older adults. Prev. Med. 2018, 110, 81–85. [Google Scholar] [CrossRef]
- Hajat, S.; Kovats, R.S.; Lachowycz, K. Heat-related and cold-related deaths in England and Wales: Who is at risk? Occup. Environ. Med. 2007, 64, 93–100. [Google Scholar] [PubMed]
- UK Health Security Agency. Research and Analysis. Heat Mortality Monitoring Report: 2022; UK Government: London, UK, 2024.
- Meng, C.; Ke, F.; Xiao, Y.; Huang, S.; Duan, Y.; Liu, G.; Yu, S.; Fu, Y.; Peng, J.; Cheng, J.; et al. Effect of cold spells and their different definitions on mortality in Shenzhen, China. Front. Public Health 2022, 9, 817079. [Google Scholar]
- Wang, L.; Liu, T.; Hu, M.; Zeng, W.; Zhang, Y.; Rutherford, S.; Lin, H.; Xiao, J.; Yin, P.; Liu, J.; et al. The impact of cold spells on mortality and effect modification by cold spell characteristics. Sci. Rep. 2016, 6, 38380. [Google Scholar] [CrossRef] [PubMed]
- Ruse, J.L. Fuel poverty and cold-related ill health. In Tackling Causes and Consequences of Health Inequalities: A Practical Guide; CRC Press: Florida, FL, USA, 2020; pp. 41–50. [Google Scholar]
- Fisk, W.; Seppanen, O. Providing better indoor environmental quality brings economic benefits. In Proceedings of the 9th REHVA World Congress Clima 2007 “WellBeing Indoors”, Helsinki, Finland, 10–14 June 2007. [Google Scholar]
- Wilkinson, P.; Pattenden, S.; Armstrong, B.; Fletcher, A.; Kovats, R.S.; Mangtani, P.; McMichael, A.J. Vulnerability to winter mortality in elderly people in Britain: Population based study. BMJ 2004, 329, 647. [Google Scholar]
- Vaisrub, S. Accidental hypothermia in the elderly. JAMA 1978, 239, 1888. [Google Scholar] [CrossRef]
- Age UK. Excess Winter Deaths: A Chilling Reminder of How the Cold Affects Older People; Age UK: Whitchurch, UK, 2016. [Google Scholar]
- Karjalainen, S. Thermal comfort and gender: A literature review. Indoor Air 2012, 22, 96–109. [Google Scholar]
- Kaciuba-Uscilko, H.; Grucza, R. Gender differences in thermoregulation. Curr. Opin. Clin. Nutr. Metab. Care 2001, 4, 533–536. [Google Scholar]
- Tejedor, B.; Casals, M.; Gangolells, M.; Macarulla, M.; Forcada, N. Human comfort modelling for elderly people by infrared thermography: Evaluating the thermoregulation system responses in an indoor environment during winter. Build. Environ. 2020, 186, 107354. [Google Scholar] [CrossRef]
- Díaz, J.; Garcia, R.; Velázquez de Castro, F.; Hernández, E.; López, C.; Otero, A. Effects of extremely hot days on people older than 65 years in Seville (Spain) from 1986 to 1997. Int. J. Biometeorol. 2002, 46, 145–149. [Google Scholar]
- Rey, G.; Jougla, E.; Fouillet, A.; Pavillon, G.; Bessemoulin, P.; Frayssinet, P.; Clavel, J.; Hémon, D. The impact of major heat waves on all—Cause and cause—Specific mortality in France from 1971 to 2003. Int. Arch. Occup. Environ. Health 2007, 80, 615–626. [Google Scholar]
- Åström, D.O.; Bertil, F.; Joacim, R. Heat wave impact on morbidity and mortality in the elderly population: A review of recent studies. Maturitas 2011, 69, 99–105. [Google Scholar] [PubMed]
- Hansen, A.; Bi, P.; Pisaniello, D.; Nitschke, M.; Tucker, G.; Newbury, J.; Kitson, A.; Grande, E.D.; Avery, J.; Zhang, Y.; et al. Heat-health behaviours of older people in two Australian states. Australas. J. Ageing 2015, 34, E19–E25. [Google Scholar] [PubMed]
- Shahzad, S.; Disci, Z.N.; Mody, S.; Basavapatna Kumaraswamy, S.; Calautit, J.K. Older people, thermal comfort behaviour and related energy use. In Proceedings of the International Conference on Applied Energy 2020, Bangkok, Thailand, 1–10 December 2020. [Google Scholar]
- Kastrup, A.; Dichgans, J.; Niemeier, M.; Schabet, M. Changes of cerebrovascular CO2 reactivity during normal aging. Stroke 1998, 29, 1311–1314. [Google Scholar]
- Liu, W.; Lou, X.; Ma, L. Use of 3D pseudo-continuous arterial spin labeling to characterize sex and age differences in cerebral blood flow. Neuroradiology 2016, 58, 943–948. [Google Scholar]
- Treloar, A.E. Menstrual cyclicity and the pre-menopause. Maturitas 1981, 3, 249–264. [Google Scholar]
- Avis, N.E.; Crawford, S.L.; Greendale, G.; Bromberger, J.T.; Everson-Rose, S.A.; Gold, E.B.; Hess, R.; Joffe, H.; Kravitz, H.M.; Tepper, P.G.; et al. Duration of menopausal vasomotor symptoms over the menopause transition. JAMA Intern. Med. 2015, 175, 531–539. [Google Scholar]
- Carter, S.K. Menopause, Hot Flushes, and Thermal Comfort in the Workplace. Ph.D. Thesis, The University of Sydney, Camperdown, Australia, 2022. [Google Scholar]
- Kronenberg, F.; Barnard, R.M. Modulation of menopausal hot flashes by ambient temperature. J. Therm. Biol. 1992, 17, 43–49. [Google Scholar]
- Tataryn, I.V.; Lomax, P.; Bajorek, J.G.; Chesarek, W.; Meldrum, D.R.; Judd, H.L. Postmenopausal hot flushes: A disorder of thermoregulation. Maturitas 1980, 2, 101–107. [Google Scholar]
- Molnar, G.W. Body temperatures during menopausal hot flashes. J. Appl. Physiol. 1975, 38, 499–503. [Google Scholar]
- Tankersley, C.G.; Nicholas, W.C.; Deaver, D.R.; Mikita, D.; Kenney, W.L. Estrogen replacement in middle-aged women: Thermoregulatory responses to exercise in the heat. J. Appl. Physiol. 1992, 73, 1238–1245. [Google Scholar]
- Putnam, L.L.; Bochantin, J. Gendered bodies: Negotiating normalcy and support. Negot. Confl. Manag. Res. 2009, 2, 57–73. [Google Scholar] [CrossRef]
- Reynolds, S.L. Protected or neglected: An examination of negative versus compassionate ageism in public conservatorship. Res. Aging 1997, 19, 3–25. [Google Scholar] [CrossRef]
- Bochantin, J. “Long live the mensi-mob”: Communicating support online with regards to experiencing menopause in the workplace. Commun. Stud. 2014, 65, 260–280. [Google Scholar] [CrossRef]
- New, K.; Gormally, A.; Friday, A.; Hazas, M. ‘We can send a man to the moon but we can’t control the temperature in our office’: A considerate approach to workplace thermal comfort by older women. In Proceedings of the 2021 CHI Conference on Human Factors in Computing Systems, Yokohama, Japan, 8–13 May 2021; pp. 1–14. [Google Scholar]
- CIBSE. CIBSE TM59 Design Methodology for the Assessment of Overheating Risk in Homes; Chartered Institute of Building Services Engineers: London, UK, 2017. [Google Scholar]
- ASHRAE. ANSI/ASHRAE Standard 55: Thermal Environmental Conditions for Human Occupancy; American Society of Heating, Refrigerating and Air-conditioning Engineers: Atlanta, GA, USA, 2013. [Google Scholar]
- Ma, T.; Xiong, J.; Lian, Z. A human thermoregulation model for the Chinese elderly. J. Therm. Biol. 2017, 70, 2–14. [Google Scholar] [CrossRef]
- WHO. Health impact of low indoor temperatures. In Health Impact of Low Indoor Temperatures; World Health Organization: Geneva, Switzerland, 1987; p. 27. [Google Scholar]
- Wookey, R.; Bone, A.; Carmichael, C.; Crossley, A. Minimum Home Temperature Thresholds for Health in Winter—A Systematic Iterature Review; Public Health England: London, UK, 2014.
- ISO7730; Ergonomics of the Thermal Environment—Analytical Determination and Interpretation of Thermal Comfort Using Calculation of the PMV and PPD Indices and Local Thermal Comfort Criteria. International Organization for Standardization: Geneva, Switzerland, 2005.
- Rawal, R.; Schweiker, M.; Kazanci, O.B.; Vardhan, V.; Jin, Q.; Duanmu, L. Personal comfort systems: A review on comfort, energy, and economics. Energy Build. 2020, 214, 109858. [Google Scholar] [CrossRef]
- Rijal, H.B.; Yoshida, K.; Humphreys, M.A.; Nicol, J.F. Development of an adaptive thermal comfort model for energy-saving building design in Japan. Archit. Sci. Rev. 2021, 64, 109–122. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Citation | Place/ Region | Age Range | Gender | Sample Size | Season | Context | Methodology | Indoor Air Temperature | Relative Humidity |
|---|---|---|---|---|---|---|---|---|---|
| Ohnaka et al. [3] | Japan | 63 to 73 | 8 females | 8 respondents | Not specified | Climatic chamber | Experiment | 35 °C hot; 10 °C cold; 25 °C moderate conditions | 60% ± 10% |
| Wong et al. [4] | Hong Kong | 25 to 93 (76 years mean) | 108 males and 332 females | 80 buildings; 579 respondents | Summer | Centres for older people and offices | Field study | 25.4 °C | 40–80% |
| Hwang and Chen [5] | Taiwan | 60+ | 37 males and 50 females | 87 respondents | Summer and winter | Houses; living room | Field study | 13.3–32.5 °C | 43–92% |
| Schellen et al. [6] | Eindhoven, Germany | Young adults (22 to 25) and older subjects (67 to 73) | 16 males | 16 respondents | Not specified | Experimental Chamber | Experiment | 21.5 °C; 17–25 °C; | 40% |
| Mendes et al. [7] | Porto, Portugal | Not specified | Not specified | 6 buildings; 425 respondents | Summer and winter | Elderly * Care Centres | Field study | 20 ± 1 °C | 50 ± 5% |
| Mendes et al. [8] | Porto, Portugal | Not specified | Not specified | 22 buildings | Summer and winter | Elderly * Care Centres | Field study | 20 ± 1 °C | 50 ± 5% |
| Bills [9] | Adelaide, Australia | 65+ | 4 males and 7 females | 10 buildings; 11 respondents | Summer and winter | Residential buildings | Field study | 18–35 °C operative temperature | 25–70% |
| Bills et al. [10] | Adelaide, Australia | Not specified | 9 males and 8 females | 15 buildings; 17 respondents | October to January | Houses | Field study | 18–35 °C operative temperature | 25–70% |
| Yang et al. [11] | Republic of Korea | 65+ | 64 males and 334 females | 26 buildings; 308 respondents | 1 year | Elderly * Care Centres | Field study | 21.3–31.3 °C | 17–87.2% |
| Jiao et al. [12] | China | 70+ (85.2 average) | Not specified | 42 buildings; 672 respondents | Summer and winter | Nursing homes | Field study | 6.4–32.5 °C | 20.6–83.2% |
| Fan et al. [13] | Beijing, China | 65+ (73.9 ± 5.8 for urban and 72.0 ± 6.7 for rural respondents) | Not specified | 100 buildings and 100 responses | Winter | Houses: urban and rural houses | Field study | 14.6 ± 3.3–21.9 ± 2.2 °C | 23–67% |
| Vellei et al. [14] | Exeter UK | 65 + | Not specified | 55 dwellings; 70 survey responses; 20 interviews | Summer | Dwellings: Houses and Flats | Field study | 22.2–24.1 °C | - |
| Panraluk and Sreshthaputra [15] | Thailand | 55+ | Not specified | 4 buildings; 163 respondents | November and March | Public health service buildings | Field study | 23–27.8 °C | 54–73% |
| Hughes et al. [16] | UK | 65+ | Not specified | 43 buildings; 59 respondents; 266 responses | Winter | Houses pre-1919 | Field study | 17.6–18.9 °C mean | 50.37–51.59% mean |
| Xiong et al. [17] | Shanghai, China | 70+ | 8 males and 8 females | 16 respondents | Summer | Climatic chamber | Experiment | 21–31 °C operative temperature | 30–70% |
| Lan et al. [18] | Shanghai, China | 65+ (71 ± 5) | 10 males and 8 females | 18 respondents | Summer | Sleep chamber | Experiment | 26.7 ± 0.2–29.8 ± 0.2 °C | 55 ± 7–61 ± 5% |
| Forcada et al. [19] | Mediterranean climate | 84.4 (46 to 99) | 156 males and 467 females | 623 respondents | Summer | Nursing homes | Field study | 23.14–28.46 °C | 52.38–69.32% |
| Yu et al. [20] | China | 12% 60 to 70: 33% 71 to 80; 48% 81 to 90; and 7% over 90 | 40% males and 60% females | 2 buildings; 60 respondents; 720 responses | 1 year | Nursing homes | Field study | 5.1–34.3 °C | 12.3–99.9% |
| Forcada et al. [21] | Spain | Not specified | Not specified | 5 buildings | Feb to Nov | Nursing homes | Field study | 19.7–28.5 °C | 57.1–84% |
| Larriva et al. [22] | Mediterranean climate | Not specified | Not specified | 18 buildings; 2690 responses | Natural ventilation season | Nursing homes | Field study | 18.2–28.8 °C | 0–96% |
| Yao et al. [23] | Lhasa, Tibet | 60+ | Males and females | 468 responses | Summer and winter | Outdoors | Field study | N/A | N/A |
| Yuan et al. [24] | China | 60+ | 73 males and 79 females | 62 buildings; 152 respondents | Winter | Rural residential buildings | Field study and simulation | 23.7–27.9 °C | 60–83% |
| Li et al. [25] | Mongolia | 60 to 93 | 45.45% males and 54.55% females | 16 buildings; 216 respondents | December | Mutual aid homes | Field study | 7.2–19.5 °C | 30.10% |
| Zheng et al. [26] | China | 60+ | Not specified | 2 buildings; 29 respondents | 1 year | Nursing homes | Field study | 9.9–35.4 °C | 12–90% |
| Kainaga et al. [27] | Nagano Prefecture, Japan | 65+ (83.7 average) | 27 males and 39 females | 1 building; 10,017 responses | Summer and winter | Elderly * care facility | Field study | 17.4–27.6 °C | 15–83% |
| Zheng et al. [28] | Baoding, China | 60 to 74; 75 to 88; and 89+ | Not specified | 2 buildings; 29 respondents | Summer | Pensioners buildings | Field study | 20.1–39.3 °C | 20.8–97% |
| Jiao et al. [29] | Shanghai, China | 70+ | 233 males and 439 females | 17 buildings; 742 respondents | Summer and winter | Elderly * Care Institutions | Field study | 6–32.5 °C | 25–80% |
| Zong et al. [30] | China | 82 years average | 161 males and 321 females | 1 building; 482 respondents | All year | Nursing Home | Field study | 11.92 ± 1.1–28.58 ± 1.1 °C | 58.77 ± 10.6–74.41 ± 4.8% |
| Yoon et al. [31] | UK | 60 to 101 | Not specified | 15 buildings; 69 respondents | Summer | Care homes | Field study | 21.5–26.5 °C | - |
| Baquero et al. [32] | Spain, Madrid Region | 65+ (87.3%) | 22% males and 78% females | 5 buildings; 1232 respondents; 1412 responses | Summer | Nursing Homes; Common areas | Field study | 28.02–24.95 °C | 16.9–83.7% |
| Citation | Place | Age Range | Gender | Sample Size | Season | Context | Methodology |
|---|---|---|---|---|---|---|---|
| Raymann and Van Someren [34] | The Netherlands | 65.8 ± 2.8 and 59.1 ± 1.9 | 8 males and 8 females | 16 | Not specified | Sleep chamber | Experiment |
| Okamoto-Mizuno and Tsuzuki [35] | Japan | 62+ (65.8 ± 2.6) | 13 males and 6 females | 19 | Winter, Summer and Autumn | Residential own bedroom | Field study |
| Tsuzuki et al. [36] | Japan | 60+ (64 ± 1) | 8 males | 8 | All year | Residential own bedroom | Field study |
| Lan et al. [18] | China | 65+ (71 ± 5) | 10 males and 8 females | 18 | Summer | Sleep chamber | Experiment |
| Xia et al. [37] | China | 66.3 ± 3.3 | 8 males and 4 females | 12 | Winter | Nursing home | Field experiments |
| Tsuzuki et al. [38] | Japan | 70+ (80 ± 5) | 8 males and 8 females | 16 | All year | Care facilities | Field study |
| Kido et al. [39] | Japan | 60+ (74.8 ± 10.3) | 37 males and 49 females | 97, including 86 older people | Summer | Residential own bedroom | Field study |
| Yan et al. [40] | China | 65+ (70.7.3 ± 5) | 19 males and 26 females | 45 | Summer | Own bedroom (not specified home vs. care home) | Field study |
| Yan et al. [41] | China | 65+ (72 ± 6) | 8 males and 8 females | 16 | Summer | Sleep chamber | Experiment |
| Age Range (years) | Research Paper | Age Range (years) | Research Paper |
|---|---|---|---|
| 25 to 93 | Wong et al. [4] | 65+ | Vellei M et al. [14] |
| 46+ | Forcada et al. [19] | Hughes et al. [16] | |
| 55+ | Panraluk and Sreshthaputra [15] | Lan et al. [18] | |
| 60+ | Hwang and Chen [5] | Kainaga et al. [27] | |
| Yu et al. [20] | Baquero et al. [32] | ||
| Yao et al. [23] | 67+ | Schellen et al. [6] | |
| Yuan et al. [24] | 70+ | Jiao et al. [12] | |
| Li et al. [25] | Xiong et al. [17] | ||
| Zheng et al. [26] | |||
| Zheng et al. [28] | Not specified | Mendes et al. [7] | |
| Yoon et al. [31] | Mendes et al. [8] | ||
| 63–73 | Ohnaka et al. [3] | Bills et al. [10] | |
| 65+ | Bills [9] | Forcada et al. [21] | |
| Yang et al. [11] | Larriva et al. [22] | ||
| Fan et al. [13] | Zong et al. [30] |
| Health Impacts of Heat Exposure | |||
|---|---|---|---|
| Direct | Indirect | ||
| Heat Illness | Dehydration | Health services | Increased ambulance call outs |
| Heat cramps | Response time | ||
| Heat stroke | Hospital admissions | ||
| Accelerated death | Respiratory disease | Storage of medicine | |
| Cardiovascular disease | Accidents risk | Drowning | |
| Other chronic disease (mental health) | Injuries and poisonings | ||
| Hospitalisation | Respiratory disease | Work related | |
| Diabetes mellitus | Transmission | Food and waterborne diseases | |
| Renal disease | |||
| Stroke | Marine algal blooms | ||
| Mental health conditions | Infrastructure disruptions | Power | |
| Water | |||
| Transportation | |||
| Productivity | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shahzad, S.; Gomez Torres, S.; Rijal, H.B.; Nicol, F. Lack of Thermal Comfort Is a Matter of Life and Death: A Systematic Review for Older People. Buildings 2025, 15, 1141. https://doi.org/10.3390/buildings15071141
Shahzad S, Gomez Torres S, Rijal HB, Nicol F. Lack of Thermal Comfort Is a Matter of Life and Death: A Systematic Review for Older People. Buildings. 2025; 15(7):1141. https://doi.org/10.3390/buildings15071141
Chicago/Turabian StyleShahzad, Sally, Sergio Gomez Torres, Hom B. Rijal, and Fergus Nicol. 2025. "Lack of Thermal Comfort Is a Matter of Life and Death: A Systematic Review for Older People" Buildings 15, no. 7: 1141. https://doi.org/10.3390/buildings15071141
APA StyleShahzad, S., Gomez Torres, S., Rijal, H. B., & Nicol, F. (2025). Lack of Thermal Comfort Is a Matter of Life and Death: A Systematic Review for Older People. Buildings, 15(7), 1141. https://doi.org/10.3390/buildings15071141