
Study on the Spatial Coupling Coordination of Public Service Facilities Around Large Comprehensive Hospitals in Beijing from a Supply–Demand Perspective

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Research Domain
2.2. Methods
2.2.1. Supply and Demand Coupling Coordination Degree Model
2.2.2. Selection of Evaluation Indicators
2.2.3. AHP to Determine Indicator Weights
- (1)
- Constructing a judgment matrix
- (2)
- Calculating the weight vector and the largest characteristic root
- (3)
- Consistency test
2.2.4. Data Sources and Processing Methods
2.2.5. Evaluation of SDCCD Model
3. SDCCD Experimental Process
3.1. Experimental Data Acquisition
- (1)
- Hospital data
- (2)
- Population and settlement data
- (3)
- Other data
3.2. Calculation of Indicators by Classification
- (1)
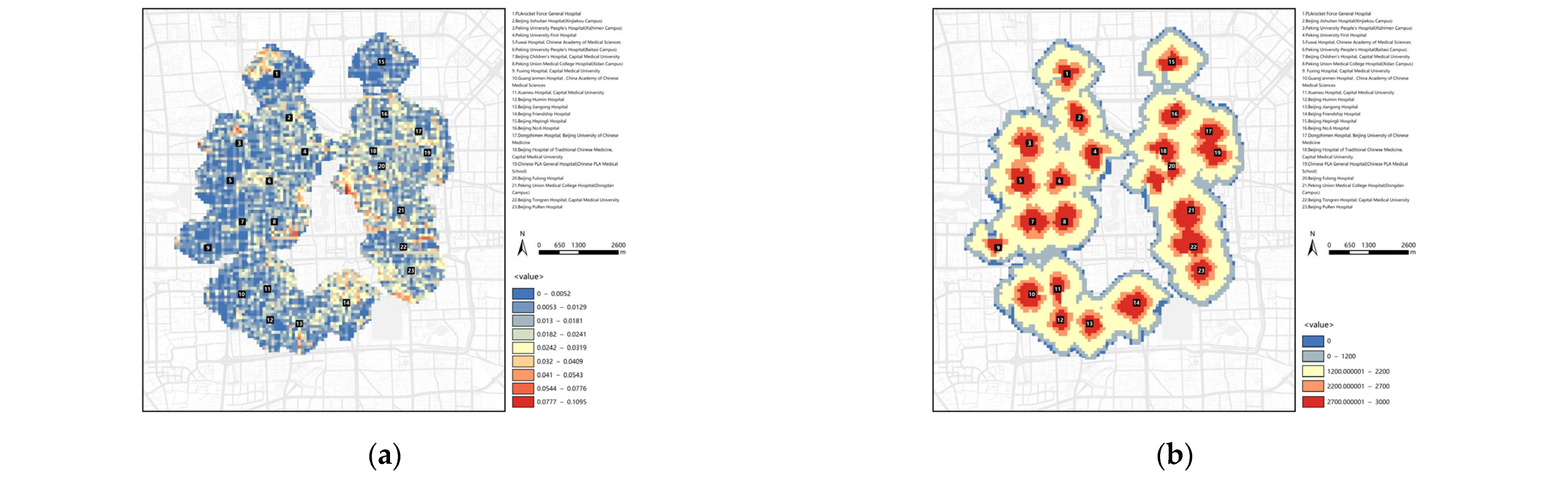
- Information on the Data of Each Indicator Under the Demand Thrust of the Population
- (2)
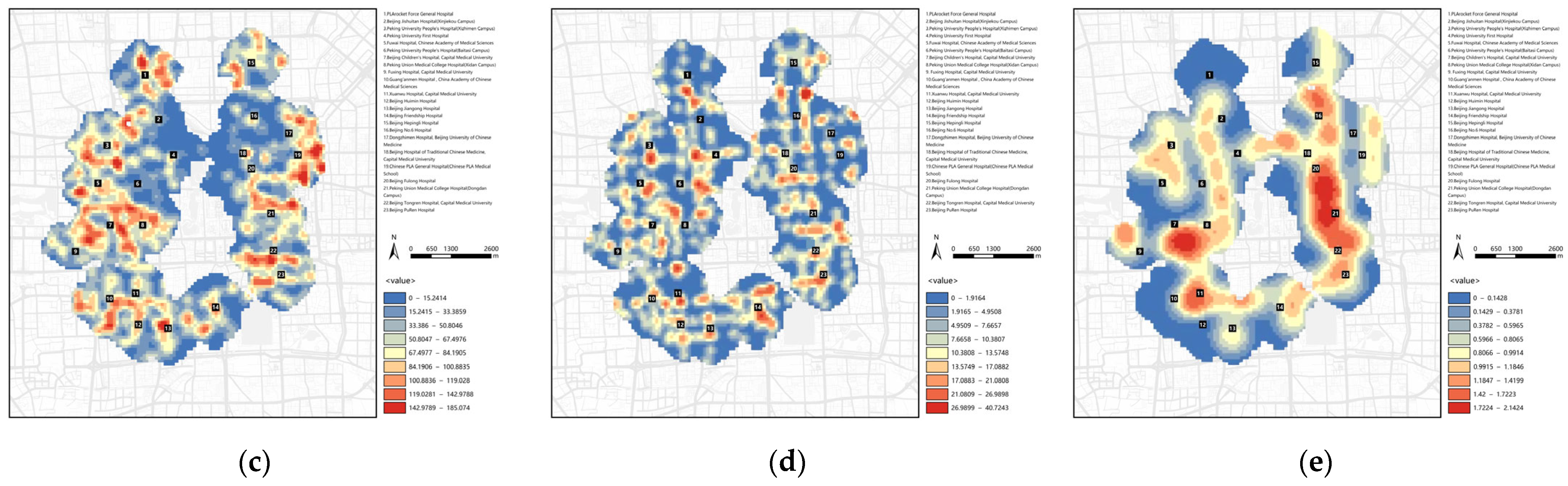
- Information on the Data of Indicators Under the Pull of Space Supply of Facilities
- (3)
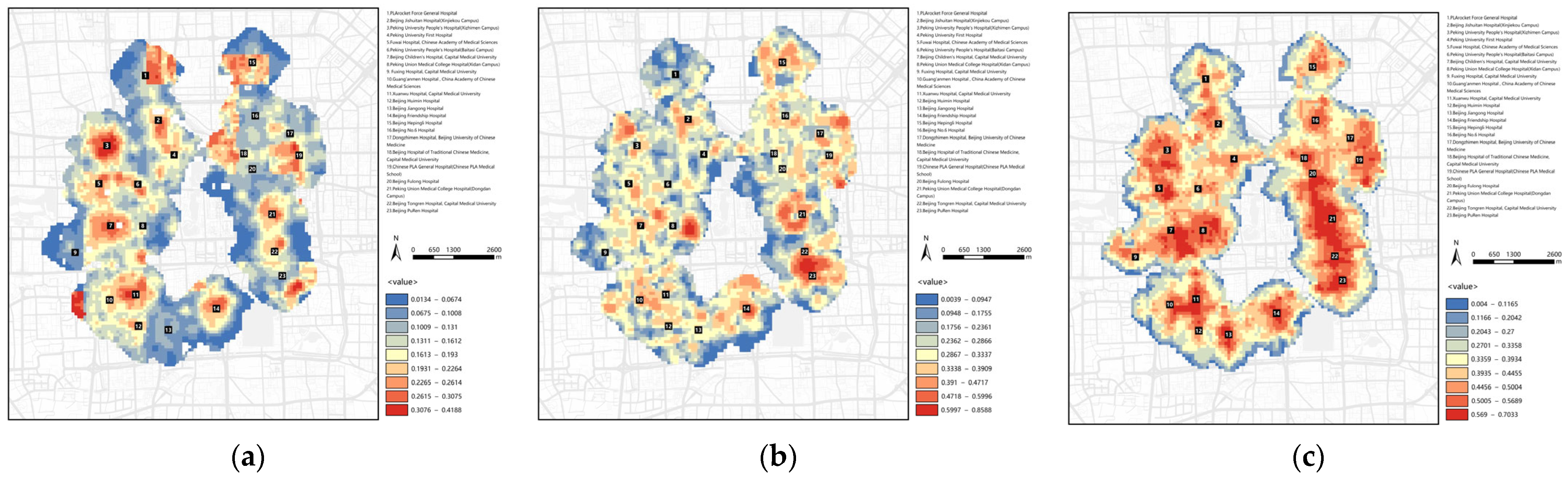
- Information on the Data for Indicators of the Effectiveness of Transportation Links
3.3. Calculation of the Overall Indicator Score
4. Analysis of Results
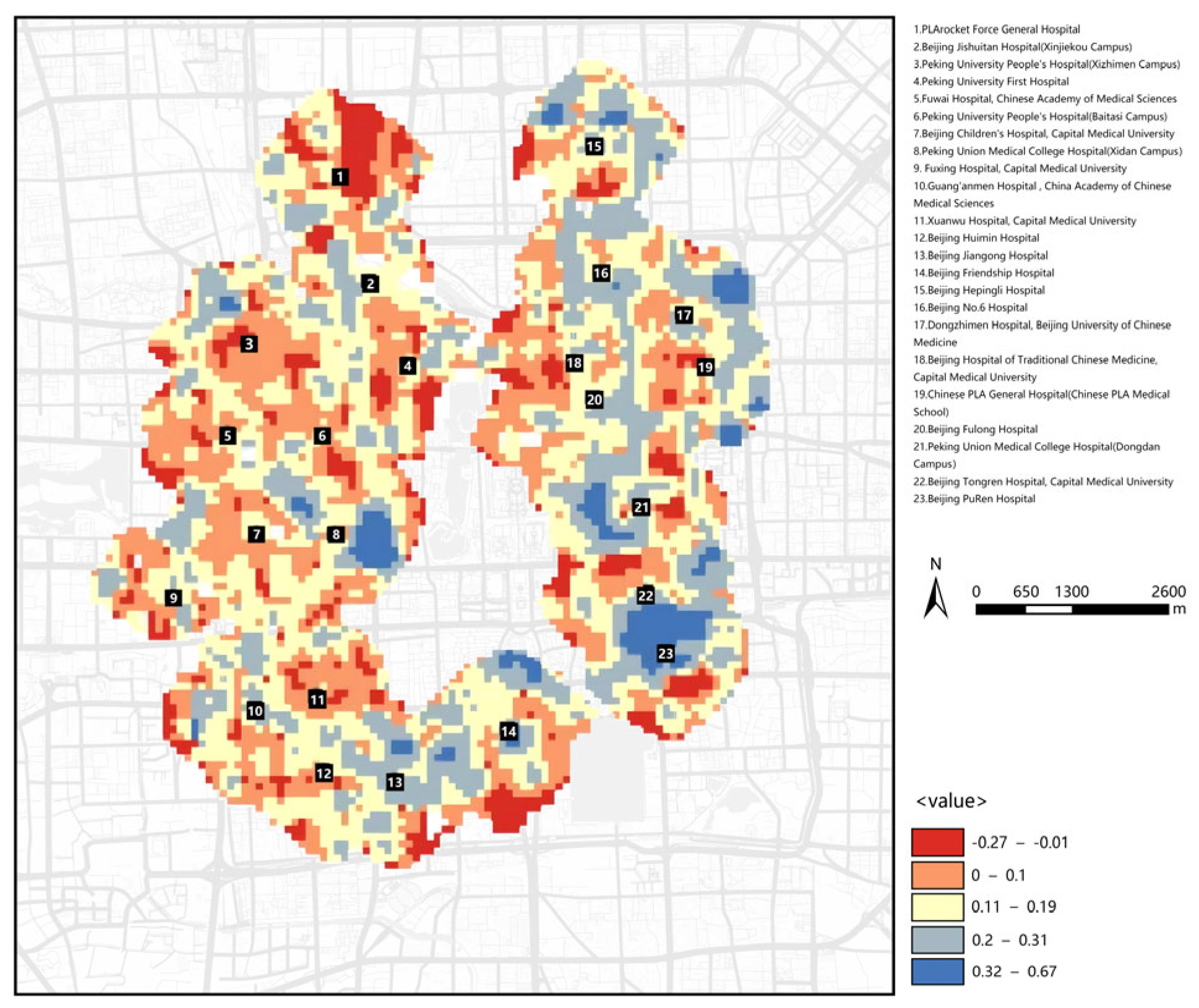
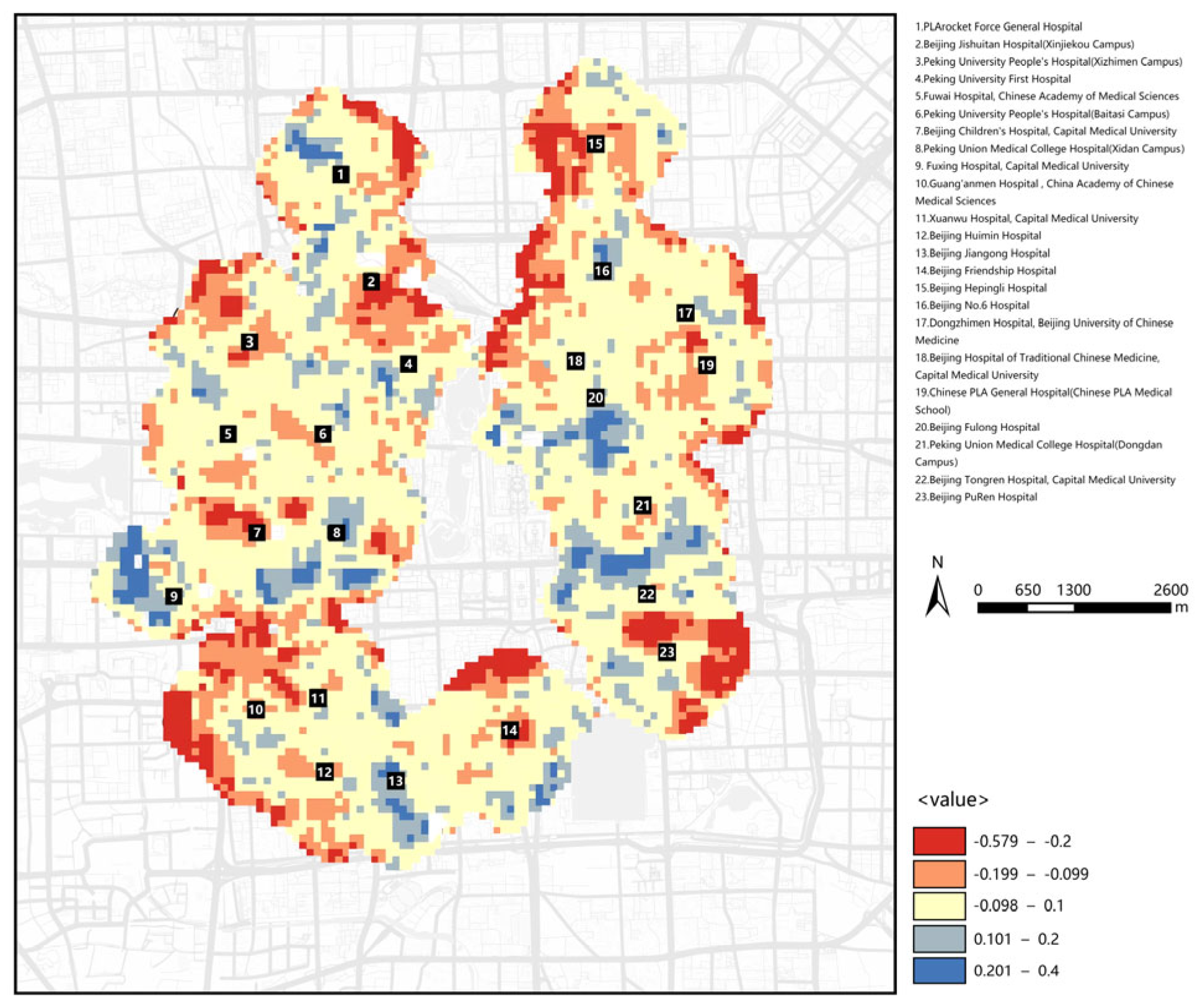
4.1. Supply and Demand Matching Analysis
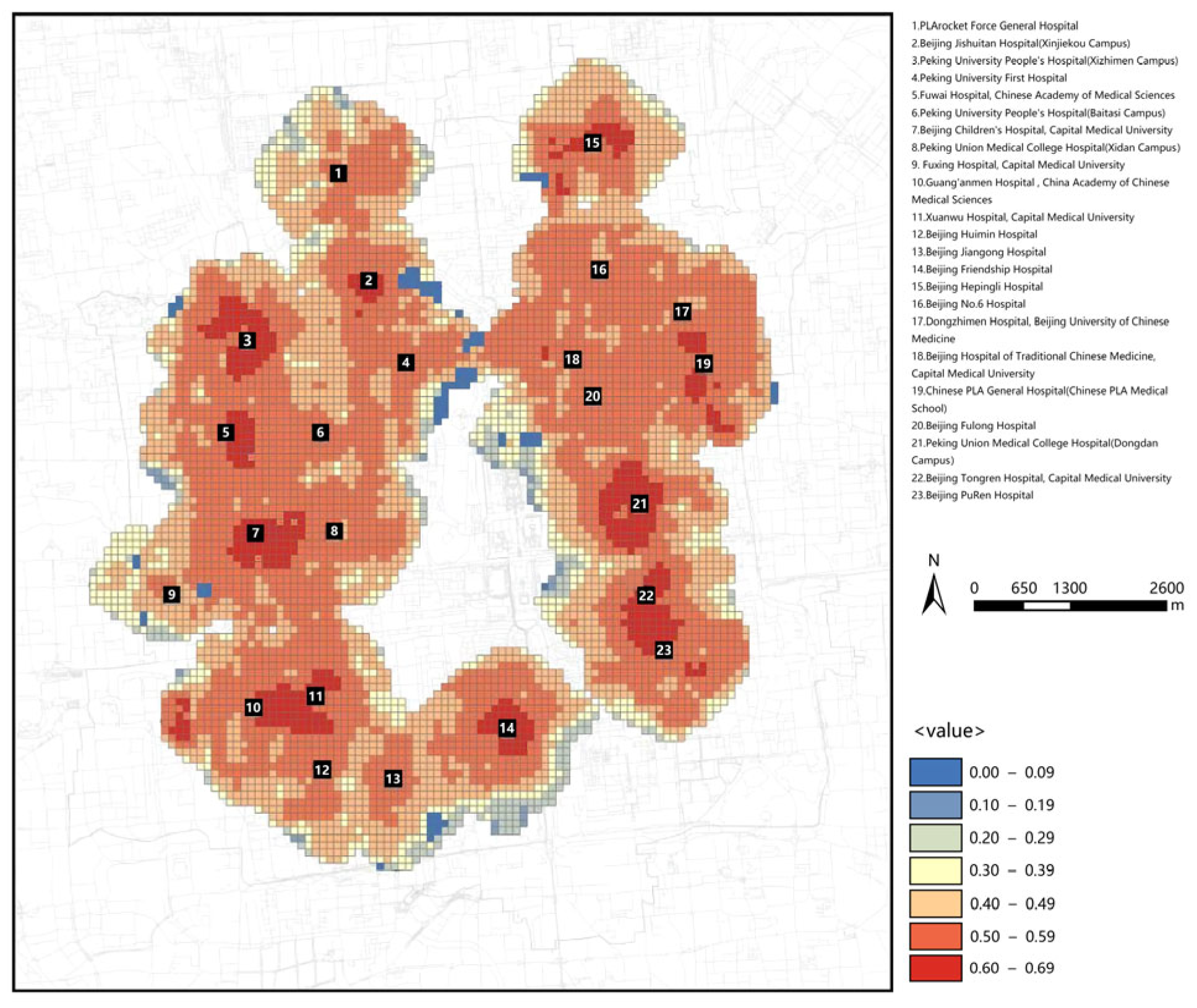
4.2. Transport Development Matching Analysis
4.3. Coupling Level Results Analysis
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zabala, F.J.; Zapata, V.Y.; Martina, M.A.; Gonzalez, A.M.; Eugenia, M.; Vargas, V.J. Urban Agriculture: As A Transformation Strategy For Social Construction And Improvement Of The Quality Of Life In Vulnerable Communities In The Urban Area. WSEAS Trans. Environ. Dev. 2018, 14, 674–687. [Google Scholar]
- Kormina, A.A. Combined effects of the living environment on the well-being of the city population. Urban Constr. Archit. 2021, 11, 128–137. [Google Scholar] [CrossRef]
- Wenqiang, W. People’s Survival and Development in the Urban Public Construction—From the Perspective of the Relationship Between Human Development and Economic Development. Reform. Strategy 2013. [Google Scholar]
- Sun, C.; Chen, L.; Tian, Y.J.E.I. Study on the urban state carrying capacity for unbalanced sustainable development regions: Evidence from the Yangtze River Economic Belt. Ecol. Indic. Integr. Monit. Assess. Manag. 2018, 89, 150–158. [Google Scholar] [CrossRef]
- Xiong, G.; Cao, X.; Hamm, N.A.S.; Lin, T.; Zhang, G.; Chen, B.J.S. Unbalanced Development Characteristics and Driving Mechanisms of Regional Urban Spatial form: A Case Study of Jiangsu Province, China. Sustainability 2021, 13, 3121. [Google Scholar] [CrossRef]
- Carmon, N.; Fainstein, S.S. Introduction: Policy, Planning, and People. In Policy, Planning, and People (Promoting Justice in Urban Development); University of Pennsylvania Press: Philadelphia, PA, USA, 2013; pp. 1–10. [Google Scholar]
- Qiao, Z.; Xu, X.; Wu, F.; Luo, W.; Wang, F.; Liu, L.; Sun, Z. Urban ventilation network model: A case study of the core zone of capital function in Beijing metropolitan area. J. Clean. Prod. 2017, 168, 526–535. [Google Scholar] [CrossRef]
- Zhao, L.; Tang, X.; Xing, X.; Cai, C. Big Data Analysis of Park and Green Space Serviceability for Elderly Population-Case Study of Core Area of Beijing. Sens. Mater. Int. J. Sens. Technol. 2022, 34, 4369–4380. [Google Scholar] [CrossRef]
- Zhang, H.; Tang, H.; Zhang, A. Study on the Characteristics and Formation Mechanism of Residential Space Division in the Core Area of Capital Functions of Beijing. Urban Dev. Stud. 2019, 26, 98–106. [Google Scholar]
- Wei, G. Research on international medical service model of large comprehensive Class A tertiary hospitals. Chin. J. Med. Educ. Res. 2018, 17, 321–324. [Google Scholar] [CrossRef]
- Gupta, D.; Potthoff, S.J.J.F.; Information, T.i.T.; Management, O. Matching Supply and Demand for Hospital Services. Found. Trends Technol. Inf. Oper. Manag. 2016, 8, 131–274. [Google Scholar] [CrossRef]
- Zhang, J.; Tan, P.Y. Assessment of spatial equity of urban park distribution from the perspective of supply-demand interactions. Urban For. Urban Green. 2023, 80, 127827. [Google Scholar] [CrossRef]
- McLeod, S. Maslow’s hierarchy of needs. SimplyPsychology 2007, 1, 1–18. [Google Scholar]
- Simons, J.A.; Irwin, D.B.; Drinnien, B.A. Maslow’s hierarchy of needs. Salenger Inc. 1987, 9, 222. [Google Scholar]
- Tian-Yi, Z.; Management, S.O. Analyses on supply side in the field of medical health care helped by healthy big data. Chin. J. Urban Rural Enterp. Hyg. 2017. [Google Scholar]
- Samat, N.; Shattar, A.K.A. Spatial Accessibility of Colorectal Cancer Patients to Health Care Facilities in Kelantan State: A Study on Medical Geography. World Appl. Sci. J. 2014, 31, 1772–1782. [Google Scholar]
- Jin, M.; Liu, L.; Tong, D.; Gong, Y.; Liu, Y. Evaluating the Spatial Accessibility and Distribution Balance of Multi-Level Medical Service Facilities. Int. J. Environ. Res. Public Health 2019, 16, 1150. [Google Scholar] [CrossRef]
- Cho, C.J. An equity-efficiency trade-off model for the optimum location of medical care facilities. Socio-Econ. Plan. Sci. 1998, 32, 99–112. [Google Scholar] [CrossRef]
- Lee, S.J.; Youn, K.H. A Study on the Convergence of Spatial Equity of Medical Welfare Facilities for Older Persons and Services. J. Internet Things Converg. 2020, 6, 65–72. [Google Scholar]
- Rong, P.; Zheng, Z.; Kwan, M.P.; Qin, Y. Evaluation of the spatial equity of medical facilities based on improved potential model and map service API: A case study in Zhengzhou, China. Appl. Geogr. 2020, 119, 102192. [Google Scholar] [CrossRef]
- Ni, J.H.; Qian, T.L.; Xi, C.B.; Rui, Y.K.; Wang, J.C. Spatial Distribution Characteristics of Healthcare Facilities in Nanjing: Network Point Pattern Analysis and Correlation Analysis. Int. J. Environ. Res. Public Health 2016, 13, 833. [Google Scholar] [CrossRef]
- Shan, X.; Xu, J.; Du, Y.; Wang, R.; Deng, H. Spatial Distribution Characteristics and Optimization Strategies of Medical Facilities in Kunming Based on POI Data. In Proceedings of the The 10th International Conference on Computer Engineering and Networks, Xi′an, China, 16–18 October 2020; Springer: Singapore, 2021. [Google Scholar]
- Yin, C.; He, Q.; Liu, Y.; Chen, W.; Gao, Y. Inequality of public health and its role in spatial accessibility to medical facilities in China. Appl. Geogr. 2018, 92, 50–62. [Google Scholar] [CrossRef]
- Qiqi, H.; Kaitai, Y.A. Spatial Distribution Characteristics and Coverage Rate of Commercial Facilities in 15-minute Radius Livelihood Service Circles of Chunshu Street. J. Landsc. Res. 2024, 16, 17–21. [Google Scholar]
- Wang, Y.; Wu, C. Research on the spatial distribution and accessibility of medical institutions in Wuhan based on GIS. IOP Conf. Ser. Earth Environ. Sci. 2021, 825, 012028. [Google Scholar] [CrossRef]
- Xu, X.; Hu, J.; Lv, L.; Yin, J.; Tian, X. Research on the Matching Relationship between the Supply of Urban Ecological Recreational Space and the Demand of Residents-A Case Study of an Urban Development Area in Wuhan. Int. J. Environ. Res. Public Health 2022, 19, 816. [Google Scholar] [CrossRef] [PubMed]
- Song, L.; Kong, X.; Cheng, P. Supply-demand matching assessment of the public service facilities in 15-minute community life circle based on residents’ behaviors. Cities 2024, 144, 1.1–1.15. [Google Scholar] [CrossRef]
- Zhan, D.S.; Zhang, W.Z.; Yu, J.H.; Dang, Y.X.; Li, X.Y. Application of questionnaire survey method in human geography studies in China. Acta Geogr. 2016, 71, 899–913. [Google Scholar]
- Royo, E.; Li, Y.; Komatsu, T. Factors influencing common space use among the elderly in chinese urban residential areas: Based on the results of a questionnaire survey conducted in three communities in zhengzhou city. J. Archit. Plan. (Trans. AIJ) 2023, 88, 424–435. [Google Scholar] [CrossRef]
- Formica, S.; Uysal, M. Destination Attractiveness Based on Supply and Demand Evaluations: An Analytical Framework. J. Travel Res. 2006, 44, 418–430. [Google Scholar] [CrossRef]
- Fang, Z. Optimization of Medical Service Facilities Allocation in Small Towns of Wuhan City from the Perspective of Supply and Demand. Master’s Thesis, Huazhong University of Science and Technology: Wuhan, China, 2017. [Google Scholar]
- Medical Xpress. Just Half of Acute Hospital Trusts in England Have Chaperone Policy. Available online: https://medicalxpress.com/news/2010-08-hospital-england-chaperon-policy.html (accessed on 6 April 2025).
- Kwon, S.; Joo, S. A Study on the proportion of functional Areas in the ward of General Hospitals. J. Korea Inst. Healthc. Archit. 2011, 17, 49–55. [Google Scholar] [CrossRef]
- How the ‘15-Minute City’ Could Help Post-Pandemic Recovery. Available online: https://www.tbsnews.net/world/global-economy/how-15-minute-city-could-help-post-pandemic-recovery-108403 (accessed on 15 July 2020).
- Xiao, Z.; Chai, Y.; Zhang, Y. Overseas Life Circle Planning And Practice. Planners 2014, 30, 89–95. [Google Scholar]
- Shanghai Urban Planning and Land Resources Administration Bureau. Land Resources Administration Bureau: Shanghai, C. Planning Guidance of 15-Minute Community-Life Circle; Shanghai Urban Planning and Land Resources Administration Bureau: Shanghai, China, 2016. [Google Scholar]
- Fan, L.H.; Lin, X.Q.; Wang, D. Spatial-temporal succession characteristics of public service facilities supply and demand coordinated development in beijing: A case study of educational and medical facilities. Hum. Geogr. 2015, 30, 90–97. [Google Scholar]
- Zhang, L.; Zhang, M.; Yuan, M.; Guo, Y. A Study on the Regional Evolution of the Hefei Political and Cultural New District Skyline Based on Exploratory Factor Analysis and Semantic Segmentation. Buildings 2024, 14, 1238. [Google Scholar] [CrossRef]
- Yu, Z.; Zhou, Y.; Wang, H. Walking Environment Satisfaction in an Historic Block Based on POE and Machine Learning: A Case Study of Tianjin Five Avenues. Buildings 2024, 14, 3047. [Google Scholar] [CrossRef]
- Kerez, C. Christian Kerez, Beijing Central Business District Core Area, Culture Center. In International 2015; A.D.A. Edita: Tokyo, Japan, 2015. [Google Scholar]
- Wu, H.; Wang, L.; Zhang, Z.; Gao, J. Analysis and optimization of 15-minute community life circle based on supply and demand matching: A case study of Shanghai. PLoS ONE 2021, 16, e0256904. [Google Scholar] [CrossRef]
- Yang, Y.; Qian, Y.; Zeng, J.; Wei, X.; Yang, M. Walkability measurement of 15-minute community life circle in Shanghai. Land 2023, 12, 153. [Google Scholar] [CrossRef]
- Mousakazemi, M.S. Urban sustainable development: Concepts and perspectives. Geogr. Res. 2001, 94–113. [Google Scholar]
- Jian-Sheng, L. The Influence of the Positioning of Beijing’s General Urban Planning on the Construction of a National Cultural Center. J. Beijing Union Univ. (Humanit. Soc. Sci.) 2015. [Google Scholar]
- Saaty, T.L. The Analytic Hierarchy Process. Appl. Stud. 2001, 1, 1073–1076. [Google Scholar]
- Jing, W.; Yaofeng, M.; Tourism, D.O.; Amp, S.V. The Comparative Study of Coupling Coordination Degree of Tourism Industry and Urbanization of the Eastern City and the Western City. Tour. Forum 2014. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Primary Indicators | Secondary Indicators | Tertiary Indicators |
|---|---|---|
| A Crowd demand push | A1 Population characteristics | A11 Population density |
| A12 Percentage of children and older persons data | ||
| A13 Demand for medical treatment | ||
| A2 Economic characteristics | A21 Level of per capita consumption | |
| B Facility supply pull | B1 Public service facilities | B11 Diversity of business |
| B12 Facility service coverage | ||
| B13 Density of various facilities | ||
| B2 Activity facilities | B21Activity space density | |
| B22 Service coverage | ||
| B3 Service level | B31 Facility satisfaction | |
| C Transport link effectiveness | C1 Transport capacity | C11 Road network density |
| C12 Road network accessibility | ||
| C2 Static transport | C21 Parking density | |
| C3 Transport facilities | C31 Density of underground stations | |
| C32 Density of bus stations |
| Scale | Definition Description |
|---|---|
| 1 | Both indicators are of equal importance |
| 3 | One factor is slightly more important than the other |
| 5 | One factor is clearly more important than the other |
| 7 | One factor is more strongly more important than the other |
| 9 | One factor is extremely more important than the other |
| 2, 4, 6, 8 | The middle value of the two adjacent judgments above |
| n | 1 | 2 | 3 | 4 | … |
|---|---|---|---|---|---|
| RI | 0 | 0 | 0.52 | 0.89 | … |
| Primary Indicators | Weight | Secondary Indicators | Weight | Tertiary Indicators | Weight |
|---|---|---|---|---|---|
| A | 1 | A1 | 0.76 | A11 | 0.37 |
| A12 | 0.16 | ||||
| A13 | 0.23 | ||||
| A2 | 0.24 | A21 | 0.24 | ||
| B | 1 | B1 | 0.59 | B11 | 0.25 |
| B12 | 0.23 | ||||
| B13 | 0.11 | ||||
| B2 | 0.20 | B21 | 0.10 | ||
| B22 | 0.10 | ||||
| B3 | 0.21 | B31 | 0.21 | ||
| C | 1 | C1 | 0.50 | C11 | 0.17 |
| C12 | 0.33 | ||||
| C2 | 0.20 | C21 | 0.20 | ||
| C3 | 0.30 | C31 | 0.22 | ||
| C32 | 0.08 |
| Degree of Coupling Coordination | Level of Coordination | Degree of Coupling Coordination | Level of Coordination |
|---|---|---|---|
| 0.90–1.00 | quality coordination | 0.40–0.49 | on the verge of dissonance |
| 0.80–0.89 | well-coordinated | 0.30–0.39 | mild disorder |
| 0.70–0.79 | mid-level coordination | 0.20–0.29 | moderate disorder |
| 0.60–0.69 | primary coordination | 0.10–0.19 | severe disorder |
| 0.50–0.59 | sue for coordination | 0.00–0.09 | extreme disorder |
| Number | Hospital Name |
|---|---|
| 1 | PLArocket Force General Hospital |
| 2 | Beijing Jishuitan Hospital (Xinjiekou Campus) |
| 3 | Peking University People’s Hospital (Xizhimen Campus) |
| 4 | Peking University First Hospital |
| 5 | Fuwai Hospital, Chinese Academy of Medical Sciences |
| 6 | Peking University People’s Hospital (Baitasi Campus) |
| 7 | Beijing Children’s Hospital, Capital Medical University |
| 8 | Peking Union Medical College Hospital (Xidan Campus) |
| 9 | Fuxing Hospital, Capital Medical University |
| 10 | Guang’anmen Hospital, China Academy of Chinese Medical Sciences |
| 11 | Xuanwu Hospital, Capital Medical University |
| 12 | Beijing Huimin Hospital |
| 13 | Beijing Jiangong Hospital |
| 14 | Beijing Friendship Hospital |
| 15 | Beijing Hepingli Hospital |
| 16 | Beijing No.6 Hospital |
| 17 | Dongzhimen Hospital, Beijing University of Chinese Medicine |
| 18 | Beijing Hospital of Traditional Chinese Medicine, Capital Medical University |
| 19 | Chinese PLA General Hospital (Chinese PLA Medical Shool) |
| 20 | Beijing Fulong Hospital |
| 21 | Peking Union Medical College Hospital (Dongdan Campus) |
| 22 | Beijing Tongren Hospital, Capital Medical University |
| 23 | Beijing PuRen Hospital |
| Hospital | Average Number of Consultations per Day (Number) | Hospital | Average Number of Consultations Everyday (Number) |
|---|---|---|---|
| 1 | 2600 | 13 | 1377 |
| 2 | 1200 | 14 | 10,000 |
| 3 | 10,000 | 15 | 1030 |
| 4 | 4000 | 16 | 1096 |
| 5 | 2711 | 17 | 1600 |
| 6 | - | 18 | 3000 |
| 7 | 10,000 | 19 | 4500 |
| 8 | 1200 | 20 | 800 |
| 9 | 1700 | 21 | 11,000 |
| 10 | 4288 | 22 | 5000 |
| 11 | 7600 | 23 | 1000 |
| 12 | 1800 |
| Hospital | Us | Ud | Uc | SD Level (Us − Ud) | SD Characteristics |
|---|---|---|---|---|---|
| 1 | 0.265 | 0.178 | 0.443 | −0.087 | supply and demand match |
| 2 | 0.265 | 0.312 | 0.454 | 0.047 | supply and demand match |
| 3 | 0.412 | 0.305 | 0.528 | −0.107 | supply lagging |
| 4 | 0.179 | 0.270 | 0.500 | 0.091 | supply and demand match |
| 5 | 0.255 | 0.306 | 0.620 | 0.051 | supply and demand match |
| 6 | 0.211 | 0.246 | 0.440 | 0.035 | supply and demand match |
| 7 | 0.402 | 0.413 | 0.570 | 0.011 | supply and demand match |
| 8 | 0.136 | 0.241 | 0.500 | 0.105 | supply ahead |
| 9 | 0.095 | 0.228 | 0.496 | 0.133 | supply ahead |
| 10 | 0.181 | 0.436 | 0.496 | 0.255 | supply ahead |
| 11 | 0.416 | 0.278 | 0.650 | −0.138 | supply lagging |
| 12 | 0.221 | 0.289 | 0.457 | 0.068 | supply and demand match |
| 13 | 0.101 | 0.303 | 0.531 | 0.201 | supply ahead |
| 14 | 0.223 | 0.620 | 0.612 | 0.397 | supply ahead |
| 15 | 0.214 | 0.394 | 0.412 | 0.180 | supply ahead |
| 16 | 0.119 | 0.291 | 0.521 | 0.172 | supply ahead |
| 17 | 0.144 | 0.300 | 0.468 | 0.156 | supply ahead |
| 18 | 0.178 | 0.278 | 0.554 | 0.100 | supply and demand match |
| 19 | 0.328 | 0.288 | 0.503 | −0.040 | supply and demand match |
| 20 | 0.100 | 0.288 | 0.578 | 0.188 | supply ahead |
| 21 | 0.232 | 0.450 | 0.694 | 0.218 | supply ahead |
| 22 | 0.256 | 0.345 | 0.563 | 0.089 | supply and demand match |
| 23 | 0.135 | 0.502 | 0.700 | 0.367 | supply ahead |
| Hospital | Us | Ud | Uc | Level of Coordinated Transport Development [Us − (Ud + Uc)] | Degree of Transport Coordination |
|---|---|---|---|---|---|
| 1 | 0.265 | 0.178 | 0.443 | 0.000 | synchronous |
| 2 | 0.265 | 0.312 | 0.454 | −0.123 | lagging |
| 3 | 0.412 | 0.305 | 0.528 | −0.189 | lagging |
| 4 | 0.179 | 0.270 | 0.500 | 0.051 | synchronous |
| 5 | 0.255 | 0.306 | 0.620 | 0.059 | synchronous |
| 6 | 0.211 | 0.246 | 0.440 | −0.017 | synchronous |
| 7 | 0.402 | 0.413 | 0.570 | −0.245 | lagging |
| 8 | 0.136 | 0.241 | 0.500 | 0.123 | ahead |
| 9 | 0.095 | 0.228 | 0.496 | 0.173 | ahead |
| 10 | 0.181 | 0.436 | 0.496 | −0.121 | lagging |
| 11 | 0.416 | 0.278 | 0.650 | −0.044 | synchronous |
| 12 | 0.221 | 0.289 | 0.457 | −0.053 | synchronous |
| 13 | 0.101 | 0.303 | 0.531 | 0.127 | ahead |
| 14 | 0.223 | 0.620 | 0.612 | −0.231 | lagging |
| 15 | 0.214 | 0.394 | 0.412 | −0.196 | lagging |
| 16 | 0.119 | 0.291 | 0.521 | 0.111 | ahead |
| 17 | 0.144 | 0.300 | 0.468 | 0.024 | synchronous |
| 18 | 0.178 | 0.278 | 0.554 | 0.098 | synchronous |
| 19 | 0.328 | 0.288 | 0.503 | −0.113 | lagging |
| 20 | 0.100 | 0.288 | 0.578 | 0.190 | ahead |
| 21 | 0.232 | 0.450 | 0.694 | 0.012 | synchronous |
| 22 | 0.256 | 0.345 | 0.563 | −0.038 | synchronous |
| 23 | 0.135 | 0.502 | 0.700 | 0.063 | synchronous |
| Hospital | Individual Score | Scores on Indicators | Overall Evaluation | ||||
|---|---|---|---|---|---|---|---|
| Us | Ud | Uc | C | T | D | ||
| 1 | 0.265 | 0.178 | 0.443 | 0.933 | 0.295 | 0.525 | sue for coordination |
| 2 | 0.265 | 0.312 | 0.454 | 0.974 | 0.344 | 0.579 | sue for coordination |
| 3 | 0.412 | 0.305 | 0.528 | 0.975 | 0.415 | 0.636 | primary coordination |
| 4 | 0.179 | 0.270 | 0.500 | 0.914 | 0.316 | 0.538 | sue for coordination |
| 5 | 0.255 | 0.306 | 0.620 | 0.926 | 0.394 | 0.604 | primary coordination |
| 6 | 0.211 | 0.246 | 0.440 | 0.949 | 0.299 | 0.533 | sue for coordination |
| 7 | 0.402 | 0.413 | 0.570 | 0.987 | 0.462 | 0.675 | primary coordination |
| 8 | 0.136 | 0.241 | 0.500 | 0.869 | 0.292 | 0.504 | sue for coordination |
| 9 | 0.095 | 0.228 | 0.496 | 0.808 | 0.273 | 0.470 | on the verge of dissonance |
| 10 | 0.181 | 0.436 | 0.496 | 0.915 | 0.371 | 0.583 | sue for coordination |
| 11 | 0.416 | 0.278 | 0.650 | 0.942 | 0.448 | 0.650 | primary coordination |
| 12 | 0.221 | 0.289 | 0.457 | 0.955 | 0.322 | 0.555 | sue for coordination |
| 13 | 0.101 | 0.303 | 0.531 | 0.814 | 0.312 | 0.504 | sue for coordination |
| 14 | 0.223 | 0.620 | 0.612 | 0.905 | 0.485 | 0.663 | primary coordination |
| 15 | 0.214 | 0.394 | 0.412 | 0.960 | 0.340 | 0.571 | sue for coordination |
| 16 | 0.119 | 0.291 | 0.521 | 0.845 | 0.310 | 0.512 | sue for coordination |
| 17 | 0.144 | 0.300 | 0.468 | 0.896 | 0.304 | 0.522 | sue for coordination |
| 18 | 0.178 | 0.278 | 0.554 | 0.896 | 0.337 | 0.549 | sue for coordination |
| 19 | 0.328 | 0.288 | 0.503 | 0.971 | 0.373 | 0.602 | primary coordination |
| 20 | 0.100 | 0.288 | 0.578 | 0.793 | 0.322 | 0.505 | sue for coordination |
| 21 | 0.232 | 0.450 | 0.694 | 0.909 | 0.459 | 0.646 | primary coordination |
| 22 | 0.256 | 0.345 | 0.563 | 0.948 | 0.388 | 0.606 | primary coordination |
| 23 | 0.135 | 0.502 | 0.700 | 0.812 | 0.446 | 0.602 | primary coordination |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, X.; Dewancker, B.J.; Fang, T.; Xu, Y.; Wang, H.; Zheng, A. Study on the Spatial Coupling Coordination of Public Service Facilities Around Large Comprehensive Hospitals in Beijing from a Supply–Demand Perspective. Buildings 2025, 15, 2188. https://doi.org/10.3390/buildings15132188
Wang X, Dewancker BJ, Fang T, Xu Y, Wang H, Zheng A. Study on the Spatial Coupling Coordination of Public Service Facilities Around Large Comprehensive Hospitals in Beijing from a Supply–Demand Perspective. Buildings. 2025; 15(13):2188. https://doi.org/10.3390/buildings15132188
Chicago/Turabian StyleWang, Xiaoqi, Bart Julien Dewancker, Tingting Fang, Yingjie Xu, Hai Wang, and Andi Zheng. 2025. "Study on the Spatial Coupling Coordination of Public Service Facilities Around Large Comprehensive Hospitals in Beijing from a Supply–Demand Perspective" Buildings 15, no. 13: 2188. https://doi.org/10.3390/buildings15132188
APA StyleWang, X., Dewancker, B. J., Fang, T., Xu, Y., Wang, H., & Zheng, A. (2025). Study on the Spatial Coupling Coordination of Public Service Facilities Around Large Comprehensive Hospitals in Beijing from a Supply–Demand Perspective. Buildings, 15(13), 2188. https://doi.org/10.3390/buildings15132188