Abstract
People with Alzheimer’s disease (PWAD) are impacted by their surroundings, and their performance improves in therapeutic environments designed to meet their specific individual needs, are adjustable in terms of their health status, and are created to accommodate their abilities. A literature review of the field revealed scarce knowledge in using a combination of building information modeling (BIM) and the Internet of Things (IoT) for the purpose of understanding the daily needs and self-orientation ability of PWAD, as well as the architectural barriers they face in their rooms in long-term healthcare centers. In this context, this paper proposes a framework based on computational design approaches to assess the existing therapeutic environment for PWAD using BIM–IoT sensors-based monitoring. The proposed framework used the user experience design concept (UX) and the design thinking framework to evaluate the resident rooms of PWAD. The UX design concept and the design thinking framework core allow for the adoption of user-centered methods to provide a comprehensive image of the issues that affect PWAD in their therapeutic environment. The proposed framework-structured approach will enable healthcare architects/designers to (1) digitalize old building architecture plans using BIM; (2) strategize IoT sensor selection; (3) recognize the activities performed by PWAD and detect any anomaly; and (4) integrate IoT real-time data into the BIM system. The proposed framework supports three types of professionals: (1) architects in decision-making processes, (2) researchers in collecting/analyzing accurate data for shadow observations, and (3) neurologists in following up the health statuses of PWAD.
1. Introduction
Alzheimer’s disease (AD) is becoming more prevalent as the world’s population ages [1]. AD is considered the most common form of dementia and may contribute to 60–70% of the dementia cases [2]. Worldwide, approximately 46.8 million people are living with Alzheimer’s disease [1,2,3]. To put the cost of this disease into perspective, if Alzheimer’s disease represented a country’s economy, it would be the 18th largest factor in terms of economic impact. If AD were a company, it would be most profitable, exceeding Walmart, with USD 414 billion [1,3]. Since AD causes cognitive decline, people suffering from deteriorating memory, language, and other thinking abilities require constant care for the rest of their lives. A smart therapeutic environment can provide new opportunities to the care of people with Alzheimer’s disease (PWAD). Smart therapeutic environments are characterized by sensors and devices embedded in everyday life activities [4]. Ambient assistive technology can provide assistance in making decisions regarding the performance of the daily activities of PWAD and by guiding residents [5]. However, to enable the ambient assistive technology and convert the rooms of PWAD at long-term healthcare centers into a smart therapeutic environment, there is a need to understand in depth the needs and problems of PWAD, especially concerning self-orientation, as well as the architectural barriers that can become obstacles to PWAD performing their daily activities in their room in long-term healthcare centers.
However, applying the same therapeutic environment design to different PWAD is inadequate because each individual’s health status and related problems differ. Each resident has a different identity, background, habits, and symptoms. For this reason, researchers should examine the possibility of developing an experience that is precisely tailored to each individual AD patient’s requirements. User natural shadowing observation via sensors can be a useful analytical tool to create a personalized smart therapeutic environment with a positive outcome for PWAD in their rooms in long-term healthcare centers. User shadowing observation is a qualitative research method that collects rich data about the behaviors of PWAD in their familiar therapeutic environments [6,7]. This research method prioritizes the users’ interaction with the therapeutic environment. It is a research method [8] with a fresh beginning in user experience design concepts (UX) and a design thinking framework. It can potentially gather critical evidence for researchers to create, develop, and improve the existing therapeutic environment for PWAD in long-term healthcare centers, transforming it into a smart environment. User shadowing observation can provide information about elementary spatial characteristics related to residents’ activities and their behavior in their living environment.
IoT technology-based monitoring systems provide an opportunity to support PWAD [9]. Such systems enhance the quality of life of PWAD and reduce caregivers’ burden and healthcare costs while maintaining patient safety [4,10]. Analyzing continuously monitored data using machine learning and artificial intelligence (AI) [11,12] can deliver accurate long-term evaluations and produce valuable information about the actions and routines of PWAD. In a smart therapeutic environment, the vast majority of recognition systems focus primarily on logical or temporal constraints and overlook the constraints of spatial aspects [13,14]. Nevertheless, these aspects can substantially impact recognition [15,16]. A spatial constraint is an object’s spatial configuration in relation to its environment and other objects. For instance, as each object has a size that represents the spatial area in 2D/3D, the area of the object (chair) should not intersect the area of another object (wardrobe) during a step (open the wardrobe door) of an activity. Constraints regarding objects engaged in an activity can be specified based on that premise [15].
Furthermore, objects can feature embedded sensors, actuators, and other devices. This can include smart connections, cloud computing, context-aware processing, etc. Based on an object-oriented approach, the building information modeling (BIM) system performs all of the features of classic 3D CAD/CAM approaches. The BIM technology can create a virtual 3D building model, including data from other analysis applications, such as energy consumption simulations, cost estimation, natural lighting, etc., as shown in Figure 1. BIM can be employed in smart homes in monitoring and management systems. Related studies have focused on managing sensor data flows and the integration of BIM and actuators in the environment [17,18,19].
Figure 1.
BIM technology advantages for facility management.
Ambient assistive technology-based smart devices reshape the therapeutic environments of PWAD, where each device can interact with other devices and humans. This connection between smart devices and systems is defined as the Internet of Things (IoT). Connecting real-time data streams from the rapidly expanding set of IoT sensor networks to BIM models provides an essential framework for applications that increase the construction and operational efficiency of the interactive therapeutic environment. However, BIM and IoT integration research is still in its early stages [20,21]. There exists a gap in the understanding of the current situation regarding BIM and IoT device integration to create interactive therapeutic environments supporting the orientation abilities of PWAD while performing their daily tasks in their rooms in long-term healthcare centers. In this context, this article focuses on strategizing the implementation of interactive indoor environments for PWAD to support their orientation abilities while performing their daily tasks in their rooms in long-term healthcare centers, so as to enhance their quality of life (QoL).
1.1. Background and Related Work
The COVID-19 pandemic adds another layer to the caregivers at the long-term healthcare centers for Alzheimer’s by increasing the demand for renovating old healthcare centers and adopting assistive technology-based monitoring in the rooms of PWAD. PWAD may be more susceptible to contracting the virus and more prone to spreading it simply because their memory of proper sterilization is not always present. Moreover, the COVID-19 pandemic highlighted the need for decision support tools in Alzheimer’s care to help researchers continue collecting and analyzing their research data; the architects in built-environment decision-making processes; and neurologists to follow up the health statuses of PWAD. The COVID-19 pandemic was the most significant difficulty encountered during the research study [22] that occurred at one of the long-term healthcare centers in Vienna, Austria. This problem has prevented the researcher from carrying out more shadow observations for PWAD in their room at the long-term healthcare center due to COVID-19 restrictions. For this objective, this paper proposes a framework based on computational design as an alternative solution for the regular shadow observation by the researcher. Furthermore, combining IoT technology such as sensors, computational design technology such as algorithms, and BIM systems such as Revit, through UX design concepts and a design thinking framework, provides a wide range of tools that could be used for decision support in Alzheimer’s care. The research questions that derive from the objective and articulate the research are: (1) How can we digitalize the as-built for a post-construction old building? (2) What is the criteria for selecting the IoT sensors-based monitoring motion within the context of PWAD? (3) How can we determine the optimal sensors’ placement? (4) What are the analyzing criteria for the movement of PWAD in their rooms at the long-term healthcare center? (5) What is the movement anomaly definition within the context of the behavior of PWAD? (6) How can we display the analyzed data output in the BIM system? (7) What is the ethical consideration for installing IoT technology-based monitoring in the rooms of PWAD at long-term healthcare centers? Dual processes are utilized in solving design challenges using design thinking frameworks and computational design technologies to answer those questions and construct the proposed framework criteria.
1.1.1. Design Thinking Framework
A design thinking framework is an approach for creating design solutions for complex problems, such as designing a therapeutic environment for PWAD. The design thinking framework focuses on the importance of privileging the built environment in user-centered design processes because the built environment is relational, capturing dynamic relationships between other factors of design problems [23]. Due to the design thinking framework serving industry and academia and its promising practices in a broad scope of social and technological innovation projects, such as the Golden Gate Regional Center (GGRC); various industry and academia institutions have developed their design thinking models. The most well-known models are as follows [24]: (1) the double diamond model; (2) IBM’s model; (3) the 31 model; and (4) Stanford d. school. The double diamond model proposed by the design council (the British Council) consists of four stages: (1) discover; (2) define; (3) develop; and (4) deliver. IBM’s model, known as the loop, employs the prompt and continued iteration methodology of (1) observing; (2) reflecting; and (3) making. The 3I model, developed by IDEO, consists of three stages: (1) inspiration; (2) ideation; and (3) implementation. Finally, Stanford d. school model consists of (1) empathizing; (2) definition; (3) ideation; (4) prototyping; and (5) testing stages. These stages are not always sequential, and the five steps are frequently part of an iterative procedure [25].
Based on what was formerly mentioned and due to the complex nature of Alzheimer’s disease, Stanford d. school model (Figure 2) will be used to create the proposed framework.
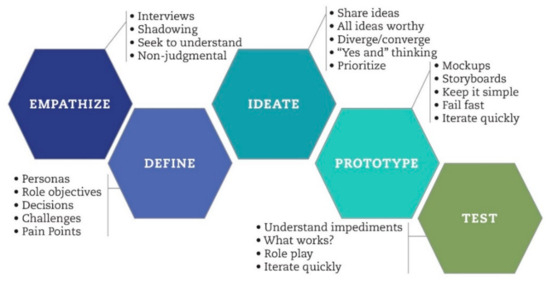
Figure 2.
Stanford d. school model (https://www.stlouisfed.org/publications/bridges/winter-2018-2019/cdac-designing-for-change, accessed on 25 May 2023).
1.1.2. Computational Design Technology
The computational-based design approach is known as computational design (CD). The CD is a design method that combines algorithms and parameters to address design problems through a sequence of logical processes with advanced computer processing. The CD grounds the design representation in its computational logic instead of its geometric aspects. Moreover, the CD is changing design theory and practice due to the wide range of CD toolsets, such as Grasshopper, Dynamo, Param-O, and Marionette, which provide architects with new design methods and tools, automate repetitive tasks, reduce design risks, reduce project costs, provide original aesthetical discourses, and provide never-before-used design/construction strategies [26]. Currently, the design process is enhanced with the power of computation for a more effective and optimized design solution. Documenting the design output is not the final target, but the aim of using CD is all about the steps to create the final result. Furthermore, the CD toolset, such as Dynamo, enables non-specialists an operating mode that does not usually require typing a code list, but rather the connection and processing of graphic entities.
There are three subsets of computational design [27]: (1) parametric design; (2) generative design; (3) and algorithmic design. The parameters influence parametric design in a model; it helps designers to utilize complex shapes, following the rules and programs to move more efficiently. In contrast, the generative design analyses ensure many options for architects to work more sustainably with the pieces of equipment to choose with better judgment. Finally, algorithmic design makes use of algorithms to generate design ideas. These algorithms are rules which describe information, defined in a logical sequence to generate a design [27].
Overall, the computational design technology supports architects in exploring new solutions to improve design processes and decision-making management.
2. Method
As mentioned previously in this paper, the therapeutic environments have either a negative or a positive impact on PWAD [28], which implies the need to understand the therapeutic environment from the perspective of PWAD, specifically in the context of spatial self-orientation, as their perspectives supplement the plans and design processes of the interactive therapeutic environments for PWAD. Understanding the behavior of PWAD is essential to assess the environment around oneself; therefore, design and methods, cross-disciplinary and digital architecture, and neurosciences were combined to create a model that explicitly relates neurological processes, behavior, design principles, and design. The international classification function (ICF) is the rationale behind the model [29,30]. ICF has two parts, each with two components:
Part 1. Functioning and Disability: (a) Body functions and structures; (b) activities and participation.
Part 2. Contextual Factors: (a) Environmental factors; (b) personal factors.
Each component consists of various domains and, within each domain category, the units of classification (Figure 3). Moreover, each component can be represented in both positive and negative terms [29].
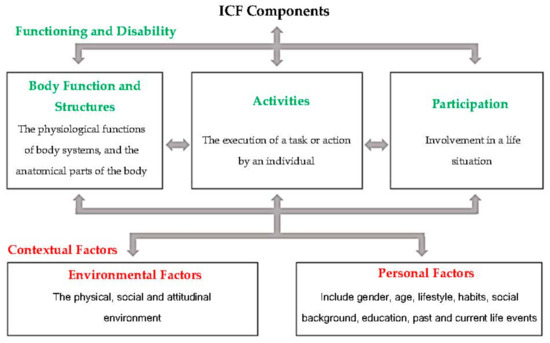
Figure 3.
The interaction between components of the International Classification of Functioning, Disability, and Health.
A scoping review based on empirical studies [31], an exploratory research with a sequential design based on experience [22], and formal knowledge based on previous studies’ results [15,32,33,34,35,36] were used to develop the assessment technique criteria of the proposed framework based on the spatial constraints’ main factors. In user experience design concepts (UX), the essential trigger for effective decision-making is the in-depth knowledge of users. Within this context, the proposed framework aims to collect real-time quantitative data about the movements of PWAD in their rooms at long-term healthcare centers via IoT sensors-based monitoring with a comprehensive analysis via computational tools. The framework then presents the output into a BIM system that aids decision-makers in investigating, analyzing, improving, and assessing the therapeutic environment through the perspective of PWAD.
3. Results
The overarching objective of this paper is to support architects and designers in designing an interactive personalized therapeutic environment; its interior and its technologies match the needs of PWAD and enhance their self-orientation abilities.
Based on the ICF model, the assessing model contains two critical parts, as follows:
1. It has to be based on insights into the neurological processes of PWAD and the resulting behavioral consequences to provide an indication to translate IoT sensors’ data within machine learning algorithms so as to detect the anomaly of the movements of PWAD.
2. It has to support the computational design processes in which design specifications convert the IoT sensor data into environmental data (BIM system) and then to concrete designs, and finally defining the architectural barriers.
Figure 4 illustrates the steps of each part of the assessing model that supports the proposed framework’s development.
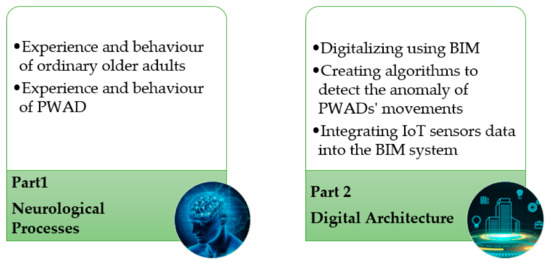
Figure 4.
The steps of the each part of the assessing model that supports the proposed framework’s development.
Based on the formal knowledge of neurology and behavioral sciences [34,36], there is a mutual interaction between a person and the environment in normal brain functioning. According to research [36], the impaired brain becomes increasingly dependent on the surrounding environment. In other words, the person–environment relationship is damaged, and the environment becomes a key determinant of behavior [31,34,35]. Moreover, the insight gained in the study [22] led the researcher to investigate alternative sophisticated techniques based on computational design technology for collecting continuous quantitative data about the movements of PWAD. Based on the insights gained in [15,22,31,32,33,34,35,36] studies, the proposed framework includes five main stages, which are: (1) digitalizing old building architecture plans using BIM; (2) selecting IoT sensors-based monitoring; (3) detecting the anomaly in the movement of PWAD; (4) integrating IoT sensor data into the BIM system (environmental data); and (5) ethical consideration. This approach is intended to replace the ordinary methods for architects in decision-making processes, for researchers collecting/analyzing accurate data for shadow observations, and for neurologists following the health statuses of PWAD.
4. Proposed Framework
Creating a therapeutic environment for PWAD is challenging because each case is different. As they depend on their surrounding environment for self-orientation, modifying the existing therapeutic environment to meet their needs is necessary. Therefore, there is a need to assess the existing therapeutic environment to be modified according to the needs and abilities of PWAD. The proposed framework based on a computational design approaches aim to assess and evaluate the therapeutic environment of PWAD through their perspective, i.e., to be more precise, to partially solve the self-disorientation of PWAD in their rooms. The goal is to provide a personalized smart therapeutic environment that serves the needs of PWAD and their health status limitations to enhance their quality of life.
Figure 5 illustrates the methodology adopted for this study, which includes five main stages. The first stage is digitalizing old building architecture plans using BIM. Most old long-term healthcare buildings for Alzheimer’s care did not use BIM systems in the pre-construction phase. Since a BIM model of an existing building is based on a real asset, collecting information about this asset is a logical first step. ‘As-planned’ documents like plans and sections are frequently the starting points for documenting an existing building. However, these are frequently insufficient, outdated, or simply absent. Nevertheless, the final design of a structure may change significantly from the architect’s original vision. As a result, onsite surveys of the actual asset are required to acquire information on its current state.

Figure 5.
The five main stages of the proposed framework.
The second stage is selecting IoT sensors-based monitoring. Sensors based-monitoring have hundreds of variations and could be categorized into two main groups: (1) wearable sensors and (2) direct environment sensors. In the context of Alzheimer’s care, the criteria for selecting the IoT sensors are developed based on formal knowledge [37], for example: (1) direct environment sensors should be unnoticeable because they might confuse PWAD and (2) the wearable sensors should be comfortable and not cause anxiety for PWAD [5,38]. Another factor to be considered when selecting the sensors is the room layout and size and the sensor’s placement. Finding the optimal placement for the sensors is a significant factor to consider when implementing and adopting the ambient sensors in the room of PWAD [39].
The third stage is detecting the anomaly in the movement of PWAD. As previously mentioned, the assessment of the therapeutic environment is based on anomaly detection in the movement of PWAD through the spatial constraints’ main factors. Moreover, according to [14], the behavior of PWAD is distinguished by recurring incoherencies in their actions, which arise when they perform complex tasks requiring cognitive abilities. In contrast, healthy people can detect and remedy their behavioral errors and mistakes. Furthermore, healthy people do not frequently act incoherently. PWAD, on the other hand, will almost surely act incoherently, even while performing familiar activities, and their behavior will become increasingly incoherent as the disease evolves. Anomalies in the behavior of PWAD will be detected utilizing this pivotal contrast based on the previous four main factors [40].
The fourth stage is integrating IoT sensor data into the BIM system (environmental data). This integration allows for collecting and analyzing real-time data, leading to better decision-making and more efficient maintenance practices. It also provides a common platform for all stakeholders involved in facility management, including architects, engineers, contractors, and facility managers. BIM and IoT integration contains three parts [17]: (1) BIM as data storage for contextual information, such as building geometry, and a list of IoT devices. Contextual information can be stored in BIM tools, for instance, Revit Suite or Archicad, as they are the most popular BIM software. (2) The time-series data record continuous sensor readings, which are stored in a well-structured database, for instance, the relational database, and can be effectively queried using, for instance, structured query language (SQL). (3) The integration method between contextual information and time-series data.
The fifth stage is the ethical consideration; concerns are also associated with using IoT technologies for PWAD [41]. The requirement for privacy and security is one of the main challenges [42]. The data collected by these sensors are sensitive and must be protected from unauthorized access. Another challenge is the need for accuracy and reliability. For these sensors to be effective, they must accurately detect motion and location.
5. Discussion
Based on the insights gained in the exploratory research [22], and since epidemics prevented continual and extensive shadow observations, there was a need to develop a framework based on computational design to help in collecting and analyzing quantitative data and support decision-making processes. The exploratory research raised three main issues: (1) The necessity of utilizing BIM in facility management at the post-construction stage. (2) The dual use of the assistive technology; firstly, using IoT sensors-based monitoring for shadow observation encourages continuity in collecting data, mainly during the pandemic, which identify the residents’ needs and problems to enhance the design thinking of the therapeutic environment and secondly, as an assistive tool to achieve a specific activity. (3) The necessity of using computational design-based decision-support approaches. As the health status and personality of PWAD might change [43], the data collected by the sensors can feed into machine learning and artificial intelligence-based applications that would facilitate the self-learning capacity of assistive technology setups and convert the smart therapeutic environment into a cognitive therapeutic environment, as it will be capable of learning new rules through the interactions of PWAD with the environment [44].
Therefore, there is a need to develop a framework based on computational design to assess the therapeutic environment of PWAD within the user experience design concept (UX) and the design thinking framework. The UX design concept and the design framework of the Stanford d. school model, with its five steps (empathizing; definition; ideation; prototyping; and testing), makes designing a therapeutic environment that matches the needs and abilities of PWAD feasible. These four steps help validate an architectural intervention that stimulates or prevents the self-orientation of PWAD in achieving their daily activities independently without caregivers’ support inside their rooms.
Creating a framework based on computational design to assess the therapeutic environment in the context of Alzheimer’s care and post-construction healthcare building with no BIM documents is challenging. On the one hand, PWAD might interact differently with IoT ambient or wearable sensors. On the other hand, the post-construction old long-term healthcare center is not eligible to integrate new technology, such as embedded devices. Therefore, the proposed framework includes five stages with a comprehensive vision to cover all the challenges that might be considered obstacles during the implementation phase.
Since BIM has become increasingly prevalent in both digitalizing old building architecture plans and for the facility management (FM) of a smart therapeutic environment [45,46], the first stage of the proposed framework is digitalizing old building architecture plans using BIM. A complete as-built geometry is required for using BIM systems. Creating an as-built BIM model differs significantly from creating an as-planned model. The computation technology provides three methods to achieve an as-built model (geometric) efficiently: (1) Laser scanning or photogrammetry [47], which is mainly known as “scan-to-BIM” for high-detail models. Most day-to-day FM operations do not require the details supplied by these models. (2) An automated conversion of 2D to 3D plans of the BIM [48], aiming to enable more fluid and flexible workflows that do not require BIM models to be manually recreated. (3) The translation of 3D geometric models to BIM [49], translating the 3D models created in Trimble SketchUp and Mc-Neel Rhino for conceptual design to Graphisoft ArchiCAD and Autodesk Revit for BIM modeling.
An IoT technology system includes four essential parts [50]: (1) external devices (sensors, actuators), which collect monitoring data; (2) a control system (AI system), which receives the data from the external devices and makes decisions; (3) transmission system (wired/wireless network) that connects the external devices and control system; and (4) data, which could be used to control the environment to enhance the quality of life for PWAD. The proposed framework depends on the collected quantitative data for the movements and activities of PWAD to assess their therapeutic environment; therefore, there is a need to combine and install both the wearable and the direct environment sensors in the rooms of PWAD to provide accurate insights. The wearable sensors have a dual use: (1) to detect the motion and movements of PWAD and (2) to collect physiological data, including blood pressure, heart rate, body temperature, etc. The wearable biosensors/sensors-based monitoring motions include vast choices, for instance, feet- and waist-mounted inertial sensors, ankle-mounted accelerometer sensors, wrist-mounted accelerometers, and leg-mounted force sensors [10,51]. The selection of the wearable sensors depends on the resident’s acceptance and which type will be comfortable and not cause anxiety to the resident.
Moreover, the direct environment sensors (ambient sensors) consist of passive infrared (PIR) sensors, preferred because of their small size, low cost, and because they consume less power and are very easy to use; pressure sensors attached to the bed; contact switch sensors (CSS) attached to doors or closets, which can capture activities such as walking, sleeping, or exiting the room; and a central energy consumption monitoring device [38,50,52]. Although most direct environment sensors are non-structural, placed on the surface of architectural elements, or installed inside furniture [53], building modification is still necessary to effectively ensure the IoT systems’ performance. The sensors’ placement is essential in monitoring the movement and activity of PWAD to avoid collecting misleading information. The computational design provides methods [54] for selecting the optimal sensor placement based on the BIM system, allowing the user to have an optimal solution displayed on the BIM after a few analysis steps. These analysis characteristics are: (1) the resident’s room size; (2) the sensor features; (3) the neighbor zones, which have to be covered by two different combinations of sensors to distinguish the target location according to sensor activation; and (4) a sensor number determined for each zone, which depends on the sensor field of view and zone size.
Activity recognition and anomaly detection are a complex process (Figure 6) characterized by four main phases: (1) selecting and adopting sensors-based monitoring to collect data on the behavior of PWAD; (2) collecting, storing, and processing information through AI; (3) creating computational models to conduct reasoning and anomaly; and (4) developing reasoning algorithms to conclude activities from sensor data [15,38,55]. The anomaly detection in the behavior data of PWAD could be determined through the spatial constraints’ main factors [15,32,33].
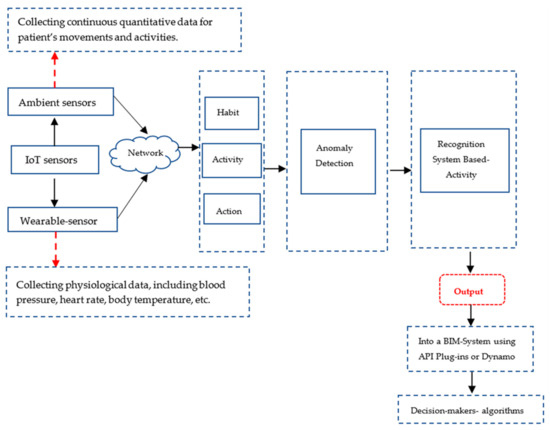
Figure 6.
The anomaly detection system in the movement of PWAD through four main factors.
For an in-depth understanding of how to detect the movement anomaly of PWAD, it is helpful to determine human behaviors at different levels of granularity. For physical behaviors, the terms “action”, “activity”, and “habit” [38,41,55] are commonly used in activity recognition communities. The term “action” refers to a simple behavior performed by a person for a short duration, for instance, opening a door, while the term “activity” refers to complicated behaviors that include a series of acts and interleaving or overlapping actions for longer durations and could be performed by one person or more, for instance, two persons preparing meals. A “habit” refers to one or more activities that are repeated regularly in a consistent way [56]. Hence, to define a set of activities as a habit, there should be no or only slight variations on how such activities are performed, for instance, taking medicine with a glass of water every morning after breakfast.
Machine learning approaches are more compatible with the four main activities and anomaly recognition phases than classical mathematics and statistical techniques in extracting knowledge and discovering, learning, and inferring activity from data [12]. Machine learning provides algorithms that connect physiological and environmental data collected by IoT technologies (sensors) [11]. These algorithms include: (1) rule-based reasoning methods and adaptive learning mechanisms to make them more personalized and (2) machine-learning techniques to learn the activities/patterns of PWAD and detect unusual behavior, as well as for the pattern detection algorithms that provide a holistic view of the activity and routines of PWAD. Pattern detection algorithms analyze PWAD data at different temporal granularities to develop automated procedures for macro- and micro-assessments. Moreover, the micro-assessment framework focuses on detecting underlying activity patterns that can be used to conclude the day-to-day well-being of PWAD and categorize them according to PWADs’ behavior and movements errors [11].
Because the BIM–IoT integration has become one of the most vital current research fields, enabling non-specialists to access computational design toolsets is becoming increasingly important. Tools are frequently improving user access to algorithms [57]. For instance, Revit/Dynamo integration for sensor data management [19]. The dynamo visual programming platform is an operating mode that does not usually require typing a code list, but instead the connection and processing of graphic entities. The visual approach simplifies the development of applications by isolating the complexity of coding to the primary users of Revit (architects, designers, engineers, companies, etc.). Moreover, for professional architects, there are more advanced methods for producing the output into the BIM system, such as the application programming interface (API). API is creating plug-ins to integrate sensor technology with the BIM model using Autodesk Revit software 2023 when using BIM to analyze the collected sensor data and display the output into the BIM system [58].
Furthermore, the use of IoT technologies for PWAD raises ethical questions such as the ability of PWAD to provide truly informed consent, how their privacy is protected, or how the confidentiality of their information is managed. Privacy, autonomy, and data ownership are considered significant issues when implanting IoT technology-based monitoring in the rooms of PWAD at the long-term healthcare center. The answer to these questions is presented throughout the literature [42,59,60]. The literature clarified three main aspects to be considered while using IoT technology-based monitoring: (1) the safety of PWAD is prioritized; (2) involve PWAD in decision-making processes; and (3) informed consent forms, the protection of privacy and confidentiality, and the acknowledgment of duty to protect, should be signed by a family member of the PWAD. IoT technology-based monitoring is allowed, according to the literature [41,60], depending on the purpose it will be used for; additionally, it is essential to have the PWAD and their family members’ approval to use such technology.
The difference between the previous framework in the same field and the one proposed here is that the proposed framework attempts to improve the therapeutic environment at Alzheimer’s long-term healthcare centers by dual processes in solving design challenges using design thinking framework and computational design technologies. Furthermore, the proposed framework evaluates each resident’s room from each resident’s perspective, abilities, and health status. These differences are the main novelty of this proposed framework.
The complex nature of Alzheimer’s disease and designing a therapeutic environment that caters to the needs and abilities of PWAD revealed the importance of combining and pursuing a cross-disciplinary approach with digital architecture and neuroscience to create an interactive personalized therapeutic environment with a positive impact on PWAD, in addition to the significant contribution of computational design technology in the decision-making process. From the insight gained from this paper, a reflective question arose: How far could the contribution of cross-disciplinary methods enhance the ethical considerations concerning gerontechnology for Alzheimer’s disease?
6. Conclusions
This paper proposed a framework based on a computational design as an alternative method to the ordinary shadow observations by researchers. The proposed framework aims to examine the problems experienced by PWAD when performing their daily activities and navigating their rooms in long-term healthcare centers. Therapeutic environments have many prospects to improve the health statuses of PWAD that could be significantly improved through specific insights into architectural and other barriers resulting from the design of the resident rooms of PWAD. The UX design concept and design thinking framework are both underpinning the proposed framework criteria to determine these insights in architectural design. Integrating IoT sensors-based monitoring within the framework of BIM has the potential to reshape the therapeutic environment for PWAD. IoT technology, such as sensors, actuators, and other devices, can create a personalized smart therapeutic environment that caters to the needs and abilities of PWAD. The proposed framework highlighted several key aspects related to implementing this technology. Using BIM in the facility management of the post-construction stage allows for the efficient monitoring and management of the therapeutic environment. Additionally, the adaptive nature of the technology enables it to accommodate the changing health statuses and personalities of PWAD through the use of machine learning and artificial intelligence-based applications. The dual use of assistive technologies was also emphasized, with sensors serving as tools for both shadow observation and specific activity assistance. By continuously collecting data on the movements of PWAD, architectural barriers can be identified and addressed, promoting their independent performance of daily activities. Moreover, assistive technologies can provide personalized support and guidance for specific tasks, further enhancing their autonomy.
However, it is important to consider ethical implications when implementing IoT technology-based monitoring in the rooms of PWAD. Privacy, informed consent, and data ownership are significant concerns that must be addressed. By using IoT technologies, new and extensive amounts of data are generated; to whom that data belongs to remains a subject of serious inquiry. It is essential to preserve the confidentiality of sensitive data and prevent exposing them in any personally identifiable way. Ensuring the safety of PWAD, involving them in decision-making processes, and obtaining informed consent from them and their family members are crucial steps in addressing these ethical considerations.
Overall, the research contributes to understanding how IoT technology-based smart devices, integrated with BIM, can reshape the therapeutic environment for PWAD. Incorporating computational design methods, collaboration, and interdisciplinary approaches can lead to holistic design solutions that address not only architectural aspects, but also healthcare requirements and the well-being of PWAD. Moving forward, further research and exploration in this area are warranted to continue advancing the development and implementation of ambient assistive technology in the context of the therapeutic environments of PWAD. By addressing the challenges and ethical considerations, we can harness the full potential of these technologies to improve the quality of life and care of PWAD.
7. Patents
Inventor: Heidi Elnimr. „Verfahren und System zur Überwachung einer Person in einem Raum“ Österreichische Patentanmeldung A 50581/2023, filed on 19 July 2023.
Funding
This research received no external funding.
Data Availability Statement
Data sharing is not applicable to this article as no new data were created or analyzed in this study.
Acknowledgments
The author acknowledges TU Wien Bibliothek for financial support through its open access funding program.
Conflicts of Interest
The author declares no conflict of interest.
References
- 2021 Alzheimer’s Disease Facts and Figures. Alzheimer’s Dement. J. Alzheimer’s Assoc. 2021, 17, 327–406. [CrossRef]
- World Health Organization. Global Action Plan on the Public Health Response to Dementia: 2017–2025; World Health Organization: Geneva, Switzerland, 2017.
- 2023 Alzheimer’s Disease Facts and Figures. Alzheimer’s Dement. 2023, 19, 1598–1695. [CrossRef]
- Evans, J.; Brown, M.; Coughlan, T.; Lawson, G.; Craven, M.P. A Systematic Review of Dementia Focused Assistive Technology. In Human-Computer Interaction: Interaction Technologies; Kurosu, M., Ed.; Springer International Publishing: Cham, Switzerland, 2015; Volume 9170, pp. 406–417. [Google Scholar]
- Lapointe, J.; Bouchard, B.; Bouchard, J.; Potvin, A.; Bouzouane, A. Smart homes for people with Alzheimer’s disease: Adapting prompting strategies to the patient’s cognitive profile. In Proceedings of the 5th International Conference on Pervasive Technologies Related to Assistive Environments, PETRA 2012, Heraklion, Crete, Greece, 6–9 June 2012; Makedon, F., Ed.; ACM: New York, NY, USA, 2012; pp. 1–30. [Google Scholar]
- Liberati, E.G. What Is the Potential of Patient Shadowing as a Patient-Centred Method? BMJ Qual. Saf. 2017, 26, 343–346. [Google Scholar] [CrossRef]
- Goodrich, J.; Ridge, D.; Cartwright, T. A Qualitative Study Exploring Patient Shadowing as a Method To Improve Patient-Centred Care: 10 Principles for A New Gold Standard. Int. J. Qual. Health Care J. Int. Soc. Qual. Health Care 2022, 34, mzac018. [Google Scholar] [CrossRef]
- Alasuutari, P.; Bickman, L.; Brannen, J. The Sage Handbook of Social Research Methods; SAGE: Los Angeles, CA, USA; London, UK, 2009. [Google Scholar]
- Urwyler, P.; Stucki, R.; Rampa, L.; Müri, R.; Mosimann, U.P.; Nef, T. Cognitive Impairment Categorized in Community-Dwelling Older Adults with and without Dementia Using In-Home Sensors that Recognise Activities of Daily Living. Sci. Rep. 2017, 7, 42084. [Google Scholar] [CrossRef]
- Sun, X.; Sun, X.; Wang, Q.; Wang, X.; Feng, L.; Yang, Y.; Jing, Y.; Yang, C.; Zhang, S. Biosensors Toward Behavior Detection in Diagnosis of Alzheimer’s Disease. Front. Bioeng. Biotechnol. 2022, 10, 1031833. [Google Scholar] [CrossRef] [PubMed]
- Enshaeifar, S.; Zoha, A.; Markides, A.; Skillman, S.; Acton, S.T.; Elsaleh, T.; Hassanpour, M.; Ahrabian, A.; Kenny, M.; Klein, S.; et al. Health Management and Pattern Analysis of Daily Living Activities of People with Dementia Using in-Home Sensors and Machine Learning Techniques. PLoS ONE 2018, 13, e0195605. [Google Scholar] [CrossRef]
- Ramasamy Ramamurthy, S.; Roy, N. Recent Trends in Machine Learning for Human Activity Recognition—A Survey. WIREs Data Min. Knowl. Discov. 2018, 8, e1254. [Google Scholar] [CrossRef]
- Mihailidis, A. (Ed.) Technology and Aging: Selected Papers from the 2007 International Conference on Technology and Aging; Ios Press: Amsterdam, The Netherlands; Oxford, UK, 2008. [Google Scholar]
- Bouchard, B.; Giroux, S.; Bouzouane, A. A Keyhole Plan Recognition Model for Alzheimer’s Patients: First Results. Appl. Artif. Intell. 2007, 21, 623–658. [Google Scholar] [CrossRef]
- Bouchard, K.; Bouchard, B.; Bouzouane, A. Spatial Recognition of Activities for Cognitive Assistance: Realistic Scenarios Using Clinical Data from Alzheimer’s Patients. J. Ambient. Intell. Humaniz. Comput. 2014, 5, 759–774. [Google Scholar] [CrossRef]
- Augusto, J.C.; Liu, J.; Mccullagh, P.; Wang, H.; Yang, J.-B. Management of Uncertainty and Spatio-Temporal Aspects for Monitoring and Diagnosis in a Smart Home. Int. J. Comput. Intell. Syst. 2008, 1, 361–378. [Google Scholar]
- Tang, S.; Shelden, D.R.; Eastman, C.M.; Pishdad-Bozorgi, P.; Gao, X. A Review of Building Information Modeling (Bim) and the Internet of Things (Iot) Devices Integration: Present Status and Future Trends. Autom. Constr. 2019, 101, 127–139. [Google Scholar] [CrossRef]
- Panteli, C.; Kylili, A.; Fokaides, P.A. Building Information Modelling Applications in Smart Buildings: From Design To Commissioning and Beyond A Critical Review. J. Clean. Prod. 2020, 265, 121766. [Google Scholar] [CrossRef]
- Desogus, G.; Quaquero, E.; Rubiu, G.; Gatto, G.; Perra, C. Bim and Iot Sensors Integration: A Framework for Consumption and Indoor Conditions Data Monitoring of Existing Buildings. Sustainability 2021, 13, 4496. [Google Scholar] [CrossRef]
- Elqasaby, A.R.; Alqahtani, F.K.; Alheyf, M. State of the Art of Bim Integration with Sensing Technologies in Construction Progress Monitoring. Sensors 2022, 22, 3497. [Google Scholar] [CrossRef] [PubMed]
- Yang, A.; Han, M.; Zeng, Q.; Sun, Y. Adopting Building Information Modeling (Bim) for the Development of Smart Buildings: A Review of Enabling Applications and Challenges. Adv. Civ. Eng. 2021, 2021, 8811476. [Google Scholar] [CrossRef]
- Elnimr, H. A Study of Architectural Barriers and the Potential Role of Assistive Technologies in Long-Term Healthcare Centres for People with Alzheimer’s. IxdA 2022, 54, 111–133. [Google Scholar] [CrossRef]
- Tham, J.C.K. Keywords in Design Thinking: A Lexical Primer for Technical Communicators & Designers; University Press of Colorado: Denver, CO, USA, 2022. [Google Scholar]
- Kwon, J.; Choi, Y.; Hwang, Y. Enterprise Design Thinking: An Investigation on User-Centered Design Processes in Large Corporations. Designs 2021, 5, 43. [Google Scholar] [CrossRef]
- Traifeh, H.; Staubitz, T.; Meinel, C. Improving Learner Experience and Participation in Moocs: A Design Thinking Approach. In 2019 IEEE Learning with Moocs; IEEE: Piscataway, NJ, USA, 2019; pp. 165–169. [Google Scholar]
- Caetano, I.; Leitão, A. Architecture Meets Computation: An Overview of the Evolution of Computational Design Approaches in Architecture. Archit. Sci. Rev. 2020, 63, 165–174. [Google Scholar] [CrossRef]
- Gu, N.; Wan, X. Computational Design Methods and Technologies: Applications in Cad, Cam, and Cae Education; Gu, N., Wang, X., Eds.; Information Science Reference: Hershey, PA, USA, 2012. [Google Scholar]
- Ron Smith, N.W. Therapeutic Environments; Wbdg: Washington, DC, USA, 2016. [Google Scholar]
- World Health Organization. International Classification of Functioning, Disability, and Health; Icf Short Version; World Health Organization: Geneva, Switzerland, 2001.
- Peterson, D.B. International Classification of Functioning, Disability and Health: An Introduction for Rehabilitation Psychologists. Rehabil. Psychol. 2005, 50, 105–112. [Google Scholar] [CrossRef]
- Elnimr, H. Interactive Architecture as a Therapeutic Environment for People with Alzheimer’s Disease, A Scoping Review. Formakademisk 2021, 14, 1–18. [Google Scholar] [CrossRef]
- Richardson, M.; Domingos, P. Markov Logic Networks. Mach. Learn. 2006, 62, 107–136. [Google Scholar] [CrossRef]
- Gayathri, K.S.; Easwarakumar, K.S. Intelligent Decision Support System for Dementia Care Through Smart Home. Procedia Comput. Sci. 2016, 93, 947–955. [Google Scholar] [CrossRef]
- Colombo, D.; Serino, S.; Tuena, C.; Pedroli, E.; Dakanalis, A.; Cipresso, P.; Riva, G. Egocentric and Allocentric Spatial Reference Frames in Aging: A Systematic Review. Neurosci. Biobehav. Rev. 2017, 80, 605–621. [Google Scholar] [CrossRef]
- Feddersen, E.; Lüdtke, I. (Eds.) Lost in Space: Architecture and Dementia; Birkhäuser: Basel, Switzerland; Berlin, Germany; Boston, MA, USA, 2014. [Google Scholar]
- Goldberg, E. The New Executive Brain: Frontal Lobes in a Complex World; Oxford University Press: New York, NY, USA, 2009. [Google Scholar]
- Orpwood, R.; Gibbs, C.; Adlam, T.; Faulkner, R.; Meegahawatte, D. The Design of Smart Homes for People with Dementia—User-Interface Aspects. Univ. Access Inf. Soc. 2005, 4, 156–164. [Google Scholar] [CrossRef]
- Chimamiwa, G.; Giaretta, A.; Alirezaie, M.; Pecora, F.; Loutfi, A. Are Smart Homes Adequate for Older Adults with Dementia? Sensors 2022, 22, 4254. [Google Scholar] [CrossRef]
- Fanti, M.P.; Roccotelli, M.; Lesage, J.-J.; Faraut, G. Automation, Ieee International Conference on Emerging Technologies and Factory. In Proceedings of the 2016 IEEE 21st International Conference on Emerging Technologies and Factory Automation (Etfa), Berlin, Germany, 6–9 September 2016; IEEE: Piscataway, NJ, USA, 2016; pp. 1–6. [Google Scholar]
- Baum, C.; Edwards, D.F. Cognitive Performance in Senile Dementia of the Alzheimer’s Type: The Kitchen Task Assessment. Am. J. Occup. Ther. Off. Publ. Am. Occup. Ther. Assoc. 1993, 47, 431–436. [Google Scholar] [CrossRef]
- Guisado-Fernández, E.; Giunti, G.; Mackey, L.M.; Blake, C.; Caulfield, B.M. Factors Influencing the Adoption of Smart Health Technologies for People with Dementia and Their Informal Caregivers: Scoping Review and Design Framework. JMIR Aging 2019, 2, e12192. [Google Scholar] [CrossRef]
- Sundgren, S.; Stolt, M.; Suhonen, R. Ethical Issues Related to the Use of Gerontechnology in Older People Care: A Scoping Review. Nurs. Ethics 2020, 27, 88–103. [Google Scholar] [CrossRef] [PubMed]
- Islam, M.; Mazumder, M.; Schwabe-Warf, D.; Stephan, Y.; Sutin, A.R.; Terracciano, A. Personality Changes with Dementia from the Informant Perspective: New Data and Meta-Analysis. J. Am. Med. Dir. Assoc. 2019, 20, 131–137. [Google Scholar] [CrossRef] [PubMed]
- Motamedi, A.; Shahinmoghadam, M. Bim-Iot-Integrated Architectures as the Backbone of Cognitive Buildings: Current State and Future Directions. In Bim-Enabled Cognitive Computing for Smart Built Environment: Potential, Requirements, and Implementation, 1st ed.; Yitmen, I., Ed.; CRC Press: Boca Raton, FL, USA, 2021; pp. 45–68. [Google Scholar]
- Bortoluzzi, B.; Efremov, I.; Medina, C.; Sobieraj, D.; Mcarthur, J.J. Automating the Creation of Building Information Models for Existing Buildings. Autom. Constr. 2019, 105, 102838. [Google Scholar] [CrossRef]
- Liu, H.; Abudayyeh, O.; Liou, W. Construction Research Congress 2020, Proceedings of the Computer Applications, Construction Research Congress 2020, Tempe, AZ, USA, 8–10 March 2020; Tang, P., Grau, D., Asmar, M.E.L., Eds.; American Society of Civil: Reston, VA, USA, 2020; pp. 1087–1095. [Google Scholar]
- Werbrouck, J.; Pauwels, P.; Bonduel, M.; Beetz, J.; Bekers, W. Scan-To-Graph: Semantic Enrichment of Existing Building Geometry. Autom. Constr. 2020, 119, 103286. [Google Scholar] [CrossRef]
- Janssen, P.; Chen, K.W.; Mohanty, A. Ecaade 2016: Complexity & Simplicity. In Proceedings of the 34th International Conference on Education and Research in Computer Aided Architectural Design in Europe (Ecaade), Oulu, Finland, 24–26 August 2016; Herneoja, A., Österlund, T., Markkanen, P., Eds.; Ecaade: Ghent, Belgium, 2016; Volume 2, pp. 583–590. [Google Scholar]
- Xue, F.; Lu, W.; Chen, K.; Webster, C.J. Bim Reconstruction from 3d Point Clouds: A Semantic Registration Approach Based on Multimodal Optimization and Architectural Design Knowledge. Adv. Eng. Inform. 2019, 42, 100965. [Google Scholar] [CrossRef]
- Udupa, P.; Yellampalli, S.S. Smart Home for Elder Care Using Wireless Sensor. Circuit World 2018, 44, 69–77. [Google Scholar] [CrossRef]
- Stavropoulos, T.G.; Papastergiou, A.; Mpaltadoros, L.; Nikolopoulos, S.; Kompatsiaris, I. Iot Wearable Sensors and Devices in Elderly Care: A Literature Review. Sensors 2020, 20, 2826. [Google Scholar] [CrossRef] [PubMed]
- Baig, M.M.; Afifi, S.; Gholamhosseini, H.; Mirza, F. A Systematic Review of Wearable Sensors and Iot-Based Monitoring Applications for Older Adults—A Focus on Ageing Population and Independent Living. J. Med. Syst. 2019, 43, 233. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Stroulia, E.; Nikolaidis, I.; Miguel-Cruz, A.; Rios Rincon, A. Smart Homes and Home Health Monitoring Technologies for Older Adults: A Systematic Review. Int. J. Med. Inform. 2016, 91, 44–59. [Google Scholar] [CrossRef]
- Ben Bachouch, R.; Fousseret, Y.; Parmantier, Y. Optimal Sensor Placement in Smart Home Using Building Information Modeling: A Home Support Application. Irbm 2023, 44, 100745. [Google Scholar] [CrossRef]
- Chen, L.; Hoey, J.; Nugent, C.D.; Cook, D.J.; Yu, Z. Sensor-Based Activity Recognition. IEEE Trans. Syst. Man Cybern. C 2012, 42, 790–808. [Google Scholar] [CrossRef]
- Thompson, M. Occupations, Habits, and Routines: Perspectives from Persons with Diabetes. Scand. J. Occup. Ther. 2014, 21, 153–160. [Google Scholar] [CrossRef]
- De Boissieu, A. Introduction To Computational Design: Subsets, Challenges in Practice and Emerging Roles. In Industry 4.0 for the Built Environment: Methodologies, Technologies and Skills, 1st ed.; Bolpagni, M., Gavina, R., Ribeiro, D., Eds.; Springer: Cham, Switzerland, 2022; Volume 20, pp. 55–75. [Google Scholar]
- Kazado, D.; Kavgic, M.; Eskicioglu, R. Integrating Building Information Modeling (Bim) and Sensor Technology for Facility Management. J. Inf. Technol. Constr. 2019, 24, 440–458. [Google Scholar]
- Serafini, J.D.; Damianakis, T.; Marziali, E. Clinical Practice Standards and Ethical Issues Applied to a Virtual Group Intervention for Spousal Caregivers of People with Alzheimer’s. Soc. Work Health Care 2007, 44, 225–243. [Google Scholar] [CrossRef] [PubMed]
- White, E.B.; Montgomery, P. Electronic Tracking for People with Dementia: An Exploratory Study of the Ethical Issues Experienced by Carers in Making Decisions about Usage. Dementia 2014, 13, 216–232. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).