1. Introduction
Wayfinding can be defined as the process of finding one’s way to a destination in a familiar or unfamiliar setting using any cues given by the environment. Due to its presence in everyday life, wayfinding appears to be an easily characterized and understood process. However, multiple studies on wayfinding have revealed that it is a profoundly complex exercise [
1]. Malaysia has many old and new hospital buildings; however, there are no locally drawn guidelines to inform the design of healthcare facilities, and current design practices tend to rely on the information and guidelines in foreign materials and resources [
2]. Outpatient areas are some of the most visually cluttered regions of a hospital’s interior environments and have little exposure to the exterior environment. Thus, they scored the lowest in terms of levels of spatial quality and overall user satisfaction, with wayfinding being one of the most challenging in this particular area [
2]. According to [
3], healthcare facilities are often considered to be complex and overwhelming for users, who indicated that wayfinding through healthcare facilities could be demanding and taxing.
Wayfinding can be considered an essential aspect of the environmental spatial quality [
2]. Ref. [
4] defined the spatial quality of environments of interiors to be the structure and enclosures formed by the architectural elements of which the domain is comprised, such as floors, ceilings, walls, windows, and vertical movement bridging features, such as stairwells and elevators. Interior elements of the environment can serve both visual and functional purposes by incorporating material properties, construction element properties, and technology. Visible elements of the built environment conform spaces into habitable and available spaces and can otherwise cause confusion and visual clutter, which can cause visual discomfort [
5], as well as several other undesirable outcomes, including high levels of stress and anxiety, a loss of perceived control, and insufficient access to positive distractions, which was described as a lack of meaningful interaction with nature by [
6,
7].
An investigation of the literature on the topic of wayfinding indicated four thematically linked research domains in which researchers have attempted to identify the concept of wayfinding. These domains are: (1) the individual domain; (2) the social domain; (3) the physical environment domain; and (4) the institutional domain (see
Table 1).
Based on the socio-ecological model (SEM), these domains can be viewed conceptually as layers or levels stemming from the center. In the SEM, human cognition occurs outwardly, leading to the social environment as the second layer, then the physical environment as the third layer. Finally, the institutional environment comprises what the institution has adopted as its standard operating procedure.
Figure 1 summarizes the various factors that can influence the wayfinding process within the framework of the SEM.
1.1. Wayfinding in Hospitals
The indoor environments of hospitals are some of the most complex environments to navigate due mainly to the high degree of intersection between functions and activities and the many functional goals and environmental concerns [
22]. Consequently, the higher levels of functional integration led to the spaces being arrayed in specific patterns to ensure that the required levels of functionality were achieved [
30]. According to [
31], interiors of healthcare facilities have been designed with assertiveness in order to achieve functional objectives. This practice-oriented tendency may create an environment that dismisses the psychological needs of patients, visitors, and staff members. [
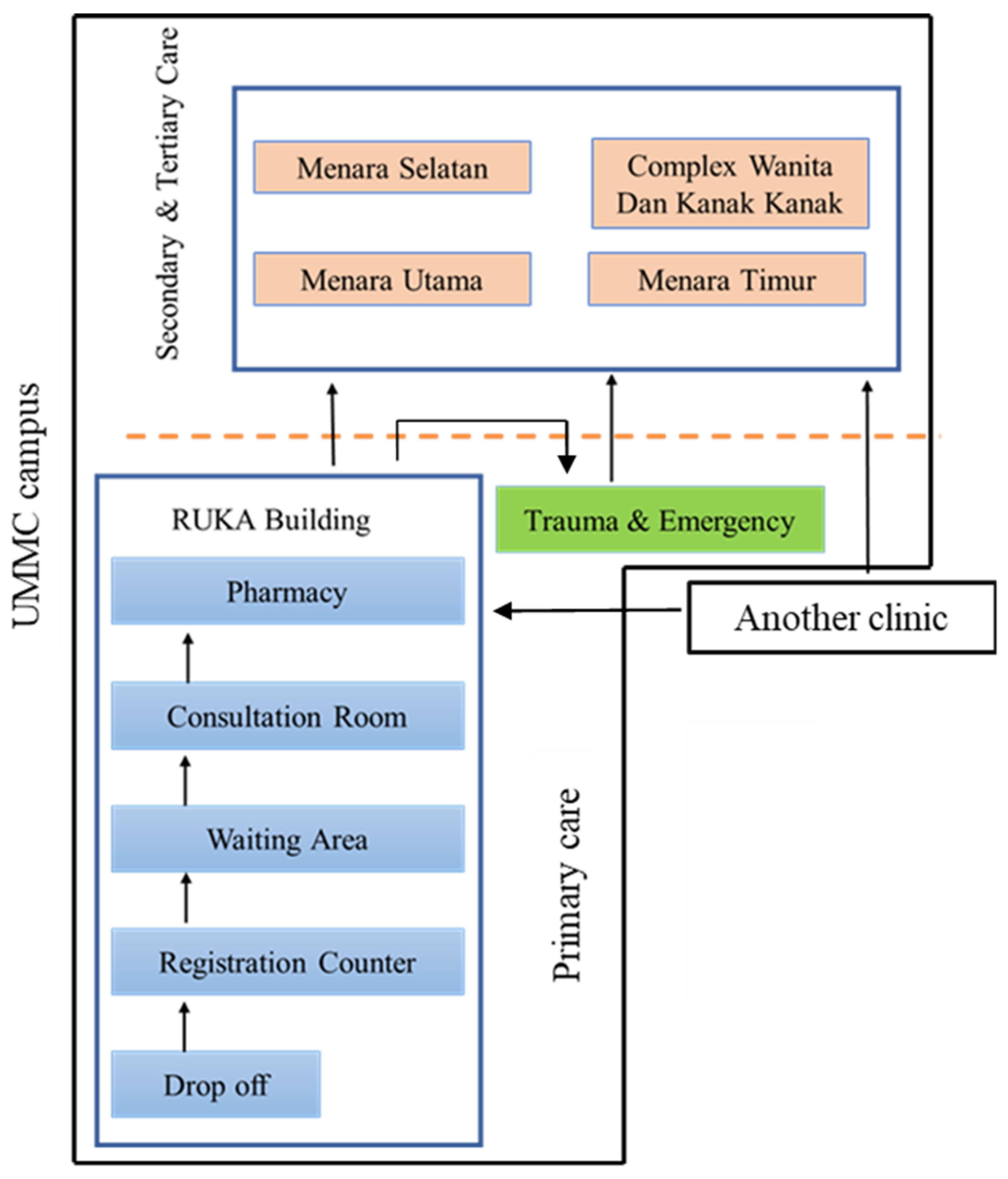
30] regarded the interior environment of these healthcare facilities as psychologically challenging and stressful to users. In this regard, the emphasis on the role of wayfinding and its effects on patients’ physical and psychological states is apparent. Furthermore, healthcare buildings are not static; new linkages are often built to connect newly built annexes to the main building [
32]. These buildings should thus be viewed as dynamic entities that grow, shift space within their morphology, and change or alter their topology.
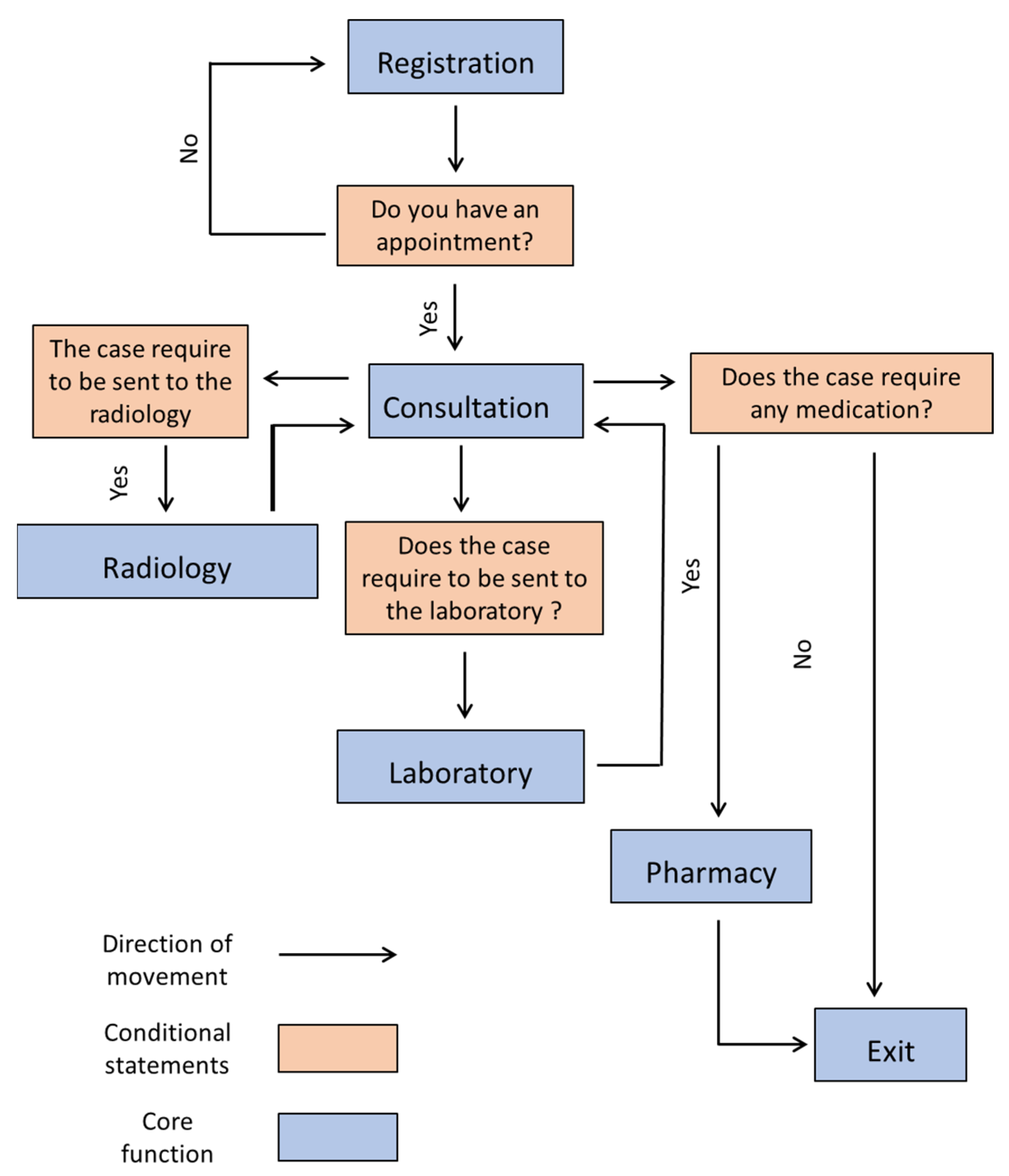
What is it that makes wayfinding especially challenging in healthcare settings compared with other structures such as airports and shopping centers? The wayfinding process in a healthcare setting is highly standardized; it has a purpose at its core. Therefore, it is considered a resolute type of wayfinding, except in spaces in which recreational wayfinding can emerge. While wayfinding in airports and shopping centers is regarded as a recreational type of wayfinding, the urgency levels differ. Furthermore, hospital patients are considered users who are cognitively operating at a sub-optimal level, which requires them to pay further attention to the nuances of wayfinding.
1.2. The Malaysian Healthcare System
The Malaysian healthcare system was initially based on the British healthcare model. It evolved and formulated the hierarchy of its referral system based on local health needs and the requirements of the World Health Organization (WHO) [
26].
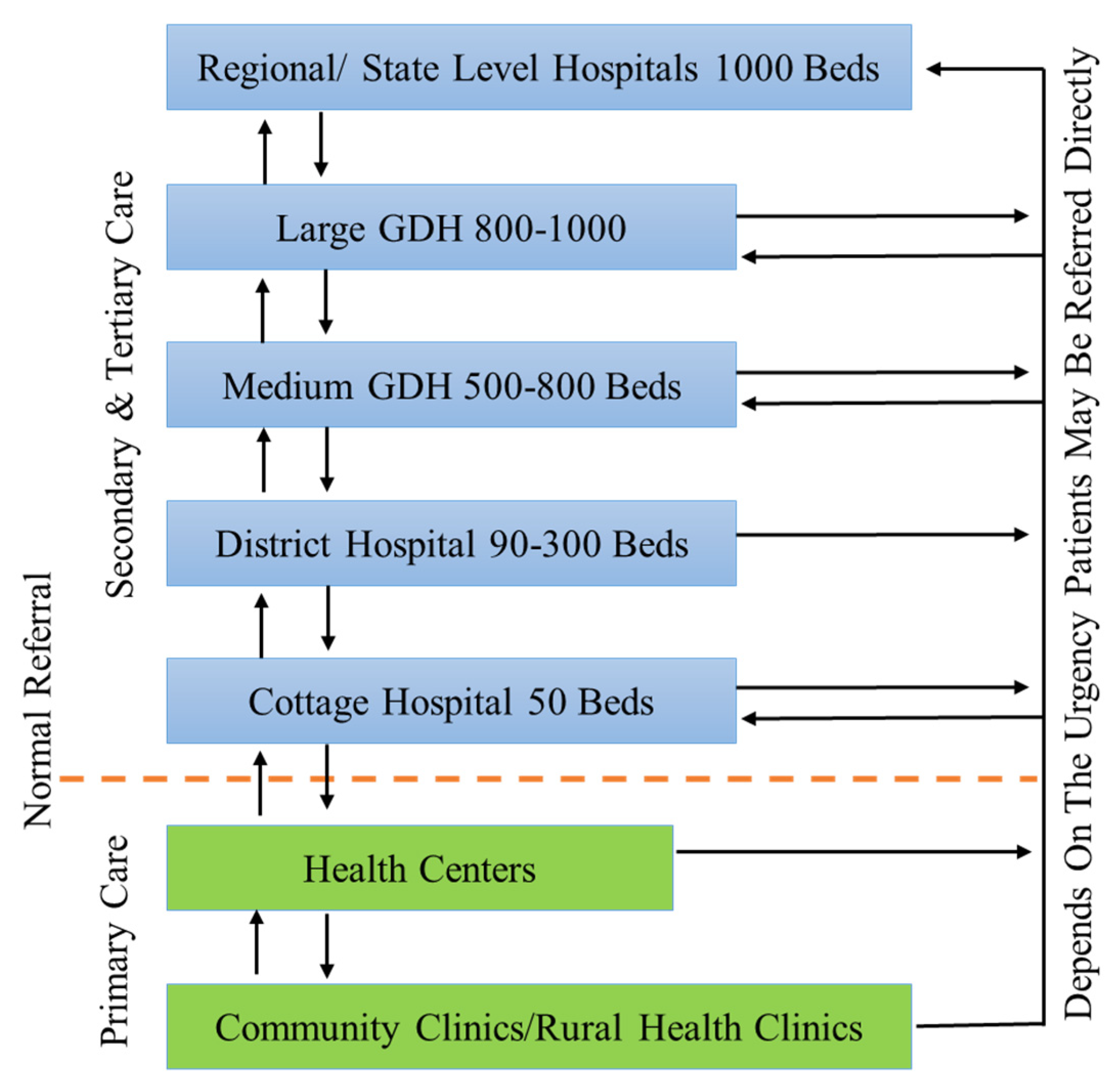
The Malaysian healthcare system has been subject to continuous development with the goal of achieving a higher-quality healthcare service. Healthcare facilities have been distributed according to the forecasted population density. According to the Malaysian Ministry of Health (MoH), the Malaysian healthcare system adopts a referral scheme [
26]. The referral scheme is divided into three phases, namely primary, secondary, and tertiary care as shown in
Figure 1. The Malaysian healthcare referral system is built upon a bottom-up sequential transfer of medical cases to other medical facilities based on the treatment requirements of the medical cases [
33]. Cases transition from widespread primary care units comprised of scattered primary care clinics to better-equipped, specialized secondary and tertiary facilities. Primary care facilities are located both in rural and urban areas. Primary care units in rural areas comprise an organized set of facilities in clinics located in the rural areas in question with the capacity to serve populations between 4000 and 5000 people within a radius of 10 km. Rural clinics refer cases to a more extensive set of healthcare facilities serving 15,000–20,000 people. However, primary care clinics function as subsidiary outpatient units in highly urbanized areas. Urban health clinics offer a consulting capacity of 500 to 1000 patients per day. Both urban and rural clinics offer thorough healthcare services, including laboratory and radiology services for the communities they serve. Patients visiting a primary healthcare clinic can then be referred to a hospital if necessary. Hospitals or secondary care centers comprise a set of hospitals that vary in terms of their size and service capacity, which ranges from 50 beds to over 1000 beds for large healthcare complexes.
Consequently, the offered services differ among hospitals depending on the needs and requirements of their locations. District hospitals are usually suitable for providing services in areas with more than 40,000 inhabitants. General District Hospitals are generally located in large states, such as Sarawak, Selangor, and Johore. General District Hospitals, in turn, refer their patients to either General State Hospitals or another Regional General Hospital, such as Penang Hospital or a National Referral Hospital in Kuala Lumpur city.
Teaching Hospitals, while under the institutional jurisdiction and management of the Ministry of Education (MoE), are a constituent of the Malaysian healthcare system and have a slightly more nuanced set of priorities geared towards learning and teaching. However, wise planning led to the use of these medical facilities to serve the populations located near them. At present, privately owned and operated healthcare facilities are not fully integrated into the national healthcare system and used in accordance with the rules and regulations of the Ministry of Health (MoH). Private healthcare facilities are normally located within urban areas and occasionally refer their cases to government hospitals. Collaboration between public and private healthcare facilities occurs in certain instances, especially when there is a need to share facilities and workforces to provide healthcare services to communities.
Despite the improvement in the Malaysian healthcare system over the past few decades, the creation of an environment that supports the healing, mental health, and wellbeing of staff, patients, and visitors has yet to be achieved in the physical, mental, and psychological domains [
26].
As Malaysia is attempting to evolve towards being a more developed nation, the quality of its healthcare facilities requires regular investigation [
18]. Since patient satisfaction and quality of life are being increasingly considered in the competitive world of healthcare, wayfinding should be a priority, especially in the pursuit of a high-quality environment for users of the Malaysian public healthcare system. Therefore, this study aimed to assess the wayfinding system of a Malaysian hospital’s outpatient unit in order to provide insights into its current state.
3. Results and Findings
The questionnaire’s scales were tested for reliability by examining the Cronbach’s alpha values for the survey results. The reliability statistics indicate a Cronbach’s alpha value of 0.845. A value of ≥0.70 is considered to be a reflection of good reliability [
36,
37].
The descriptive statistics were grouped based on the nature of the item investigated. The first section displays the responses to items of the physical environment (see
Table 2), while the second section groups the responses to items of the human-related elements listed in
Table 3.
The result on the question investigating the availability of a sufficient number of signs scored a mean response of 3.61 regarding the number of signs available in the built environment with a standard deviation of 0.686, indicating an insufficient number of available signs based on the five-point Likert scale employed in the questionnaire. Similarly, the response to the question investigating the positioning and orientation of the signage scored a mean response of 3.98 with a standard deviation of 0.529, indicating a tendency toward perceptual dissatisfaction regarding the positioning and orientation of the signage (see
Figure 5).
Regarding the legibility of the signage, the respondents averaged a score of 3.13 with a standard deviation of 0.726. Similarly, the mean score of responses to the level of color differentiation of signage against the background color was 3.85 with a standard deviation of 0.577. Regarding the legibility of text within the signage, the respondents recorded a mean response of 3.30 with a standard deviation of 0.657.
Regarding the comprehensibility or clarity of the information within the signage, the respondents recorded a mean response of 3.64 with a standard deviation of 0.699, indicating a tendency toward a low level of satisfaction with the clarity of the information within the signage available on site. However, on the question investigating whether the use of a multi-lingual signage system would positively affect the overall wayfinding experience, the mean response registered was 3.19 with a standard deviation of 0.671. This indicates a good level of agreement amongst the study’s subjects about employing a multi-lingual signage system.
Similarly, when asked about the usage of symbols in the signage system, the respondents registered an average score of 3.84 with a standard deviation of 0.624, indicating dissatisfaction with the frequency of the employment of symbols in the built environment. Moreover, when asked about the usefulness of symbols to the wayfinding system, subjects registered an average response of 3.16 with a standard deviation of 0.683. This indicates a good level of appreciation for the usage of symbols in the wayfinding system amongst the study’s subjects.
Furthermore, when asked about how sufficient the usage of maps in the built environment was, the respondents registered an average response of 4.04 with a standard deviation of 0.528, indicating dissatisfaction with the low level of usage of maps in the building. Similarly, when asked about how comprehensible the available maps were, subjects responded with an average score of 3.29 and a standard deviation of 0.663, indicating that the subjects perceived the maps available on site to be incomprehensible.
Regarding the overall organization of the interior environment, subjects responded with an average score of 3.98 and a standard deviation of 0.584, indicating dissatisfaction with the organization of the interior environment.
Finally, when asked about whether a better-designed signage system would make their journey easier when being referred from one place to another within the building or from one building to another, the respondents registered an average response of 3.57 with a standard deviation of 0.783, agreeing with this statement (see
Table 2).
The responses regarding the environmental elements indicate the need for better placement of signage, better differentiation of signage from the background, the placement of signage in more locations, as well as an improvement in the graphics and comprehensibility of the signage in general. An analysis of the users’ responses indicates that an upgrade of the overall interior environmental conditions might be required. The results suggest that this could be achieved by employing symbols instead of just text and a multi-lingual signage system, which could be useful due to the cultural diversity of the setting.
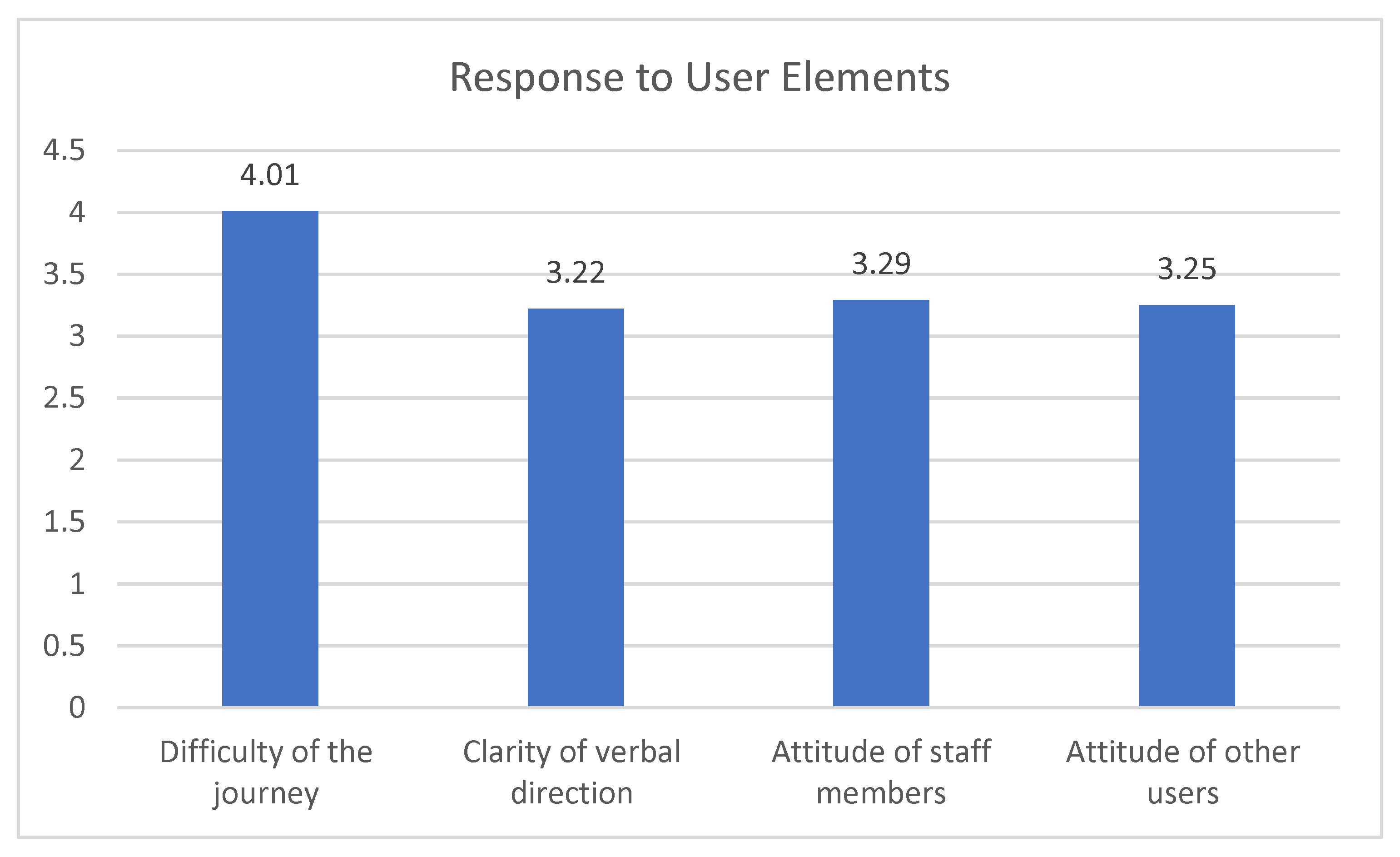
When the subjects were asked to rate the difficulty of their overall journey within the hospital, they registered an average response of 4.01 with a standard deviation of 0.512, indicating that the subjects found wayfinding within the building difficult (see
Figure 6).
Consequently, when asked about the number of times that they required assistance with wayfinding by asking for directions, the subjects registered an average response of 2.22 and a standard deviation of 0.675.
Furthermore, when asked about the clarity of the verbal direction provided to them, the subjects registered a mean response of 3.22 and a standard deviation of 0. 638, indicating that the subjects were dissatisfied with the clarity of the provided verbal direction.
When the subjects were asked to rate the attitude of staff members toward being asked for help with directions, the mean response registered was 3.29 with a standard deviation of 0.724, leaning toward a negative reaction to the attitude of staff members when asked for directions. Similarly, when asked to rate the attitude of other hospital users (patients/visitors) toward being asked for directions, the mean response was 3.25 with a standard deviation of 0.687 (see
Table 3).
Analysis of the human-related elements within the questionnaire indicated a perceived difficulty with performing wayfinding tasks in the setting and highlighted a potential outcome represented by users having to ask for directions multiple times on average during their journey within the environment. In addition, the analysis of the human-related elements demonstrated a lack of verbal clarity when giving directions and a poor attitude from both staff members and other users toward being asked for directions within the environment. This may be due to a lack of awareness on the part of users who are more familiar with the setting, such as staff members and more experienced users, about the difficulty of the wayfinding process, especially for patients who might be operating under less-than-optimal mental conditions. An institutional intervention might be required in this case to raise the level of awareness and perhaps provide training to staff members to handle such situations.
A Pearson’s correlation test was employed to statistically test the correlation between the investigated variables and subjects’ responses. This test can reveal intercorrelations, the corresponding levels of significance of these intercorrelations (sig, two-tailed), and the correlation strength. A system of assessing the strength of the relationship between variables was implemented in which correlation values are weak when they are less than 0.30, strong when they are greater than 0.50, and of medium strength when they lie in between these values [
38].
The results suggest that age is positively correlated with the subjects’ responses to all questions except for the question on environmental organization, where a negative correlation value was detected. However, the test results suggest that not all of the correlation values are statistically significant. The Sig(two-tailed) values for the questions investigating the perceived difficulty of the journey, the usage of maps, and the environmental organization did not register statistical significance based on a confidence level of 0.05. Conversely, the rest of the questions showed Sig(two-tailed) values less than 0.05, indicating a statistically significant correlation between respondents’ age and responses.
Moreover, when testing whether gender correlated with subjects’ responses, the Pearson’s correlation test results indicated a statistically significant correlation to the number of signs in the building, which registered a correlation coefficient value of 0.160, a weak positive correlation, and a Sig(two-tailed) value of 0.04. The positive coefficient value indicates a higher response score from female respondents on average. However, the correlation coefficient value suggests a weak correlation, indicating that gender does not account for much of the change in the overall response.
Furthermore, the Pearson’s correlation test indicated that LoE correlates positively with responses on the number of signs, the positioning and orientation of signage, the legibility of text on signage, the degree to which signage contrasts with the background, the clarity of information provided by signage, the usage of a multi-lingual signage system, and the usage of symbols. Each of these variables registered a statistically significant correlation (Sig(two-tailed) values of 0.003, 0.000, 0.042, 0.001, 0.001, 0.000, 0.000, 0.045, 0.002, 0.022, and 0.000, respectively). The responses on symbols’ usefulness, the number of instances where subjects required external help, dissatisfaction with the attitude of other hospital patients/visitors, and the difficulty of using the maps available on site did not register a significant correlation.
In addition, we tested whether the number of visits (NoV) correlated with subjects’ responses. The test results indicate statistically significant correlations with nine items. The correlation test registered a positive correlation between the NoV and the number of signs, the legibility of signage, the legibility of text, the clarity of information, the employment of a multi-lingual signage system, the frequency of use of symbols within the environment, the number of times that visitors required help, the clarity of verbal directions, and the attitude of other users toward being asked for directions (correlation values of (0.403, 0.246, 0.170, 0.277, 0.257, 0.170, 0.203, 0.192, and 0.171, respectively).
Moreover, the test results indicate a statistically significant negative correlation between subjects’ purpose of visit (PoV) and the overall responses. This suggests that the level of satisfaction toward the number of signs available in the building was affected by the PoV, whereby the visitors were less satisfied with the number of available signs (Sig (two-tailed) values of 0.008 and 0.018 and correlation values of −0.207 and 0.184, respectively). On the other hand, there was a positive correlation between the PoV and the response to the attitude of staff members towards being asked for directions. This finding indicates that, on average, patients were less satisfied with the attitude of staff members toward being asked for directions (a correlation value of 0.184 and a Sig(two-tailed) value of 0.018).
Furthermore, we investigated the relationship between subjects’ LoI and their responses. The test results indicate a positive, statistically significant correlation in all items except three (the perceived difficulty of the journey, the number of times subjects required assistance and asked for directions, and the organization of the interior environment). Moreover, no statistically significant correlation was found between respondents’ ethnic background and their responses to all of the items investigated in the questionnaire.
Lastly, when investigating the relationship between the respondents’ LoP and their responses, no significant correlation was found in the responses to all of the questions except for the questions on the difficulty of the overall journey through the building and the number of times the respondents required help. Correlation values of −0.180 and −0.165 and Sig(two-tailed) values of 0.021 and 0.034 were obtained, indicating that respondents’ LoP is inversely correlated to the response to these questions. In both cases, the correlation values were less than 0.3, indicating a weak relationship between the respondents’ ethnic background and their responses as listed in
Table 4.
The correlation test results indicate that, while the responses to various elements varied amongst demographic groups, the coefficient values show an overall homogenous response to the items investigated. This suggests that the variables studied had a similar overall impact on the various groups, with a few exceptions for specific items.
Table 4 shows that the registered correlation coefficients were all greater than 0.3 and no group registered a correlation coefficient greater than 0.5.


 ,
, 


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}