
An Integrated Conceptual Model to Understand Suicidality among Queer Youth to Inform Suicide Prevention

 ,
, {kind=link}
Abstract
1. An Introduction to Youth Suicidality in the United States
2. Queer Youth Suicidality
3. Need for a Conceptual Model on Suicidality among Queer Youth
4. Theories and Conceptual Frameworks to Understand Suicidality among Queer Youth
4.1. Minority Stress Theory (MST)
4.2. Person-in-Environment and Risk and Resilience (PIE-R&R) Framework
4.3. Interpersonal-Psychological Theory of Suicide (IPTS)
4.4. Intersectionality Framework
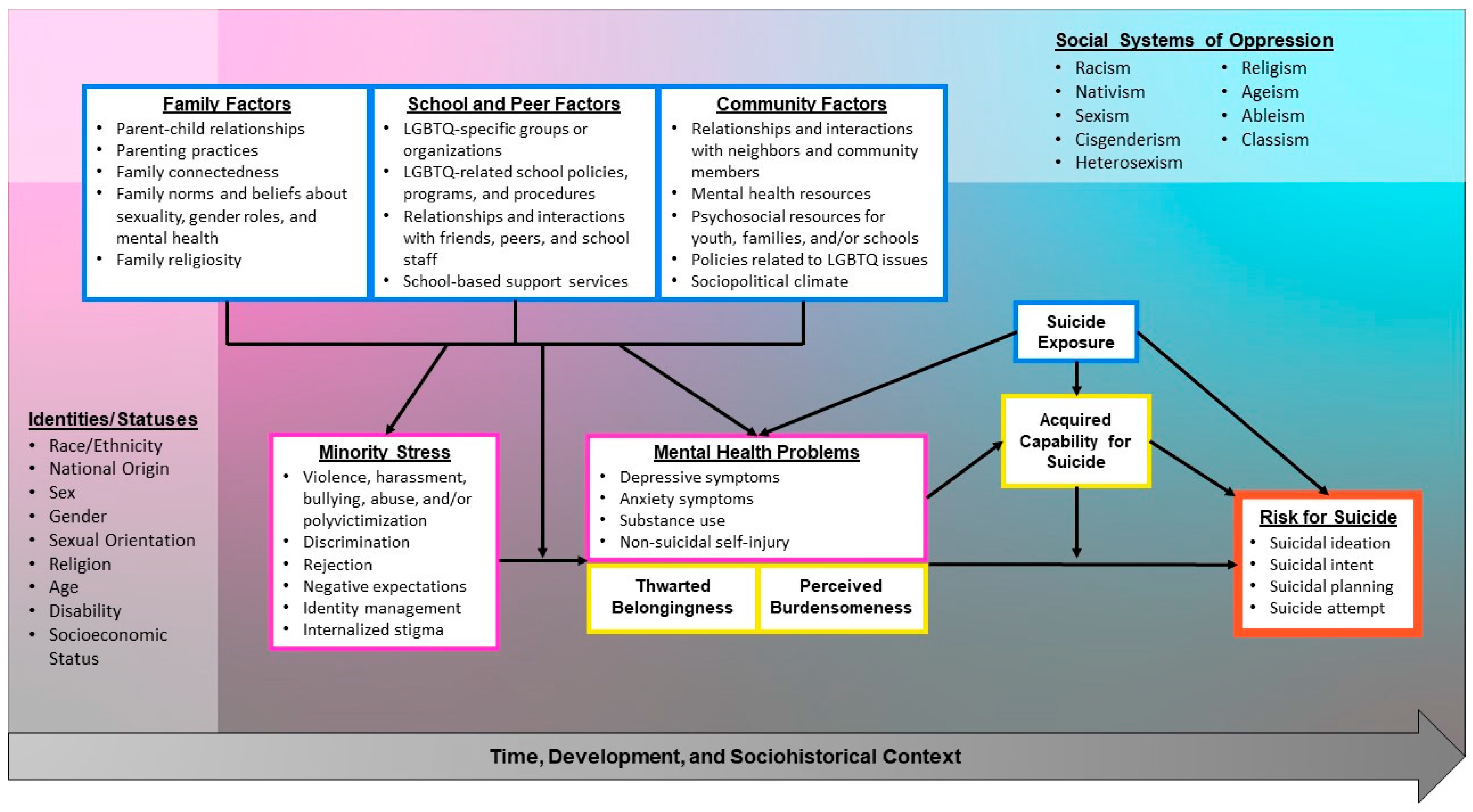
5. An Integrated Conceptual Model to Understand Suicidality among Queer Youth
5.1. Minority Stress
5.1.1. Violence, Polyvictimization, and Abuse
5.1.2. Discrimination, Rejection, Negative Expectations, and Identity Management
5.1.3. Internalized Stigma
5.2. Interpersonal and Psychological Factors of Suicide Risk
5.2.1. Mental Health Problems
5.2.2. Thwarted Belongingness and Perceived Burdensomeness
5.3. Socioecological Factors
5.3.1. Family Factors
5.3.2. School and Peer Factors
5.3.3. Community Factors
5.3.4. Suicide Exposure and Acquired Capability for Suicide
5.4. Intersectionality: Identities and Systems of Oppression
6. Discussion
6.1. Implications for Research and Policy
6.2. Implications for Practice
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Appendix A

References
- Ertl, A.; Crosby, A.E.; Blair, J.M. Youth suicide: An opportunity for prevention. J. Am. Acad. Child Adolesc. Psychiatry 2020, 59, 1019–1021. [Google Scholar] [CrossRef]
- Hawkins, J.D.; Jenson, J.M.; Catalano, R.; Fraser, M.W.; Botvin, G.J.; Shapiro, V.; Hendricks Brown, C.; Beardslee, W.; Brent, D.; Leslie, L.K.; et al. Unleashing the Power of Prevention; National Academy of Medicine: Washington, DC, USA, 2015. [Google Scholar]
- Centers for Disease Control & Prevention. Preventing Suicide. 2021. Available online: https://www.cdc.gov/suicide/pdf/preventing-suicide-factsheet-2021-508.pdf (accessed on 23 May 2022).
- Elfein, J. Distribution of the 10 Leading Causes of Death among Teenagers Aged 15 to 19 Years in the United States in 2019. Statista, 2021. Available online: https://www.statista.com/statistics/1017959/distribution-of-the-10-leading-causes-of-death-among-teenagers/ (accessed on 23 May 2022).
- Ramchand, R.; Gordon, J.A.; Pearson, J.L. Trends in suicide rates by race and ethnicity in the United States. JAMA Netw. Open 2021, 4, e2111563. [Google Scholar] [CrossRef]
- Kohlbeck, S.; Hargarten, S.; Cassidy, L.D. Age- and sex-specific risk factors for youth suicide: A mixed methods review. Wis. Med. J. 2020, 119, 165–170. [Google Scholar]
- Alvarez, K.; Polanco-Roman, L.; Samuel Breslow, A.; Molock, S. Structural racism and suicide prevention for ethnoracially minoritized youth: A conceptual framework and illustration across systems. Am. J. Psychiatry 2022, 179, 422–433. [Google Scholar] [CrossRef]
- Braudt, D.B.; Lawrence, E.M.; Tilstra, A.M.; Rogers, R.G.; Hummer, R.A. Family socioeconomic status and early life mortality risk in the United States. Matern. Child Health J. 2019, 23, 1382–1391. [Google Scholar] [CrossRef] [PubMed]
- Gordon, J. Addressing the Crisis of Black Youth Suicide; National Institute of Mental Health: Bethesda, MD, USA, 2020. Available online: https://www.nimh.nih.gov/about/director/messages/2020/addressing-the-crisis-of-black-youth-suicide (accessed on 28 February 2022).
- Yildiz, M.; Orak, U.; Walker, M.H.; Solakoglu, O. Suicide contagion, gender, and suicide attempts among adolescents. Death Stud. 2019, 43, 365–371. [Google Scholar] [CrossRef]
- Conron, K.J. LGBT Youth Population in the United States; University of California, Los Angeles Williams Institute School of Law: Los Angeles, CA, USA, 2020; Available online: https://williamsinstitute.law.ucla.edu/wp-content/uploads/LGBT-Youth-US-Pop-Sep-2020.pdf (accessed on 23 February 2022).
- Adelson, S.L.; Graeme, R.; Miller, A.M.; Sandfort, T.G.M. Health justice for LGBT youths: Combining public health and human rights. J. Am. Acad. Child Adolesc. Psychiatry 2021, 60, 804–807. [Google Scholar] [CrossRef]
- Toomey, R.B.; Syvertsen, A.K.; Shramko, M. Transgender adolescent suicide behavior. Pediatrics 2018, 142, e20174218. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. 1991–2019 High School Youth Risk Behavior Survey Data. 2019. Available online: http://nccd.cdc.gov/youthonline (accessed on 18 August 2022).
- Johns, M.M.; Lowry, R.; Andrzejewski, J.; Barrios, L.C.; Demissie, Z.; Rasberry, C.N.; Robin, L.; Underwood, J.M. Transgender identity and experiences of violence victimization, substance use, suicide risk, and sexual risk behaviors among high school students—19 States and Large Urban School Districts, 2017. Morb. Mortal. Wkly. Rep. 2019, 68, 67–71. [Google Scholar] [CrossRef] [PubMed]
- Horwitz, A.G.; Grupp-Phelan, J.; Brent, D.; Barney, B.J.; Casper, T.C.; Berona, J.; Chernick, L.S.; Shenoi, R.; Cwik, M.; King, C.A. Risk and protective factors for suicide among sexual minority youth seeking emergency medical services. J. Affect. Disord. 2021, 279, 274–281. [Google Scholar] [CrossRef]
- Nock, M.K.; Borges, G.; Bromet, E.J.; Cha, C.B.; Kessler, R.C.; Lee, S. Suicide and suicidal behavior. Epidemiol. Rev. 2008, 30, 133–154. [Google Scholar] [CrossRef]
- Singer, J.B.; Erbacher, T.A.; Rosen, P. School-based suicide prevention: A framework for evidence-based practice. School Ment. Health 2019, 11, 54–71. [Google Scholar] [CrossRef]
- The Trevor Project. National Survey on LGBTQ Youth Mental Health 2021. 2021. Available online: https://www.thetrevorproject.org/survey-2021/?section=SuicideMentalHealth (accessed on 28 February 2022).
- Borgogna, N.C.; McDermott, R.C.; Aita, S.L.; Kridel, M.M. Anxiety and depression across gender and sexual minorities: Implications for transgender, gender nonconforming, pansexual, demisexual, asexual, queer, and questioning individuals. Psychol. Sex. Orientat. Gend. Divers. 2019, 6, 54–63. [Google Scholar] [CrossRef]
- Tejera, C.H.; Horner-Johnson, W.; Andresen, E.M. Application of an intersectional framework to understanding the association of disability and sexual orientation with suicidal ideation among Oregon teens. Disabil. Health J. 2019, 12, 557–563. [Google Scholar] [CrossRef]
- Dawes, H.C.; Williams, D.Y.; Klein, L.B.; Hirst, L.E.; Forte, A.B.; Gibbs, D.J.; Hall, W.J. Experiences of LGBTQ POC in mental health services and substance abuse: A systematic review. J. Soc. Soc. Work Res. 2022. [Google Scholar] [CrossRef]
- Hughes, E.; Rawlings, V.; McDermott, E. Mental health staff perceptions and practice regarding self-harm, suicidality and help-seeking in LGBTQ youth: Findings from a cross-sectional survey in the UK. Issues Ment. Health Nurs. 2018, 39, 30–36. [Google Scholar] [CrossRef]
- Galster, G.; Sharkey, P. Spatial foundations of inequality: A conceptual model and empirical overview. Russell Sage Found. J. Soc. Sci. 2017, 3, 1–33. Available online: https://www.jstor.org/stable/10.7758/rsf.2017.3.2.01 (accessed on 6 June 2022). [CrossRef]
- Barth, R.P.; Messing, J.T.; Shanks, T.R.; Williams, J.H. (Eds.) Grand Challenges for Social Work and Society, 2nd ed.; Oxford University Press: New York, NY, USA, 2022. [Google Scholar]
- Hatchel, T.; Polanin, J.R.; Espelage, D.L. Suicidal thoughts and behaviors among LGBTQ youth: Meta-analyses and a systematic review. Arch. Suicide Res. 2021, 25, 1–37. [Google Scholar] [CrossRef]
- Price-Feeney, M.; Green, A.E.; Dorison, S. Understanding the mental health of transgender and nonbinary youth. J. Adolesc. Health 2020, 66, 684–690. [Google Scholar] [CrossRef]
- Thoma, B.C.; Salk, R.H.; Choukas-Bradley, S.; Goldstein, T.R.; Levine, M.D.; Marshal, M.P. Suicidality disparities between transgender and cisgender adolescents. Pediatrics 2019, 144, e20191183. [Google Scholar] [CrossRef]
- Hirsch, J.K.; Cohn, T.K.; Rowe, C.A.; Rimmer, S.E. Minority sexual orientation, gender identity status and suicidal behavior: Serial indirect effects of hope, hopelessness and depressive symptoms. Int. J. Ment. Health Addict. 2017, 15, 260–270. [Google Scholar] [CrossRef]
- Kang, N.; You, J.; Huang, J.; Ren, Y.; Lin, M.-P.; Xu, S. Understanding the pathways from depression to suicidal risk from the perspective of the interpersonal–psychological theory of suicide. Suicide Life-Threat. Behav. 2018, 49, 684–694. [Google Scholar] [CrossRef] [PubMed]
- Franklin, J.C.; Ribeiro, J.D.; Fox, K.R.; Bentley, K.H.; Kleiman, E.M.; Huang, X.; Musacchio, K.M.; Jaroszewski, A.C.; Chang, B.P.; Nock, M.K. Risk factors for suicidal thoughts and behaviors: A meta-analysis of 50 years of research. Psychol. Bull. 2017, 143, 187–232. [Google Scholar] [CrossRef]
- Meyer, I.H. Minority stress and mental health in gay men. J. Health Soc. Behav. 1995, 36, 38–56. [Google Scholar] [CrossRef] [PubMed]
- Meyer, I.H. Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: Conceptual issues and research evidence. Psychol. Bull. 2003, 129, 674–697. [Google Scholar] [CrossRef]
- Hall, W.J.; Lanier, P.; Jenson, J.M.; Fraser, M.W. A multisystems risk and resilience approach to social policy for children, youth, and families. In Social Policy for Children and Families: A Risk and Resilience Perspective, 4th ed.; Hall, W.J., Lanier, P., Jenson, J.M., Fraser, M.W., Eds.; Sage: New York, NY, USA, 2022; pp. 1–26. [Google Scholar]
- Joiner, T.E. Why People Die by Suicide; Harvard University Press: Cambridge, MA, USA, 2005. [Google Scholar]
- Crenshaw, K. Mapping the margins: Intersectionality, identity politics, and violence against women of color. Stanf. Law Rev. 1990, 43, 1241. [Google Scholar] [CrossRef]
- Hendricks, M.L.; Testa, R.J. A conceptual framework for clinical work with transgender and gender nonconforming clients: An adaptation of the Minority Stress Model. Prof. Psychol. Res. Pract. 2012, 43, 460. [Google Scholar] [CrossRef]
- Fulginiti, A.; Goldbach, J.T.; Mamey, M.R.; Rusow, J.; Srivastava, A.; Rhoades, H.; Schrager, S.M.; Bond, D.W.; Marshal, M.P. Integrating minority stress theory and the interpersonal theory of suicide among sexual minority youth who engage crisis services. Suicide Life-Threat. Behav. 2020, 50, 601–616. [Google Scholar] [CrossRef]
- Goldbach, J.T.; Schrager, S.M.; Mamey, M.R. Criterion and divergent validity of the Sexual Minority Adolescent Stress Inventory. Front. Psychol. 2017, 8, 2057. [Google Scholar] [CrossRef]
- Goldbach, J.T.; Schrager, S.M.; Mamey, M.R.; Rhoades, H. Confirming the reliability and validity of the Sexual Minority Adolescent Stress Inventory in a national sample of sexual minority adolescents. Front. Psychol. 2021, 12, 720199. [Google Scholar] [CrossRef]
- Goldbach, J.T.; Gibbs, J.J. A developmentally informed adaptation of minority stress for sexual minority adolescents. J. Adolesc. 2017, 55, 36–50. [Google Scholar] [CrossRef]
- Hoy-Ellis, C.P. Minority stress and mental health: A review of the literature. J. Homosex. 2021, 1–25. [Google Scholar] [CrossRef]
- Kondrat, M.E. Person-in-environment. In Oxford Research Encyclopedia of Social Work; Franklin, C., Ed.; National Association of Social Workers Press: Washington, DC, USA; Oxford University Press: Oxford, UK, 2013. [Google Scholar]
- Hatzenbuehler, M.L. The social environment and suicide attempts in lesbian, gay, and bisexual youth. Pediatrics 2011, 127, 896–903. [Google Scholar] [CrossRef]
- Fraser, M.W. The ecology of childhood: A multisystems perspective. In Risk and Resilience in Childhood, 2nd ed.; Fraser, M.W., Ed.; NASW Press: Washington, DC, USA, 2004; pp. 1–12. [Google Scholar]
- Fraser, M.W.; Richman, J.M.; Galinsky, M.J. Risk, protection, and resilience: Towards a conceptual framework for social work practice. Soc. Work Res. 1999, 23, 131–144. [Google Scholar] [CrossRef]
- Fraser, M.W.; Kirby, L.D.; Smokowski, P.R. Risk and resilience in childhood. In Risk and Resilience in Childhood: An Ecological Perspective, 2nd ed.; Fraser, M.W., Ed.; NASW Press: Washington, DC, USA, 2004; pp. 13–66. [Google Scholar]
- Fraser, M.W.; Terzian, M.A. Risk and resilience in child development: Practice principles and strategies. In Handbook of Children, Youth, and Family Services: Practice, Policies, and Programs; Mallon, G.P., Hess, P.M., Eds.; Columbia University Press: New York, NY, USA, 2005; pp. 55–71. [Google Scholar]
- Diamond, G.; Kodish, T.; Ewing ES, K.; Hunt, Q.A.; Russon, J.M. Family processes: Risk, protective and treatment factors for youth at risk for suicide. Aggress. Violent Behav. 2022, 64, 101586. [Google Scholar] [CrossRef]
- Joiner, T.E.; Jeon, M.E.; Lieberman, A.; Janakiraman, A.; Duffy, M.E.; Gai, A.R.; Dougherty, S.P. On prediction, refutation, and explanatory reach: A consideration of the interpersonal theory of suicidal behavior. Prev. Med. 2021, 152, 106453. [Google Scholar] [CrossRef]
- Calear, A.L.; McCallum, S.; Kazan, D.; Werner-Seidler, A.; Christensen, H.; Batterham, P.J. Application of the interpersonal psychological theory of suicide in a non-clinical community-based adolescent population. J. Affect. Disord. 2021, 294, 235–240. [Google Scholar] [CrossRef] [PubMed]
- Grossman, A.H.; Park, J.Y.; Russell, S.T. Transgender youth and suicidal behaviors: Applying the interpersonal psychological theory of suicide. J. Gay Lesbian Ment. Health 2016, 20, 329–349. [Google Scholar] [CrossRef] [PubMed]
- Bryan, C.J.; Butner, J.E.; May, A.M.; Rugo, K.F.; Harris, J.; Oakey, D.N.; Rozek, D.C.; Bryan, A.O. Nonlinear change processes and the emergence of suicidal behavior: A conceptual model based on the fluid vulnerability theory of suicide. New Ideas Psychol. 2021, 57, 1–22. [Google Scholar] [CrossRef]
- Buchmann-Schmitt, J.M.; Chiurliza, B.; Chu, C.; Michaels, M.S.; Joiner, T.E. Suicidality in adolescent populations: A review of the extant literature through the lens of the interpersonal theory of suicide. Int. J. Behav. Consult. Ther. 2014, 9, 26–34. [Google Scholar] [CrossRef]
- O’Connor, R.C.; Kirtley, O.J. The integrated motivational-volitional model of suicidal behaviour. Philos. Trans. R. Soc. B 2018, 373, 20170268. [Google Scholar] [CrossRef] [PubMed]
- Bowleg, L. The problem with the phrase women and minorities: Intersectionality—An important theoretical framework for public health. Am. J. Public Health 2012, 102, 1267–1273. [Google Scholar] [CrossRef]
- Collins, P.H. Intersectionality’s definitional dilemmas. Ann. Rev. Sociol. 2015, 41, 1–20. [Google Scholar] [CrossRef]
- Garcia, B.; Van Soest, D. Oppression. In Encyclopedia of Social Work; Franklin, C., Ed.; National Association of Social Workers Press: Washington, DC, USA; Oxford University Press: Oxford, UK, 2019. [Google Scholar]
- Young, I.M. Five faces of oppression. In Readings for Diversity and Social Justice, 4th ed.; Adams, M., Blumenfeld, W.J., Catalano, D.C.J., DeJong, K.S., Hackman, H.W., Hopkins, L.E., Love, B.J., Peters, M.L., Shlasko, D., Zuniga, X., Eds.; Routledge: London, UK, 2018; pp. 49–58. [Google Scholar]
- Shangani, S.; Gamarel, K.E.; Ogunbajo, A.; Cai, J.; Operario, D. Intersectional minority stress disparities among sexual minority adults in the USA: The role of race/ethnicity and socioeconomic status. Cult. Health Sex. 2020, 22, 398–412. [Google Scholar] [CrossRef] [PubMed]
- Williams, S.L.; Job, S.A.; Todd, E.; Braun, K. A critical deconstructed quantitative analysis: Sexual and gender minority stress through an intersectional lens. J. Soc. Issues 2020, 76, 859–879. [Google Scholar] [CrossRef]
- Johns, M.M.; Lowry, R.; Hipp, T.N.; Robin, L.; Shafir, S. Differences in adolescent experiences of polyvictimization and suicide risk by sexual minority status. J. Res. Adolesc. 2021, 31, 240–252. [Google Scholar] [CrossRef]
- Green, A.E.; Price-Feeney, M.N.; Dorison, S.H. Cumulative minority stress and suicide risk among LGBTQ youth. Am. J. Community Psychol. 2022, 69, 157–168. [Google Scholar] [CrossRef] [PubMed]
- Kassing, F.; Casanova, T.; Griffin, J.A.; Wood, E.; Stepleman, L.M. The effects of polyvictimization on mental and physical health outcomes in an LGBTQ sample. J. Trauma. Stress 2021, 34, 161–171. [Google Scholar] [CrossRef]
- Sterzing, P.R.; Gartner, R.E.; Goldbach, J.T.; McGeough, B.L.; Ratliff, G.A.; Johnson, K.C. Polyvictimization prevalence rates for sexual and gender minority adolescents: Breaking down the silos of victimization research. Psychol. Violence 2019, 9, 419–430. [Google Scholar] [CrossRef]
- Interagency Working Group on Youth Programs. Child Welfare. In Youth.Gov.; 2015. Available online: https://youth.gov/youth-topics/lgbtq-youth/child-welfare#_ftn (accessed on 10 February 2022).
- Scheer, J.R.; Edwards, K.M.; Helminen, E.C.; Watson, R.J. Victimization typologies among a large national sample of sexual and gender minority adolescents. LGBT Health 2021, 8, 507–518. [Google Scholar] [CrossRef]
- Gibbs, J.J.; Goldbach, J. Religious conflict, sexual identity, and suicidal behaviors among LGBT young adults. Arch. Suicide Res. 2015, 19, 472–488. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.J.; Kellerman, J.; Feinstein, B.A.; Selby, E.A.; Goldbach, J.T. Greater minority stress is associated with lower intentions to disclose suicidal thoughts among LGBTQ plus youth. Arch. Suicide Res. 2022, 26, 626–640. [Google Scholar] [CrossRef] [PubMed]
- Dyar, C.; Feinstein, B.A.; Sarno, E.L.; Pirog, S.; Newcomb, M.E.; Whitton, S.W. Prospective associations between bi+ minority stressors and internalizing symptoms: The mediating roles of general and group-specific processes. J. Consult. Clin. Psychol. 2021, 89, 845–855. [Google Scholar] [CrossRef]
- Chodzen, G.; Hidalgo, M.A.; Chen, D.; Garofalo, R. Minority stress factors associated with depression and anxiety among transgender and gender-nonconforming youth. J. Adolesc. Health 2019, 64, 467–471. [Google Scholar] [CrossRef] [PubMed]
- Jackman, K.B.; Dolezal, C.; Bockting, W.O. Generational differences in internalized transnegativity and psychological distress among feminine spectrum transgender people. LGBT Health 2018, 5, 54–60. [Google Scholar] [CrossRef]
- Hall, W.J. Psychosocial risk and protective factors for depression among lesbian, gay, bisexual, and queer youth: A systematic review. J. Homosex. 2018, 65, 263–316. [Google Scholar] [CrossRef]
- Taliaferro, L.A.; Muehlenkamp, J.J. Risk and protective factors that distinguish adolescents who attempt suicide from those who only consider suicide in the past year. Suicide Life-Threat. Behav. 2014, 44, 6–22. [Google Scholar] [CrossRef]
- Rogers, M.L.; Joiner, T.E. Rumination, suicidal ideation, and suicide attempts: A meta-analytic review. Rev. Gen. Psychol. 2017, 21, 132–142. [Google Scholar] [CrossRef]
- Timmins, L.; Rimes, K.A.; Rahman, Q. Minority stressors, rumination, and psychological distress in lesbian, gay, and bisexual individuals. Arch. Sex. Behav. 2020, 49, 661–680. [Google Scholar] [CrossRef]
- O’Loughlin, C.M.; Gomer, B.; Ammerman, B.A. The social context of nonsuicidal self-injury: Links to severity, suicide risk, and social factors. J. Clin. Psychol. 2021, 77, 1004–1017. [Google Scholar] [CrossRef]
- Gay, Lesbian & Straight Education Network. The Safe Space Kit: Guide to Being an Ally to LGBT Students. 2016. Available online: https://www.glsen.org/sites/default/files/GLSEN%20Safe%20Space%20Kit.pdf (accessed on 19 October 2022).
- Chang, C.J.; Feinstein, B.A.; Fulginiti, A.; Dyar, C.; Selby, E.A.; Goldbach, J.T. A longitudinal examination of the interpersonal theory of suicide for predicting suicidal ideation among LGBTQ+ youth who utilize crisis services: The moderating effect of gender. Suicide Life-Threat. Behav. 2021, 51, 1015–1025. [Google Scholar] [CrossRef] [PubMed]
- Chu, C.; Buchman-Schmitt, J.M.; Stanley, I.H.; Hom, M.A.; Tucker, R.P.; Hagan, C.R.; Rogers, M.L.; Podlogar, M.C.; Chiurliza, B.; Ringer, F.B.; et al. The interpersonal theory of suicide: A systematic review and meta-analysis of a decade of cross-national research. Psychol. Bull. 2017, 143, 1313–1345. [Google Scholar] [CrossRef]
- Almeida, J.; Johnson, R.M.; Corliss, H.L.; Molnar, B.E.; Azrael, D. Emotional distress among LGBT youth: The influence of perceived discrimination based on sexual orientation. J. Youth Adolesc. 2009, 38, 1001–1014. [Google Scholar] [CrossRef]
- Mustanski, B.; Liu, R.T.A. Longitudinal study of predictors of suicide attempts among lesbian, gay, bisexual, and transgender youth. Arch. Sex. Behav. 2013, 42, 437–448. [Google Scholar] [CrossRef]
- Gorse, M. Risk and protective factors to LGBTQ+ youth suicide: A review of the literature. Child Adolesc. Soc. Work J. 2020, 39, 17–28. [Google Scholar] [CrossRef]
- Katz-Wise, S.L.; Sarda, V.; Austin, S.B.; Harris, S.K. Longitudinal effects of gender minority stressors on substance use and related risk and protective factors among gender minority adolescents. PLoS ONE 2021, 16, e0250500. [Google Scholar] [CrossRef]
- Kidd, S.; Henrich, C.C.; Brookmeyer, K.A.; Davidson, L.; King, R.A.; Shahar, G. The social context of adolescent suicide attempts: Interactive effects of parent, peer, and school social relations. Suicide Life-Threat. Behav. 2006, 36, 386–395. [Google Scholar] [CrossRef]
- Ryan, C.; Russell, S.T.; Huebner, D.; Diaz, R.; Sanchez, J. Family acceptance in adolescence and the health of LGBT young adults. J. Child Adolesc. Psychiatr. Nurs. 2010, 23, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Whitlock, J.; Wyman, P.A.; Moore, S.R. Connectedness and suicide prevention in adolescents: Pathways and implications. Suicide Life-Threat. Behav. 2014, 44, 246–272. [Google Scholar] [CrossRef]
- Puckett, J.A.; Horne, S.G.; Surace, F.; Carter, A.; Noffsinger-Frazier, N.; Shulman, J.; Detrie, P.; Ervin, A.; Mosher, C. Predictors of sexual minority youth’s reported suicide attempts and mental health. J. Homosex. 2017, 64, 697–715. [Google Scholar] [CrossRef]
- Schmitz, R.M.; Robinson, B.A.; Sanchez, J. Intersectional family systems approach: LGBTQ+ Latino/a youth, family dynamics, and stressors. Fam. Relat. 2020, 69, 832–848. [Google Scholar] [CrossRef]
- McKay, T.; Berzofsky, M.; Landwehr, J.; Hsieh, P.; Smith, A. Suicide etiology in youth: Differences and similarities by sexual and gender minority status. Child. Youth Serv. Rev. 2019, 102, 79–90. [Google Scholar] [CrossRef]
- Mereish, E.H.; Cox, D.J.; Harris, J.C.; Anderson, Q.R. Emerging ideas: Familial influences, shame, guilt, and depression among sexual minority adolescents. Fam. Relat. 2021, 70, 1546–1555. [Google Scholar] [CrossRef]
- Gattis, M.N.; Woodford, M.R.; Han, Y. Discrimination and depressive symptoms among sexual minority youth: Is gay-affirming religious affiliation a protective factor? Arch. Sex. Behav. 2014, 43, 1589–1599. [Google Scholar] [CrossRef]
- Blosnich, J.R.; Henderson, E.R.; Coulter, R.W.S.; Goldbach, J.T.; Meyer, I.H. Sexual orientation change efforts, adverse childhood experiences, and suicide ideation and attempt among sexual minority adults, United States, 2016–2018. Am. J. Public Health 2020, 110, 1024–1030. [Google Scholar] [CrossRef]
- Ryan, C.; Toomey, R.B.; Diaz, R.M.; Russell, S.T. Parent-initiated sexual orientation change efforts with LGBT adolescents: Implications for young adult mental health and adjustment. J. Homosex. 2018, 67, 159–173. [Google Scholar] [CrossRef]
- Anderson, O.S.; McGuire, J.K. “I feel like God doesn’t like me”: Faith and ambiguous loss among transgender youth. Fam. Relat. 2021, 70, 390–401. [Google Scholar] [CrossRef]
- Green, A.E.; Price-Feeney, M.; Dorison, S.H. Association of sexual orientation acceptance with reduced suicide attempts among lesbian, gay, bisexual, transgender, queer, and questioning youth. LGBT Health 2020, 8, 26–31. [Google Scholar] [CrossRef]
- Caputi, T.L.; Shover, C.L.; Watson, R.J. Physical and sexual violence among gay, lesbian, bisexual, and questioning adolescents. JAMA Pediatr. 2020, 174, 791–793. [Google Scholar] [CrossRef]
- Gordon, A.R.; Conron, K.J.; Calzo, J.P.; White, M.T.; Reisner, S.L.; Austin, S.B. Gender expression, violence, and bullying victimization: Findings from probability samples of high school students in 4 U.S. school districts. J. School Health 2018, 88, 306–314. [Google Scholar] [CrossRef]
- Garcia, J.; Vargas, N.; Clark, J.L.; Magaña Álvarez, M.; Nelons, D.A.; Parker, R.G. Social isolation and connectedness as determinants of well-being: Global evidence mapping focused on LGBTQ youth. Glob. Public Health 2020, 15, 497–519. [Google Scholar] [CrossRef] [PubMed]
- Day, J.K.; Fish, J.N.; Grossman, A.H.; Russell, S.T. Gay-straight alliances, inclusive policy, and school climate: LGBTQ youths’ experiences of social support and bullying. J. Res. Adolesc. 2020, 30, 418–430. [Google Scholar] [CrossRef] [PubMed]
- Kosciw, J.G.; Palmer, N.A.; Kull, R.M.; Greytak, E.A. The effect of negative school climate on academic outcomes for LGBT youth and the role of in-school supports. J. School Violence 2013, 12, 45–63. [Google Scholar] [CrossRef]
- Marx, R.A.; Kettrey, H.H. Gay-straight alliances are associated with lower levels of school-based victimization of LGBTQ+ youth: A systematic review and meta-analysis. J. Youth Adolesc. 2016, 45, 1269–1282. [Google Scholar] [CrossRef] [PubMed]
- Hatchel, T.; Espelage, D.L.; Huang, Y. Sexual harassment victimization, school belonging, and depressive symptoms among LGBTQ adolescents: Temporal insights. Am. J. Orthopsychiatr. 2018, 88, 422–430. [Google Scholar] [CrossRef]
- Kiekens, W.; La Roi, C.; Bos HM, W.; Kretschmer, T.; Van Bergen, D.D.; Veenstra, R. Explaining health disparities between heterosexual and LGB adolescents by integrating the minority stress and psychological mediation frameworks: Findings from the TRAILS study. J. Youth Adolesc. 2020, 49, 1767–1782. [Google Scholar] [CrossRef]
- Poteat, V.P.; Sinclair, K.O.; DiGiovanni, C.D.; Koenig, B.W.; Russell, S.T. Gay-straight alliances are associated with student health: A multischool comparison of LGBTQ and heterosexual youth. J. Res. Adolesc. 2013, 23, 319–330. [Google Scholar] [CrossRef]
- Marraccini, M.E.; Brier, Z.M. School connectedness and suicidal thoughts and behaviors: A systematic meta-analysis. School Psychol. Q. 2017, 32, 5. [Google Scholar] [CrossRef]
- Poland, S.; Lieberman, R.; Niznik, M. Suicide Contagion and Clusters—Part 1: What School Psychologists Should Know. Communiqué 2019, 47, 21–23. Available online: https://www.nasponline.org/publications/periodicals/communique/issues/volume-47-issue-5/suicide-contagion-and-clusters%E2%80%94part-1-what-school-psychologists-should-know (accessed on 23 March 2020).
- Davies, R.D.; Kessel, B. Gender minority stress, depression, and anxiety in a transgender high school student. Am. J. Psychiatry 2017, 174, 1151–1152. [Google Scholar] [CrossRef]
- Abrutyn, S.; Mueller, A.S. Are suicidal behaviors contagious in adolescence? Using longitudinal data to examine suicide suggestion. Am. Sociol. Rev. 2014, 79, 211–227. [Google Scholar] [CrossRef]
- Abrutyn, S.; Mueller, A.S.; Osborne, M. Rekeying cultural scripts for youth suicide: How social networks facilitate suicide diffusion and suicide clusters following exposure to suicide. Soc. Ment. Health 2020, 10, 112–135. [Google Scholar] [CrossRef]
- Poland, S.; Ferguson, S. Youth suicide in the school context. Aggress. Violent Behav. 2021, 16, 101579. [Google Scholar] [CrossRef]
- Fontanella, C.A.; Hiance-Steelesmith, D.L.; Phillips, G.S.; Bridge, J.A.; Lester, N.; Sweeney, H.A.; Campo, J.V. Widening rural-urban disparities in youth suicides, United States, 1996–2010. JAMA Pediatr. 2015, 169, 466–473. [Google Scholar] [CrossRef]
- Randall, J.R.; Nickel, N.C.; Colman, I. Contagion from peer suicidal behavior in a representative sample of American adolescents. J. Affect. Disord. 2015, 186, 219–225. [Google Scholar] [CrossRef]
- O’Neill, J.C. Are Schools Prepared for Suicide Contagion Effects? An Analysis of School Psychologists’ Perceive Competency in Postvention Response. (UMI No. 10791912). Ph.D. Thesis, University of North Carolina at Chapel Hill, Chapel Hill, NC, USA, 2017. [Google Scholar]
- Siegel, M. Everyone Needs Broadband Access—Especially LGBTQ Youth; New America: Washington, DC, USA, 2021; Available online: https://www.newamerica.org/oti/blog/everyone-needs-broadband-access-especially-lgbtq-youth/ (accessed on 10 March 2022).
- Marchant, A.; Hawton, K.; Stewart, A.; Montgomery, P.; Singaravelu, V.; Lloyd, K.; Purdy, N.; Daine, K.; John, A. A systematic review of the relationship between internet use, self-harm and suicidal behaviour in young people: The good, the bad and the unknown. PLoS ONE 2017, 12, e0181722. [Google Scholar] [CrossRef]
- Andriessen, K. Can postvention be prevention? Crisis 2009, 30, 43–47. [Google Scholar] [CrossRef]
- Levi-Belz, Y.; Lev-Ari, L. “Let’s talk about it”: The moderating role of self-disclosure on complicated grief over time among suicide survivors. Int. J. Environ. Res. Public Health 2019, 16, 3740. [Google Scholar] [CrossRef]
- Cerel, J.; Campbell, F.R. Suicide survivors seeking mental health services: A preliminary examination of the role of an active postvention model. Suicide Life-Threat. Behav. 2008, 38, 30–34. [Google Scholar] [CrossRef]
- Cha, J.M.; Kim, J.E.; Kim, M.A.; Shim, B.; Cha, M.J.; Lee, J.J.; Han, D.H.; Chung, U.S. Five months follow-up study of school-based crisis intervention for Korean high school students who experienced a peer suicide. J. Korean Med. Sci. 2018, 33, e192. [Google Scholar] [CrossRef]
- Cheng, Q.; Li, H.; Silenzio, V.; Caine, E.D. Suicide contagion: A systematic review of definitions and research utility. PLoS ONE 2014, 9, e108724. [Google Scholar] [CrossRef] [PubMed]
- Andriessen, K.; Draper, B.; Dudley, M.; Mitchell, P.B. Bereavement after suicide: Disentangling clues to better help bereaved adolescents. Crisis 2015, 36, 299–303. [Google Scholar] [CrossRef] [PubMed]
- Capps, R.E.; Michael, K.D.; Jameson, J.P. Lethal means and adolescent suicidal risk: An expansion of the PEACE Protocol. J. Rural Ment. Health 2019, 43, 3–16. [Google Scholar] [CrossRef]
- Ghabrial, M.A. “Trying to figure out where we belong”: Narratives of racialized sexual minorities on community, identity, discrimination, and health. Sex. Res. Soc. Policy 2017, 14, 42–55. [Google Scholar] [CrossRef]
- Hart, T.A.; Sharvendiran, R.; Chikermane, V.; Kidwai, A.; Grace, D. At the intersection of homophobia and racism: Sociocultural context and the sexual health of South Asian Canadian gay and bisexual men. Stigma Health 2021. [Google Scholar] [CrossRef]
- Thoma, B.C.; Huebner, D.M. Health consequences of racist and antigay discrimination for multiple minority adolescents. Cult. Divers. Ethn. Minor. Psychol. 2013, 19, 404–413. [Google Scholar] [CrossRef]
- Movement Advancement Project. LGBTQ Youth Issues. 2022. Available online: https://www.lgbtmap.org/ (accessed on 1 March 2022).
- GLSEN. Research and Education Webinars. Available online: https://www.glsen.org/resources/webinars-and-workshops (accessed on 9 September 2022).
- Fetner, T.; Elafros, A. The GSA difference: LGBTQ and ally experiences in high schools with and without gay-straight alliances. Soc. Sci. 2015, 4, 563–581. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Williams, D.Y.; Hall, W.J.; Dawes, H.C.; Rizo, C.F.; Goldbach, J.T. An Integrated Conceptual Model to Understand Suicidality among Queer Youth to Inform Suicide Prevention. Societies 2022, 12, 170. https://doi.org/10.3390/soc12060170
Williams DY, Hall WJ, Dawes HC, Rizo CF, Goldbach JT. An Integrated Conceptual Model to Understand Suicidality among Queer Youth to Inform Suicide Prevention. Societies. 2022; 12(6):170. https://doi.org/10.3390/soc12060170
Chicago/Turabian StyleWilliams, Denise Yookong, William J. Hall, Hayden C. Dawes, Cynthia Fraga Rizo, and Jeremy T. Goldbach. 2022. "An Integrated Conceptual Model to Understand Suicidality among Queer Youth to Inform Suicide Prevention" Societies 12, no. 6: 170. https://doi.org/10.3390/soc12060170
APA StyleWilliams, D. Y., Hall, W. J., Dawes, H. C., Rizo, C. F., & Goldbach, J. T. (2022). An Integrated Conceptual Model to Understand Suicidality among Queer Youth to Inform Suicide Prevention. Societies, 12(6), 170. https://doi.org/10.3390/soc12060170