The Age-Related Association of Movement in Irish Adolescent Youth


 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants and Setting
2.2. Data Collection
2.3. Measures
2.4. Data Analysis
3. Results
3.1. Fundamental Movement Skills
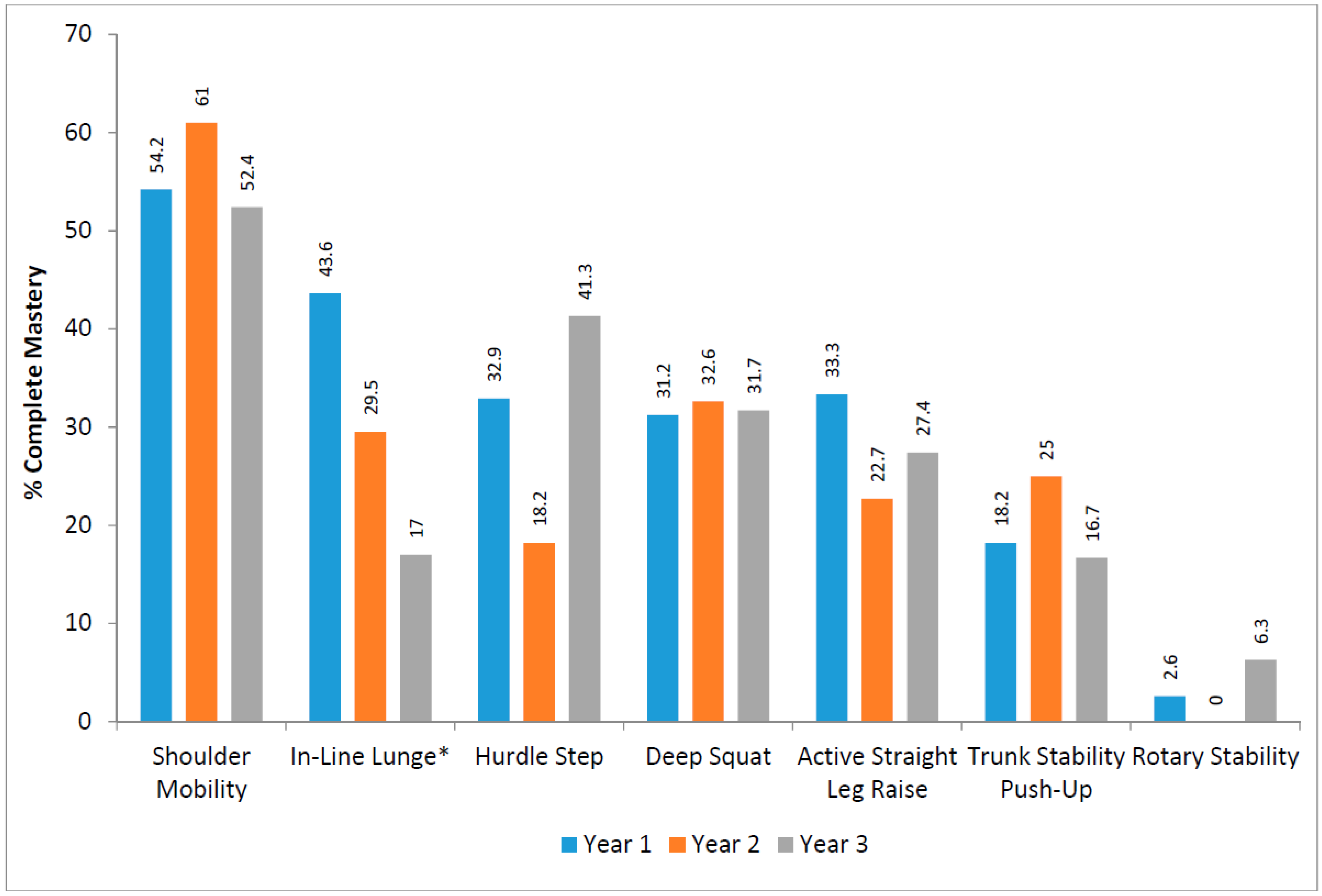
3.2. Functional Movement Screen
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Woods, C.B.; Tannehill, D.; Quinlan, A.; Moyna, N.; Walsh, J. The Children’s Sport Participation and Physical Activity (CSPPA); Research Report No 1; School of Health and Human Performance, Dublin City University and The Irish Sports Council: Dublin, Ireland, 2010. [Google Scholar]
- Hallal, P.C.; Andersen, L.B.; Bull, F.C.; Guthold, R.; Haskell, W.L.; Ekelund, U. Global Physical Activity Levels: Surveillance Progress, Pitfalls, and Prospects. Lancet 2012. [Google Scholar] [CrossRef]
- Barnett, L.M.; van Beurden, E.; Morgan, P.J.; Brooks, L.O.; Beard, J.R. Childhood Motor Skill Proficiency as a Predictor of Adolescent Physical Activity. J. Adolesc. Heal. 2009, 44, 252–259. [Google Scholar] [CrossRef] [PubMed]
- Lubans, D.R.; Morgan, P.J.; Cliff, D.P.; Barnett, L.M.; Okely, A.D. Fundamental Movement Skills in Children and Adolescents: Review of Associated Health Benefits. Sports Med. 2010, 40, 1019–1035. [Google Scholar] [CrossRef] [PubMed]
- Fisher, A.; Reilly, J.J.; Kelly, L.A.; Montgomery, C.; Williamson, A.; Paton, J.Y.; Grant, S. Fundamental Movement Skills and Habitual Physical Activity in Young Children. Med. Sci. Sports Exerc. 2005, 37, 684–688. [Google Scholar] [CrossRef] [PubMed]
- Lloyd, M.; Saunders, T.J.; Bremer, E.; Tremblay, M.S. Long-Term Importance of Fundamental Motor Skills: A 20-Year Follow-up Study. Adapt. Phys. Act. Quart. 2014, 31, 67–78. [Google Scholar] [CrossRef] [PubMed]
- Wrotniak, B.H.; Epstein, L.H.; Dorn, J.M.; Jones, K.E.; Kondilis, V.A. The Relationship between Motor Proficiency and Physical Activity in Children. Pediatrics 2006, 118, e1758–e1765. [Google Scholar] [CrossRef] [PubMed]
- Belton, S.; O’Brien, W.; Meegan, S.; Woods, C.B.; Issartel, J. Youth-Physical Activity Towards Health: Evidence and Background to the Development of the Y-PATH Physical Activity Intervention for Adolescents. BMC Public Health 2014, 14, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Hardy, L.L.; Barnett, L.M.; Espinel, P.; Okely, A.D. Thirteen-Year Trends in Child and Adolescent Fundamental Movement Skills: 1997–2010. Med. Sci. Sports Exerc. 2013, 45, 1965–1970. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, W.; Belton, S.; Issartel, J. Fundamental Movement Skill Proficiency amongst Adolescent Youth. Phys. Educ. Sport Pedagog. 2016. [Google Scholar] [CrossRef]
- O’Brien, W.; Belton, S.; Issartel, J. The Relationship between Adolescents’ Physical Activity, Fundamental Movement Skills and Weight Status. J. Sports Sci. 2016, 34, 1–9. [Google Scholar]
- Abraham, A.; Sannasi, R.; Nair, R. Normative Values for the Functional Movement Screentm in Adolescent School Aged Children. Int. J. Sports Phys. Ther. 2015, 10, 29–36. [Google Scholar] [PubMed]
- Cook, G.; Burton, L.; Hoogenboom, B. Pre-Participation Screening: The Use of Fundamental Movements as an Assessment of Function—Part 1. N. Am. J. Sports Phys. Ther. 2006, 1, 62–72. [Google Scholar] [PubMed]
- Cook, G.; Burton, L.; Hoogenboom, B. Pre-Participation Screening: The Use of Fundamental Movements as an Assessment of Function—Part 2. N. Am. J. Sports Phys. Ther. 2006, 1, 132–139. [Google Scholar] [PubMed]
- Clark, J.E.; Metcalfe, J.S. The Mountain of Motor Development: A Metaphor. In Motor Development: Research and Review; NASPE Pulications: Reston, VA, USA, 2002. [Google Scholar]
- Hands, B.P. How Fundamental Are Fundamental Movement Skills? Act. Healthy Mag. 2012, 19, 14–17. [Google Scholar]
- Department of Education Victoria. Fundamental Motor Skills: A Manual for Classroom Teachers; Department of Education Victoria: Melbourne, Australia, 1996.
- Gallahue, D.L.; Ozmun, J.C.; Goodway, J.D. Understanding Motor Development: Infants, Children, Adolescents, Adults; McGraw-Hill: New York, NY, USA, 2012. [Google Scholar]
- Butterfield, S.A.; Angell, R.M.; Mason, C.A. Age and Sex Differences in Object Control Skills by Children Ages 5 to 14. Percept. Mot. Skills 2012, 114, 261–274. [Google Scholar] [CrossRef] [PubMed]
- Stodden, D.F.; Goodway, J.D.; Langendorfer, S.J.; Roberton, M.A.; Rudisill, M.E.; Garcia, C.; Garcia, L.E. A Developmental Perspective on the Role of Motor Skill Competence in Physical Activity: An Emergent Relationship. Quest 2008, 60, 290–306. [Google Scholar] [CrossRef]
- Venetsanou, F.; Kambas, A. Can Motor Proficiency in Preschool Age Affect Physical Activity in Adolescence? Pediatr. Exerc. Sci. 2017, 29, 254–259. [Google Scholar] [CrossRef] [PubMed]
- Rose, B.; Larkin, D.; Berger, B. Perceptions of Social Support in Children of Low, Moderate and High Levels of Coordination. ACHPER Healthy Lifestyles J. 1994, 41, 18–21. [Google Scholar]
- US Department of Health and Human Services. Guidelines for School and Community Programs to Promote Lifelong Physical Activity among Young People. Morbidity and Mortality Weekly Report; US Department of Health and Human Services: Washington, DC, USA, 1997.
- Lopes, V.P.; Stodden, D.F.; Bianchi, M.M.; Maia, J.A.R.; Rodrigues, L.P. Correlation between BMI and Motor Coordination in Children. J. Sci. Med. Sport 2012, 15, 38–43. [Google Scholar] [CrossRef] [PubMed]
- Bryant, E.S.; Duncan, M.J.; Birch, S.L. Fundamental Movement Skills and Weight Status in British Primary School Children. Eur. J. Sport Sci. 2014, 14, 730–736. [Google Scholar] [CrossRef] [PubMed]
- Bremer, E.; Cairney, J. Fundamental Movement Skills and Health-Related Outcomes: A Narrative Review of Longitudinal and Intervention Studies Targeting Typically Developing Children. Am. J. Lifestyle Med. 2016. [Google Scholar] [CrossRef]
- O’ Brien, W.; Duncan, M.J.; Farmer, O.; Lester, D. Do Irish Adolescents Have Adequate Functional Movement Skill and Confidence? J. Mot. Learn. Dev. 2017. [Google Scholar] [CrossRef]
- Duncan, M.J.; Stanley, M.; Leddington Wright, S. The Association between Functional Movement and Overweight and Obesity in British Primary School Children. BMC Sport Sci. Med. Rehabil. 2013, 5, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Kraus, K.; Schutz, E.; Taylor, W.R.; Doyscher, R. Efficacy of the Functional Movement Screen: A Review. J. Strength Cond. Res. 2014, 28, 3571–3584. [Google Scholar] [CrossRef] [PubMed]
- Cook, G.; Burton, L.C.; Fields, K. The Functional Movement Screen and Exercise Progressions Manual. Functional Movement Systems. 2012. Available online: https://www.functionalmovement.com/files/imagebyname?fileName=717a_650a_FMS%20Level%201%20Online%20V1%203-21-2016.pdf (accessed on 1 October 2017).
- Valentini, N.C.; Logan, S.W.; Spessato, B.C.; de Souza, M.S.; Pereira, K.G.; Rudisill, M.E. Fundamental Motor Skills across Childhood: Age, Sex, and Competence Outcomes of Brazilian Children. J. Mot. Learn. Dev. 2016, 4, 16–36. [Google Scholar] [CrossRef]
- Bodden, J.G.; Needham, R.A.; Chockalingam, N. The Effect of an Intervention Program on Functional Movement Screen Test Scores in Mixed Martial Arts Athletes. J. Strength Cond. Res. 2015, 29, 219–225. [Google Scholar] [CrossRef] [PubMed]
- Perry, F.T.; Koehle, M.S. Normative Data for the Functional Movement Screen in Middle-Aged Adults. J. Strength Cond. Res. 2013, 27, 458–462. [Google Scholar] [CrossRef] [PubMed]
- Barnett, L.M.; van Beurden, E.; Morgan, P.J.; Brooks, L.O.; Beard, J.R. Gender Differences in Motor Skill Proficiency from Childhood to Adolescence: A Longitudinal Study. Res. Q. Exerc. Sport 2010, 81, 162–170. [Google Scholar] [PubMed]
- Ulrich, D.A. Test of Gross Motor Development 2: Examiner’s Manual, 2nd ed.; Pro-Ed: Austin, TX, USA, 2000. [Google Scholar]
- Logan, S.W.; Barnett, L.M.; Goodway, J.D.; Stodden, D.F. Comparison of Performance on Process- and Product-Oriented Assessments of Fundamental Motor Skills across Childhood. J. Sports Sci. 2017, 35, 634–641. [Google Scholar] [CrossRef] [PubMed]
- Cools, W.; de Martelaer, K.; Samaey, C.; Andries, C. Movement Skill Assessment of Typically Developing Preschool Children: A Review of Seven Movement Skill Assessment Tools. J. Sports Sci. Med. 2009, 8, 154–168. [Google Scholar] [PubMed]
- Ulrich, D.A. Test of Gross Motor Development; Pro-Ed: Austin, TX, USA, 1985. [Google Scholar]
- McGrane, B.; Belton, S.; Powell, D.; Issartel, J. The Relationship between Fundamental Movement Skill Proficiency and Physical Self-Confidence among Adolescents. J. Sports Sci. 2017, 35, 1709–1714. [Google Scholar] [CrossRef] [PubMed]
- Okely, A.D.; Booth, M.L. Mastery of Fundamental Movement Skills among Children in New South Wales: Prevalence and Sociodemographic Distribution. J. Sci. Med. Sport 2004, 7, 358–372. [Google Scholar] [CrossRef]
- Cook, G.; Burton, L.; Fields, K.; Kiesel, K.B. The Functional Movement Screen; Athletic Testing Services, Inc.: Danville, CA, USA, 1998. [Google Scholar]
- Letafatkar, A.; Hadadnezhad, M.; Shojaedin, S.; Mohamadi, E. Relationship between Functional Movement Screening Score and History of Injury. Int. J. Sports Phys. Ther. 2014, 9, 21–27. [Google Scholar] [PubMed]
- O’Connor, F.G.; Deuster, P.A.; Davis, J.; Pappas, C.G.; Knapik, J.J. Functional Movement Screening: Predicting Injuries in Officer Candidates. Med. Sci. Sports Exerc. 2011, 43, 2224–2230. [Google Scholar] [CrossRef] [PubMed]
- Bardenett, S.M.; Micca, J.J.; DeNoyelles, J.T.; Miller, S.D.; Jenk, D.T.; Brooks, G.S. Functional Movement Screen Normative Values and Validity in High School Athletes: Can the FMSTM Be Used as a Predictor of Injury? Int. J. Sports Phys. Ther. 2015, 10, 303–308. [Google Scholar] [PubMed]
- Cook, G. Movement: Functional Movement Systems: Screening, Assessment and Corrective Strategies; On Target Publications: Santa Cruz, CA, USA, 2010. [Google Scholar]
- Duncan, M.J.; Stanley, M. Functional Movement Is Negatively Associated with Weight Status and Positively Associated with Physical Activity in British Primary School Children. J. Obes. 2012. [Google Scholar] [CrossRef] [PubMed]
- Schneiders, A.G.; Davidsson, A.; Hörman, E.; Sullivan, S.J. Functional Movement Screen Normative Values in a Young, Active Population. Int. J. Sports Phys. Ther. 2011, 6, 75–82. [Google Scholar] [PubMed]
- Lunn, P.; Kelly, E.; Fitzpatrick, N. Keeping Them in the Game: Taking up and Dropping out of Sport and Exercise in Ireland; The Economic and Social Research Institute (ESRI): Dublin, Ireland, 2013. [Google Scholar]
- Gallahue, D.L.; Ozmun, J.C. Understanding Motor Development: Infants, Children, Adolescents, Adults, 6th ed.; Mc-Graw Hill: New York, NY, USA, 2006. [Google Scholar]
- Seefeldt, V. Developmental Motor Patterns: Implications for Elementary School Physical Education. Psychol. Mot. Behav. Sport. 1980, 36, 314–323. [Google Scholar]
- Haywood, K.M.; Getchell, N. Life Span Motor Development, 5th ed.; Human Kinetics: Champaign, IL, USA, 2009. [Google Scholar]
- Fjørtoft, I. The Natural Environment as a Playground for Children: The Impact of Outdoor Play Activities in Pre-Primary School Children. Early Child. Educ. J. 2001, 29, 111–117. [Google Scholar] [CrossRef]
- Hoehner, C.M.; Soares, J.; Perez, D.P.; Ribeiro, I.C.; Joshu, C.E.; Pratt, M.; Brownson, R.C. Physical Activity Interventions in Latin American: A Systematic Review. Am. J. Prev. Med. 2008, 34, 224–233. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Monteiro, C.; Popkin, B.M. Trends of Obesity and Underweight in Older Children and Adolescents in the United States, Brazil, China, and Russia. Am. J. Clin. Nutr. 2002, 75, 971–977. [Google Scholar] [PubMed]
- Booth, M.L.; Okely, A.D.; McLellan, L.; Phongsavan, P.; Macaskill, P.; Patterson, J.; Wright, J.; Holland, B. Mastery of Fundamental Motor Skills among New South Wales School Students: Prevalence and Sociodemographic Distribution. J. Sci. Med. Sport 1999, 2, 93–105. [Google Scholar] [CrossRef]
- Portas, M.D.; Parkin, G.; Roberts, J.; Batterham, A.M. Maturational Effect on Functional Movement ScreenTM Score in Adolescent Soccer Players. J. Sci. Med. Sport 2016, 19, 854–858. [Google Scholar] [CrossRef] [PubMed]
- Paszkewicz, J.R.; McCarty, C.W.; van Lunen, B.L. Comparison of Functional and Static Evaluation Tools among Adolescent Athletes. J. Strength Cond. Res. 2013, 27, 2842–2850. [Google Scholar] [CrossRef] [PubMed]
- Cook, G.; Burton, L.; Hoogenboom, B.J.; Voight, M.L. Functional Movement Screening: The Use of Fundamental Movements as an Assssment of Function—Part 1. Int. J. Sports Phys. Ther. 2014, 9, 549–563. [Google Scholar] [PubMed]
- Bremer, E.; Lloyd, M. The Importance of Fundamental Motor Skill Proficiency for Physical Activity in Elementary School Age Females. PHEnex J. 2014, 6, 1–12. [Google Scholar]
- O’Brien, W.; Belton, S.; Issartel, J. Promoting Physical Literacy in Irish Adolescent Youth: The Youth-Physical Activity Towards Health (Y-PATH) Intervention. MOJ Public Health 2015, 2, 1–6. [Google Scholar]
- Lai, S.K.; Costigan, S.A.; Stodden, D.F.; Salmon, J.; Barnett, L.M. Do School-Based Interventions Focusing on Physical Activity, Fitness, or Fundamental Movement Skill Competency Produce a Sustained Impact in These Outcomes in Children and Adolescents? A Systematic Review of Follow-up Studies. Sports Med. 2014, 44, 67–79. [Google Scholar] [CrossRef] [PubMed]
- Logan, S.W.; Robinson, L.E.; Wilson, A.E.; Lucas, W.A. Getting the Fundamentals of Movement: A Meta-Analysis of the Effectiveness of Motor Skill Interventions in Children. Child Care Health Dev. 2011, 38, 305–315. [Google Scholar] [CrossRef] [PubMed]
- Morgan, P.J.; Barnett, L.M.; Cliff, D.P.; Okely, A.D.; Scott, H.A.; Cohen, K.E.; Lubans, D.R. Fundamental Movement Skill Interventions in Youth: A Systematic Review and Meta-Analysis. Pediatrics 2013, 132, e1361–e1383. [Google Scholar] [CrossRef] [PubMed]
- Robinson, L.E.; Stodden, D.F.; Barnett, L.M.; Lopes, V.P.; Logan, S.W.; Rodrigues, L.P.; D’Hondt, E. Motor Competence and Its Effect on Positive Developmental Trajectories of Health. Sports Med. 2015, 45, 1273–1284. [Google Scholar] [CrossRef] [PubMed]
- Barnett, L.M.; Hardy, L.L.; Lubans, D.R.; Cliff, D.P.; Okely, A.D.; Hills, A.P.; Morgan, P.J. Australian Children Lack the Basic Movement Skills to Be Active and Healthy. Health Promot. J. Aust. 2013, 24, 82–84. [Google Scholar] [CrossRef] [PubMed]
- van Beurden, E.; Barnett, L.M.; Zask, A.; Dietrich, U.C.; Brooks, L.O.; Beard, J.R. Can We Skill and Activate Children through Primary School Physical Education lessons? “Move It Groove It”—A Collaborative Health Promotion Intervention. Prev. Med. 2003, 36, 493–501. [Google Scholar] [CrossRef]
- Mitchell, B.; McLennan, S.; Latimer, K.; Graham, D.; Gilmore, J.; Rush, E. Improvement of Fundamental Movement Skills through Support and Mentorship of Class Room Teachers. Obes. Res. Clin. Pract. 2013, 7, e230–e234. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, W.; Issartel, J.; Belton, S. Evidence for the Efficacy of the Youth-Physical Activity Towards Health (Y-PATH) Intervention. Adv. Phys. Educ. 2013, 3, 145–153. [Google Scholar] [CrossRef]
- Barnett, L.M.; Stodden, D.F.; Cohen, K.E.; Smith, J.J.; Lubans, D.R.; Lenoir, M.; Iivonen, S.; Miller, A.D.; Laukkanen, A.I.; Dudley, D.; et al. Fundamental Movement Skills: An Important Focus. J. Teach. Phys. Educ. 2016, 35, 219–225. [Google Scholar] [CrossRef]
- Kiesel, K.B.; Plisky, P.J.; Butler, R.J. Functional Movement Test Scores Improve Following a Standardized off-Season Intervention Program in Professional Football Players. Scand. J. Med. Sci. Sport 2009. [Google Scholar] [CrossRef] [PubMed]
- Kalaja, S.P.; Jaakkola, T.T.; Liukkonen, J.O.; Digelidis, N. Development of Junior High School Students’ Fundamental Movement Skills and Physical Activity in a Naturalistic Physical Education Setting. Phys. Educ. Sport Pedagog. 2012, 17, 411–428. [Google Scholar] [CrossRef]
- Martin, E.H.; Rudisill, M.E.; Hastie, P.A. Motivational Climate and Fundamental Motor Skill Performance in a Naturalistic Physical Education Setting. Phys. Educ. Sport Pedagog. 2009, 14, 227–240. [Google Scholar] [CrossRef]
- Stobierski, L.M.; Fayson, S.D.; Minthorn, L.M.; Valovich McLeod, T.C.; Welch, C.E. Reliability of Clinician Scoring of the Functional Movement Screen to Assess Movement Patterns. J. Sport Rehabil. 2015, 24, 219–222. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| FMS Component | Males | Females | ||||
|---|---|---|---|---|---|---|
| Year 1 (n = 46) | Year 2 (n = 28) | Year 3 (n = 34) | Year 1 (n = 33) | Year 2 (n = 15) | Year 3 (n = 25) | |
| Catch | ||||||
| (1) Preparation phase where hands are in front of the body and elbows are flexed. | 93.5 | 96.4 | 91.4 | 97.0 | 100 | 100 |
| (2) Arms extend while reaching for the ball as it arrives. | 91.3 | 78.6 | 85.7 | 93.9 | 100 | 100 |
| (3) Ball is caught be hands only. | 97.8 | 85.7 | 80.0 | 87.9 | 100 | 100 |
| Run | ||||||
| (1) Arms move in opposition to legs, elbows bent. | 91.3 | 89.3 | 91.7 | 81.8 | 86.7 | 89.3 |
| (2) Brief period where both feet are off the ground. | 100 | 100 | 100 | 100 | 100 | 100 |
| (3) Narrow foot placement landing on heel or toe. | 97.8 | 100 | 97.2 | 97.0 | 100 | 100 |
| (4) Non-support leg bent approximately 90 degrees. | 82.6 | 89.3 | 88.9 | 87.9 | 80.0 | 96.4 |
| Balance | ||||||
| (1) Support leg still, foot flat on the ground. | 100 | 100 | 97.1 | 100 | 100 | 100 |
| (2) Non-support leg bent, not touching the support leg. | 93.5 | 89.3 | 94.3 | 84.8 | 100 | 92.3 |
| (3) Head stable, eyes focused forward. | 97.8 | 92.9 | 68.6 | 100 | 100 | 96.2 |
| (4) Trunk stable and upright. | 89.1 | 92.9 | 94.3 | 100 | 93.3 | 100 |
| (5) No excessive arm movements. | 87.0 | 85.7 | 94.3 | 84.8 | 93.3 | 100 |
| Skip | ||||||
| (1) A rhythmical repetition of the step-hop on alternate feet. | 89.1 | 100 | 94.4 | 93.9 | 100 | 100 |
| (2) Foot of non-support leg carried near surface during the hop phase. | 93.5 | 100 | 94.4 | 93.9 | 100 | 100 |
| (3) Arms alternately moving in opposition to legs at about the waist level. | 60.9 | 75.0 | 86.1 | 69.7 | 86.7 | 78.6 |
| Kick | ||||||
| (1) Rapid continuous approach to the ball. | 60.9 | 64.3 | 55.6 | 33.3 | 20.0 | 40.7 |
| (2) An elongated stride or leap immediately prior to ball contact. | 100 | 96.4 | 91.7 | 81.8 | 66.7 | 66.7 |
| (3) Non-kicking foot placed even with or slightly in back of the ball. | 87.0 | 92.9 | 86.1 | 39.4 | 46.7 | 55.6 |
| (4) Kicks ball with instep of preferred foot (shoelaces) or toe. | 100 | 100 | 94.4 | 93.9 | 86.7 | 96.3 |
| Dribble | ||||||
| (1) Contacts ball with one hand at about the belt level. | 63.0 | 32.1 | 42.9 | 36.4 | 60.0 | 34.6 |
| (2) Pushes ball with fingertips (not a slap). | 95.7 | 96.4 | 91.4 | 84.8 | 73.3 | 88.5 |
| (3) Ball contacts surface in front of or to the outside of foot on preferred side. | 87.0 | 71.4 | 62.9 | 87.9 | 86.7 | 46.2 |
| (4) Maintains control of ball for four consecutive bounces without having to move the feet to retrieve it. | 82.6 | 92.9 | 88.6 | 97.0 | 86.7 | 88.5 |
| Strike | ||||||
| (1) Dominant hand grips bat above non-dominant hand. | 45.7 | 57.1 | 69.4 | 60.6 | 60.0 | 72.4 |
| (2) Non-preferred side of body faces the imaginary tosser with feet parallel. | 95.7 | 96.4 | 88.9 | 57.6 | 80.0 | 82.8 |
| (3) Hip and shoulder rotation during swing. | 100 | 100 | 100 | 87.9 | 60.0 | 86.2 |
| (4) Transfers body weight to front foot. | 73.9 | 71.4 | 86.1 | 60.6 | 40.0 | 51.7 |
| (5) Bat contacts ball. | 80.4 | 85.7 | 88.9 | 69.7 | 86.7 | 72.4 |
| Vertical Jump | ||||||
| (1) Eyes focused forward or upward throughout the jump. | 63.0 | 60.7 | 67.6 | 75.8 | 53.3 | 76.9 |
| (2) Crouch with knees bent and arms behind the body. | 71.7 | 71.4 | 73.5 | 45.5 | 53.3 | 57.7 |
| (3) Forceful forward and upward swing of the arms. | 34.8 | 10.7 | 47.1 | 42.4 | 46.7 | 38.5 |
| (4) Legs straighten in air. | 95.7 | 92.9 | 97.1 | 87.9 | 100 | 96.2 |
| (5) Land on balls of feet and bend knees to absorb landing. | 87.0 | 92.9 | 100 | 97.0 | 100 | 100 |
| (6) Controlled landing with ≤1 step any direction. | 87.0 | 100 | 100 | 100 | 100 | 100 |
| Throw | ||||||
| (1) Wind-up is initiated with downward movement of hand/arm. | 97.8 | 100 | 100 | 97.0 | 93.3 | 100 |
| (2) Rotates hip and shoulder to a point where the non-throwing side faces the wall. | 50.0 | 39.3 | 8.6 | 9.1 | 6.7 | 0 |
| (3) Weight is transferred by stepping with the foot opposite the throwing hand. | 71.7 | 71.4 | 37.1 | 51.5 | 26.7 | 17.2 |
| (4) Follow-through beyond ball release diagonally across the body towards the non-preferred side. | 84.8 | 92.9 | 57.1 | 51.5 | 20.0 | 34.5 |
| Horizontal Jump | ||||||
| (1) Preparatory movement includes flexion of both knees with arms extended behind body. | 87.0 | 85.7 | 88.6 | 69.7 | 73.3 | 76.9 |
| (2) Arms extend forcefully forward and upward reaching full extension above the head. | 28.3 | 25.0 | 14.3 | 9.1 | 20.0 | 0 |
| (3) Take off and land on both feet simultaneously. | 84.8 | 89.3 | 97.1 | 87.9 | 93.3 | 80.8 |
| (4) Arms thrust downward during landing. | 89.1 | 92.9 | 85.7 | 69.7 | 66.7 | 61.5 |
| FMS™ Component | Year 1 (n = 68) | Year 2 (n = 41) | Year 3 (n = 43) | |||
|---|---|---|---|---|---|---|
| Active Straight Leg Raise | L | R | L | R | L | R |
| (1) Knee on floor remains in contact with (i.e., touching) the board. | 62.7 | 53.3 | 61.4 | 59.1 | 66.1 | 69.4 |
| (2) Leg on floor does not externally rotate at the hip. | 85.3 | 89.3 | 86.4 | 95.3 | 91.9 | 93.5 |
| Deep Squat | - | - | - | |||
| (1) Dowel maximally pressed overhead and aligned over feet. Note lumbar flexion. | 77.9 | 81.4 | 76.7 | |||
| (2) Toes point forward. | 75.3 | 86 | 88.3 | |||
| (3) Knees aligned over feet and knees do not go passed the toe line. | 72.7 | 81.4 | 78.3 | |||
| (4) Thighs break parallel with the floor on descent (i.e., femur below horizontal). | 77.9 | 72.1 | 73.3 | |||
| Hurdle Step | L | R | L | R | L | R |
| (1) Hips, knees and ankles aligned. | 53.2 | 53.2 | 40.9 | 29.5 | 46 | 57.1 |
| (2) Maintains a stable torso with minimal to no movement in lumbar (i.e., lower) spine. | 79.7 | 84.8 | 86.4 | 93.2 | 92.1 | 93.7 |
| (3) Dowel and hurdle remain parallel. | 84.8 | 89.9 | 97.7 | 97.7 | 96.8 | 98.4 |
| (4) Foot and/or heel touches the floor while standing leg remains in extended position. | 96.2 | 97.5 | 97.7 | 100 | 100 | 100 |
| (5) No contact between foot and hurdle. | 98.7 | 100 | 100 | 100 | 100 | 100 |
| In-Line Lunge | L | R | L | R | L | R |
| (1) Dowel remains in contact with head, thoracic spine and sacrum. | 69.2 | 67.9 | 65.9 | 54.5 | 31.7 | 36.2 |
| (2) Dowel remains vertical. | 70.5 | 69.2 | 77.3 | 65.9 | 55.6 | 55.3 |
| (3) No torso movement (i.e., balance is maintained). | 91 | 91 | 86.4 | 97.7 | 92.1 | 93.6 |
| (4) Knee touches board behind heel of front foot. | 85.9 | 85.9 | 95.5 | 93.2 | 63.5 | 72.3 |
| (5) The front heel remains in contact with the board and the back heel touches board when returning to starting position. | 70.5 | 66.7 | 68.2 | 72.7 | 69.8 | 76.6 |
| Rotary Stability | L | R | L | R | L | R |
| (1) Ankles dorsiflexed (i.e., toes tucked under). | 9.5 | 14.9 | 13.6 | 18.2 | 19 | 17.5 |
| (2) Back remains flat (i.e., spine remains parallel to board). | 81.1 | 86.5 | 84.1 | 81.8 | 87.3 | 82.5 |
| Shoulder Mobility | L | R | L | R | L | R |
| (1) Does not walk hands towards each other (i.e., one single motion). | 83.3 | 89.2 | 85.4 | 90.2 | 100 | 98.4 |
| (2) Head remains in neutral position. | 76.4 | 77 | 76.9 | 79.5 | 93.7 | 92.1 |
| Trunk Stability Push-Up | - | - | - | |||
| (1) Body lifts as a unit with no lag in lumbar (i.e., lower) spine when performing the push-up (i.e., chest and stomach come off the floor at the same instance). | 24.7 | 31.8 | 25 | |||
| (2) Ankles are dorsiflexed in both the preparatory and performance phases of the movement. | 42.9 | 47.7 | 45 | |||
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lester, D.; McGrane, B.; Belton, S.; Duncan, M.J.; Chambers, F.C.; O’Brien, W. The Age-Related Association of Movement in Irish Adolescent Youth. Sports 2017, 5, 77. https://doi.org/10.3390/sports5040077
Lester D, McGrane B, Belton S, Duncan MJ, Chambers FC, O’Brien W. The Age-Related Association of Movement in Irish Adolescent Youth. Sports. 2017; 5(4):77. https://doi.org/10.3390/sports5040077
Chicago/Turabian StyleLester, Diarmuid, Bronagh McGrane, Sarahjane Belton, Michael J. Duncan, Fiona C. Chambers, and Wesley O’Brien. 2017. "The Age-Related Association of Movement in Irish Adolescent Youth" Sports 5, no. 4: 77. https://doi.org/10.3390/sports5040077
APA StyleLester, D., McGrane, B., Belton, S., Duncan, M. J., Chambers, F. C., & O’Brien, W. (2017). The Age-Related Association of Movement in Irish Adolescent Youth. Sports, 5(4), 77. https://doi.org/10.3390/sports5040077