
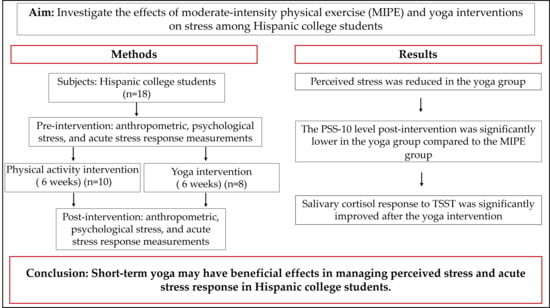
The Effects of Moderate-Intensity Physical Exercise and Yoga Interventions on Stress in Hispanic College Students: A Pilot Study

 and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Research Design
2.2. Participants
2.3. Interventions
2.4. Physical Measurement
2.5. Research Instruments
2.5.1. Perceived Stress Scale-10 Item
2.5.2. Trier Social Stress Test (TSST)
2.5.3. Nutrition and Physical Activity Questionnaire (NPAQ-A)
2.6. Saliva Samples
2.6.1. Saliva Sample Collection
2.6.2. Salivary Cortisol Measurement
2.7. Statistical Analysis
2.8. Reliability and Validation of Study
3. Results
3.1. Anthropometric Characteristics, Perceived Stress, and Cortisol Associations
3.2. Associations of Perceived Stress and Cortisol Levels with Dietary and Physical Activity Habits Before the Interventions
3.3. Physiological and Psychological Stress and Salivary Cortisol Response to TSST in the Intervention Groups
3.4. Acute Stress Response to Stressor (TSST) Pre- and Post-Intervention
4. Discussion
4.1. Association Between Psychological Stress and Lifestyle
4.1.1. Psychological Stress and Diet
4.1.2. Psychological Stress and Attitude to Exercise
4.2. Effects of MIPE and Yoga Intervention on Psychological Stress
4.3. Effects of MIPE and Yoga Intervention on Acute Stress Response
4.3.1. Effects of MIPE Intervention on Acute Stress Response
4.3.2. Effects of Yoga on Acute Stress Response
5. Study Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ACHA NCHA | American College Health Association’s National College Health Assessment |
| BMI | Body mass index |
| HPA | Hypothalamic–pituitary–adrenal |
| IRB | Institutional Review Board |
| MIPE | Moderate-intensity physical exercise |
| NPAQ-A | Nutrition and Physical Activity Questionnaire-Adult |
| PSS | Perceived stress scale |
| TSST | Trier Social Stress Test |
| UTRGV | University of Texas Rio Grande Valley |
References
- ACHA. Undergraduate Reference Group Executive Summary, Fall 2024. Available online: https://www.acha.org/wp-content/uploads/NCHA-IIIb_FALL_2024_UNDERGRADUATE_REFERENCE_GROUP_EXECUTIVE_SUMMARY.pdf (accessed on 12 June 2025).
- Wagner, T.; Yelverton, C. Perceived stress and burnout syndrome in chiropractic students at a South African university during the COVID-19 pandemic: A cross-sectional study. J. Chiropr. Educ. 2024, 38, 172–178. [Google Scholar] [CrossRef] [PubMed]
- Neseliler, S.; Tannenbaum, B.; Zacchia, M.; Larcher, K.; Coulter, K.; Lamarche, M.; Marliss, E.B.; Pruessner, J.; Dagher, A. Academic stress and personality interact to increase the neural response to high-calorie food cues. Appetite 2017, 116, 306–314. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.; Chen, A.; Chen, Y. College students’ stress and health in the COVID-19 pandemic: The role of academic workload, separation from school, and fears of contagion. PLoS ONE 2021, 16, e0246676. [Google Scholar] [CrossRef]
- Sinha, R. Role of addiction and stress neurobiology on food intake and obesity. Biol. Psychol. 2018, 131, 5–13. [Google Scholar] [CrossRef]
- Yoon, E.S.; So, W.Y.; Jang, S. Association between Perceived Psychological Stress and Exercise Behaviors: A Cross-Sectional Study Using the Survey of National Physical Fitness. Life 2023, 13, 2059. [Google Scholar] [CrossRef]
- Lei, A.A.; Phang, V.W.X.; Lee, Y.Z.; Kow, A.S.F.; Tham, C.L.; Ho, Y.C.; Lee, M.T. Chronic Stress-Associated Depressive Disorders: The Impact of HPA Axis Dysregulation and Neuroinflammation on the Hippocampus-A Mini Review. Int. J. Mol. Sci. 2025, 26, 2940. [Google Scholar] [CrossRef]
- McCabe, D.; Bednarz, J.; Lockwood, C.; Barker, T.H. Specific Nutrient Intake Via Diet and/or Supplementation in Relation to Female Stress: A Cross-Sectional Study. Womens Health Rep. 2020, 1, 241–251. [Google Scholar] [CrossRef]
- Rabasa, C.; Dickson, S.L. Impact of stress on metabolism and energy balance. Curr. Opin. Behav. Sci. 2016, 9, 71–77. [Google Scholar] [CrossRef]
- Ling, J.; Zahry, N.R. Relationships among perceived stress, emotional eating, and dietary intake in college students: Eating self-regulation as a mediator. Appetite 2021, 163, 105215. [Google Scholar] [CrossRef] [PubMed]
- Knezevic, E.; Nenic, K.; Milanovic, V.; Knezevic, N.N. The Role of Cortisol in Chronic Stress, Neurodegenerative Diseases, and Psychological Disorders. Cells 2023, 12, 2726. [Google Scholar] [CrossRef]
- Zhang, H.; Yao, Z.; Lin, L.; Sun, X.; Shi, X.; Zhang, L. Early life stress predicts cortisol response to psychosocial stress in healthy young adults. Psych. J. 2019, 8, 353–362. [Google Scholar] [CrossRef]
- Shin, D.W.; Lee, S.H. Blunted hypothalamo-pituitary-adrenal axis reactivity is associated with the poor intelligence performance in children with attention-deficit/hyperactivity disorder. Neuropediatrics 2007, 38, 298–303. [Google Scholar] [CrossRef]
- Ginty, A.T.; Phillips, A.C.; Roseboom, T.J.; Carroll, D.; Derooij, S.R. Cardiovascular and cortisol reactions to acute psychological stress and cognitive ability in the Dutch Famine Birth Cohort Study. Psychophysiology 2012, 49, 391–400. [Google Scholar] [CrossRef] [PubMed]
- Cordova, A.; Caballero-Garcia, A.; Drobnic, F.; Roche, E.; Noriega, D.C. Influence of Stress and Emotions in the Learning Process: The Example of COVID-19 on University Students: A Narrative Review. Healthcare 2023, 11, 1787. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.L.; Chen, C.H. Effectiveness of aerobic gymnastic exercise on stress, fatigue, and sleep quality during postpartum: A pilot randomized controlled trial. Int. J. Nurs. Stud. 2018, 77, 1–7. [Google Scholar] [CrossRef]
- Streeter, C.C.; Gerbarg, P.L.; Saper, R.B.; Ciraulo, D.A.; Brown, R.P. Effects of yoga on the autonomic nervous system, gamma-aminobutyric-acid, and allostasis in epilepsy, depression, and post-traumatic stress disorder. Med. Hypotheses 2012, 78, 571–579. [Google Scholar] [CrossRef] [PubMed]
- Koschel, T.L.; Young, J.C.; Navalta, J.W. Examining the Impact of a University-Driven Exercise Programming Event on End-of-Semester Stress in Students. Int. J. Exerc. Sci. 2017, 10, 754–763. [Google Scholar] [CrossRef]
- Benvenutti, M.J.; Alves, E.D.S.; Michael, S.; Ding, D.; Stamatakis, E.; Edwards, K.M. A single session of hatha yoga improves stress reactivity and recovery after an acute psychological stress task-A counterbalanced, randomized-crossover trial in healthy individuals. Complement. Ther. Med. 2017, 35, 120–126. [Google Scholar] [CrossRef]
- Ballard, P.J.; Hoyt, L.T.; Yazdani, N.; Kornbluh, M.; Cohen, A.K.; Davis, A.L.; Hagan, M.J. Election-related sociopolitical stress and coping among college students in the United States. J. Am. Coll. Health 2024, 72, 2494–2504. [Google Scholar] [CrossRef]
- Van Doren, N.; Zhu, Y.; Vazquez, M.M.; Shah, J.; Grammer, A.C.; Fitzsimmons-Craft, E.E.; Eisenberg, D.; Wilfley, D.E.; Taylor, C.B.; Newman, M.G. Racial and Ethnic Disparities in Barriers to Mental Health Treatment Among U.S. College Students. Psychiatr. Serv. 2024, 75, 839–846. [Google Scholar] [CrossRef]
- Fernandez, L.R.; Giron, S.E.; Killoren, S.E.; Campione-Barr, N. Latinx college students’ anxiety, academic stress, and future aspirations: The role of sibling relationship quality. J. Child. Fam. Stud. 2022, 32, 1936–1945. [Google Scholar] [CrossRef]
- Lazarevich, I.; Irigoyen-Camacho, M.E.; Radilla-Vazquez, C.C.; Gutierrez-Tolentino, R.; Velazquez-Alva, M.C.; Zepeda-Zepeda, M.A. Mindful Eating and Its Relationship with Obesity, Eating Habits, and Emotional Distress in Mexican College Students. Behav. Sci. 2025, 15, 669. [Google Scholar] [CrossRef]
- NCES. National Center for Education Statistics. 2022. Available online: https://nces.ed.gov/programs/coe/indicator/cge (accessed on 7 July 2025).
- Tsuzuki, A.; Kamada, M.; Amagasa, S.; Kitayuguchi, J.; Miyashita, T.; Abe, T.; Gomi, T.; Okuyama, K.; Taguri, M.; Inoue, S. Two-year scale-up dissemination study of a multi-strategic community-wide intervention promoting physical activity: A single-arm pre-post hybrid effectiveness-implementation trial. Int. J. Behav. Nutr. Phys. Act. 2024, 21, 131. [Google Scholar] [CrossRef]
- Walia, S.; Kumar, P.; Kataria, C. Interventions to Improve Standing Balance in Individuals with Incomplete Spinal Cord Injury: A Systematic Review and Meta-Analysis. Top. Spinal Cord Inj. Rehabil. 2023, 29, 56–83. [Google Scholar] [CrossRef] [PubMed]
- Lemay, V.; Hoolahan, J.; Buchanan, A. Impact of a Yoga and Meditation Intervention on Students’ Stress and Anxiety Levels. Am. J. Pharm. Educ. 2019, 83, 7001. [Google Scholar] [CrossRef] [PubMed]
- Carusotto, A.F. Impact of Hatha Yoga on Level of Perceived Stress in Doctor of Physical Therapy Students. J. Allied Health 2023, 52, e127–e131. [Google Scholar]
- UTRGV. UTRGV Strategic Analysis and Institutional Reporting. Available online: https://www.utrgv.edu/sair/ (accessed on 2 July 2025).
- Piercy, K.L.; Troiano, R.P. Physical Activity Guidelines for Americans from the US Department of Health and Human Services. Circ. Cardiovasc. Qual. Outcomes 2018, 11, e005263. [Google Scholar] [CrossRef]
- Gurung, J.; Turner, J.; Freeman, E.; Coleman, C.; Iacovou, S.; Hemingway, S. An Evaluation of MINDFIT-A Student Therapeutic Running Group as a Multi-Layered Intervention in the United Kingdom. Nurs. Rep. 2023, 13, 456–469. [Google Scholar] [CrossRef] [PubMed]
- Danielsen, K.K.; Cabral, D.; Sveaas, S.H. “Students Moving Together”, Tailored Exercise for Students Facing Mental Health Challenges-A Pilot Feasibility Study. Int. J. Environ. Res. Public Health 2023, 20, 6639. [Google Scholar] [CrossRef]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef]
- Kirschbaum, C.; Pirke, K.M.; Hellhammer, D.H. The ‘Trier Social Stress Test’—A tool for investigating psychobiological stress responses in a laboratory setting. Neuropsychobiology 1993, 28, 76–81. [Google Scholar] [CrossRef]
- EFNEP. Nutrition and Physical Activity Questionnaire-Adult. Available online: https://www.nifa.usda.gov/efnep-evaluation-adult-program (accessed on 1 June 2022).
- Peterson, K.T.; Barraco, G.; Rodgers, M.; Niessner, J.; Bopp, M. Cardiometabolic Risk Factors Associated with Physical Fitness and Activity Levels: An Exploratory Study of US College Students. Int. J. Exerc. Sci. 2025, 18, 379–393. [Google Scholar] [CrossRef]
- Xiao, T.; Zhu, F.; Wang, D.; Liu, X.; Xi, S.J.; Yu, Y. Psychometric validation of the Perceived Stress Scale (PSS-10) among family caregivers of people with schizophrenia in China. BMJ Open 2023, 13, e076372. [Google Scholar] [CrossRef] [PubMed]
- Zimet, G.D.; Powell, S.S.; Farley, G.K.; Werkman, S.; Berkoff, K.A. Psychometric characteristics of the Multidimensional Scale of Perceived Social Support. J. Pers. Assess. 1990, 55, 610–617. [Google Scholar] [CrossRef] [PubMed]
- Koenings, M.; Chipman, H. Adoption, Implementation and Maintenance of the Food and Physical Activity Questionnaire for National Nutrition Education Program Evaluation. Curr. Dev. Nutr. 2020, 4, 1319. [Google Scholar] [CrossRef]
- Buesing, D.; Fourman, S.; Ulrich-Lai, Y.M. Time-limited access to palatable food reveals differential effects of psychological stress on homeostatic vs. hedonic feeding behavior in male rats. Appetite 2024, 206, 107791. [Google Scholar] [CrossRef] [PubMed]
- Stults-Kolehmainen, M.A.; Sinha, R. The effects of stress on physical activity and exercise. Sports Med. 2014, 44, 81–121. [Google Scholar] [CrossRef]
- Letang, S.K.; Lin, S.S.; Parmelee, P.A.; McDonough, I.M. Ethnoracial disparities in cognition are associated with multiple socioeconomic status-stress pathways. Cogn. Res. Princ. Implic. 2021, 6, 64. [Google Scholar] [CrossRef]
- Michels, N.; Sioen, I.; Braet, C.; Huybrechts, I.; Vanaelst, B.; Wolters, M.; De Henauw, S. Relation between salivary cortisol as stress biomarker and dietary pattern in children. Psychoneuroendocrinology 2013, 38, 1512–1520. [Google Scholar] [CrossRef]
- Kistenmacher, A.; Goetsch, J.; Ullmann, D.; Wardzinski, E.K.; Melchert, U.H.; Jauch-Chara, K.; Oltmanns, K.M. Psychosocial stress promotes food intake and enhances the neuroenergetic level in men. Stress 2018, 21, 538–547. [Google Scholar] [CrossRef]
- de Almeida Silva, F.M.; Menezes, A.S. Sedentary Behavior, Psychosocial Stress Indicators, and Health-Risk Behaviors Among Adolescents in Northeastern Brazil. J. Phys. Act. Health 2018, 15, 169–175. [Google Scholar] [CrossRef]
- Stults-Kolehmainen, M.A.; Bartholomew, J.B. Psychological stress impairs short-term muscular recovery from resistance exercise. Med. Sci. Sports Exerc. 2012, 44, 2220–2227. [Google Scholar] [CrossRef] [PubMed]
- Gubelmann, C.; Kuehner, C.; Vollenweider, P.; Marques-Vidal, P. Association of activity status and patterns with salivary cortisol: The population-based CoLaus study. Eur. J. Appl. Physiol. 2018, 118, 1507–1514. [Google Scholar] [CrossRef] [PubMed]
- Ofosu, E.F.; de Nys, L.; Connelly, J.; Ryde, G.C.; Whittaker, A.C. Dimensions of Physical Activity Are Important in Managing Anxiety in Older Adults: A Systematic Review and Meta-Analysis. J. Aging Phys. Act. 2023, 31, 679–692. [Google Scholar] [CrossRef] [PubMed]
- Paolucci, E.M.; Loukov, D.; Bowdish, D.M.E.; Heisz, J.J. Exercise reduces depression and inflammation but intensity matters. Biol. Psychol. 2018, 133, 79–84. [Google Scholar] [CrossRef]
- Kim, J.; Park, H.Y.; Lim, K. Effects of 12 Weeks of Combined Exercise on Heart Rate Variability and Dynamic Pulmonary Function in Obese and Elderly Korean Women. Iran. J. Public Health 2018, 47, 74–81. [Google Scholar]
- Cross, S.P.; Karin, E.; Staples, L.G.; Bisby, M.A.; Ryan, K.; Duke, G.; Nielssen, O.; Kayrouz, R.; Fisher, A.; Dear, B.F.; et al. Factors associated with treatment uptake, completion, and subsequent symptom improvement in a national digital mental health service. Internet Interv. 2022, 27, 100506. [Google Scholar] [CrossRef]
- Schleinzer, A.; Moosburner, A.; Anheyer, D.; Burgahn, L.; Cramer, H. Effects of yoga on stress in stressed adults: A systematic review and meta-analysis. Front. Psychiatry 2024, 15, 1437902. [Google Scholar] [CrossRef]
- Bergmann, C.; Muth, T.; Loerbroks, A. Medical students’ perceptions of stress due to academic studies and its interrelationships with other domains of life: A qualitative study. Med. Educ. Online 2019, 24, 1603526. [Google Scholar] [CrossRef]
- Childs, E.; de Wit, H. Regular exercise is associated with emotional resilience to acute stress in healthy adults. Front. Physiol. 2014, 5, 161. [Google Scholar] [CrossRef]
- Antoun, M.; Ding, D.; Bohn-Goldbaum, E.E.; Michael, S.; Edwards, K.M. Driving in an urban environment, the stress response and effects of exercise. Ergonomics 2018, 61, 1273–1281. [Google Scholar] [CrossRef]
- Popovic, B.; Popovic, D.; Macut, D.; Antic, I.B.; Isailovic, T.; Ognjanovic, S.; Bogavac, T.; Kovacevic, V.E.; Ilic, D.; Petrovic, M.; et al. Acute Response to Endurance Exercise Stress: Focus on Catabolic/Anabolic Interplay Between Cortisol, Testosterone, and Sex Hormone Binding Globulin in Professional Athletes. J. Med. Biochem. 2019, 38, 6–12. [Google Scholar] [CrossRef]
- Georgakouli, K.; Manthou, E.; Georgoulias, P.; Ziaka, A.; Fatouros, I.G.; Mastorakos, G.; Koutedakis, Y.; Theodorakis, Y.; Jamurtas, A.Z. Exercise training reduces alcohol consumption but does not affect HPA-axis activity in heavy drinkers. Physiol. Behav. 2017, 179, 276–283. [Google Scholar] [CrossRef] [PubMed]
- Creswell, J.D.; Pacilio, L.E.; Lindsay, E.K.; Brown, K.W. Brief mindfulness meditation training alters psychological and neuroendocrine responses to social evaluative stress. Psychoneuroendocrinology 2014, 44, 1–12. [Google Scholar] [CrossRef]
- Morgan, J.A.; Corrigan, F.; Baune, B.T. Effects of physical exercise on central nervous system functions: A review of brain region specific adaptations. J. Mol. Psychiatry 2015, 3, 3. [Google Scholar] [CrossRef] [PubMed]
- Sasse, S.K.; Greenwood, B.N.; Masini, C.V.; Nyhuis, T.J.; Fleshner, M.; Day, H.E.; Campeau, S. Chronic voluntary wheel running facilitates corticosterone response habituation to repeated audiogenic stress exposure in male rats. Stress. 2008, 11, 425–437. [Google Scholar] [CrossRef]
- Gamelin, F.X.; Aucouturier, J.; Iannotti, F.A.; Piscitelli, F.; Mazzarella, E.; Aveta, T.; Leriche, M.; Dupont, E.; Cieniewski-Bernard, C.; Leclair, E.; et al. Exercise training and high-fat diet elicit endocannabinoid system modifications in the rat hypothalamus and hippocampus. J. Physiol. Biochem. 2016, 73, 335–347. [Google Scholar] [CrossRef] [PubMed]
- Hegberg, N.J.; Hayes, J.P.; Hayes, S.M. Exercise Intervention in PTSD: A Narrative Review and Rationale for Implementation. Front. Psychiatry 2019, 10, 133. [Google Scholar] [CrossRef]
- Rojas, S.M.; Grzywacz, J.G.; Zapata Roblyer, M.I.; Crain, R.; Cervantes, R.C. Stressors among Hispanic adults from immigrant families in the United States: Familismo as a context for ambivalence. Cultur. Divers. Ethn. Minor. Psychol. 2016, 22, 408–416. [Google Scholar] [CrossRef]
- NCES. National Center for Education Statistics: College Student Employment. Available online: https://nces.ed.gov/programs/coe/indicator/ssa/college-student-employment (accessed on 7 July 2025).
- Valdez, L.A.; Jaeger, E.C.; Garcia, D.O.; Griffith, D.M. Breaking Down Machismo: Shifting Definitions and Embodiments of Latino Manhood in Middle-Aged Latino Men. Am. J. Men’s Health 2023, 17, 15579883231195118. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| MIPE Intervention (n = 10) | ||||
|---|---|---|---|---|
| Before | After | p-value | Cohen’s d | |
| Body weight (kg) | 61.50 ± 4.43 | 62.01 ± 4.42 | 0.180 | −0.459 |
| BMI | 23.65 ± 1.71 | 23.84± 1.67 | 0.162 | −0.476 |
| Waist (cm) | 74.39 ± 3.47 | 79.50 ± 3.61 | 0.048 | −0.723 |
| Blood pressure (mmHg) | ||||
| Systolic | 111.70 ± 2.86 | 113.10 ±2.51 | 0.530 | −0.206 |
| Diastolic | 70.30 ± 1.75 | 72.30 ± 2.44 | 0.474 | −0.236 |
| Stress (PSS-10) | 20.90 ± 1.52 | 19.50 ± 1.47 | 0.542 | 0.201 |
| Salivary cortisol (µg/dL) | ||||
| Morning | 1.15 ± 0.15 | 1.13 ± 0.13 | 0.900 | 0.041 |
| Night | 0.52 ± 0.06 | 0.54 ± 0.08 | 0.596 | −0.174 |
| TSST-time mark | ||||
| Pre-TSST (0 min) | 0.98 ± 0.09 | 1.19 ± 0.10 | 0.096 | −0.588 |
| TSST 35 min | 1.14 ± 0.08 | 1.31 ± 0.10 | 0.204 | −0.433 |
| TSST 50 min | 1.23 ± 0.04 | 1.33 ± 0.09 | 0.250 | −0.389 |
| TSST change | ||||
| 35 min to 0 min | 0.17 ± 0.07 | 0.12 ± 0.01 | 0.533 | 0.205 |
| 50 min to 0 min | 0.25 ± 0.06 | 0.17 ± 0.04 | 0.266 | 0.375 |
| 50 min to 35 min | 0.09 ± 0.07 | 0.03 ± 0.04 | 0.385 | 0.289 |
| Yoga Intervention (n = 8) | ||||
|---|---|---|---|---|
| Before | After | p-value | Cohen’s d | |
| Body weight (kg) | 78.33 ± 8.51 | 77.18 ± 7.77 | 0.320 | 0.378 |
| BMI | 28.97 ± 3.13 | 28.50 ± 2.80 | 0.299 | 0.408 |
| Waist (cm) | 86.23 ± 6.87 | 89.25 ± 7.03 | 0.173 | −0.537 |
| Blood pressure (mmHg) | ||||
| Systolic | 127.50 ± 5.51 | 119.00 ± 2.07 | 0.147 | 0.576 |
| Diastolic | 79.13 ± 3.76 | 69.00 ± 2.09 | 0.069 | 0.760 |
| Stress (PSS-10) | 17.00 ± 1.17 | 12.63 ± 1.72 | 0.056 | 0.811 |
| Salivary cortisol (µg/dL) | ||||
| Morning | 1.19 ± 0.12 | 1.18 ± 0.07 | 0.902 | 0.045 |
| Night | 0.69 ± 0.11 | 0.68 ± 0.11 | 0.239 | 0.455 |
| TSST time mark | ||||
| Pre-TSST (0 min) | 0.98 ± 0.07 | 1.05 ± 0.06 | 0.109 | −0.650 |
| TSST 35 min | 1.20 ± 0.06 | 1.24 ± 0.05 | 0.145 | −0.579 |
| TSST 50 min | 1.18 ± 0.06 | 1.35 ± 0.03 | 0.007 | −1.338 |
| TSST change | ||||
| 35 min vs. 0 min | 0.22 ± 0.04 | 0.19 ± 0.03 | 0.598 | 0.195 |
| 50 min vs. 0 min | 0.19 ± 0.06 | 0.31 ± 0.04 | 0.047 | −0.848 |
| 50 min vs. 35 min | −0.02 ± 0.03 | 0.11 ± 0.03 | 0.030 | −0.960 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lu, H.; Saenz, F.; Raju, P.; Gutierrez, E.N.; Chew, S.A.; Nair, S. The Effects of Moderate-Intensity Physical Exercise and Yoga Interventions on Stress in Hispanic College Students: A Pilot Study. Sports 2025, 13, 266. https://doi.org/10.3390/sports13080266
Lu H, Saenz F, Raju P, Gutierrez EN, Chew SA, Nair S. The Effects of Moderate-Intensity Physical Exercise and Yoga Interventions on Stress in Hispanic College Students: A Pilot Study. Sports. 2025; 13(8):266. https://doi.org/10.3390/sports13080266
Chicago/Turabian StyleLu, Hongxing, Florentino Saenz, Preethi Raju, Ednia N. Gutierrez, Sue Anne Chew, and Saraswathy Nair. 2025. "The Effects of Moderate-Intensity Physical Exercise and Yoga Interventions on Stress in Hispanic College Students: A Pilot Study" Sports 13, no. 8: 266. https://doi.org/10.3390/sports13080266
APA StyleLu, H., Saenz, F., Raju, P., Gutierrez, E. N., Chew, S. A., & Nair, S. (2025). The Effects of Moderate-Intensity Physical Exercise and Yoga Interventions on Stress in Hispanic College Students: A Pilot Study. Sports, 13(8), 266. https://doi.org/10.3390/sports13080266