

Analysis of Differences in Injuries in Padel Players According to Sport-Specific Factors, Level of Physical Activity, Adherence to the Mediterranean Diet, and Psychological Status



Abstract
1. Introduction
2. Materials and Methods
2.1. Design
2.2. Participants
2.3. Instruments
2.4. Procedure
2.5. Data Analysis
3. Results
3.1. Analysis of Differences According to Injury Occurrence
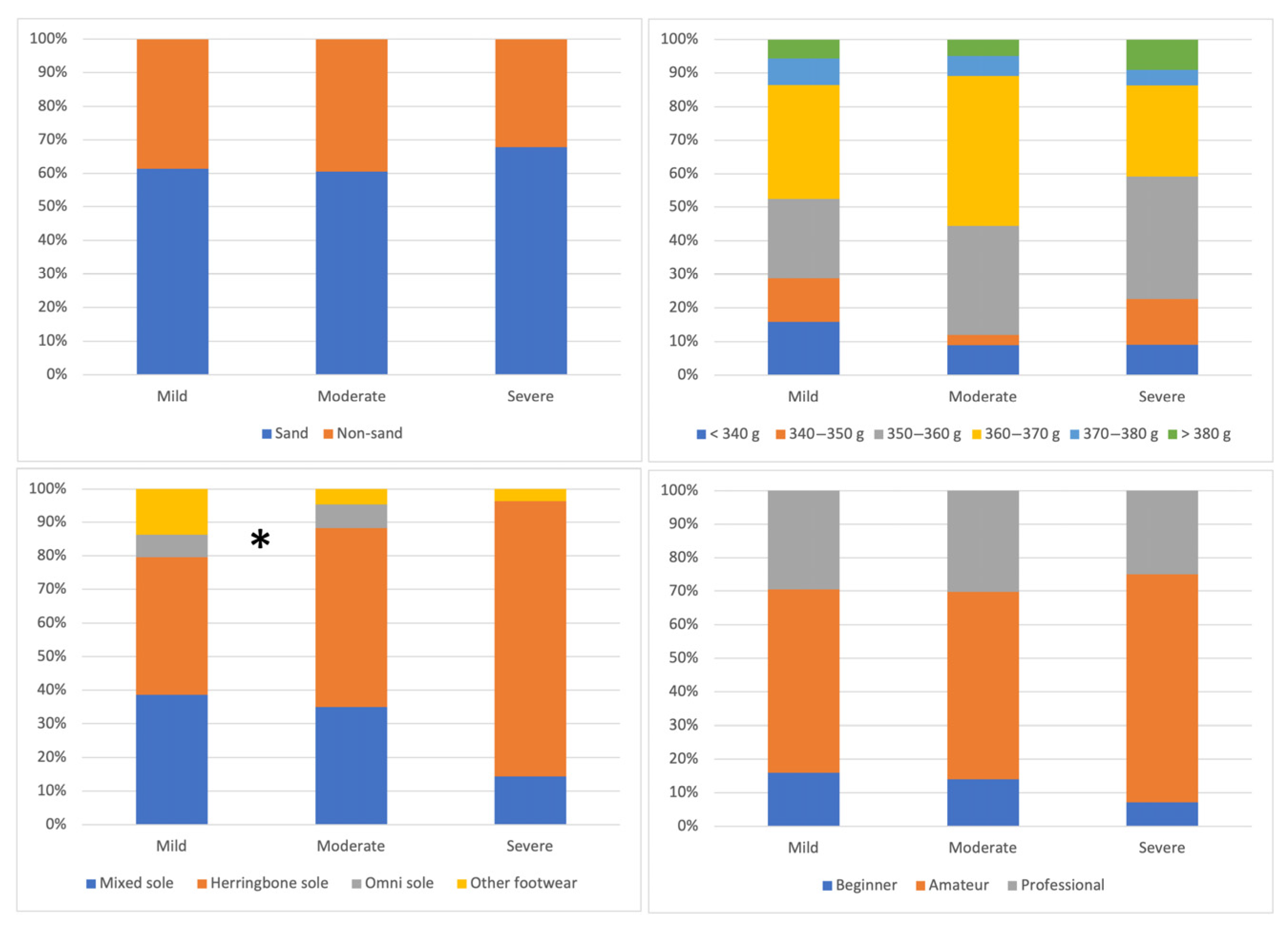
3.2. Analysis of Differences According to Injury Severity
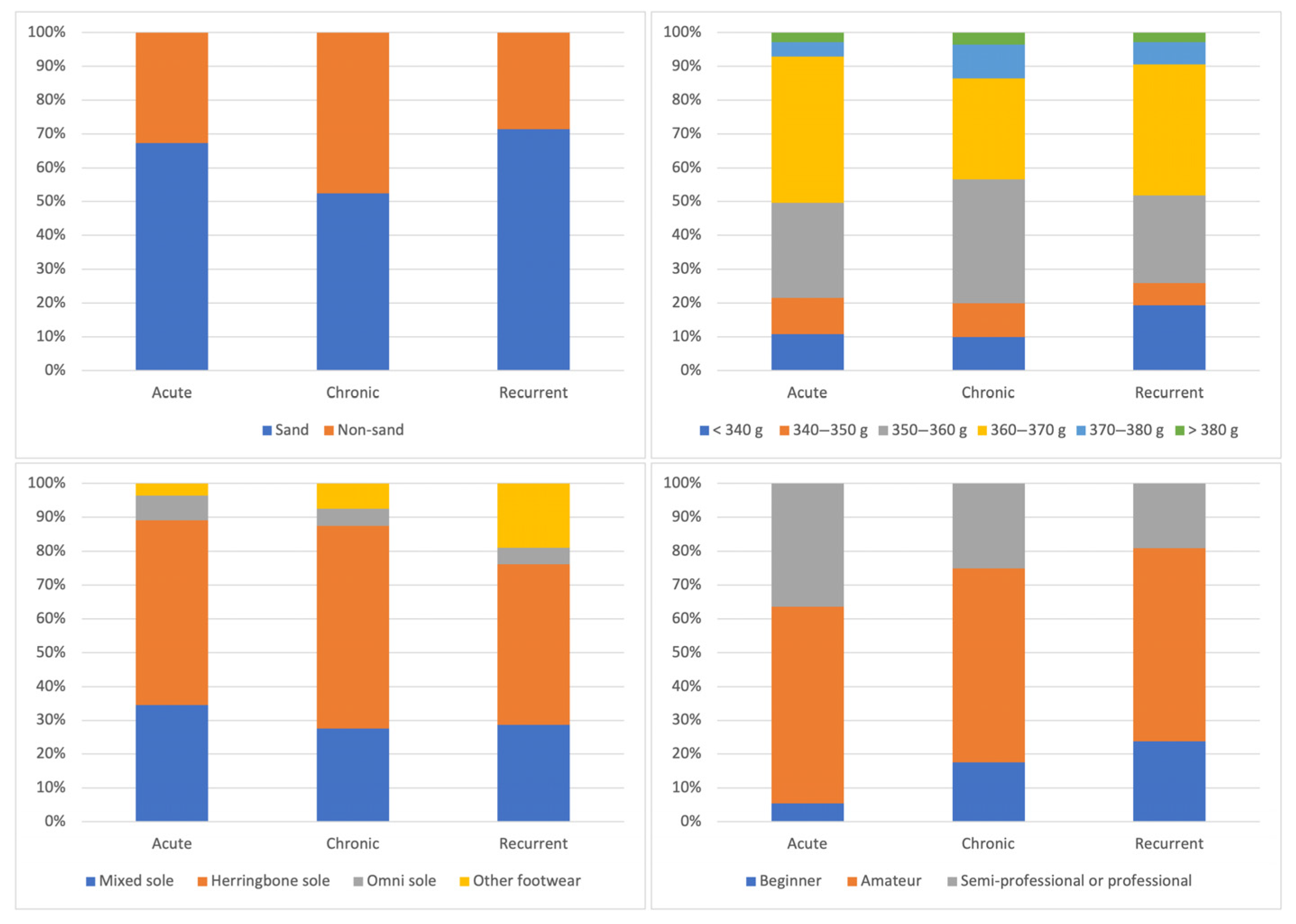
3.3. Analysis of Differences According to Injury Progression
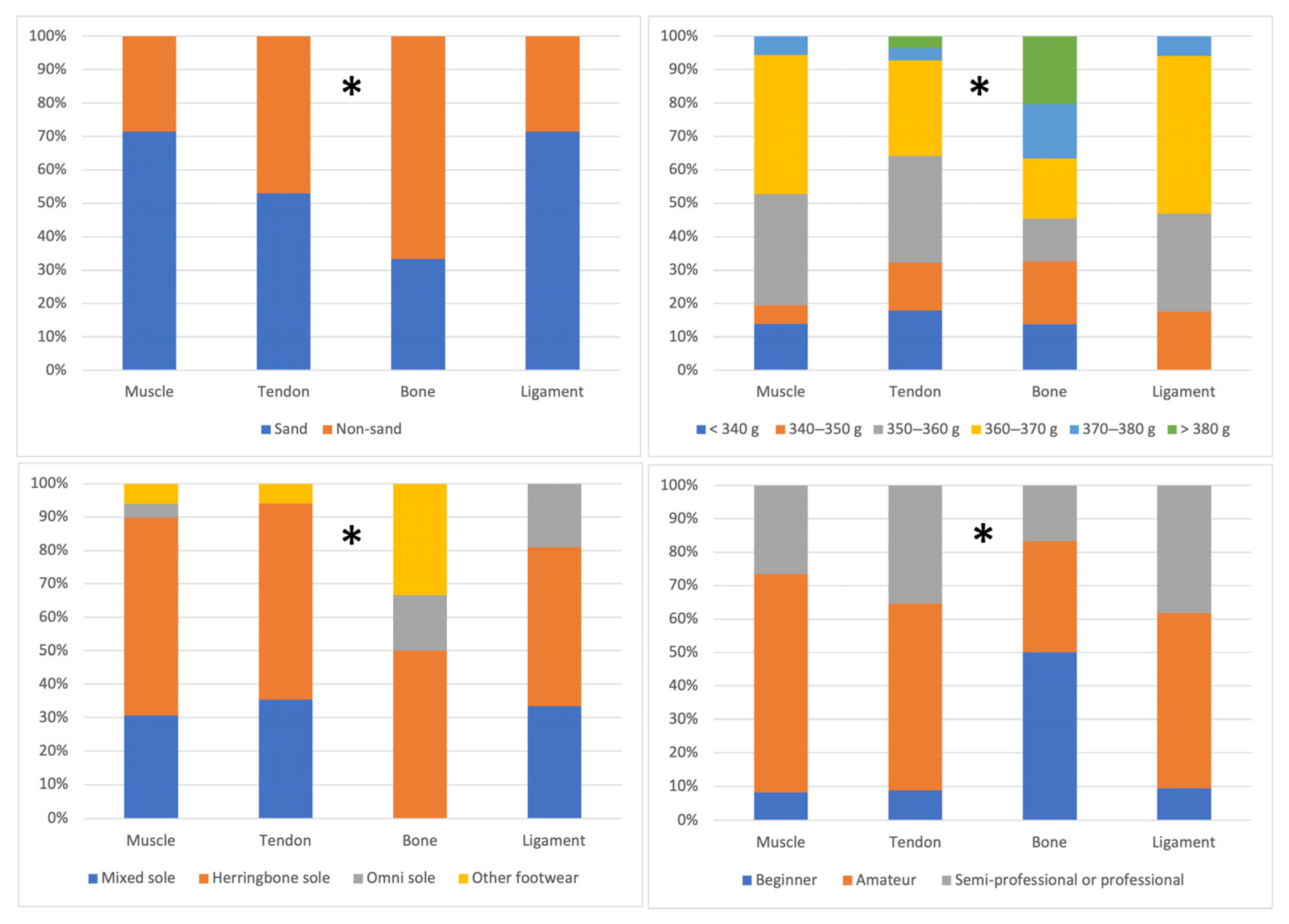
3.4. Analysis of Differences According to the Injured Anatomical Structure
4. Discussion
4.1. Differences in the Study Variables According to Injury Occurrence
4.2. Differences in the Study Variables According to Injury Severity
4.3. Differences in the Study Variables According to Injury Progression
4.4. Differences in the Study Variables According to Injured Anatomical Structure
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Almonacid, B. Perfil de Juego En Pádel de Alto Nivel; Universidad de Jaén: Jaén, Spain, 2011. [Google Scholar]
- Federación Internacional de Pádel. Reglamento de Juego Del Pádel; Federación Internacional de Pádel: Madrid, Spain, 2021. [Google Scholar]
- Villena-Serrano, M.; Castro-López, R.; Lara-Sánchez, A.; Cachón-Zagalaz, J. Revisió Sistemàtica de Les Característiques i Incidència Del Pàdel a Espanya. Apunt. Educ. Física Deportes 2016, 126, 7–22. [Google Scholar] [CrossRef]
- Martín-Miguel, I.; Escudero-Tena, A.; Muñoz, D.; Sánchez-Alcaraz, B.J. Performance Analysis in Padel: A Systematic Review. J. Hum. Kinet. 2023, 89, 213–230. [Google Scholar] [CrossRef] [PubMed]
- García-Giménez, A.; Pradas de la Fuente, F.; Castellar Otín, C.; Carrasco Páez, L. Performance Outcome Measures in Padel: A Scoping Review. Int. J. Environ. Res. Public Health 2022, 19, 4395. [Google Scholar] [CrossRef]
- Sánchez-Alcaraz, B.; Jiménez, V.; Muñoz, D.; Ramón-Llin, J. Diferencias En Los Parámetros de Carga Externa Entre El Pádel Masculino y Femenino Profesional. J. Sport Health Res. 2021, 13, 445–454. [Google Scholar]
- García-Benítez, S.; Courel-Ibáñez, J.; Pérez-Bilbao, T.; Felipe, J.L. Game Responses During Young Padel Match Play: Age and Sex Comparisons. J. Strength Cond. Res. 2018, 32, 1144–1149. [Google Scholar] [CrossRef]
- Sánchez-Alcaraz, B.; Courel-Ibáñez, J.; Díaz, J.; Grijota, F.; Muñoz, D. Effects of Score Difference and Relevance of the Point on Temporal Structure in First Division Padel Matches. J. Sport Health Res. 2019, 11, 151–160. [Google Scholar]
- Ramón-Llín, J.; Guzmán, J.; Llana, S.; Vuckovic, G.; Muñoz, D.; Sánchez-Alcaraz Martínez, B.J. Análisis de La Distancia Recorrida En Pádel En Función Del Nivel de Juego y El Número de Puntos Por Partido (Analysis of Distance Covered in Padel Based on Level of Play and Number of Points per Match). Retos 2020, 39, 205–209. [Google Scholar] [CrossRef]
- Ramón-Llin, J.; Llana, S.; Guzmán, J.; Vuckovic, G.; Muñoz, D.; Sánchez-Alcaraz, B. Analysis of Distance Covered in Padel According to the Player’s Strategic Role and Level. Acción Mot. 2020, 25, 59–67. [Google Scholar]
- Ramón-Llin, J.; Guzmán, J.; Martínez-Gallego, R.; Vučković, G.; Muñoz, D.; Sánchez-Alcaraz, B.J. Comparison of Service Tactic Formation on Players’ Movements and Point Outcome between National and Beginner Level Padel. PLoS ONE 2021, 16, e0250225. [Google Scholar] [CrossRef]
- Ramón-Llín, J.; Guzmán, J.F.; Muñoz, D.; Martínez-Gallego, R.; Sánchez-Pay, A.; Sánchez-Alcaraz, B.J. Análisis Secuencial de Golpeos Finales Del Punto En Pádel Mediante Árbol Decisional. Rev. Int. Med. Cienc. Act. Física Deporte 2022, 22, 933–947. [Google Scholar] [CrossRef]
- Sánchez-Alcaraz, B.; Muñoz, D.; Escudero-Tena, A.; Martín-Miguel, I.; Martínez-García, J. Análisis de Las Zonas de Golpeo En Pádel Profesional. Rev. Kronos 2022, 21, 1–9. [Google Scholar] [CrossRef]
- Mellado-Arbelo, O.; Vidal, E.; Usón, M. Analysis of Game Actions in Professional Male Padel. Cult. Cienc. Deporte 2019, 14, 191–201. [Google Scholar] [CrossRef]
- Díaz García, J.; Grijota Pérez, F.J.; Robles Gil, M.C.; Maynar Mariño, M.; Muñoz Marín, D. Estudio de La Carga Interna En Pádel Amateur Mediante La Frecuencia Cardíaca. Apunt. Educ. Física I Esports 2017, 1, 75–81. [Google Scholar] [CrossRef]
- Parraca, J.A.; Alegrete, J.; Villafaina, S.; Batalha, N.; Fuentes-García, J.P.; Muñoz, D.; Fernandes, O. Heart Rate Variability Monitoring during a Padel Match. Int. J. Environ. Res. Public Health 2022, 19, 3623. [Google Scholar] [CrossRef] [PubMed]
- Shaffer, F.; Ginsberg, J.P. An Overview of Heart Rate Variability Metrics and Norms. Front. Public Health 2017, 5, 258. [Google Scholar] [CrossRef]
- Castillo-Rodríguez, A.; Alvero-Cruz, J.R.; Hernández-Mendo, A.; Fernández-García, J.C. Physical and Physiological Responses in Paddle Tennis Competition. Int. J. Perform. Anal. Sport 2014, 14, 524–534. [Google Scholar] [CrossRef]
- Courel-Ibáñez, J.; Herrera-Gálvez, J.J. Fitness Testing in Padel: Performance Differences According to Players’ Competitive Level. Sci. Sports 2020, 35, e11–e19. [Google Scholar] [CrossRef]
- Müller, C.B.; Del Vecchio, F.B. Physical Fitness of Amateur Paddle Players: Comparisons between Different Competitive Levels. Motricidade 2018, 14, 42–51. [Google Scholar] [CrossRef]
- Pradas, F.; Sánchez-Pay, A.; Muñoz, D.; Sánchez-Alcaraz, B.J. Gender Differences in Physical Fitness Characteristics in Professional Padel Players. Int. J. Environ. Res. Public Health 2021, 18, 5967. [Google Scholar] [CrossRef]
- Sánchez-Alcaraz Martínez, B.J.; Orozco Ballesta, V.; Courel Ibáñez, J.; Sánchez Pay, A. Evaluación de La Velocidad, Agilidad y Fuerza En Jóvenes Jugadores de Pádel (Speed, Agility, and Strength Assessment in Young Padel Players). Retos 2018, 34, 263–266. [Google Scholar] [CrossRef]
- Sánchez-Muñoz, C.; Muros, J.J.; Cañas, J.; Courel-Ibáñez, J.; Sánchez-Alcaraz, B.J.; Zabala, M. Anthropometric and Physical Fitness Profiles of World-Class Male Padel Players. Int. J. Environ. Res. Public Health 2020, 17, 508. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Alcaraz, B.J.; Cánovas Martínez, J.; Sánchez Pay, A.; Muñoz, D. Investigación En Pádel. Revisión Sistemática. Padel Sci. J. 2022, 1, 81–118. [Google Scholar] [CrossRef]
- Rodríguez-Cayetano, A.; Amondarain-González, I.; ´Pérez-Muñoz, S.; Morales-Campo, P.T. La Ansiedad Precompetitiva y El Estado de Ánimo Postcompetitivo En Jugadores y Jugadoras de Pádel. Padel Sci. J. 2025, 3, 59–78. [Google Scholar] [CrossRef]
- Sánchez Alcaraz-Martínez, B.J.; Courel Ibáñez, J.; Díaz García, J.; Muñoz Marín, D. Estudio Descriptivo de Lesiones de Pádel: Relación Con El Género, Edad, Nivel de Los Jugadores y Localización de Las Lesiones. Rev. Andal. Med. Deport. 2019, 12, 29–34. [Google Scholar] [CrossRef]
- Dahmen, J.; Emanuel, K.S.; Fontanellas-Fes, A.; Verhagen, E.; Kerkhoffs, G.M.M.J.; Pluim, B.M. Incidence, Prevalence and Nature of Injuries in Padel: A Systematic Review. BMJ Open Sport. Exerc. Med. 2023, 9, e001607. [Google Scholar] [CrossRef]
- Castillo-Lozano, R.; Casuso-Holgado, M.J. A Comparison Musculoskeletal Injuries among Junior and Senior Paddle-Tennis Players. Sci. Sports 2015, 30, 268–274. [Google Scholar] [CrossRef]
- García González, C.; Albaladejo Vicente, R.; Villanueva Orbáiz, R.; Navarro Cabello, E. Deporte de Ocio En España: Epidemiología de Las Lesiones y Sus Consecuencias. Apunt. Educ. Física Deportes 2015, 1, 62–70. [Google Scholar] [CrossRef]
- García–Fernández, P.; Guodemar–Pérez, J.; Ruiz-López, M.; Rodríguez-López, E.S.; García-Heras, A.; Hervás–Pérez, J.P. Epidemiología Lesional En Jugadores Españoles de Padel Profesionales y Amateur. Rev. Int. Med. Cienc. Act. Física Deporte 2019, 19, 641. [Google Scholar] [CrossRef]
- Castillo-Lozano, R.; Casuso-Holgado, M.J. Incidence of Musculoskeletal Sport Injuries in a Sample of Male and Female Recreational Paddle-Tennis Players. J. Sports Med. Phys. Fit. 2017, 57, 816–821. [Google Scholar] [CrossRef]
- Delgado-García, G. Protocolos Para La Evaluación Biomecánico-Técnica y La Prevención de Lesiones Musculo-Esqueléticas En Deportistas de Raqueta; Universidad de Granada: Granada, Spain, 2021. [Google Scholar]
- Pas, H.I.M.F.L.; Bodde, S.; Kerkhoffs, G.M.M.J.; Pluim, B.; Tiemessen, I.J.H.; Tol, J.L.; Verhagen, E.; Gouttebarge, V. Systematic Development of a Tennis Injury Prevention Programme. BMJ Open Sport Exerc. Med. 2018, 4, e000350. [Google Scholar] [CrossRef]
- Prado, F.; Sánchez-Alcaraz, B.; García-Navarro, J.; Burruezo, A. Prevención de Lesiones En El Pádel. Trances 2014, 6, 175–188. [Google Scholar]
- Muñoz, D.; Coronado, M.; Robles-Gil, M.C.; Martín, M.; Escudero-Tena, A. Incidence of Upper Body Injuries in Amateur Padel Players. Int. J. Environ. Res. Public Health 2022, 19, 16858. [Google Scholar] [CrossRef]
- Ding, L.; Luo, J.; Smith, D.M.; Mackey, M.; Fu, H.; Davis, M.; Hu, Y. Effectiveness of Warm-Up Intervention Programs to Prevent Sports Injuries among Children and Adolescents: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 6336. [Google Scholar] [CrossRef] [PubMed]
- Díaz-García, J.; Rubio-Morales, A.; Manzano-Rodríguez, D.; García-Calvo, T.; Ring, C. Cognitive Priming During Warmup Enhances Sport and Exercise Performance: A Goldilocks Effect. Brain Sci. 2025, 15, 235. [Google Scholar] [CrossRef]
- Sevilla, E.P.; Pleguezuelo, T.N.; Galván, C.D.T. Valoración de Los Hábitos de Vida Saludables En Jugadores de Pádel. Rev. Andal. Med. Deport. 2015, 8, 184. [Google Scholar] [CrossRef]
- Bloemers, F.; Collard, D.; Paw, M.C.A.; Van Mechelen, W.; Twisk, J.; Verhagen, E. Physical Inactivity Is a Risk Factor for Physical Activity-Related Injuries in Children. Br. J. Sports Med. 2012, 46, 669–674. [Google Scholar] [CrossRef] [PubMed]
- Hootman, J.M. Association among Physical Activity Level, Cardiorespiratory Fitness, and Risk of Musculoskeletal Injury. Am. J. Epidemiol. 2001, 154, 251–258. [Google Scholar] [CrossRef] [PubMed]
- Melguizo-Ibáñez, E.; Ubago-Jiménez, J.L.; Sanz-Martín, D.; Alonso-Vargas, J.M. Health-Related Quality of Life and Injuries in Physical Education Students: A Multi-Group Model According to the Degree of Adherence to the Mediterranean Diet. Eur. J. Investig. Health Psychol. Educ. 2024, 14, 1140–1152. [Google Scholar] [CrossRef]
- Leão, C.; Rocha-Rodrigues, S.; Machado, I.; Lemos, J.; Leal, S.; Nobari, H. Adherence to the Mediterranean Diet in Young Male Soccer Players. BMC Nutr. 2023, 9, 101. [Google Scholar] [CrossRef] [PubMed]
- Keller, B.; Braga, A.M.; Coelho, R.W. Relação Entre a Personalidade e Lesões Musculares Em Atletas de Tênis de Campo. Rev. Bras. Med. Esporte 2013, 19, 120–122. [Google Scholar] [CrossRef]
- Senisik, S.; Koyagasioglu, O. The Effects of Psychological Factors on Injuries in Football Players. Med. J. Süleyman Demiral Univ. 2021, 28, 323–331. [Google Scholar] [CrossRef]
- Papadopoulou, S.K. Rehabilitation Nutrition for Injury Recovery of Athletes: The Role of Macronutrient Intake. Nutrients 2020, 12, 2449. [Google Scholar] [CrossRef]
- Örsçelik, A.; Acar, V.; Ataoğlu, B.; Uğurlu, B.; Ercan, S. The Impact of Adhering to a Mediterranean Diet on the Severity of Overuse Tendinopathy Symptoms. Duzce Med. J. 2024, 26, 209–213. [Google Scholar] [CrossRef]
- Olmedilla, A.; García, C.; Martínez, F. Factores Psicológicos y Vulnerabilidad a Las Lesiones Deportivas: Un Estudio En Futbolistas. Rev. Psicol. Deporte 2006, 15, 37–52. [Google Scholar]
- Gimeno, F.; Buceta, J.; Pérez-Llantada, M. Influencia de Las Variables Psicológicas En El Deporte de Competición: Evaluación Mediante El Cuestionario Características Psicológicas Relacionadas Con El Rendimiento Deportivo. Psicothema 2007, 19, 667–672. [Google Scholar]
- Vandenbroucke, J.P.; von Elm, E.; Altman, D.G.; Gøtzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and Elaboration. Int. J. Surg. 2014, 12, 1500–1524. [Google Scholar] [CrossRef] [PubMed]
- Alhammad, A.; Almalki, H.; Ghulam, H.; Al-harbi, R.; Al-harbi, S.; Al-shareif, S.; Althomali, O.; Taiar, R. Assessing the Spread of the Sport of Padel and the Prevalence and Causes of Injuries Among Padel Players. Healthcare 2025, 13, 367. [Google Scholar] [CrossRef]
- Carretero-Dios, H.; Pérez, C. Normas Para El Desarrollo y Revisión de Estudios Instrumentales. Int. J. Clin. Health Psychol. 2005, 5, 521–551. [Google Scholar]
- Hagströmer, M.; Oja, P.; Sjöström, M. The International Physical Activity Questionnaire (IPAQ): A Study of Concurrent and Construct Validity. Public Health Nutr. 2006, 9, 755–762. [Google Scholar] [CrossRef]
- García-Conesa, M.-T.; Philippou, E.; Pafilas, C.; Massaro, M.; Quarta, S.; Andrade, V.; Jorge, R.; Chervenkov, M.; Ivanova, T.; Dimitrova, D.; et al. Exploring the Validity of the 14-Item Mediterranean Diet Adherence Screener (MEDAS): A Cross-National Study in Seven European Countries around the Mediterranean Region. Nutrients 2020, 12, 2960. [Google Scholar] [CrossRef]
- Gimeno, F.; Buceta, J.M.; Pérez-Llanta, M.D.C. El Cuestionario «Características Psicológicas Relacionadas Con El Rendimiento Deportivo» (CPRD): Características Psicométricas. Análise Psicológica 2001, 11, 93–113. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: Hillsdale, MI, USA, 1988; ISBN 9781626239777. [Google Scholar]
- Hopkins, W.G.; Marshall, S.W.; Batterham, A.M.; Hanin, J. Progressive Statistics for Studies in Sports Medicine and Exercise Science. Med. Sci. Sports Exerc. 2009, 41, 3–12. [Google Scholar] [CrossRef]
- Valério, M.M.; Drews, R.; Macksoud, M.P.; Silva, F.M. da Lesões No Esporte de Rendimento: Uma Análise Em Atletas Brasileiros de Pádel. Fisioter. Pesqui. 2022, 29, 74–80. [Google Scholar] [CrossRef]
- Oscar, M.-A.; Baiget, E. Activity Profile and Physiological Demand of Padel Match Play. Kinesiology 2022, 54, 51–61. [Google Scholar] [CrossRef]
- Conde-Ripoll, R.; Escudero-Tena, A.; Clemente-Suárez, V.J.; Navarro Jimenez, E.; Bustamante-Sánchez, Á. Training under Pressure Mirrors Competition: Technical-Tactical Insights from High-Level Male Padel Players. Front. Sports Act. Living 2025, 7, 1505817. [Google Scholar] [CrossRef] [PubMed]
- Pérez, F.; de la Rubia, A.; Cañadas, E.; Lorenzo-Calvo, J.; Marquina, M.; García-Sánchez, C. Musculoskeletal Injury Prevalence in Professional Padel Players. A Retrospective Study of the 2021 Season. Phys. Ther. Sport 2023, 63, 9–16. [Google Scholar] [CrossRef]
- Courel-Ibáñez, J.; Sánchez-Alcaraz Martinez, B.J.; Muñoz Marín, D. Exploring Game Dynamics in Padel: Implications for Assessment and Training. J. Strength Cond. Res. 2019, 33, 1971–1977. [Google Scholar] [CrossRef]
- Priego Quesada, J.I.; Sanchís Almenara, M.; Kerr, Z.Y.; Alcantara, E. Examination of the Risk Factors Associated with Injured Recreational Padel Players in Spain. J. Sports Med. Phys. Fit. 2017, 58, 98–105. [Google Scholar] [CrossRef]
- Thomas, E.; Giustino, V.; Ferrisi, E.; Patti, A.; Cassarino, M.; Drid, P.; Bianco, A. Incidence of Injuries and Associated Risk Factors in a Sample of Italian Recreational Padel Players. J. Sports Med. Phys. Fit. 2023, 63, 1324–1330. [Google Scholar] [CrossRef]
- Martin, C.; Touzard, P.; Horvais, N.; Puchaud, P.; Kulpa, R.; Bideau, B.; Sorel, A. Influence of Shoe Torsional Stiffness on Foot and Ankle Biomechanics during Tennis Forehand Strokes. Eur. J. Sport Sci. 2023, 23, 914–924. [Google Scholar] [CrossRef]
- Luethi, S.M.; Frederick, E.C.; Hawes, M.R.; Nigg, B.M. Influence of Shoe Construction on Lower Extremity Kinematics and Load during Lateral Movements in Tennis. Int. J. Sport Biomech. 1986, 2, 166–174. [Google Scholar] [CrossRef]
- Kwon, J.; Jang, J. Factors Influencing Injury Severity and Frequency among Korean Sports Participants in Their 20s and 30s. Healthcare 2024, 12, 664. [Google Scholar] [CrossRef] [PubMed]
- Malmir, H.; Saneei, P.; Larijani, B.; Esmaillzadeh, A. Adherence to Mediterranean Diet in Relation to Bone Mineral Density and Risk of Fracture: A Systematic Review and Meta-Analysis of Observational Studies. Eur. J. Nutr. 2018, 57, 2147–2160. [Google Scholar] [CrossRef]
- Rizzone, K.H.; Ackerman, K.E.; Roos, K.G.; Dompier, T.P.; Kerr, Z.Y. The Epidemiology of Stress Fractures in Collegiate Student-Athletes, 2004–2005 Through 2013–2014 Academic Years. J. Athl. Train. 2017, 52, 966–975. [Google Scholar] [CrossRef]
- Griffiths, A.; Matu, J.; Whyte, E.; Akin-Nibosun, P.; Clifford, T.; Stevenson, E.; Shannon, O.M. The Mediterranean Dietary Pattern for Optimising Health and Performance in Competitive Athletes: A Narrative Review. Br. J. Nutr. 2022, 128, 1285–1298. [Google Scholar] [CrossRef] [PubMed]
- Grande del Arco, J. Fracturas de Estrés En Atletas. Rev. Int. Cienc. Podol. 1970, 12, 63. [Google Scholar] [CrossRef]
- de Sire, A.; Demeco, A.; Frizziero, A.; Marotta, N.; Spano, R.; Carozzo, S.; Costantino, C.; Ammendolia, A. Risk of Injury and Kinematic Assessment of the Shoulder Biomechanics during Strokes in Padel Players: A Cross-Sectional Study. J. Sports Med. Phys. Fit. 2024, 64, 383–391. [Google Scholar] [CrossRef]
- Olmedilla, A.; Prieto Andreu, J.; Blas Redondo, A. Historia de Lesiones y Su Relación Con Las Variables Psicológicas En Tenistas. Anu. Psicol. Clínica Salud 2009, 5, 67–74. [Google Scholar]
- Díaz-García, J.; Habay, J.; Rubio-Morales, A.; de Wachter, J.; García-Calvo, T.; Roelands, B.; Van Cutsem, J. Mental Fatigue Impairs Padel-specific Psychomotor Performance in Youth-elite Male Players. Eur. J. Sport Sci. 2024, 24, 508–517. [Google Scholar] [CrossRef]
- Binaghi, D.; Carrozza, V.; Rasumoff, A.; Burgos, J. Lesiones Musculares Deportivas En Localizaciones Atípicas. Rev. Asoc. Argent. Traumatol. Deporte 2010, 2, 91–96. [Google Scholar]
- Catalfamo, L.M.; Scozzaro, C.; Cicchiello, S.; Scozzaro, M.P.; Romeo, C.; De Rinaldis, D.; Saccà, S.; Nava, C.; Calvo, A.; De Ponte, F.S. Maxillofacial Injuries in Padel Game. J. Maxillofac. Oral. Surg. 2022, 21, 1393–1396. [Google Scholar] [CrossRef] [PubMed]
- Néri-Fuchs, J.-B.; Sedeaud, A.; Marc, A.; De Larochelambert, Q.; Toussaint, J.-F.; Brocherie, F. Medical Withdrawals in Elite Tennis in Reference to Playing Standards, Court Surfaces and Genders. J. Sci. Med. Sport 2023, 26, 296–300. [Google Scholar] [CrossRef] [PubMed]
- Sanchis Almenara, M. Contribución a La Regulación Técnica de Los Pavimentos de Hierba Artificial Para La Práctica Del Pádel a Través de Una Investigación Prenormativa; Universidad Politécnica de Valencia: Valencia, Spain, 2015. [Google Scholar]
- Torres-Luque, G.; Ramirez, A.; Cabello-Manrique, D.; Nikolaidis, T.P.; Alvero-Cruz, J.R. Match Analysis of Elite Players during Paddle Tennis Competition. Int. J. Perform. Anal. Sport 2015, 15, 1135–1144. [Google Scholar] [CrossRef]
- Pimentel, G.; Fernández, A.; Fernández, J.; Llorente, S.; Pallares, E. Revisión de Las Lesiones Deportivas Más Frecuentes En La Práctica Del Pádel. Seram 2022, 1, 1–32. [Google Scholar]
- Sánchez-Alcaraz, B.J.; Martínez-Gallego, R.; Llana, S.; Vučković, G.; Muñoz, D.; Courel-Ibáñez, J.; Sánchez-Pay, A.; Ramón-Llin, J. Ball Impact Position in Recreational Male Padel Players: Implications for Training and Injury Management. Int. J. Environ. Res. Public Health 2021, 18, 435. [Google Scholar] [CrossRef]
- Escudero-Tena, A.; Martín-Miguel, I.; Conde-Ripoll, R.; Fernández-de-Osso, A.I. Technical–Tactical Actions of Continuity in Professional and Amateur Padel: A Comparative Analysis by Sex and Level. Int. J. Sports Physiol. Perform. 2025, 20, 899–906. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | n (%) | |
|---|---|---|
| Dominant hand | ||
| Right | 199 (92.10%) | |
| Left | 17 (7.90%) | |
| Court position | ||
| Forehand side | 103 (47.70%) | |
| Backhand side | 113 (52.30%) | |
| Court surface | ||
| Sand | 141 (65.28%) | |
| Non-sand | 75 (34.72%) | |
| Racket weight (g) | ||
| <340 g | 14 (9.50%) | |
| 340–350 g | 17 (11.60%) | |
| 350–360 g | 44 (29.90%) | |
| 360–370 g | 58 (39.50%) | |
| 370–380 g | 11 (7.50%) | |
| >380 g | 3 (2.00%) | |
| Footwear type | ||
| Mixed sole | 61 (28.20%) | |
| Herringbone sole | 113 (52.30%) | |
| Omni sole | 14 (6.50%) | |
| Other footwear | 28 (13.00%) | |
| Playing level | ||
| Beginner | 56 (25.90%) | |
| Amateur | 111 (51.40%) | |
| Semi-professional or professional | 49 (22.70%) | |
| Variable | n (%) | |
|---|---|---|
| Injury while playing padel | ||
| Yes | 117 (54.20%) | |
| No | 99 (45.80%) | |
| Injured anatomical structure | ||
| Muscle | 49 (43.60%) | |
| Tendon | 34 (30.60%) | |
| Bone | 6 (6.50%) | |
| Ligament | 21 (19.30%) | |
| Injury severity | ||
| Mild | 44 (38.30%) | |
| Moderate | 43 (37.40%) | |
| Severe | 28 (24.30%) | |
| Injury location | ||
| Knee | 20 (18.20%) | |
| Elbow | 11 (10.50%) | |
| Shoulder | 16 (14.80%) | |
| Arm | 6 (6.20%) | |
| Ankle/Foot | 18 (16.50%) | |
| Leg and thigh | 19 (16.60%) | |
| Wrist | 8 (6.90%) | |
| Forearm | 5 (4.30%) | |
| Lower back | 4 (3.40%) | |
| Face | 3 (2.60%) | |
| Injury progression | ||
| Acute | 55 (47.40%) | |
| Chronic | 40 (34.50%) | |
| Recurrent | 21 (18.10%) | |
| Variable | Injured | Not Injured | Mean Diff. | t | p | 95% CI | d |
|---|---|---|---|---|---|---|---|
| Match hours | 3.91 ± 2.50 | 2.86 ± 1.89 | 1.05 | 3.43 | 0.001 | 0.44; 1.65 | 2.24 |
| Training hours | 1.51 ± 1.88 | 1.41 ± 3.17 | 0.10 | 0.28 | 0.780 | −0.59; 0.79 | 2.55 |
| Years of experience | 7.12 ± 7.62 | 3.74 ± 3.82 | 3.38 | 4.01 | <0.001 | 1.72; 5.05 | 6.18 |
| Physical activity (METS) | 7687.78 ± 2327.76 | 7314.07 ± 4699.16 | 373.71 | 0.15 | 0.880 | −4502.99; 5250.41 | 1.51 |
| AMD | 8.10 ± 1.64 | 8.53 ± 1.68 | −0.42 | −1.87 | 0.060 | −0.87; 0.02 | 1.66 |
| Psychological variables | |||||||
| Stress control | 49.37 ± 11.43 | 49.89 ± 12.54 | −0.52 | −0.32 | 0.751 | −3.74; 2.70 | 11.95 |
| Influence of performance evaluation | 30.49 ± 8.31 | 32.30 ± 8.00 | −1.82 | −1.63 | 0.114 | −4.02; 0.38 | 8.17 |
| Motivation | 17.22 ± 5.27 | 17.26 ± 5.55 | −0.04 | −0.06 | 0.963 | −1.49; 1.41 | 5.40 |
| Mental ability | 19.14 ± 5.29 | 19.45 ± 5.27 | −0.32 | −0.44 | 0.666 | −1.74; 1.10 | 5.28 |
| Team cohesion | 14.95 ± 5.90 | 14.85 ± 5.92 | 0.10 | 0.12 | 0.907 | −1.49; 1.69 | 5.91 |
| Variable | Mild | Moderate | Severe | F | p | Effect Size |
|---|---|---|---|---|---|---|
| Match hours | 3.61 ± 2.03 | 3.85 ± 2.13 | 4.38 ± 3.57 | 0.790 | 0.456 | 0.01 |
| Training hours | 1.31 ± 1.43 | 1.36 ± 1.42 | 1.96 ± 2.89 | 1.193 | 0.307 | 0.02 |
| Years of experience | 5.59 ± 5.20 | 7.02 ± 4.86 | 9.50 ± 12.55 | 2.287 | 0.106 | 0.04 |
| Physical activity (METS) | 12,352.91 ± 3732.92 | 4413.65 ± 2854.74 | 5126.89 ± 5859.34 | 1.466 | 0.235 | 0.03 |
| AMD | 8.14 ± 1.71 | 8.19 ± 1.53 | 8.11 ± 1.66 | 0.022 | 0.979 | 0.00 |
| Psychological variables | ||||||
| Stress control | 51.36 ± 12.26 | 48.53 ± 11.52 | 47.18 ± 10.06 | 1.284 | 0.281 | 0.02 |
| Influence of performance evaluation | 32.02 ± 8.89 | 30.09 ± 7.24 | 28.46 ± 8.57 | 1.659 | 0.195 | 0.03 |
| Motivation | 17.16 ± 5.75 | 16.53 ± 5.10 | 18.46 ± 4.77 | 1.140 | 0.323 | 0.02 |
| Mental ability | 18.36 ± 5.27 | 19.07 ± 5.07 | 20.79 ± 5.51 | 1.844 | 0.163 | 0.03 |
| Team cohesion | 14.95 ± 6.51 | 15.00 ± 6.20 | 14.93 ± 4.52 | 0.001 | 0.999 | 0.00 |
| Variable | Acute | Chronic | Recurrent | F | p | Effect Size |
|---|---|---|---|---|---|---|
| Match hours | 3.99 ± 2.07 | 3.98 ± 3.19 | 3.50 ± 2.12 | 0.318 | 0.728 | 0.01 |
| Training hours | 1.37 ± 1.38 | 1.60 ± 2.57 | 1.64 ± 1.54 | 0.238 | 0.788 | 0.00 |
| Years of experience | 5.71 ± 5.08 * | 9.63 ± 10.87 * | 6.19 ± 4.18 | 3.366 | 0.038 * | 0.06 |
| Physical activity (METS) | 9989.20 ± 3258.75 | 4433.23 ± 5071.63 | 7529.76 ± 1363.14 | 0.651 | 0.523 | 0.01 |
| AMD | 8.07 ± 1.80 | 8.15 ± 1.27 | 8.19 ± 1.86 | 0.048 | 0.953 | 0.00 |
| Psychological variables | ||||||
| Stress control | 51.05 ± 11.52 | 47.58 ± 11.61 | 48.19 ± 10.94 | 1.197 | 0.306 | 0.02 |
| Influence of performance evaluation | 30.75 ± 7.95 | 30.05 ± 9.74 | 30.95 ± 6.50 | 0.110 | 0.896 | 0.00 |
| Motivation | 17.35 ± 4.95 | 17.15 ± 5.50 | 16.90 ± 5.97 | 0.054 | 0.947 | 0.00 |
| Mental ability | 19.07 ± 4.72 | 18.98 ± 5.46 | 19.76 ± 6.56 | 0.165 | 0.848 | 0.00 |
| Team cohesion | 14.96 ± 5.36 | 14.73 ± 6.27 | 15.14 ± 6.84 | 0.037 | 0.963 | 0.00 |
| Variable | Muscle | Tendon | Bone | Ligament | F | p | Effect Size |
|---|---|---|---|---|---|---|---|
| Match hours | 3.62 ± 1.74 | 4.00 ± 3.27 | 3.17 ± 2.56 | 4.67 ± 2.76 | 0.654 | 0.659 | 0.03 |
| Training hours | 1.47 ± 1.50 | 1.20 ± 1.63 | 3.25 ± 5.06 | 1.45 ± 1.49 | 1.328 | 0.258 | 0.06 |
| Years of experience | 6.47 ± 4.89 * | 8.15 ± 6.17 | 15.83 ± 25.28 * | 5.57 ± 4.72 * | 2.305 | 0.049 | 0.10 |
| Physical activity (METS) | 9311.10 ± 3438.34 | 5921.38 ± 6126.37 | 4251.50 ± 2166.27 | 7310.90 ± 1451.06 | 0.132 | 0.985 | 0.01 |
| AMD | 8.18 ± 1.78 | 8.09 ± 1.62 | 7.50 ± 1.05 | 8.10 ± 1.61 | 0.360 | 0.875 | 0.02 |
| Psychological variables | |||||||
| Stress control | 49.71 ± 10.72 | 49.15 ± 10.83 | 46.67 ± 21.50 | 47.57 ± 10.55 | 1.334 | 0.255 | 0.06 |
| Influence of performance evaluation | 30.14 ± 7.66 | 32.74 ± 8.26 | 24.17 ± 13.95 | 27.81 ± 7.22 | 2.598 | 0.069 | 0.11 |
| Motivation | 17.61 ± 4.38 | 15.91 ± 6.49 | 16.67 ± 4.37 | 18.86 ± 4.91 | 1.149 | 0.339 | 0.05 |
| Mental ability | 20.69 ± 4.76 * | 16.82 ± 5.76 * | 19.50 ± 5.09 | 20.00 ± 4.79 | 2.798 | 0.020 | 0.11 |
| Team cohesion | 15.59 ± 5.12 | 12.65 ± 7.09 | 14.33 ± 5.00 | 16.86 ± 4.76 | 2.180 | 0.062 | 0.09 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rocamora-López, G.; Mateo-Orcajada, A. Analysis of Differences in Injuries in Padel Players According to Sport-Specific Factors, Level of Physical Activity, Adherence to the Mediterranean Diet, and Psychological Status. Sports 2025, 13, 228. https://doi.org/10.3390/sports13070228
Rocamora-López G, Mateo-Orcajada A. Analysis of Differences in Injuries in Padel Players According to Sport-Specific Factors, Level of Physical Activity, Adherence to the Mediterranean Diet, and Psychological Status. Sports. 2025; 13(7):228. https://doi.org/10.3390/sports13070228
Chicago/Turabian StyleRocamora-López, Guillermo, and Adrián Mateo-Orcajada. 2025. "Analysis of Differences in Injuries in Padel Players According to Sport-Specific Factors, Level of Physical Activity, Adherence to the Mediterranean Diet, and Psychological Status" Sports 13, no. 7: 228. https://doi.org/10.3390/sports13070228
APA StyleRocamora-López, G., & Mateo-Orcajada, A. (2025). Analysis of Differences in Injuries in Padel Players According to Sport-Specific Factors, Level of Physical Activity, Adherence to the Mediterranean Diet, and Psychological Status. Sports, 13(7), 228. https://doi.org/10.3390/sports13070228