Effects of Resistance Training Experience on Bone Mineral Density and Stress Fractures in Female College Athletes: A Retrospective Cohort Study

 , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Experimental Approach to the Problem
2.2. Participants
2.3. Procedures
2.4. Statistical Analyses
3. Results
3.1. SF Incidence
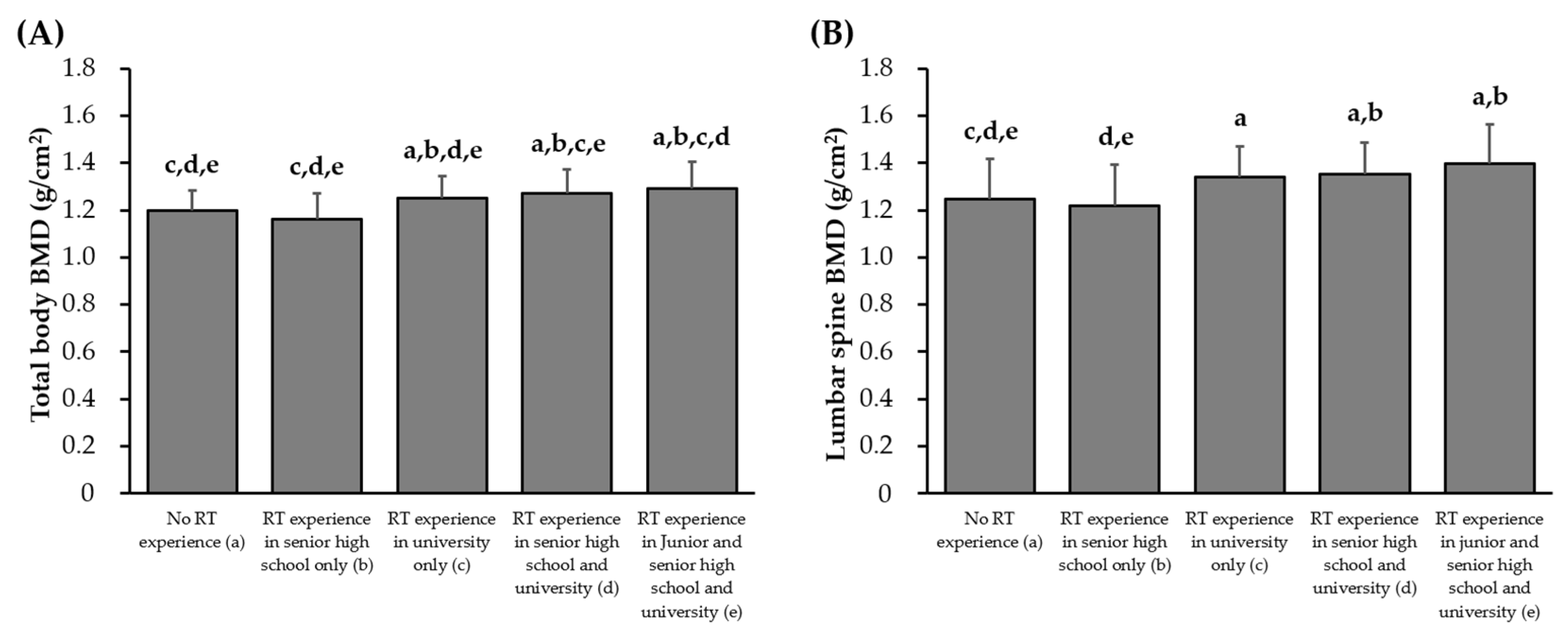
3.2. BMD Based on Each Sport Type and RT Experience
3.3. Effects of RT Experience on SFs
3.4. Comparison of BMD Between Athletes with and Without SFs During College
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BMD | Bone mineral density |
| CI | Confidence interval |
| DEXA | Dual-energy X-ray absorptiometry |
| OR | Odds ratio |
| SF | Stress fracture |
| RT | Resistance training |
References
- Iwamoto, J.; Takeda, T. Stress fractures in athletes: Review of 196 cases. J. Orthop. Sci. 2003, 8, 273–278. [Google Scholar] [CrossRef]
- Schnackenburg, K.E.; Macdonald, H.M.; Ferber, R.; Wiley, J.P.; Boyd, S.K. Bone quality and muscle strength in female athletes with lower limb stress fractures. Med. Sci. Sports Exerc. 2011, 43, 2110–2119. [Google Scholar] [CrossRef]
- Bennell, K.L.; Malcolm, S.A.; Thomas, S.A.; Reid, S.J.; Brukner, P.D.; Ebeling, P.R.; Wark, J.D. Risk factors for stress fractures in track and field athletes: A twelve-month prospective study. Am. J. Sports Med. 1996, 24, 810–818. [Google Scholar] [CrossRef]
- Rizzone, K.H.; Ackerman, K.E.; Roos, K.G.; Dompier, T.P.; Kerr, Z.Y. The epidemiology of stress fractures in collegiate student-athletes, 2004–2005 through 2013–2014 academic years. J. Athl. Train. 2017, 52, 966–975. [Google Scholar] [CrossRef]
- Ekegren, C.L.; Quested, R.; Brodrick, A. Injuries in pre-professional ballet dancers: Incidence, characteristics and consequences. J. Sci. Med. Sport 2014, 17, 271–275. [Google Scholar] [CrossRef]
- Tenforde, A.S.; Sayres, L.C.; McCurdy, M.L.; Sainani, K.L.; Fredericson, M. Identifying sex-specific risk factors for stress fractures in adolescent runners. Med. Sci. Sports Exerc. 2013, 45, 1843–1851. [Google Scholar] [CrossRef]
- Beck, B.; Drysdale, L. Risk factors, diagnosis and management of bone stress injuries in adolescent athletes: A narrative review. Sports 2021, 9, 52. [Google Scholar] [CrossRef]
- Abbott, A.; Bird, M.L.; Wild, E.; Brown, S.M.; Stewart, G.; Mulcahey, M.K. Part I: Epidemiology and risk factors for stress fractures in female athletes. Phys. Sportsmed. 2020, 48, 17–24. [Google Scholar] [CrossRef]
- Warden, S.J.; Burr, D.B.; Brukner, P.D. Stress fractures: Pathophysiology, epidemiology, and risk factors. Curr. Osteoporos. Rep. 2006, 4, 103–109. [Google Scholar] [CrossRef]
- Tenforde, A.S.; Sayres, L.C.; Sainani, K.L.; Fredericson, M. Evaluating the Relationship of Calcium and Vitamin D in the Prevention of Stress Fracture Injuries in the Young Athlete: A Review of the Literature. Phys. Med. Rehabil. 2010, 2, 945–949. [Google Scholar] [CrossRef]
- Wentz, L.; Liu, P.Y.; Haymes, E.; Ilich, J.Z. Females have a greater incidence of stress fractures than males in both military and athletic populations: A systematic review. Mil. Med. 2011, 176, 420–430. [Google Scholar] [CrossRef]
- Nattiv, A.; Loucks, A.B.; Manore, M.M.; Sanborn, C.F.; Sundgot-Borgen, J.; Warren, M.P.; American College of Sports Medicine. American College of Sports Medicine position stand: The female athlete triad. Med. Sci. Sports Exerc. 2007, 39, 1867–1882. [Google Scholar] [PubMed]
- Barrack, M.T.; Gibbs, J.C.; De Souza, M.J.; Williams, N.I.; Nichols, J.F.; Rauh, M.J.; Nattiv, A. Higher incidence of bone stress injuries with increasing female athlete triad-related risk factors: A prospective multisite study of exercising girls and women. Am. J. Sports Med. 2014, 42, 949–958. [Google Scholar] [CrossRef] [PubMed]
- De Souza, M.J.; Nattiv, A.; Joy, E.; Misra, M.; Williams, N.I.; Mallinson, R.J.; Gibbs, J.C.; Olmsted, M.; Goolsby, M.; Matheson, G.; et al. 2014 female athlete triad coalition consensus statement on treatment and return to play of the female athlete triad: 1st International Conference held in San Francisco, California, May 2012 and 2nd International Conference held in Indianapolis, Indiana, May 2013. Br. J. Sports Med. 2014, 48, 289. [Google Scholar]
- Nose-Ogura, S.; Yoshino, O.; Dohi, M.; Kigawa, M.; Harada, M.; Hiraike, O.; Onda, T.; Osuga, Y.; Fujii, T.; Saito, S. Risk factors of stress fractures due to the female athlete triad: Differences in teens and twenties. Scand. J. Med. Sci. Sports 2019, 29, 1501–1510. [Google Scholar] [CrossRef]
- Kelley, G.A.; Kelley, K.S.; Tran, Z.V. Resistance training and bone mineral density in women: A meta-analysis of controlled trials. Am. J. Phys. Med. Rehabil. 2001, 80, 65–77. [Google Scholar] [CrossRef]
- Layne, J.E.; Nelson, M.E. The effects of progressive resistance training on bone density: A review. Med. Sci. Sports Exerc. 1999, 31, 25–30. [Google Scholar] [CrossRef]
- Duplanty, A.A.; Levitt, D.E.; Hill, D.W.; McFarlin, B.K.; DiMarco, N.M.; Vingren, J.L. Resistance training is associated with higher bone mineral density among young adult male distance runners independent of physiological factors. J. Strength Cond. Res. 2018, 32, 1594–1600. [Google Scholar] [CrossRef]
- Ponzano, M.; Rodrigues, I.B.; Hosseini, Z.; Ashe, M.C.; Butt, D.A.; Chilibeck, P.D.; Stapleton, J.; Thabane, L.; Wark, J.D.; Giangregorio, L.M. Progressive resistance training for improving health-related outcomes in people at risk of fracture: A systematic review and meta-analysis of randomized controlled trials. Phys. Ther. 2021, 101, pzaa221. [Google Scholar] [CrossRef]
- Nickols-Richardson, S.M.; Miller, L.E.; Wootten, D.F.; Ramp, W.K.; Herbert, W.G. Concentric and eccentric isokinetic resistance training similarly increases muscular strength, fat-free soft tissue mass, and specific bone mineral measurements in young women. Osteoporos. Int. 2007, 18, 789–796. [Google Scholar] [CrossRef]
- Mosti, M.P.; Carlsen, T.; Aas, E.; Hoff, J.; Stunes, A.K.; Syversen, U. Maximal strength training improves bone mineral density and neuromuscular performance in young adult women. J. Strength Cond. Res. 2014, 28, 2935–2945. [Google Scholar] [CrossRef]
- Kobayashi, T.; Seki, S.; Hwang, I. Effects of resistance training on bone mineral density and resting serum hormones in female collegiate distance runners: A randomized controlled pilot trial. J. Sports Med. Phys. Fitness 2023, 63, 765–772. [Google Scholar] [CrossRef]
- Nussbaum, E.D.; Bjornaraa, J.; Gatt, C.J., Jr. Identifying factors that contribute to adolescent bony stress injury in secondary school athletes: A comparative analysis with a healthy athletic control group. Sports Health 2019, 11, 375–379. [Google Scholar] [CrossRef]
- Tenforde, A.S.; Carlson, J.L.; Sainani, K.L.; Chang, A.O.; Kim, J.H.; Golden, N.H.; Fredericson, M. Sport and triad risk factors influence bone mineral density in collegiate athletes. Med. Sci. Sports Exerc. 2018, 50, 2536–2543. [Google Scholar] [CrossRef]
- Lauersen, J.B.; Andersen, T.E.; Andersen, L.B. Strength training as superior, dose-dependent and safe prevention of acute and overuse sports injuries: A systematic review, qualitative analysis and meta-analysis. Br. J. Sports Med. 2018, 52, 1557–1563. [Google Scholar] [CrossRef]
- Frost, H.M. Bone “mass” and the “mechanostat”: A proposal. Anat. Rec. 1987, 219, 1–9. [Google Scholar] [CrossRef]
- Kohrt, W.M.; Bloomfield, S.A.; Little, K.D.; Nelson, M.E.; Yingling, V.R.; American College of Sports Medicine. American College of Sports Medicine Position Stand: Physical activity and bone health. Med. Sci. Sports Exerc. 2004, 36, 1985–1996. [Google Scholar] [CrossRef]
- Kraemer, W.J.; Marchitelli, L.; Gordon, S.E.; Harman, E.; Dziados, J.E.; Mello, R.; Frykman, P.; McCurry, D.; Fleck, S.J. Hormonal and growth factor responses to heavy resistance exercise protocols. J. Appl. Physiol. (1985) 1990, 69, 1442–1450. [Google Scholar] [CrossRef]
- Myburgh, K.H.; Hutchins, J.; Fataar, A.B.; Hough, S.F.; Noakes, T.D. Low bone density is an etiologic factor for stress fractures in athletes. Ann. Intern. Med. 1990, 113, 754–759. [Google Scholar] [CrossRef]
- Carbon, R.; Sambrook, P.N.; Deakin, V.; Fricker, P.; Eisman, J.A.; Kelly, P.; Maguire, K.; Yeates, M.G. Bone density of elite female athletes with stress fractures. Med. J. Aust. 1990, 153, 373–376. [Google Scholar] [CrossRef]
- Grimston, S.K.; Engsberg, J.R.; Kloiber, R.; Hanley, D.A. Bone mass, external loads, and stress fracture in female runners. Int. J. Sport Biomech. 1991, 7, 293–302. [Google Scholar] [CrossRef]
- Korpelainen, R.; Orava, S.; Karpakka, J.; Siira, P.; Hulkko, A. Risk factors for recurrent stress fractures in athletes. Am. J. Sports Med. 2001, 29, 304–310. [Google Scholar] [CrossRef]
- Paul, I.L.; Munro, M.B.; Abernethy, P.J.; Simon, S.R.; Radin, E.L.; Rose, R.M. Musculo-skeletal shock absorption: Relative contribution of bone and soft tissues at various frequencies. J. Biomech. 1978, 11, 237–239. [Google Scholar] [CrossRef]
- NIH Consensus Development Panel on Osteoporosis Prevention, Diagnosis, and Therapy. Osteoporosis prevention, diagnosis, and therapy. JAMA 2001, 285, 785–795. [Google Scholar] [CrossRef]
- Fonseca, H.; Moreira-Gonçalves, D.; Coriolano, H.J.A.; Duarte, J.A. Bone quality: The determinants of bone strength and fragility. Sports Med. 2014, 44, 37–53. [Google Scholar] [CrossRef] [PubMed]
- Franklyn, M.; Oakes, B.; Field, B.; Wells, P.; Morgan, D. Section modulus is the optimum geometric predictor for stress fractures and medial tibial stress syndrome in both male and female athletes. Am. J. Sports Med. 2008, 36, 1179–1189. [Google Scholar] [CrossRef]
- Popp, K.L.; Frye, A.C.; Stovitz, S.D.; Hughes, J.M. Bone geometry and lower extremity bone stress injuries in male runners. J. Sci. Med. Sport 2020, 23, 145–150. [Google Scholar] [CrossRef]
- Faigenbaum, A.D.; Myer, G.D. Resistance training among young athletes: Safety, efficacy and injury prevention effects. Br. J. Sports Med. 2010, 44, 56–63. [Google Scholar] [CrossRef]
- Faigenbaum, A.D.; Kraemer, W.J.; Blimkie, C.J.; Jeffreys, I.; Micheli, L.J.; Nitka, M.; Rowland, T.W. Youth resistance training: Updated position statement paper from the national strength and conditioning association. J. Strength Cond. Res. 2009, 23, S60–S79. [Google Scholar] [CrossRef]
- Lloyd, R.S.; Faigenbaum, A.D.; Stone, M.H.; Oliver, J.L.; Jeffreys, I.; Moody, J.A.; Brewer, C.; Pierce, K.C.; McCambridge, T.M.; Howard, R.; et al. Position statement on youth resistance training: The 2014 International Consensus. Br. J. Sports Med. 2014, 48, 498–505. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| All Participants (n = 492) | |
|---|---|
| Age (y) | 20.2 ± 1.4 |
| Height (cm) | 161.0 ± 6.0 |
| Weight (kg) | 57.8 ± 7.6 |
| BMI (kg/m2) | 22.3 ± 2.5 |
| %Fat (%) | 14.2 ± 3.9 |
| Fat mass (kg) | 41.3 ± 4.6 |
| Fat free mass (kg) | 24.2 ± 4.3 |
| Categories | n | Non-Stress Fractures | Stress Fractures | Unadjusted Model | Model Adjusted for Sport Type | Model Adjusted for Sport Type and University Year | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| OR (95%CI) | p | OR (95%CI) | p | OR (95%CI) | p | |||||||
| RT experience | ||||||||||||
| No experience | 51 | 32 | (62.7%) | 19 | (37.3%) | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | ||||
| Senior high school only | 10 | 8 | (80.0%) | 2 | (20.0%) | 0.44 (0.09–2.32) | 0.336 | 0.57 (0.10–3.30) | 0.532 | 0.50 (0.08–3.33) | 0.477 | |
| University only | 191 | 175 | (91.6%) | 16 | (8.4%) | 0.16 (0.08–0.35) | <0.001 | 0.50 (0.16–1.56) | 0.230 | 0.35 (0.11–1.13) | 0.080 | |
| Senior high school and university | 189 | 174 | (92.1%) | 15 | (7.9%) | 0.16 (0.07–0.35) | <0.001 | 0.50 (0.15–1.64) | 0.249 | 0.42 (0.13–1.41) | 0.161 | |
| Junior and senior high school and university | 51 | 50 | (98.0%) | 1 | (2.0%) | 0.04 (0.01–0.28) | 0.002 | 0.10 (0.01–0.91) | 0.041 | 0.06 (0.01–0.59) | 0.016 | |
| Sport type | ||||||||||||
| Low-impact | 40 | 22 | (55.0%) | 18 | (45.0%) | 1.00 (reference) | 1.00 (reference) | |||||
| Non-impact | 77 | 73 | (94.8%) | 4 | (5.2%) | 0.13 (0.03–0.59) | 0.009 | 0.15 (0.03–0.70) | 0.016 | |||
| Multidirectional | 219 | 202 | (92.2%) | 17 | (7.8%) | 0.17 (0.06–0.54) | 0.002 | 0.25 (0.08–0.79) | 0.018 | |||
| High-impact | 156 | 142 | (91.0%) | 14 | (9.0%) | 0.24 (0.07–0.84) | 0.026 | 0.45 (0.12–1.64) | 0.227 | |||
| University year | ||||||||||||
| First-year | 103 | 101 | (98.1%) | 2 | (1.9%) | 1.00 (reference) | ||||||
| Second-year | 118 | 112 | (94.9%) | 6 | (5.1%) | 2.69 (0.52–14.07) | 0.240 | |||||
| Third-year | 88 | 79 | (89.8%) | 9 | (10.2%) | 6.25 (1.27–30.78) | 0.024 | |||||
| Fourth-year | 183 | 147 | (80.3%) | 36 | (19.7%) | 12.97 (2.94–57.29) | <0.001 | |||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kobayashi, T.; Seki, S.; Liu, M.; Chiba, I.; Oguro, T.; Makino, Y.; Kobayashi, Y.; Matsumoto, H.; Hwang, I. Effects of Resistance Training Experience on Bone Mineral Density and Stress Fractures in Female College Athletes: A Retrospective Cohort Study. Sports 2025, 13, 227. https://doi.org/10.3390/sports13070227
Kobayashi T, Seki S, Liu M, Chiba I, Oguro T, Makino Y, Kobayashi Y, Matsumoto H, Hwang I. Effects of Resistance Training Experience on Bone Mineral Density and Stress Fractures in Female College Athletes: A Retrospective Cohort Study. Sports. 2025; 13(7):227. https://doi.org/10.3390/sports13070227
Chicago/Turabian StyleKobayashi, Tetsuro, Shotaro Seki, Mengrong Liu, Itaru Chiba, Takashi Oguro, Yosuke Makino, Yasunaga Kobayashi, Hiroyuki Matsumoto, and Inkwan Hwang. 2025. "Effects of Resistance Training Experience on Bone Mineral Density and Stress Fractures in Female College Athletes: A Retrospective Cohort Study" Sports 13, no. 7: 227. https://doi.org/10.3390/sports13070227
APA StyleKobayashi, T., Seki, S., Liu, M., Chiba, I., Oguro, T., Makino, Y., Kobayashi, Y., Matsumoto, H., & Hwang, I. (2025). Effects of Resistance Training Experience on Bone Mineral Density and Stress Fractures in Female College Athletes: A Retrospective Cohort Study. Sports, 13(7), 227. https://doi.org/10.3390/sports13070227