

Initial Effects of Dynamic Tape on Foot Arch Height Under Cyclic Loading: A Pilot Study Among University Students


 and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Subjects
2.2. Taping Technique
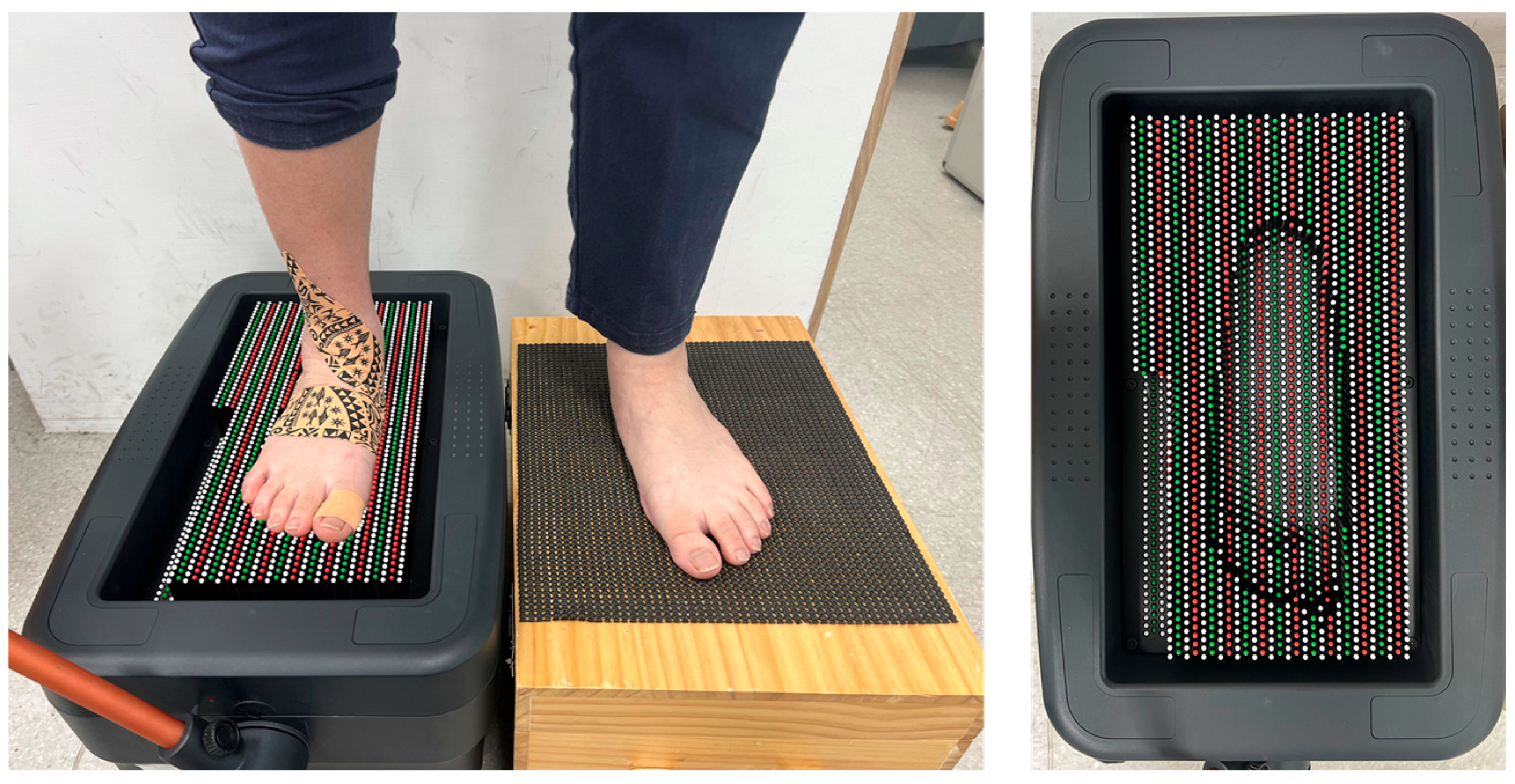
2.3. Apparatus
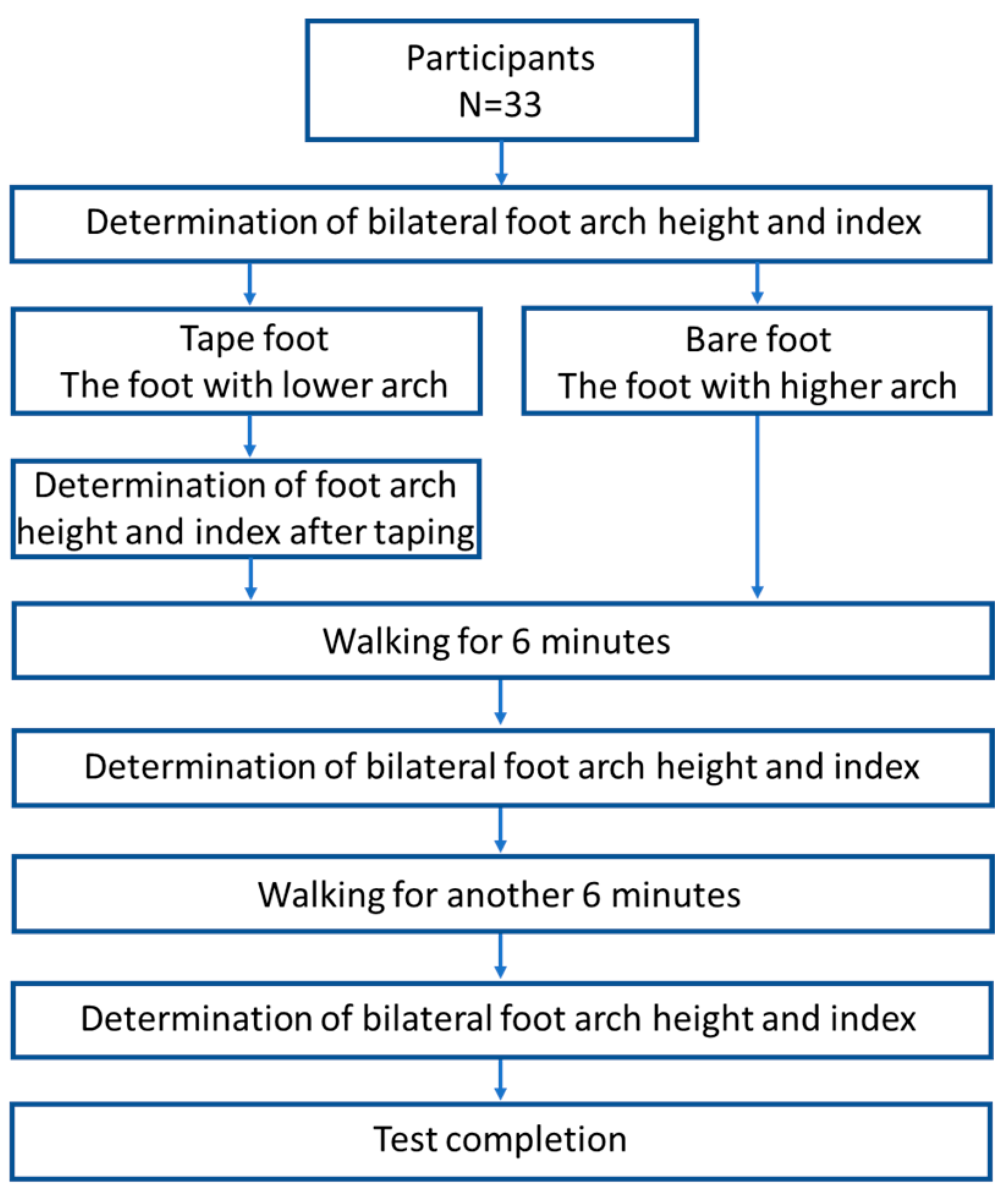
2.4. Test Procedure
2.5. Index
2.6. Data Analysis
2.7. Limitations
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Van Boerum, D.H.; Sangeorzan, B.J. Biomechanics and pathophysiology of flat foot. Foot Ankle Clin. 2003, 8, 419–430. [Google Scholar] [CrossRef]
- Chen, Y.N.; Chang, C.W.; Li, C.T.; Chang, C.H.; Lin, C.F. Finite element analysis of plantar fascia during walking: A quasi-static simulation. Foot Ankle Int. 2015, 36, 90–97. [Google Scholar] [CrossRef]
- Tourillon, R.; Gojanovic, B.; Fourchet, F. How to Evaluate and Improve Foot Strength in Athletes: An Update. Front. Sports Act. Living 2019, 1, 46. [Google Scholar] [CrossRef]
- Winters, M. The diagnosis and management of medial tibial stress syndrome: An evidence update. Unfallchirurg 2020, 123 (Suppl. S1), 15–19. [Google Scholar] [CrossRef]
- Reshef, N.; Guelich, D.R. Medial tibial stress syndrome. Clin. Sports Med. 2012, 31, 273–290. [Google Scholar] [CrossRef]
- Reinking, M.F.; Austin, T.M.; Richter, R.R.; Krieger, M.M. Medial Tibial Stress Syndrome in Active Individuals: A Systematic Review and Meta-analysis of Risk Factors. Sports Health 2017, 9, 252–261. [Google Scholar] [CrossRef]
- Trojian, T.; Tucker, A.K. Plantar Fasciitis. Am. Fam. Physician 2019, 99, 744–750. [Google Scholar]
- Kashif, M.; Albalwi, A.; Alharbi, A.; Iram, H.; Manzoor, N. Comparison of subtalar mobilisation with conventional physiotherapy treatment for the management of plantar fasciitis. J. Pak. Med. Assoc. 2021, 71, 2705–2709. [Google Scholar]
- Sánchez-Rodríguez, R.; Valle-Estévez, S.; Fraile-García, P.A.; Martínez-Nova, A.; Gómez-Martín, B.; Escamilla-Martínez, E. Modification of Pronated Foot Posture after a Program of Therapeutic Exercises. Int. J. Environ. Res. Public Health 2020, 17, 8406. [Google Scholar] [CrossRef]
- Pabón-Carrasco, M.; Castro-Méndez, A.; Vilar-Palomo, S.; Jiménez-Cebrián, A.M.; García-Paya, I.; Palomo-Toucedo, I.C. Randomized Clinical Trial: The Effect of Exercise of the Intrinsic Muscle on Foot Pronation. Int. J. Environ. Res. Public Health 2020, 17, 4882. [Google Scholar] [CrossRef]
- Naderi, A.; Degens, H.; Sakinepoor, A. Arch-support foot-orthoses normalize dynamic in-shoe foot pressure distribution in medial tibial stress syndrome. Eur. J. Sport. Sci. 2019, 19, 247–257. [Google Scholar] [CrossRef]
- Kirmizi, M.; Sengul, Y.S.; Akcali, O.; Angin, S. Effects of foot exercises and customized arch support insoles on foot posture, plantar force distribution, and balance in people with flexible flatfoot: A randomized controlled trial. Gait Posture 2024, 113, 106–114. [Google Scholar] [CrossRef]
- Peng, Y.; Wong, D.W.-C.; Chen, T.L.-W.; Wang, Y.; Zhang, G.; Yan, F.; Zhang, M. Influence of arch support heights on the internal foot mechanics of flatfoot during walking: A muscle-driven finite element analysis. Comput. Biol. Med. 2021, 132, 104355. [Google Scholar] [CrossRef]
- Kogler, G.F.; Solomonidis, S.E.; Paul, J.P. Biomechanics of longitudinal arch support mechanisms in foot orthoses and their effect on plantar aponeurosis strain. Clin. Biomech. 1996, 11, 243–252. [Google Scholar] [CrossRef]
- Bishop, C.; Arnold, J.B.; May, T. Effects of Taping and Orthoses on Foot Biomechanics in Adults with Flat-Arched Feet. Med. Sci. Sports Exerc. 2016, 48, 689–696. [Google Scholar] [CrossRef]
- Newell, T.; Simon, J.; Docherty, C.L. Arch-Taping Techniques for Altering Navicular Height and Plantar Pressures During Activity. J. Athl. Train. 2015, 50, 825–832. [Google Scholar] [CrossRef]
- Tang, M.; Zeng, Z.; Li, C.; Hu, X.; Wang, L. Acute effects of athletic taping on arch deformity and plantar pressure in young female adults with flexible flatfoot. Gait Posture 2024, 108, 250–256. [Google Scholar] [CrossRef]
- Tahmasbi, A.; Shadmehr, A.; Moghadam, B.A.; Fereydounnia, S. Does Kinesio taping of tibialis posterior or peroneus longus have an immediate effect on improving foot posture, dynamic balance, and biomechanical variables in young women with flexible flatfoot? Foot 2023, 56, 102032. [Google Scholar] [CrossRef]
- Bruening, D.A.; Messick, C.L.; Waid, D.C.; Krupp, T.D.; Stringer, J.R.; Parry, D.J.; Berry, L.J. For plantar taping, direction of elasticity matters. Sci. Rep. 2023, 13, 22811. [Google Scholar] [CrossRef]
- Yoho, R.; Rivera, J.J.; Renschler, R.; Vardaxis, V.G.; Dikis, J. A biomechanical analysis of the effects of low-Dye taping on arch deformation during gait. Foot 2012, 22, 283–286. [Google Scholar] [CrossRef]
- Song, J.; Lin, J.; Austin, T.; Teter, R.; Oshiokpekhai, K.; An, M.; Tran, H.; Palamarchuk, H.; Pettineo, S. Does QUICK TAPE Offer Comparable Support and Off-loading as Low-Dye Taping? J. Am. Podiatr. Med. Assoc. 2021, 111, 09. [Google Scholar]
- Kim, D.H.; Lee, Y. Effect of Dynamic Taping versus Kinesiology Taping on Pain, Foot Function, Balance, and Foot Pressure in 3 Groups of Plantar Fasciitis Patients: A Randomized Clinical Study. Med. Sci. Monit. 2023, 29, e941043. [Google Scholar] [CrossRef]
- de Ru, E.; Mikołajewska, E. Skin irritation incidence following kinesiology tape use in patients with neurological disorders: Multicenter observation. In Annales Academiae Medicae Silesiensis; Śląski Uniwersytet Medyczny w Katowicach: Katowice, Poland, 2017. [Google Scholar]
- Gatt, M.; Willis, S.; Leuschner, S. A meta-analysis of the effectiveness and safety of kinesiology taping in the management of cancer-related lymphoedema. Eur. J. Cancer Care 2017, 26, e12510. [Google Scholar] [CrossRef]
- Hertzog, M.A. Considerations in determining sample size for pilot studies. Res. Nurs. Health 2008, 31, 180–191. [Google Scholar] [CrossRef]
- Chen, T.-Y.; Kuo, C.-C.; Hung, L.-W.; Lee, W.-C.; Lo, J.-H.; Lu, H.-L.; Lu, T.-W. Test-Retest Reliability of Sole Morphology Measurements Using a Novel Single-Image-Based Pin-Array Impression Reconstruction Method. Appl. Sci. 2021, 11, 4447. [Google Scholar] [CrossRef]
- Aguilar, M.B.; Abián-Vicén, J.; Halstead, J.; Gijon-Nogueron, G. Effectiveness of neuromuscular taping on pronated foot posture and walking plantar pressures in amateur runners. J. Sci. Med. Sport 2016, 19, 348–353. [Google Scholar] [CrossRef]
- Warren, B.L. Plantar fasciitis in runners. Treatment and prevention. Sports Med. 1990, 10, 338–345. [Google Scholar]
- Wu, W.T.; Hong, C.Z.; Chou, L.W. The Kinesio Taping Method for Myofascial Pain Control. Evid. Based Complement. Altern. Med. 2015, 2015, 950519. [Google Scholar]
- Matheus, J.P.C.; Zille, R.R.; Matheus, L.B.G.; Lemos, T.V.; Carregaro, R.L.; Shimano, A.C. Comparison of the mechanical properties of therapeutic elastic tapes used in sports and clinical practice. Phys. Ther. Sport 2017, 24, 74–78. [Google Scholar] [CrossRef]
- Luque-Suarez, A.; Gijon-Nogueron, G.; Baron-Lopez, F.J.; Labajos-Manzanares, M.T.; Hush, J.; Hancock, M.J. Effects of kinesiotaping on foot posture in participants with pronated foot: A quasi-randomised, double-blind study. Physiotherapy 2014, 100, 36–40. [Google Scholar] [CrossRef]
- Ordahan, B. Extracorporeal Shockwave Therapy Versus Kinesiology Taping in the Management of Plantar Fasciitis: A Randomized Clinical Trial. Arch. Rheumatol. 2017, 32, 227–233. [Google Scholar] [CrossRef] [PubMed]
- Botsis, A.E.; Schwarz, N.A.; Harper, M.E.; Liu, W.; Rooney, C.A.; Gurchiek, L.R.; Kovaleski, J.E. Effect of Kinesio® Taping on Ankle Complex Motion and Stiffness and Jump Landing Time to Stabilization in Female Ballet Dancers. J. Funct. Morphol. Kinesiol. 2019, 4, 19. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.L.-W.; Wong, D.W.-C.; Peng, Y.; Zhang, M. Prediction on the plantar fascia strain offload upon Fascia taping and Low-Dye taping during running. J. Orthop. Transl. 2020, 20, 113–121. [Google Scholar]
- Song, Y.; Cen, X.; Wang, M.; Bálint, K.; Tan, Q.; Sun, D.; Gao, S.; Li, F.; Gu, Y.; Wang, Y.; et al. The influence of simulated worn shoe and foot inversion on heel internal biomechanics during running impact: A subject-specific finite element analysis. J. Biomech. 2025, 180, 112517. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
| Participants (N = 33) | Range | |
|---|---|---|
| Age, years | 20.33 ± 0.72 | 19–22 |
| Body height, cm | 164.15 ± 6.66 | 151–177 |
| Body weight, kg | 58.76 ± 12.97 | 49–100 |
| Rt/Lt | 3/32 | - |
| Women/men | 22/11 | - |
| Index | Condition | Baseline | 6 min | 12 min | p | |
|---|---|---|---|---|---|---|
| Total cases | Arch height (mm) | Taped foot | 9.88 ± 3.29 | 9.39 ± 3.33 | 9.61 ± 3.43 | 0.074 |
| Untaped foot | 13.24 ± 4.24 | 12.24 ± 4.04 | 12.82 ± 4.21 | 0.055 | ||
| Difference between taped and untaped foot | −3.36 ± 2.68 | −2.89 ± 2.22 | −3.21 ± 2.41 | 0.515 | ||
| Arch index | Taped foot | 0.258 ± 0.086 | 0.273 ± 0.085 | 0.279 ± 0.072 * | 0.029 | |
| Untaped foot | 0.234 ± 0.081 | 0.240 ± 0.085 | 0.240 ± 0.083 | 0.195 | ||
| Difference between taped and untaped foot | 0.025 ± 0.073 | 0.034 ± 0.082 | 0.039 ± 0.083 | 0.845 | ||
| Women | Arch height (mm) | Taped foot | 9.68 ± 3.43 | 8.95 ± 3.37 * | 9.41 ± 3.54 | 0.023 |
| Untaped foot | 12.95 ± 4.31 | 12 ± 3.92 | 12.64 ± 4.36 | 0.106 | ||
| Difference between taped and untaped foot | −3.27 ± 2.99 | −3.05 ± 2.08 | −3.23 ± 2.78 | 0.753 | ||
| Arch index | Taped foot | 0.254 ± 0.09 | 0.279 ± 0.087 | 0.275 ± 0.077 | 0.133 | |
| Untaped foot | 0.225 ± 0.091 | 0.233 ± 0.089 | 0.232 ± 0.088 | 0.071 | ||
| Difference between taped and untaped foot | 0.029 ± 0.080 | 0.045 ± 0.090 | 0.043 ± 0.096 | 0.919 | ||
| Men | Arch height (mm) | Taped foot | 10.27 ± 3.10 | 10.27 ± 3.23 | 10.00 ± 3.32 | 0.809 |
| Untaped foot | 13.82 ± 4.24 | 12.73 ± 4.43 | 13.18 ± 4.07 | 0.291 | ||
| Difference between taped and untaped foot | −3.55 ± 2.02 | −2.45 ± 2.54 | −3.18 ± 1.54 | 0.256 | ||
| Arch index | Taped foot | 0.267 ± 0.080 | 0.263 ± 0.084 | 0.285 ± 0.063 | 0.076 | |
| Untaped foot | 0.251 ± 0.055 | 0.253 ± 0.079 | 0.255 ± 0.072 | 0.924 | ||
| Difference between taped and untaped foot | 0.016 ± 0.057 | 0.010 ± 0.060 | 0.030 ± 0.050 | 0.311 |
| Index | Condition | 6 min Later | 12 min Later | p | |
|---|---|---|---|---|---|
| Total cases | Difference in arch height (mm) | Taped foot | −0.48 ± 1.23 | −0.27 ± 1.66 | 0.965 |
| Untaped foot | −1 ± 2.40 | −0.42 ± 1.89 | 0.082 | ||
| p | 0.289 | 0.971 | |||
| Arch index | Taped foot | 0.015 ± 0.061 | 0.020 ± 0.062 | 0.330 | |
| Untaped foot | 0.006 ± 0.061 | 0.006 ± 0.051 | 0.715 | ||
| p | 0.543 | 0.360 | |||
| Women | Difference in arch height (mm) | Taped foot | −0.73 ± 1.20 | −0.28 ± 1.88 | 0.472 |
| Untaped foot | −0.95 ± 2.61 | −0.32 ± 2.19 | 0.172 | ||
| p | 0.920 | 0.687 | |||
| Arch index | Taped foot | 0.025 ± 0.069 | 0.021 ± 0.063 | 1.00 | |
| Untaped foot | 0.008 ± 0.065 | 0.007 ± 0.052 | 0.911 | ||
| p | 0.330 | 0.513 | |||
| Men | Difference in arch height (mm) | Taped foot | 0 ± 1.18 | −0.27 ± 1.19 | 0.359 |
| Untaped foot | −1.09 ± 2.02 | −0.64 ± 1.12 | 0.290 | ||
| p | 0.122 | 0.257 | |||
| Arch index | Taped foot | −0.005 ± 0.036 | 0.018 ± 0.064 | 0.109 | |
| Untaped foot | 0.002 ± 0.05 | 0.005 ± 0.052 | 0.623 | ||
| p | 0.759 | 0.444 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, T.-C.; Cheng, P.-C.; Chung, Y.-H.; Chang, C.-W.; Chen, Y.-N.; Chang, C.-J. Initial Effects of Dynamic Tape on Foot Arch Height Under Cyclic Loading: A Pilot Study Among University Students. Sports 2025, 13, 138. https://doi.org/10.3390/sports13050138
Chang T-C, Cheng P-C, Chung Y-H, Chang C-W, Chen Y-N, Chang C-J. Initial Effects of Dynamic Tape on Foot Arch Height Under Cyclic Loading: A Pilot Study Among University Students. Sports. 2025; 13(5):138. https://doi.org/10.3390/sports13050138
Chicago/Turabian StyleChang, Ting-Chen, Po-Cheng Cheng, Yu-Hsuan Chung, Chih-Wei Chang, Yen-Nien Chen, and Chia-Jung Chang. 2025. "Initial Effects of Dynamic Tape on Foot Arch Height Under Cyclic Loading: A Pilot Study Among University Students" Sports 13, no. 5: 138. https://doi.org/10.3390/sports13050138
APA StyleChang, T.-C., Cheng, P.-C., Chung, Y.-H., Chang, C.-W., Chen, Y.-N., & Chang, C.-J. (2025). Initial Effects of Dynamic Tape on Foot Arch Height Under Cyclic Loading: A Pilot Study Among University Students. Sports, 13(5), 138. https://doi.org/10.3390/sports13050138