Resistance Training Causes the Stretch-Induced Force Deficit—A Randomized Cross-Over Study


 ,
,  and
and
Abstract
1. Introduction
2. Methods
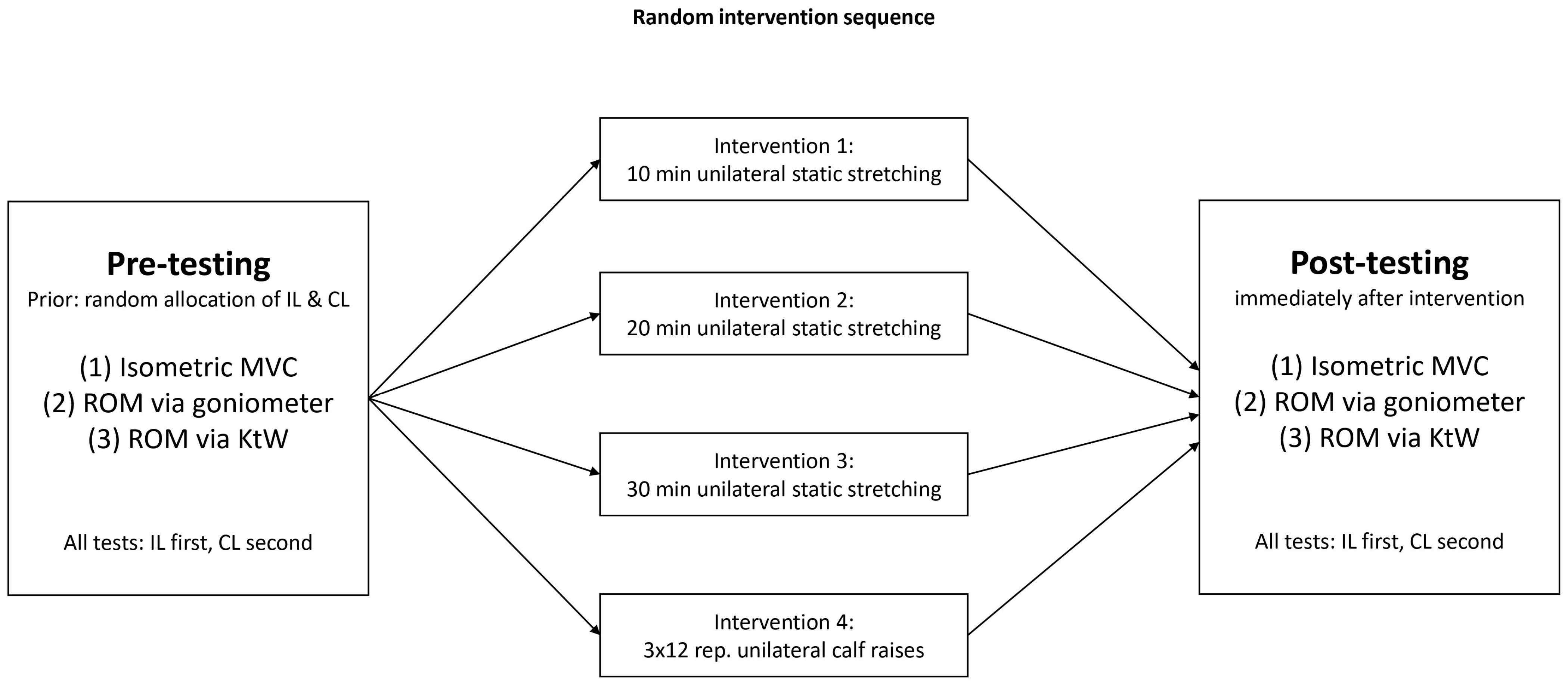
2.1. Experimental Design
2.2. Participants
Testing Procedure
2.3. Maximal Voluntary Isometric Contraction (MVIC) Strength
2.4. Dorsiflexion (DF) ROM with Extended Knee Joint
2.5. Dorsiflexion ROM Measurement with Flexed Knee Joint Using the Knee to Wall Test (KtW)
Intervention
3. Data Analysis
4. Results
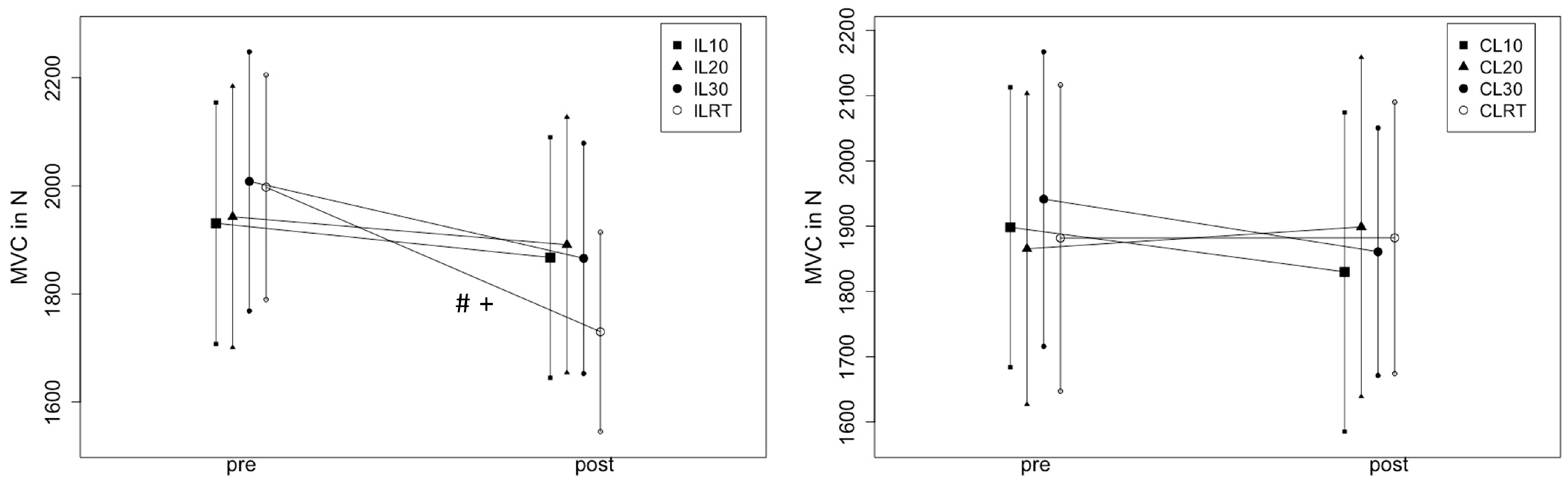
4.1. Effects of Stretching Intervention and Strength Training on MVC
4.1.1. 2 × 2 ANOVA (Leg × TIME)
4.1.2. 2 × 2 ANOVA (Condition × Time)
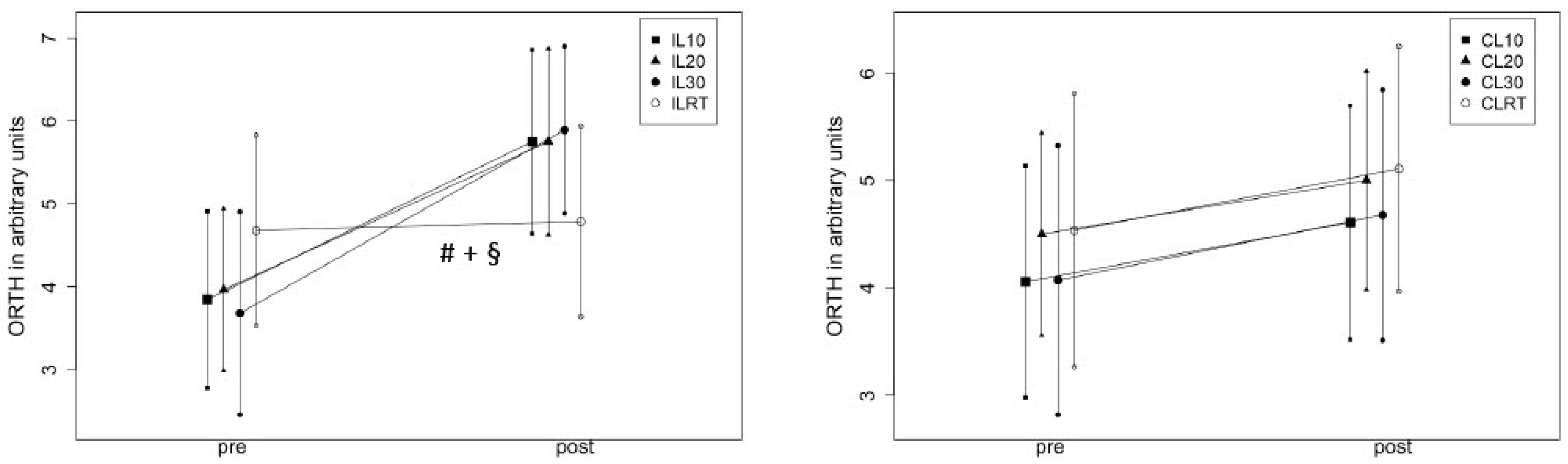
4.2. Effects on ROM
4.2.1. 2 ×2 ANOVA (Leg × Time)
4.2.2. 2 ×2 ANOVA (Condition × Time)
4.2.3. 2 × 2 ANOVA (Leg × Time)
4.2.4. 2 × 2 ANOVA (Condition × Time)
5. Discussion
Stretch-Induced Force Deficit
6. Range of Motion
7. Limitations
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Behm, D.G.; Alizadeh, S.; Daneshjoo, A.; Anvar, S.H.; Graham, A.; Zahiri, A.; Goudini, R.; Edwards, C.; Culleton, R.; Scharf, C.; et al. Acute Effects of Various Stretching Techniques on Range of Motion: A Systematic Review with Meta-Analysis. Sports Med. Open. 2023, 9, 107. [Google Scholar] [CrossRef]
- Cai, P.; Liu, L.; Li, H. Dynamic and static stretching on hamstring flexibility and stiffness: A systematic review and meta-analysis. Heliyon 2023, 9, e18795. [Google Scholar] [CrossRef]
- Kay, A.D.; Blazevich, A.J. Effect of acute static stretch on maximal muscle performance: A systematic review. Med. Sci. Sports Exerc. 2012, 44, 154–164. [Google Scholar] [CrossRef]
- Simic, L.; Sarabon, N.; Markovic, G. Does pre-exercise static stretching inhibit maximal muscular performance? A meta-analytical review. Scand J. Med. Sci. Sports 2013, 23, 131–148. [Google Scholar] [CrossRef]
- Behm, D.G.; Blazevich, A.J.; Kay, A.D.; McHugh, M. Acute effects of muscle stretching on physical performance, range of motion, and injury incidence in healthy active individuals: A systematic review. Appl. Physiol. Nutr. Metab. 2016, 41, 1–11. [Google Scholar] [CrossRef]
- Behm, D.G.; Chaouachi, A. A review of the acute effects of static and dynamic stretching on performance. Eur. J. Appl. Physiol. 2011, 111, 2633–2651. [Google Scholar] [CrossRef]
- Kokkonen, J.; Nelson, A.G.; Cornwell, A. Acute Muscle Stretching Inhibits Maximal Strength Performance. Res. Q. Exerc. Sport 1998, 69, 411–415. [Google Scholar] [CrossRef]
- Leone, D.C.P.G.; Pezarat, P.; Valamatos, M.J.; Fernandes, O.; Freitas, S.; Moraes, A.C. Upper body force production after a low-volume static and dynamic stretching. Eur. J. Sport Sci. 2014, 14, 69–75. [Google Scholar] [CrossRef]
- Siatras, T.A.; Mittas, V.P.; Mameletzi, D.N.; Vamvakoudis, E.A. The Duration of the Inhibitory Effects with Static Stretching on Quadriceps Peak Torque Production. J. Strength Cond. Res. 2008, 22, 40–46. [Google Scholar] [CrossRef]
- Marchetti, P.H.; Miyatake, M.M.S.; Magalhaes, R.A.; Gomes, W.A.; Da Silva, J.J.; Brigatto, F.A.; Zanini, T.C.C.; Behm, D.G. Different volumes and intensities of static stretching affect the range of motion and muscle force output in well-trained subjects. Sports Biomech. 2022, 21, 155–164. [Google Scholar] [CrossRef]
- Bacurau, R.F.P.; Monteiro, G.A.; Ugrinowitsch, C.; Tricoli, V.; Cabral, L.F.; Aoki, M.S. Acute Effect of a Ballistic and a Static Stretching Exercise Bout on Flexibility and Maximal Strength. J. Strength Cond. Res. 2009, 23, 304–308. [Google Scholar] [CrossRef]
- Warneke, K.; Wohlann, T.; Lohmann, L.H.; Wirth, K.; Schiemann, S. Acute effects of long-lasting stretching and strength training on maximal strength and flexibility in the calf muscle. Ger. J. Exerc. Sport Res. 2022, 53, 148–154. [Google Scholar] [CrossRef]
- Behm, D.G.; Kay, A.D.; Trajano, G.S.; Blazevich, A.J. Mechanisms underlying performance impairments following prolonged static stretching without a comprehensive warm-up. Eur. J. Appl. Physiol. 2021, 121, 67–94. [Google Scholar] [CrossRef]
- Farina, D.; Fosci, M.; Merletti, R. Motor unit recruitment strategies investigated by surface EMG variables. J. Appl. Physiol. 2002, 92, 235–247. [Google Scholar] [CrossRef]
- Trajano, G.S.; Nosaka, K.; Blazevich, A.J. Neurophysiological Mechanisms Underpinning Stretch-Induced Force Loss. Sports Med. 2017, 47, 1531–1541. [Google Scholar] [CrossRef]
- Kay, A.D.; Blazevich, A.J. Isometric contractions reduce plantar flexor moment, Achilles tendon stiffness, and neuromuscular activity but remove the subsequent effects of stretch. J. Appl. Physiol. 2009, 107, 1181–1189. [Google Scholar] [CrossRef]
- Trajano, G.S.; Taylor, J.L.; Orssatto, L.B.R.; McNulty, C.R.; Blazevich, A.J. Passive muscle stretching reduces estimates of persistent inward current strength in soleus motor units. J. Exp. Biol. 2020, 223, jeb229922. [Google Scholar] [CrossRef]
- Binder, M.D.; Powers, R.K.; Heckman, C.J. Nonlinear Input-Output Functions of Motoneurons. Physiology 2020, 35, 31–39. [Google Scholar] [CrossRef]
- Takeuchi, K.; Nakamura, M.; Fukaya, T.; Konrad, A.; Mizuno, T. Acute and Long-Term Effects of Static Stretching on Muscle-Tendon Unit Stiffness: A Systematic Review and Meta-Analysis. J. Sports Sci. Med. 2023, 22, 465–475. [Google Scholar] [CrossRef]
- Konrad, A.; Nakamura, M.; Paternoster, F.K.; Tilp, M.; Behm, D.G. A comparison of a single bout of stretching or foam rolling on range of motion in healthy adults. Eur. J. Appl. Physiol. 2022, 122, 1545–1557. [Google Scholar] [CrossRef]
- Kubo, K.; Kawakami, Y.; Fukunaga, T. Influence of elastic properties of tendon structures on jump performance in humans. J. Appl. Physiol. 1999, 87, 2090–2096. [Google Scholar] [CrossRef]
- Chaabene, H.; Behm, D.G.; Negra, Y.; Granacher, U. Acute Effects of Static Stretching on Muscle Strength and Power: An Attempt to Clarify Previous Caveats. Front. Physiol. 2019, 10, 1468. [Google Scholar] [CrossRef]
- Pinninger, G.J.; Steele, J.R.; Groeller, H. Does fatigue induced by repeated dynamic efforts affect hamstring muscle function? Med. Sci. Sports Exerc. 2000, 32, 647–653. [Google Scholar] [CrossRef]
- Neyroud, D.; Maffiuletti, N.A.; Kayser, B.; Place, N. Mechanisms of Fatigue and Task Failure Induced by Sustained Submaximal Contractions. Med. Sci. Sports Exerc. 2012, 44, 1243–1251. [Google Scholar] [CrossRef]
- Bigland-Ritchie, B.; Furbush, F.; Woods, J.J. Fatigue of intermittent submaximal voluntary contractions: Central and peripheral factors. J. Appl. Physiol. 1986, 61, 421–429. [Google Scholar] [CrossRef]
- Silva, B.; Clemente, F.M.; Martins, F.M. Associations between Functional Movement Screen Scores and Performance Variables in Surf Athletes. J. Sports Med. Phys. Fit. 2018, 58, 583–590. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for Behavioral Sciences, 2nd ed.; Erlbaum: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef]
- Alizadeh, S.; Daneshjoo, A.; Zahiri, A.; Anvar, S.H.; Goudini, R.; Hicks, J.P.; Konrad, A.; Behm, D.G. Resistance Training Induces Improvements in Range of Motion: A Systematic Review and Meta-Analysis. Sports Med. 2023, 53, 707–722. [Google Scholar] [CrossRef]
- Behm, D.G.; St-Pierre, D.M.M. Effects of fatigue duration and muscle type on voluntary and evoked contractile properties. J. Appl. Physiol. 1997, 82, 1654–1661. [Google Scholar] [CrossRef]
- Smith, L.L.; Brunetz, M.H.; Chenier, T.C.; McCammon, M.R.; Houmard, J.A.; Franklin, M.E.; Israel, R.G. The effects of static and ballistic stretching on delayed onset muscle soreness and creatine kinase. Res. Q. Exerc. Sport 1993, 64, 103–107. [Google Scholar] [CrossRef]
- Wohlann, T.; Warneke, K.; Hillebrecht, M.; Petersmann, A.; Ferrauti, A.; Schiemann, S. Effects of daily static stretch training over 6 weeks on maximal strength, muscle thickness, contraction properties, and flexibility. Front. Sports Act. Living 2023, 5, 1139065. [Google Scholar] [CrossRef]
- Hotta, K.; Behnke, B.J.; Arjmandi, B.; Ghosh, P.; Chen, B.; Brooks, R.; Maraj, J.J.; Elam, M.L.; Maher, P.; Kurien, D.; et al. Daily muscle stretching enhances blood flow, endothelial function, capillarity, vascular volume and connectivity in aged skeletal muscle. J. Physiol. 2018, 596, 1903–1917. [Google Scholar] [CrossRef]
- Mahoney, S.J.; Dicks, N.D.; Lyman, K.J.; Christensen, B.K.; Hackney, K.J. Acute Cardiovascular, Metabolic, and Muscular Responses to Blood Flow Restricted Rowing Exercise. Aerosp. Med. Hum. Perform. 2019, 90, 440–446. [Google Scholar] [CrossRef]
- Santiago-Pescador, S.; Fajardo-Blanco, D.; López-Ortiz, S.; Peñín-Grandes, S.; Méndez-Sánchez, R.; Lucia, A.; Martín-Hernández, J.; Santos-Lozano, A. Acute effects of electrostimulation and blood flow restriction on muscle thickness and fatigue in the lower body. Eur. J. Sport Sci. 2023, 23, 1591–1599. [Google Scholar] [CrossRef]
- Chua, M.T.; Sim, A.; Burns, S.F. Acute and Chronic Effects of Blood Flow Restricted High-Intensity Interval Training: A Systematic Review. Sports Med. Open 2022, 8, 122. [Google Scholar] [CrossRef]
- Warneke, K.; Plöschberger, G.; Lohmann, L.H.; Lichtenstein, E.; Jochum, D.; Siegel, S.D.; Zech, A.; Behm, D.G. Foam rolling and stretching do not provide superior acute flexibility and stiffness improvements compared to any other warm-up intervention: A systematic review with meta-analysis. J. Sport Health Sci. 2024, accepted. [Google Scholar] [CrossRef]
- Roberts, H.M.; Law, R.-J.; Thom, J.M. The time course and mechanisms of change in biomarkers of joint metabolism in response to acute exercise and chronic training in physiologic and pathological conditions. Eur. J. Appl. Physiol. 2019, 119, 2401–2420. [Google Scholar] [CrossRef]
- Behm, D.G.; Alizadeh, S.; Drury, B.; Granacher, U.; Moran, J. Non-local acute stretching effects on strength performance in healthy young adults. Eur. J. Appl. Physiol. 2021, 121, 1517–1529. [Google Scholar] [CrossRef]
- Andrade, R.J.; Freitas, S.R.; Hug, F.; Le Sant, G.; Lacourpaille, L.; Gross, R.; McNair, P.; Nordez, A. The potential role of sciatic nerve stiffness in the limitation of maximal ankle range of motion. Sci. Rep. 2018, 8, 14532. [Google Scholar] [CrossRef]
- Lim, W.; Park, H. No significant correlation between the intensity of static stretching and subject’s perception of pain. J. Phys. Ther. Sci. 2017, 10, 1856–1859. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Pre-Test (M ± SD) In ° | Post-Test (M ± SD) In ° |
|---|---|---|
| MVC10IL | 1930.71 ± 426.32 | 1867.29 ± 424.77 |
| MVC10CL | 1898.36 ± 409.32 | 1829.93 ± 466.69 |
| MVC20IL | 1942.71 ± 461.10 | 1890.93 ± 451.14 |
| MVC20CL | 1865.36 ± 454.64 | 1898.86 ± 496.05 |
| MVC30IL | 2008.14 ± 457.48 | 1865.79 ± 406.70 |
| MVC30CL | 1941.50 ± 430.77 | 1860.86 ± 362.16 |
| MVCSTIL | 1997.36 ± 396.63 | 1729.86 ± 351.92 |
| MVCSTCL | 1881.86 ± 447.85 | 1882.14 ± 397.00 |
| ORTH10IL | 3.84 ± 2.04 | 5.75 ± 2.12 |
| ORTH10CL | 4.06 ± 2.06 | 4.61 ± 2.08 |
| ORTH20IL | 3.96 ± 1.87 | 5.75 ± 2.15 |
| ORTH20CL | 4.50 ± 1.80 | 5.00 ± 1.94 |
| ORTH30IL | 3.68 ± 2.34 | 5.89 ± 1.92 |
| ORTH30CL | 4.07 ± 2.39 | 4.68 ± 2.22 |
| ORTHFIL | 4.68 ± 2.20 | 4.79 ± 2.20 |
| ORTHFCL | 4.50 ± 2.43 | 5.00 ± 2.18 |
| KTW10IL | 13.71 ± 2.79 | 14.25 ± 2.96 |
| KTW10CL | 13.86 ± 2.83 | 14.14 ± 2.81 |
| KTW20IL | 14.07 ± 2.79 | 14.39 ± 3.27 |
| KTW20CL | 13.86 ± 3.26 | 14.21 ± 3.18 |
| KTW30IL | 14.39 ± 2.92 | 15.18 ± 3.21 |
| KTW30CL | 14.25 ± 2.80 | 14.50 ± 3.11 |
| KTWFIL | 14.11 ± 3.09 | 14.57 ± 3.42 |
| KTWFCL | 14.04 ± 3.05 | 15.32 ± 2.93 |
| MVC 3-Way ANOVA | ||
|---|---|---|
| Effect | Significance (p-Value) | Effect Size (Partial eta Squared) |
| Leg × Time | <0.001 * | 0.62 |
| Leg × Condition | 0.19 | 0.34 |
| Time × Condition | 0.21 | 0.33 |
| Leg × Time × Condition | 0.02 * | 0.57 |
| MVC 10 min stretching 2-way ANOVA | ||
| Time | 0.07 | 0.24 |
| Leg × Time | 0.91 | 0.001 |
| MVC 20 min stretching 2-way ANOVA | ||
| Time | 0.83 | 0.04 |
| Leg × Time | 0.10 | 0.20 |
| MVC 30 min stretching 2-way ANOVA | ||
| Time | 0.003 * | 0.52 |
| Leg × Time | 0.13 | 0.17 |
| MVC RT 2-way ANOVA | ||
| Time | 0.008 * | 0.43 |
| Leg × Time | <0.001 * | 0.62 |
| ROM (ORTH) 3-way ANOVA | ||
| Effect | Significance (p-value) | Effect size (partial eta squared) |
| Leg × Time | 0.001 * | 0.56 |
| Leg × Condition | 0.44 | 0.21 |
| Time × Condition | 0.01 * | 0.62 |
| Leg × Time × Condition | <0.001 * | 0.76 |
| ROM (ORTH) 10 min stretching 2-way ANOVA | ||
| Time | <0.001 * | 0.62 |
| Leg × Time | 0.008 * | 0.43 |
| MVC 20 min stretching 2-way ANOVA | ||
| Time | <0.001 * | 0.78 |
| Leg × Time | 0.002 * | 0.55 |
| ROM (ORTH)stretching 2-way ANOVA | ||
| Time | <0.001 * | 0.67 |
| Leg × Time | <0.001 * | 0.62 |
| ROM (ORTH) RT 2-way ANOVA | ||
| Time | 0.06 | 0.26 |
| Leg × Time | 0.06 | 0.25 |
| ROM (KtW) 3-way ANOVA | ||
| Effect | Significance (p-value) | Effect size (partial eta squared) |
| Leg × Time | 0.23 | 0.11 |
| Leg × Condition | 0.30 | 0.27 |
| Time × Condition | 0.75 | 0.10 |
| Leg × Time × Condition | 0.82 | 0.078 |
| ROM (KtW) 10 min stretching 2-way ANOVA | ||
| Time | 0.02 * | 0.35 |
| Leg × Time | 0.33 | 0.07 |
| ROM (KtW) 20 min stretching 2-way ANOVA | ||
| Time | 0.15 | 0.06 |
| Leg × Time | 0.92 | 0.15 |
| ROM (KtW)30 min stretching 2-way ANOVA | ||
| Time | 0.02 * | 0.37 |
| Leg × Time | 0.20 | 0.12 |
| ROM (KtW) RT 2-way ANOVA | ||
| Time | <0.001 * | 0.62 |
| Leg × Time | 0.59 | 0.02 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Warneke, K.; Turau, K.; Lohmann, L.H.; Hillebrecht, M.; Behm, D.G.; Konrad, A.; Schmidt, T. Resistance Training Causes the Stretch-Induced Force Deficit—A Randomized Cross-Over Study. Sports 2024, 12, 145. https://doi.org/10.3390/sports12060145
Warneke K, Turau K, Lohmann LH, Hillebrecht M, Behm DG, Konrad A, Schmidt T. Resistance Training Causes the Stretch-Induced Force Deficit—A Randomized Cross-Over Study. Sports. 2024; 12(6):145. https://doi.org/10.3390/sports12060145
Chicago/Turabian StyleWarneke, Konstantin, Katharina Turau, Lars Hubertus Lohmann, Martin Hillebrecht, David G. Behm, Andreas Konrad, and Tobias Schmidt. 2024. "Resistance Training Causes the Stretch-Induced Force Deficit—A Randomized Cross-Over Study" Sports 12, no. 6: 145. https://doi.org/10.3390/sports12060145
APA StyleWarneke, K., Turau, K., Lohmann, L. H., Hillebrecht, M., Behm, D. G., Konrad, A., & Schmidt, T. (2024). Resistance Training Causes the Stretch-Induced Force Deficit—A Randomized Cross-Over Study. Sports, 12(6), 145. https://doi.org/10.3390/sports12060145