
Comparison of the Electromyography Activity during Exercises with Stable and Unstable Surfaces: A Systematic Review and Meta-Analysis

 , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
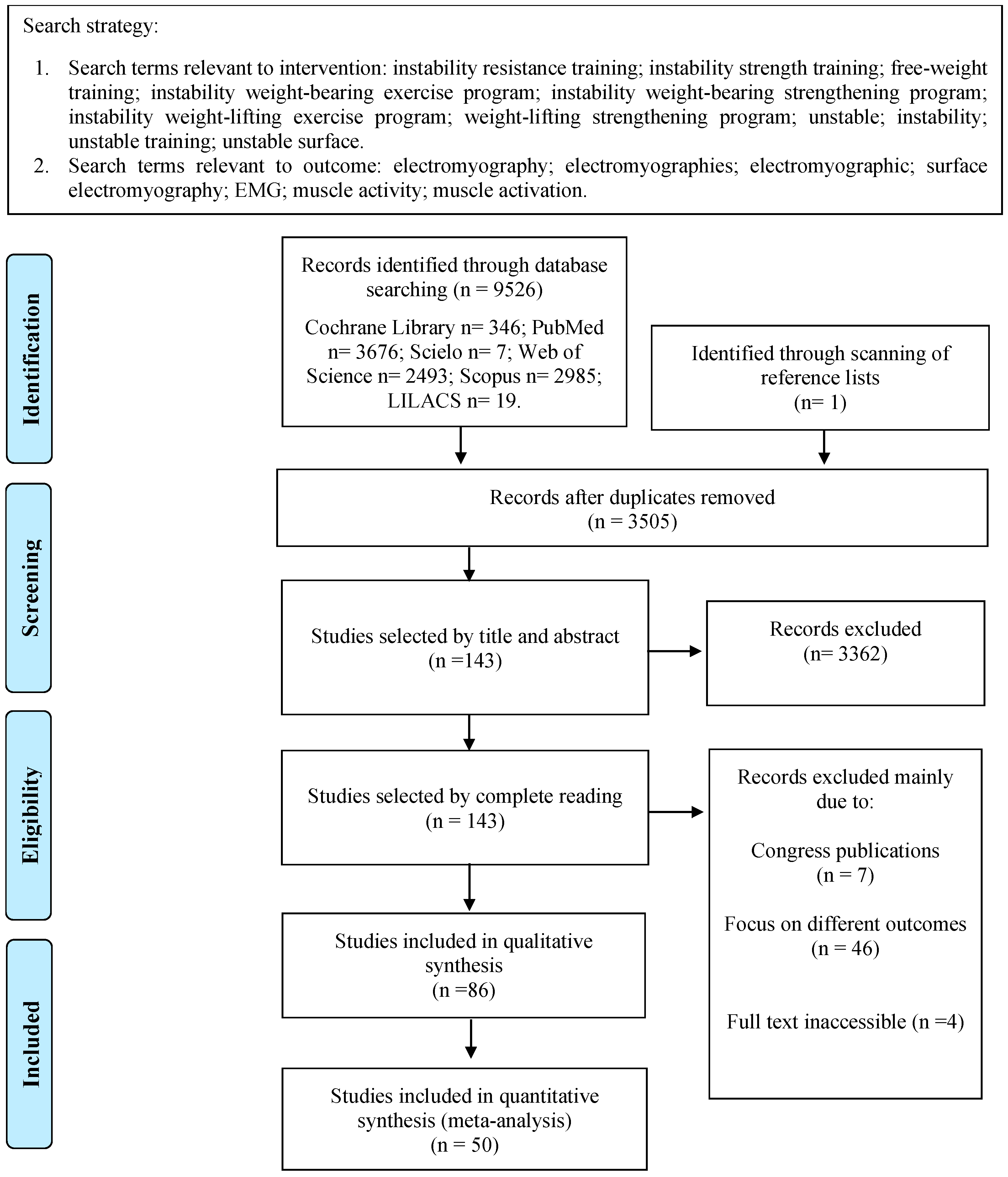
2.1. Data Sources and Searches
2.2. Study Selection
2.3. Data Extraction
2.4. Methodological Quality Assessment
2.5. Data Analysis
3. Results
3.1. Study Characteristics
3.2. Methodological Quality Assessment
3.3. Qualitative Analysis
3.4. Quantitative Analysis
3.4.1. Core
3.4.2. Upper Limbs
3.4.3. Lower Limbs
4. Discussion
4.1. Core
4.2. Lower Limbs
4.3. Upper Limbs
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Behm, D.G.; Anderson, K.G. The role of instability with resistance training. J. Strength Cond. Res. 2006, 20, 716–722. [Google Scholar] [PubMed]
- Sousa, D.S.F.; de Farias, W.M.; de Amorim Batista, G.; de Oliveira, V.M.A.; Pirauá, A.L.T.; Beltrão, N.B.; Pitangui, A.C.R.; de Araújo, R.C. Activation of Upper Limb Muscles in Subjects with Scapular Dyskinesis during Bench-Press and Dumbbell Fly on Stable and Unstable Surfaces. J. Back Musculoskelet. Rehabil. 2022, 35, 1289–1297. [Google Scholar] [CrossRef] [PubMed]
- Palma, F.; Perramont, N.; Rojas, V.; Bertolotto, B.; Tuesta, M. Electromyographic Amplitude and Coactivation of the Core Muscles during Different Unstable Push-up Exercises. Med. Sport 2021, 74, 209–222. [Google Scholar] [CrossRef]
- Bouillon, L.E.; Hofener, M.; O’Donnel, A.; Milligan, A.; Obrock, C. Comparison of Muscle Activity Using Unstable Devices during a Forward Lunge. J. Sport. Rehabil. 2019, 29, 394–399. [Google Scholar] [CrossRef] [PubMed]
- Buscà, B.; Aguilera-Castells, J.; Arboix-Alió, J.; Miró, A.; Fort-Vanmeerhaeghe, A.; Peña, J. Influence of the Amount of Instability on the Leg Muscle Activity during a Loaded Free Barbell Half-Squat. Int. J. Environ. Res. Public Health 2020, 17, 8046. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Lee, J.-H.; Heo, J.; Chang, E. Differences of Thigh Muscle Activation during Various Squat Exercise on Stable and Unstable Surfaces. Exerc. Sci. 2021, 30, 387–395. [Google Scholar] [CrossRef]
- Pirauá, A.L.T.; Cavalcante, B.R.; Oliveira, V.M.A.; Beltrão, N.B.; Amorim Batista, G.; Pitangui, A.C.R.; Behm, D.; Araújo, R.C. Effect of 24-week Strength Training on Unstable Surfaces on Mobility, Balance, and Concern about Falling in Older Adults. Scand. J. Med. Sci. Sports 2019, 29, 1805–1812. [Google Scholar] [CrossRef]
- Cavalcante, B.R.; de Souza, M.F.; Falck, R.S.; Liu-Ambrose, T.; Behm, D.G.; Pitangui, A.C.R.; de Araújo, R.C. Effects of Resistance Exercise with Instability on Cognitive Function (REI Study): A Proof-Of-Concept Randomized Controlled Trial in Older Adults with Cognitive Complaints. J. Alzheimer’s Dis. 2020, 77, 227–239. [Google Scholar] [CrossRef]
- Nascimento, V.Y.S.; Torres, R.J.B.; Beltrão, N.B.; dos Santos, P.S.; Pirauá, A.L.T.; de Oliveira, V.M.A.; Pitangui, A.C.R.; de Araújo, R.C. Shoulder Muscle Activation Levels During Exercises with Axial and Rotational Load on Stable and Unstable Surfaces. J. Appl. Biomech. 2017, 33, 118–123. [Google Scholar] [CrossRef] [PubMed]
- Melo, B.; Pirauá, A.; Beltrão, N.; Pitangui, A.C.; Araújo, R. A Utilização de Superfície Instável Aumenta a Atividade Eletromiográfica Dos Músculos Da Cintura Escapular No Exercício Crucifixo. Rev. Bras. Atividade Física Saúde 2014, 19, 342–350. [Google Scholar] [CrossRef]
- Behm, D.G.; Muehlbauer, T.; Kibele, A.; Granacher, U. Effects of Strength Training Using Unstable Surfaces on Strength, Power and Balance Performance Across the Lifespan: A Systematic Review and Meta-Analysis. Sports Med. 2015, 45, 1645–1669. [Google Scholar] [CrossRef] [PubMed]
- Behm, D.; Colado, J.C. The Effectiveness of Resistance Training Using Unstable Surfaces and Devices for Rehabilitation. Int. J. Sports Phys. Ther. 2012, 7, 226–241. [Google Scholar] [PubMed]
- Behm, D.G.; Colado Sanchez, J.C. Instability Resistance Training across the Exercise Continuum. Sports Health 2013, 5, 500–503. [Google Scholar] [CrossRef] [PubMed]
- Luk, J.T.C.; Kwok, F.K.C.; Ho, I.M.K.; Wong, D.P. Acute Responses of Core Muscle Activity during Bridge Exercises on the Floor vs. the Suspension System. Int. J. Environ. Res. Public Health 2021, 18, 5908. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.J.; Kwon, O.Y.; Yi, C.H.; Jeon, H.S.; Oh, J.S.; Cynn, H.S.; Weon, J.H. Comparison of Abdominal Muscle Activity during a Single-Legged Hold in the Hook-Lying Position on the Floor and on a Round Foam Roll. J. Athl. Train. 2011, 46, 403–408. [Google Scholar] [CrossRef] [PubMed]
- De Araújo, R.C.; De Andrade, R.; Tucci, H.T.; Martins, J.; De Oliveira, A.S. Shoulder Muscular Activity during Isometric Three-Point Kneeling Exercise on Stable and Unstable Surfaces. J. Appl. Biomech. 2011, 27, 192–196. [Google Scholar] [CrossRef] [PubMed]
- Snarr, R.L.; Esco, M.R. Electromyographic Comparison of Traditional and Suspension Push-Ups. J. Hum. Kinet. 2013, 39, 75–83. [Google Scholar] [CrossRef]
- Li, Y.; Cao, C.; Chen, X. Similar Electromyographic Activities of Lower Limbs between Squatting on a Reebok Core Board and Ground. J. Strength Cond. Res. 2013, 27, 1349–1353. [Google Scholar] [CrossRef] [PubMed]
- Youdas, J.W.; Hubble, J.W.; Johnson, P.G.; McCarthy, M.M.; Saenz, M.M.; Hollman, J.H. Scapular Muscle Balance and Spinal Stabilizer Recruitment during an Inverted Row. Physiother. Theory Pract. 2020, 36, 432–443. [Google Scholar] [CrossRef]
- Uribe, B.P.; Coburn, J.W.; Brown, L.E.; Judelson, D.A.; Khamoui, A.V.; Nguyen, D. Muscle Activation When Performing the Chest Press and Shoulder Press on a Stable Bench vs. a Swiss Ball. J. Strength Cond. Res. 2010, 24, 1028–1033. [Google Scholar] [CrossRef]
- De Araújo, R.C.; Andrade da Silva, H.; Pereira dos Passos, M.H.; Alves de Oliveira, V.M.; Rodarti Pitangui, A.C. Use of Unstable Exercises in Periscapular Muscle Activity: A Systematic Review and Meta-Analysis of Electromyographic Studies. J. Bodyw. Mov. Ther. 2021, 26, 318–328. [Google Scholar] [CrossRef] [PubMed]
- Mendez-Rebolledo, G.; Orozco-Chavez, I.; Morales-Verdugo, J.; Ramirez-Campillo, R.; Cools, A.M.J. Electromyographic Analysis of the Serratus Anterior and Upper Trapezius in Closed Kinetic Chain Exercises Performed on Different Unstable Support Surfaces: A Systematic Review and Meta-Analysis. PeerJ 2022, 10, e13589. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Syed-Abdul, M.M.; Soni, D.S.; Miller, W.M.; Johnson, R.J.; Barnes, J.T.; Pujol, T.J.; Wagganer, J.D. Traditional vs. Suspended Pushup Muscle Activation in Athletes and Sedentary Females. J. Strength Cond. Res. 2018, 32, 1816–1820. [Google Scholar] [CrossRef] [PubMed]
- Hwangbo, G.; Kim, M.K. The Effects of Ankle Joint Position in Various Lower Limb Ground States on the Activation of the Shoulder and Trunk Muscles during Push-up Exercises. J. Phys. Ther. Sci. 2012, 24, 411–414. [Google Scholar] [CrossRef]
- Calatayud, J.; Borreani, S.; Colado, J.C.; Martin, F.; Rogers, M.E. Muscle Activity Levels in Upper-Body Push Exercises with Different Loads and Stability Conditions. Physician Sportsmed. 2014, 42, 106–119. [Google Scholar] [CrossRef] [PubMed]
- Borreani, S.; Calatayud, J.; Colado, J.C.; Tella, V.; Moya-Nájera, D.; Martin, F.; Rogers, M.E. Shoulder Muscle Activation during Stable and Suspended Push-Ups at Different Heights in Healthy Subjects. Phys. Ther. Sport 2015, 16, 248–254. [Google Scholar] [CrossRef] [PubMed]
- Calatayud, J.; Borreani, S.; Colado, J.C.; Martín, F.F.; Rogers, M.E.; Behm, D.G.; Andersen, L.L. Muscle Activation during Push-Ups with Different Suspension Training Systems. J. Sports Sci. Med. 2014, 13, 502–510. [Google Scholar] [PubMed]
- Borreani, S.; Calatayud, J.; Colado, J.C.; Moya-Nájera, D.; Triplett, N.T.; Martin, F. Muscle Activation during Push-Ups Performed under Stable and Unstable Conditions. J. Exerc. Sci. Fit. 2015, 13, 94–98. [Google Scholar] [CrossRef]
- Kim, M.-K.; Jung, J.-M.; Lee, S.-Y.; Hwangbo, G.; Lee, Y.-S. Effects of Various Lower Limb Ground States on Activation of the Shoulder and Trunk Muscles during Push-up Exercises. J. Phys. Ther. Sci. 2012, 24, 161–164. [Google Scholar] [CrossRef]
- Youdas, J.W.; Hartman, J.P.; Murphy, B.A.; Rundle, A.M.; Ugorowski, J.M.; Hollman, J.H. Magnitudes of Muscle Activation of Spine Stabilizers, Gluteals, and Hamstrings during Supine Bridge to Neutral Position. Physiother. Theory Pract. 2015, 31, 418–427. [Google Scholar] [CrossRef] [PubMed]
- Sundstrup, E.; Jakobsen, M.D.; Andersen, C.H.; Jay, K.; Andersen, L.L. Swiss Ball Abdominal Crunch with Added Elastic Resistance Is an Effective Alternative to Training Machines. Int. J. Sports Phys. Ther. 2012, 7, 372–380. [Google Scholar] [PubMed]
- Aguilera-Castells, J.; Buscà, B.; Morales, J.; Solana-Tramunt, M.; Fort-Vanmeerhaeghe, A.; Rey-Abella, F.; Bantulà, J.; Peña, J. Muscle Activity of Bulgarian Squat. Effects of Additional Vibration, Suspension and Unstable Surface. PLoS ONE 2019, 14, e0221710. [Google Scholar] [CrossRef] [PubMed]
- Siegfried, N.; Muller, M.; Deeks, J.; Volmink, J.; Egger, M.; Low, N.; Walker, S.; Williamson, P. HIV and Male Circumcision—A Systematic Review with Assessment of the Quality of Studies. Lancet Infect. Dis. 2005, 5, 165–173. [Google Scholar] [CrossRef] [PubMed]
- Kinsella, R.; Pizzari, T. Electromyographic Activity of the Shoulder Muscles during Rehabilitation Exercises in Subjects with and without Subacromial Pain Syndrome: A Systematic Review. Shoulder Elbow 2017, 9, 112–126. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Hoboken, NJ, USA, 2019; ISBN 1119536618. [Google Scholar]
- Oliva-Lozano, J.M.; Muyor, J.M. Core Muscle Activity during Physical Fitness Exercises: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 4306. [Google Scholar] [CrossRef] [PubMed]
- Marshall, P.; Murphy, B. Changes in Muscle Activity and Perceived Exertion during Exercises Performed on a Swiss Ball. Appl. Physiol. Nutr. Metab. 2006, 31, 376–383. [Google Scholar] [CrossRef]
- Aranda, L.C.; Mancini, M.; Werneck, F.Z.; Novaes, J.D.S.; Da Silva-Grigoletto, M.E.; Vianna, J.M. Electromyographic Activity and 15RM Load during Resistance Exercises on Stable and Unstable Surfaces. J. Exerc. Physiol. Online 2016, 19, 114–123. [Google Scholar]
- Behm, D.G.; Leonard, A.M.; Young, W.B.; Bonsey, W.A.C.; MacKinnon, S.N. Trunk Muscle Electromyographic Activity with Unstable and Unilateral Exercises. J. Strength Cond. Res. 2005, 19, 193–201. [Google Scholar] [CrossRef]
- Snarr, R.L.; Esco, M.R. Electromyographical Comparison of Plank Variations Performed with and without Instability Devices. J. Strength. Cond. Res. 2014, 28, 3298–3305. [Google Scholar] [CrossRef]
- Atkins, S.J.; Bentley, I.; Brooks, D.; Burrows, M.P.; Hurst, H.T.; Sinclair, J.K. Electromyographic Response of Global Abdominal Stabilizers in Response to Stable- and Unstable-Base Isometric Exercise. J. Strength Cond. Res. 2015, 29, 1609–1615. [Google Scholar] [CrossRef]
- Lee, S.; Park, J.; Lee, D. Effects of Bridge Exercise Performed on an Unstable Surface on Lumbar Stabilizing Muscles According to the Knee Angle. J. Phys. Ther. Sci. 2015, 27, 2633–2635. [Google Scholar] [CrossRef] [PubMed]
- Byrne, J.M.; Bishop, N.S.; Caines, A.M.; Crane, K.A.; Feaver, A.M.; Pearcey, G.E.P. Effect of Using a Suspension Training System on Muscle Activation during the Performance of a Front Plank Exercise. J. Strength Cond. Res. 2014, 28, 3049–3055. [Google Scholar] [CrossRef] [PubMed]
- Czaprowski, D.; Afeltowicz, A.; Gebicka, A.; Pawłowska, P.; Kedra, A.; Barrios, C.; Hadała, M. Abdominal Muscle EMG-Activity during Bridge Exercises on Stable and Unstable Surfaces. Phys. Ther. Sport 2014, 15, 162–168. [Google Scholar] [CrossRef]
- Biscarini, A.; Contemori, S.; Grolla, G. Activation of Scapular and Lumbopelvic Muscles During Core Exercises Executed on a Whole-Body Wobble Board. J. Sport Rehabil. 2019, 28, 623–634. [Google Scholar] [CrossRef]
- Imai, A.; Kaneoka, K.; Okubo, Y.; Shiina, I.; Tatsumura, M.; Izumi, S.; Shiraki, H. Trunk Muscle Activity during Lumbar Stabilization Exercises on Both a Stable and Unstable Surface. J. Orthop. Sports Phys. Ther. 2010, 40, 369–375. [Google Scholar] [CrossRef]
- Yoon, J.-O.; Kang, M.-H.; Kim, J.-S.; Oh, J.-S. Effect of Modified Bridge Exercise on Trunk Muscle Activity in Healthy Adults: A Cross Sectional Study. Braz. J. Phys. Ther. 2018, 22, 161–167. [Google Scholar] [CrossRef]
- Andrade, L.S.; Mochizuki, L.; Pires, F.O.; da Silva, R.A.S.; Mota, Y.L. Application of Pilates Principles Increases Paraspinal Muscle Activation. J. Bodyw. Mov. Ther. 2015, 19, 62–66. [Google Scholar] [CrossRef]
- Youdas, J.W.; Coleman, K.C.; Holstad, E.E.; Long, S.D.; Veldkamp, N.L.; Hollman, J.H. Magnitudes of Muscle Activation of Spine Stabilizers in Healthy Adults during Prone on Elbow Planking Exercises with and without a Fitness Ball. Physiother. Theory Pract. 2017, 34, 212–222. [Google Scholar] [CrossRef]
- Vilaça-Alves, J.; Guimarães, F.; Rosa, C.; Neves, E.B.; Saavedra, F.; Fernandes, A.O.; Reis, V.M. Electromyography Analysis of the Abdominal Crunch in Stable and Unstable Surface. Gazz. Medica Ital. Arch. Sci. Mediche 2016, 175, 189–194. [Google Scholar]
- Sternlicht, E.; Rugg, S.; Fujii, L.L.; Tomomitsu, K.F.; Seki, M.M. Electromyographic Comparison of a Stability Ball Crunch with a Traditional Crunch. J. Strength. Cond. Res. 2007, 21, 506. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Feldwieser, F.M.; Sheeran, L.; Meana-Esteban, A.; Sparkes, V. Electromyographic Analysis of Trunk-Muscle Activity during Stable, Unstable and Unilateral Bridging Exercises in Healthy Individuals. Eur. Spine J. 2012, 21, 171–186. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.-H.; Oh, J.-S. Effects of Performing an Abdominal Hollowing Exercise on Trunk Muscle Activity during Curl-up Exercise on an Unstable Surface. J. Phys. Ther. Sci. 2015, 27, 501–503. [Google Scholar] [CrossRef]
- Saeterbakken, A.H.; Andersen, V.; Jansson, J.; Kvellestad, A.C.; Fimland, M.S. Effects of BOSU Ball(s) During Sit-Ups with Body Weight and Added Resistance on Core Muscle Activation. J. Strength Cond. Res. 2014, 28, 3515–3522. [Google Scholar] [CrossRef]
- Lehman, G.J.; Gordon, T.; Langley, J.; Pemrose, P.; Tregaskis, S. Replacing a Swiss Ball for an Exercise Bench Causes Variable Changes in Trunk Muscle Activity during Upper Limb Strength Exercises. Dyn. Med. 2005, 4, 6. [Google Scholar] [CrossRef]
- Ha, S.; Oh, J.; Jeon, I.; Kwon, O. The Effects of Surface Condition on Abdominal Muscle Activity during Single-Legged Hold Exercise. J. Electromyogr. Kinesiol. 2015, 25, 28–33. [Google Scholar] [CrossRef]
- Lee, D.; Lee, Y.; Cho, H.-Y.; Lee, K.-B.; Hong, S.; Pyo, S.; Lee, G. Investigation of Trunk Muscle Activity for Modified Plank Exercise: A Preliminary Study. Isokinet. Exerc. Sci. 2017, 25, 209–213. [Google Scholar] [CrossRef]
- Kim, J.H.; Kim, Y.; Chung, Y. The Influence of an Unstable Surface on Trunk and Lower Extremity Muscle Activities during Variable Bridging Exercises. J. Phys. Ther. Sci. 2014, 26, 521–523. [Google Scholar] [CrossRef]
- Kim, C.-M.; Kong, Y.-S.; Hwang, Y.-T.; Park, J. The Effect of the Trunk and Gluteus Maximus Muscle Activities According to Support Surface and Hip Joint Rotation during Bridge Exercise. J. Phys. Ther. Sci. 2018, 30, 943–947. [Google Scholar] [CrossRef][Green Version]
- Hyong, I.H.; Kang, J.H. Activities of the Vastus Lateralis and Vastus Medialis Oblique Muscles during Squats on Different Surfaces. J. Phys. Ther. Sci. 2013, 25, 915–917. [Google Scholar] [CrossRef][Green Version]
- Park, J.-K.; Lee, D.-Y.; Kim, J.-S.; Hong, J.-H.; You, J.-H.; Park, I.-M. Effects of Visibility and Types of the Ground Surface on the Muscle Activities of the Vastus Medialis Oblique and Vastus Lateralis. J. Phys. Ther. Sci. 2015, 27, 2435–2437. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Souto Maior, B.; Simão, A.; Freitas De Salles, R.; Miranda, B.; Costa, H.; Brando, P. Neuromuscular activity during the squat exercise on an unstable platform. Braz. J. Biomot. 2009, 3, 121–129. [Google Scholar]
- McBride, J.M.; Larkin, T.R.; Dayne, A.M.; Haines, T.L.; Kirby, T.J. Effect of Absolute and Relative Loading on Muscle Activity during Stable and Unstable Squatting. Int. J. Sports Physiol. Perform. 2010, 5, 177–183. [Google Scholar] [CrossRef] [PubMed]
- McBride, J.M.; Cormie, P.; Deane, R. Isometric Squat Force Output and Muscle Activity in Stable and Unstable Conditions. J. Strength Cond. Res. 2006, 20, 915. [Google Scholar] [CrossRef] [PubMed]
- Andersen, V.; Fimland, M.S.; Brennset, O.; Haslestad, L.R.; Lundteigen, M.S.; Skalleberg, K.; Saeterbakken, A.H. Muscle Activation and Strength in Squat and Bulgarian Squat on Stable and Unstable Surface. Int. J. Sports Med. 2014, 35, 1196–1202. [Google Scholar] [CrossRef] [PubMed]
- Anderson, K.; Behm, D.G. Trunk Muscle Activity Increases with Unstable Squat Movements. Can. J. Appl. Physiol. 2005, 30, 33–45. [Google Scholar] [CrossRef] [PubMed]
- Jeon, G.-R.; Yu, Y.-W.; To, M.; Hong, J.-H.; Yu, J.-H.; Kim, J.-S.; Lee, D.-Y. A Study on the Selective Strengthening Exercise of the Quadriceps Muscle According to Various Squat Types. Med.-Leg. Update 2020, 20, 1857–1862. [Google Scholar] [CrossRef]
- Kang, J.-I.; Park, J.-S.; Choi, H.; Jeong, D.-K.; Kwon, H.-M.; Moon, Y.-J. A Study on Muscle Activity and Ratio of the Knee Extensor Depending on the Types of Squat Exercise. J. Phys. Ther. Sci. 2017, 29, 43–47. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Choi, Y.H.; Kim, J. The Effects of Changes in Support and Inclined Boards on Lower-Extremity Muscle Activity. J. Phys. Ther. Sci. 2017, 29, 1045–1047. [Google Scholar] [CrossRef][Green Version]
- Marín, P.J.; Hazell, T.J. Effects of Whole-Body Vibration with an Unstable Surface on Muscle Activation. J. Musculoskelet. Neuronal Interact. 2014, 14, 213–219. [Google Scholar]
- Saeterbakken, A.H.; Fimland, M.S. Muscle Force Output and Electromyographic Activity in Squats with Various Unstable Surfaces. J. Strength Cond. Res. 2013, 27, 130–136. [Google Scholar] [CrossRef]
- Gündoğan, B.; Aydin, E.M.; Sağlam, A.F. Muscle Activation during Squat on Different Surfaces. Pamukkale J. Sport. Sci. 2023, 14, 398–407. [Google Scholar] [CrossRef]
- Nairn, B.C.; Sutherland, C.A.; Drake, J.D.M. Motion and Muscle Activity Are Affected by Instability Location during a Squat Exercise. J. Strength Cond. Res. 2017, 31, 677–685. [Google Scholar] [CrossRef] [PubMed]
- Han, D.; Nam, S.; Song, J.; Lee, W.; Kang, T. The Effect of Knee Flexion Angles and Ground Conditions on the Muscle Activation of the Lower Extremity in the Squat Position. J. Phys. Ther. Sci. 2017, 29, 1852–1855. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Krause, D.A.; Elliott, J.J.; Fraboni, D.F.; McWilliams, T.J.; Rebhan, R.L.; Hollman, J.H. Electromyography of the hip and thigh muscles during two variations of the lunge exercise: A cross-sectional study. Int. J. Sports Phys. Ther. 2018, 13, 137–142. [Google Scholar] [CrossRef]
- Miller, W.M.; Barnes, J.T.; Sofo, S.S.; Wagganer, J.D. Comparison of Myoelectric Activity During a Suspension-Based and Traditional Split Squat. J. Strength Cond. Res. 2019, 33, 3236–3241. [Google Scholar] [CrossRef] [PubMed]
- Wahl, M.J.; Behm, D.G. Not All Instability Training Devices Enhance Muscle Activation in Highly Resistance-Trained Individuals. J. Strength Cond. Res. 2008, 22, 1360–1370. [Google Scholar] [CrossRef] [PubMed]
- Behm, D.G.; Anderson, K.; Curnew, R.S. Muscle Force and Activation under Stable and Unstable Conditions. J. Strength Cond. Res. 2002, 16, 416–422. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.-W.; Han, J.-Y.; Kang, M.-H.; Ha, S.-M.; Oh, J.-S. Comparison of Posterior Oblique Sling Activity during Hip Extension in the Prone Position on the Floor and on a Round Foam Roll. J. Phys. Ther. Sci. 2013, 25, 977–979. [Google Scholar] [CrossRef][Green Version]
- Sandhu, J.; Mahajan, S.; Shenoy, S. An Electromyographic Analysis of Shoulder Muscle Activation during Push-up Variations on Stable and Labile Surfaces. Int. J. Shoulder Surg. 2008, 2, 30. [Google Scholar] [CrossRef]
- De Mey, K.; Danneels, L.; Cagnie, B.; Borms, D.; T’Jonck, Z.; Van Damme, E.; Cools, A.M. Shoulder Muscle Activation Levels during Four Closed Kinetic Chain Exercises with and without Redcord Slings. J. Strength Cond. Res. 2014, 28, 1626–1635. [Google Scholar] [CrossRef] [PubMed]
- Park, S.-Y.; Yoo, W.-G. Effects of Push-up Exercise Phase and Surface Stability on Activation of the Scapulothoracic Musculature. Int. J. Athl. Ther. Train. 2013, 18, 34–38. [Google Scholar] [CrossRef]
- Nairn, B.C.; Sutherland, C.A.; Drake, J.D.M. Location of Instability During a Bench Press Alters Movement Patterns and Electromyographical Activity. J. Strength Cond. Res. 2015, 29, 3162–3170. [Google Scholar] [CrossRef] [PubMed]
- Lehman, G.J.; MacMillan, B.; MacIntyre, I.; Chivers, M.; Fluter, M. Shoulder Muscle EMG Activity during Push up Variations on and off a Swiss Ball. Dyn. Med. 2006, 5, 7. [Google Scholar] [CrossRef] [PubMed]
- Torres, R.J.B.; Pirauá, A.L.T.; Nascimento, V.Y.S.; dos Santos, P.S.; Beltrão, N.B.; de Oliveira, V.M.A.; Pitangui, A.C.R.; de Araújo, R.C. Shoulder Muscle Activation Levels during the Push-up-plus Exercise on Stable and Unstable Surfaces. J. Sport. Rehabil. 2017, 26, 281–286. [Google Scholar] [CrossRef] [PubMed]
- De Bezerra, E.S.; da Orssatto, L.B.R.; Werlang, L.C.; Generoso, A.M.; Moraes, G.; Sakugawa, R.L. Effect of Push-up Variations Performed with Swiss Ball on Muscle Electromyographic Amplitude in Trained Men: A Cross-Sectional Study. J. Bodyw. Mov. Ther. 2020, 24, 74–78. [Google Scholar] [CrossRef] [PubMed]
- de Oliveira, A.S.; de Morais Carvalho, M.; de Brum, D.P.C. Activation of the Shoulder and Arm Muscles during Axial Load Exercises on a Stable Base of Support and on a Medicine Ball. J. Electromyogr. Kinesiol. 2008, 18, 472–479. [Google Scholar] [CrossRef] [PubMed]
- Herrington, L.; Waterman, R.; Smith, L. Electromyographic Analysis of Shoulder Muscles during Press-up Variations and Progressions. J. Electromyogr. Kinesiol. 2015, 25, 100–106. [Google Scholar] [CrossRef] [PubMed]
- Pontillo, M.; Orishimo, K.F.; Kremenic, I.J.; McHugh, M.P.; Mullaney, M.J.; Tyler, T.F. Shoulder Musculature Activity and Stabilization during Upper Extremity Weight-Bearing Activities. N. Am. J. Sports Phys. Ther. 2007, 2, 90–96. [Google Scholar]
- Patterson, J.M.; Vigotsky, A.D.; Oppenheimer, N.E.; Feser, E.H. Differences in Unilateral Chest Press Muscle Activation and Kinematics on a Stable versus Unstable Surface While Holding One versus Two Dumbbells. PeerJ 2015, 3, e1365. [Google Scholar] [CrossRef]
- Anderson, K.G.; Behm, D.G. Maintenance of EMG Activity and Loss of Force Output with Instability. J. Strength Cond. Res. 2004, 18, 637–640. [Google Scholar] [PubMed]
- Marshall, P.W.M.; Murphy, B.A. Increased Deltoid and Abdominal Muscle Activity during Swiss Ball Bench Press. J. Strength Cond. Res. 2006, 20, 745–750. [Google Scholar] [PubMed]
- Saeterbakken, A.H.; Fimland, M.S. Electromyographic Activity and 6RM Strength in Bench Press on Stable and Unstable Surfaces. J. Strength Cond. Res. 2013, 27, 1101–1107. [Google Scholar] [CrossRef] [PubMed]
- Reiser, F.C.; Lira, J.L.O.; Bonfim, B.M.A.; Filho, S.J.A.S.; Durante, B.G.; Cardoso, J.M.D.; Miotto, H.; Soares, M.A.A.; Bonuzzi, G.M.G.; Tavares, L.D. Electromyography of Dumbbell Fly Exercise Using Different Planes and Labile Surfaces. J. Exerc. Physiol. Online 2017, 20, 31–40. [Google Scholar]
- Park, S.; Yoo, W.; Kwon, H.; Kim, D.; Lee, S.; Park, M. Scapulothoracic Muscle Activation on Stable and Unstable Support Surfaces. Int. J. Athl. Ther. Train. 2013, 18, 25–29. [Google Scholar] [CrossRef]
- Anderson, G.S.; Gaetz, M.; Holzmann, M.; Twist, P. Comparison of EMG Activity during Stable and Unstable Push-up Protocols. Eur. J. Sport. Sci. 2013, 13, 42–48. [Google Scholar] [CrossRef]
- Kohler, J.M.; Flanagan, S.P.; Whiting, W.C. Muscle Activation Patterns While Lifting Stable and Unstable Loads on Stable and Unstable Surfaces. J. Strength Cond. Res. 2010, 24, 313–321. [Google Scholar] [CrossRef] [PubMed]
- Jeong, S.Y.; Chung, S.H.; Shim, J.H. Comparison of Upper Trapezius, Anterior Deltoid, and Serratus Anterior Muscle Activity during Pushup plus Exercise on Slings and a Stable Surface. J. Phys. Ther. Sci. 2014, 26, 937–939. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Kendall, F.; McCreary, E.; Provance, P. Muscles: Testing and Function, 4th ed.; Williams and Wilkins: Baltimore, MD, USA, 1993. [Google Scholar]
- George, S.Z.; Fritz, J.M.; Silfies, S.P.; Schneider, M.J.; Beneciuk, J.M.; Lentz, T.A.; Gilliam, J.R.; Hendren, S.; Norman, K.S.; Beattie, P.F.; et al. Interventions for the Management of Acute and Chronic Low Back Pain: Revision 2021. J. Orthop. Sports Phys. Ther. 2021, 51, CPG1–CPG60. [Google Scholar] [CrossRef]
- Seo, B.-D.; Yun, Y.-D.; Kim, H.-R.; Lee, S.-H. Effect of 12-Week Swiss Ball Exercise Program on Physical Fitness and Balance Ability of Elderly Women. J. Phys. Ther. Sci. 2012, 2, 11–15. [Google Scholar] [CrossRef]
- Pirauá, A.L.T.; Pitangui, A.C.R.; Silva, J.P.; dos Passos, M.H.P.; de Oliveira, V.M.A.; da Batista, L.S.P.; de Araújo, R.C. Electromyographic Analysis of the Serratus Anterior and Trapezius Muscles during Push-Ups on Stable and Unstable Bases in Subjects with Scapular Dyskinesis. J. Electromyogr. Kinesiol. 2014, 24, 675–681. [Google Scholar] [CrossRef] [PubMed]
- Ebben, W.P.; Wurm, B.; VanderZanden, T.L.; Spadavecchia, M.L.; Durocher, J.J.; Bickham, C.T.; Petushek, E.J. Kinetic Analysis of Several Variations of Push-Ups. J. Strength Cond. Res. 2011, 25, 2891–2894. [Google Scholar] [CrossRef] [PubMed]
- Pirauá, A.L.T.; Beltrão, N.B.; Santos, C.X.; Pitangui, A.C.R.; de Araújo, R.C. Analysis of Muscle Activity during the Bench Press Exercise Performed with the Pre-Activation Method on Stable and Unstable Surfaces. Kinesiology 2017, 49, 161–168. [Google Scholar] [CrossRef][Green Version]
- Lephart, S.M.; Henry, T.J. The Physiological Basis for Open and Closed Kinetic Chain Rehabilitation for the Upper Extremity. J. Sports Rehab. 1996, 5, 71–87. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Muscle | ↑ Unstable Surface | ↑ Stable Surface | ↔ No Difference between Surfaces | Total Number of Studies | |
|---|---|---|---|---|---|
| Core | Rectus abdominis | 12 studies [14,15,32,38,40,41,42,43,44,45,46,47] | ---- | 11 studies [48,49,50,51,52,53,54,55,56,57,58] | 23 studies |
| External oblique | 9 studies [15,41,43,44,45,46,47,59,60] | 2 studies [42,55] | 10 studies [32,38,50,51,52,53,54,56,57,58] | 21 studies | |
| Internal oblique | 3 studies [43,46,57] | ---- | 4 studies [48,50,54,56] | 7 studies | |
| Erector spinae | 3 studies [14,41,59] | ---- | 9 studies [32,40,42,46,47,48,56,58,60] | 12 studies | |
| Lumbar multifidus | 1 study [14] | 1 study [49] | 6 studies [31,46,47,48,50,53] | 8 studies | |
| Transversus abdominis | 1 study [54] | ---- | 1 study [54] | 2 studies | |
| Lower limbs | Vastus lateralis | 4 studies [5,61,62,63] | 2 studies [64,65] | 13 studies [6,18,33,38,39,66,67,68,69,70,71,72,73] | 19 studies |
| Vastus medialis | 6 studies [5,61,62,63,71,74] | 1 study [65] | 11 studies [4,6,18,66,68,69,70,72,73,75] | 18 studies | |
| Rectus femoris | 3 studies [33,63,74] | 1 study [72] | 9 studies [4,6,18,66,68,70,76,77,78] | 13 studies | |
| Quadriceps | ---- | 1 study [79] | ---- | 1 study | |
| Biceps femoris | 2 studies [5,74] | 1 study [64] | 13 studies [4,6,18,33,38,39,65,66,67,72,75,78,80] | 16 studies | |
| Gluteus maximus | 3 studies [76,77,80] | ---- | 2 studies [18,74] | 5 studies | |
| Semitendinosus | 1 study [6] | ---- | ---- | 1 study | |
| Semimembranosus | ---- | ---- | 1 study [6] | 1 study | |
| Hamstring | 1 study [76] | ---- | ---- | 1 study | |
| Soleus | 1 study [79] | ---- | ---- | 1 study | |
| Upper limbs | Pectoralis major | 11 studies [9,10,16,17,25,26,28,30,81,82,83] | 1 study [84] | 17 studies [2,3,20,27,38,39,85,86,87,88,89,90,91,92,93,94,95] | 29 studies |
| Triceps brachii | 13 studies [16,17,26,27,28,30,38,81,85,87,90,96,97] | 3 studies [84,94,98] | 9 studies [2,9,19,24,25,83,86,92,93] | 25 studies | |
| Anterior deltoid | 8 studies [9,10,17,24,84,88,93,99] | 8 studies [2,26,27,28,82,86,87,90] | 8 studies [20,29,39,89,92,94,95,98] | 24 studies | |
| Latissimus dorsi | 1 study [82] | ---- | 1 study [19] | 2 studies | |
| Middle trapezius | ---- | 1 study [82] | 1 study [19] | 2 studies | |
| Posterior deltoid | ---- | ---- | 2 studies [19,82] | 2 studies | |
| Biceps brachii | 1 study [9] | ---- | 2 studies [2,19] | 3 studies |
| Subgroup Categories | Types of Exercises | Studies | Std. Mean Difference, Random [95% CI] | I-Squared [%] | Std. Mean Difference, Random [95% CI] (Sensitivity Analysis) | I-Squared [%] (Sensitivity Analysis) | |
|---|---|---|---|---|---|---|---|
| Core | Rectus abdominis | 7 | [14,15,41,43,45,46,48,50,51,52,53,57,58] | 0.54 [0.33, 0.75] | 56% | 0.51 [0.37, 0.66] | 0% |
| External oblique | 6 | [15,41,43,45,46,50,51,52,53,57,58,59] | 0.48 [0.29, 0.67] | 39% | 0.44 [0.28, 0.61] | 19% | |
| Internal oblique | 1 | [43,46] | 1.04 [0.02, 2.07] | 74% | Not possible | - | |
| Erector spinae | 4 | [14,41,46,48,58,59] | 0.47 [0.18, 0.76] | 53% | 0.37 [0.04, 0.71] | 52% | |
| Lumbar multifidus | 3 | [14,46,48,53] | 0.35 [0.08, 0.61] | 32% | Not performed | - | |
| Lower limbs | Vastus lateralis | 4 | [5,6,18,33,38,39,61,62,66,68,69,71,72,73] | 0.27 [−0.17, 0.72] | 85% | 0.03 [−0.14, 0.21] | 0% |
| Vastus medialis | 4 | [5,6,18,61,62,64,68,69,71,72,73,75] | 0.20 [−0.35, 0.76] | 88% | −0.10 [−0.40, 0.20] | 43% | |
| Rectus femoris | 1 | [6,68,72] | −0.93 [−2.36, 0.50] | 94% | −0.26 [−1.01, 0.49] | 61% | |
| Biceps femoris | 4 | [5,6,18,33,38,39,64,66,72,75] | 0.12 [−0.09, 0.33] | 0% | 0.09 [−0.14, 0.32] | 0% | |
| Upper limbs | Pectoralis major | 7 | [2,3,17,20,25,26,27,28,30,38,39,81,82,83,85,89,90,94] | 0.29 [0.14, 0.44] | 21% | 0.28 [0.09, 0.47] | 31% |
| Triceps brachii | 4 | [2,17,24,25,26,27,28,30,81,83,85,94,96,97] | 0.48 [0.12, 0.84] | 80% | 0.45 [0.25, 0.66] | 7% | |
| Anterior deltoid | 4 | [2,17,20,24,26,27,28,29,38,39,89,90,94] | −0.11 [−0.43, 0.21] | 72% | 0.08 [−0.14, 0.30] | 24% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Batista, G.d.A.; Beltrán, S.P.; Passos, M.H.P.d.; Calixtre, L.B.; Santos, L.R.d.H.; de Araújo, R.C. Comparison of the Electromyography Activity during Exercises with Stable and Unstable Surfaces: A Systematic Review and Meta-Analysis. Sports 2024, 12, 111. https://doi.org/10.3390/sports12040111
Batista GdA, Beltrán SP, Passos MHPd, Calixtre LB, Santos LRdH, de Araújo RC. Comparison of the Electromyography Activity during Exercises with Stable and Unstable Surfaces: A Systematic Review and Meta-Analysis. Sports. 2024; 12(4):111. https://doi.org/10.3390/sports12040111
Chicago/Turabian StyleBatista, Gabriel de Amorim, Sol Patricia Beltrán, Muana Hiandra Pereira dos Passos, Letícia Bojikian Calixtre, Laís Regina de Holanda Santos, and Rodrigo Cappato de Araújo. 2024. "Comparison of the Electromyography Activity during Exercises with Stable and Unstable Surfaces: A Systematic Review and Meta-Analysis" Sports 12, no. 4: 111. https://doi.org/10.3390/sports12040111
APA StyleBatista, G. d. A., Beltrán, S. P., Passos, M. H. P. d., Calixtre, L. B., Santos, L. R. d. H., & de Araújo, R. C. (2024). Comparison of the Electromyography Activity during Exercises with Stable and Unstable Surfaces: A Systematic Review and Meta-Analysis. Sports, 12(4), 111. https://doi.org/10.3390/sports12040111