
The Influence of Menstrual Cycle Phases on Maximal Strength Performance in Healthy Female Adults: A Systematic Review with Meta-Analysis

 ,
,  , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Literature Search
2.2. Selection Criteria
2.3. Methodological Study Quality
2.4. Data Extraction and Data Processing
2.5. Statistical Analysis
3. Results
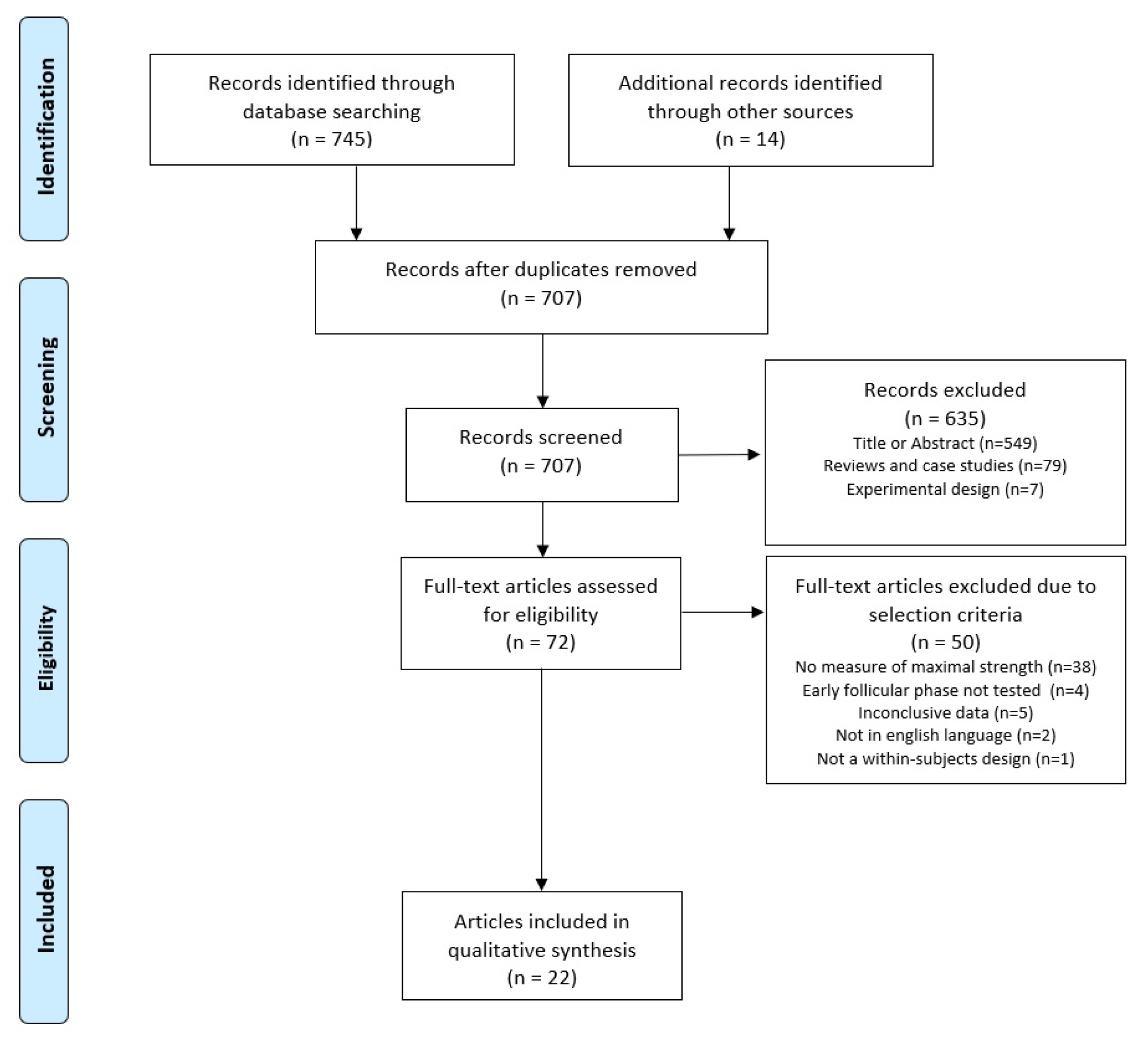
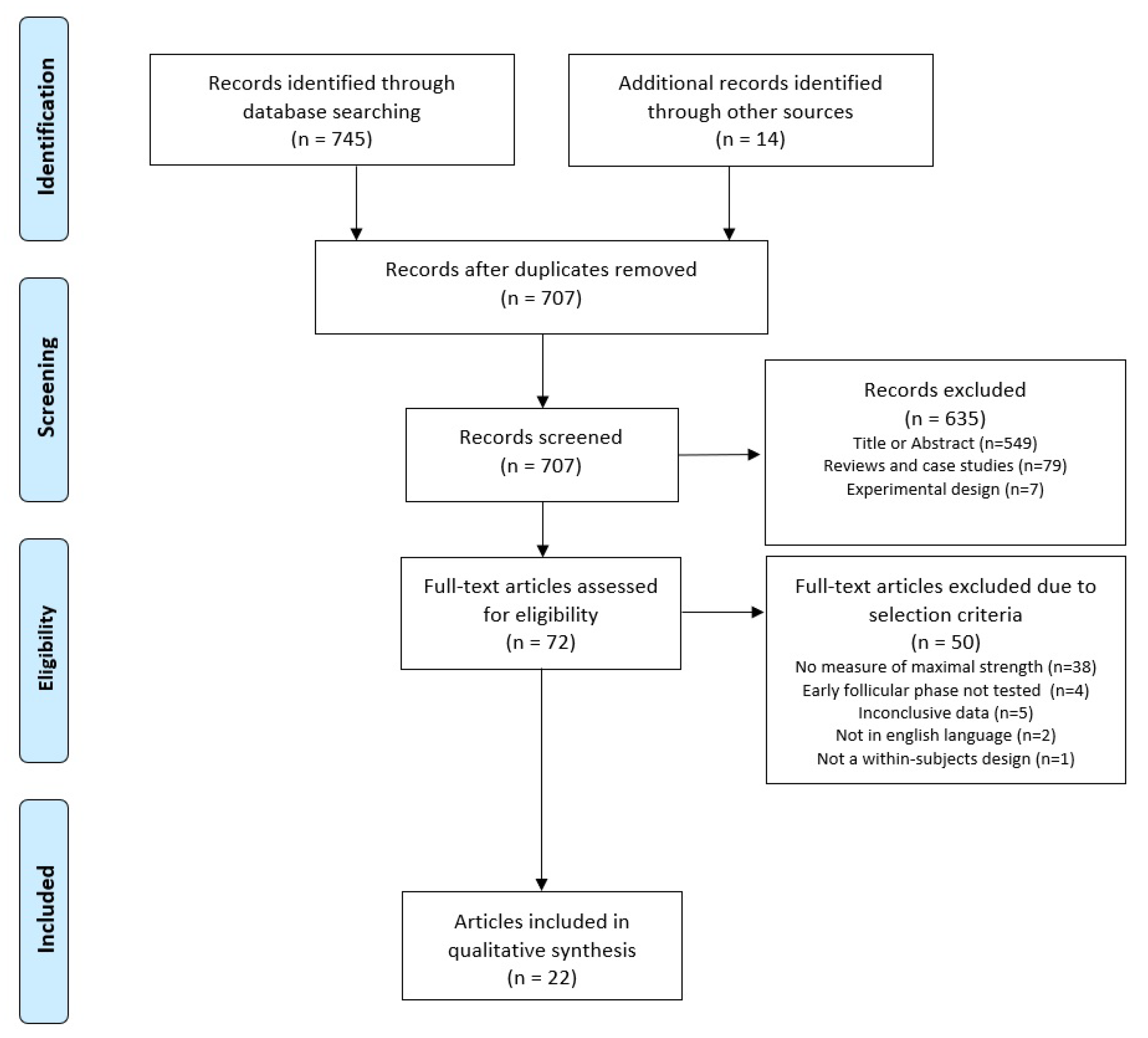
3.1. Selection of Studies
3.2. Study Characteristics
3.3. Methodological Study Quality
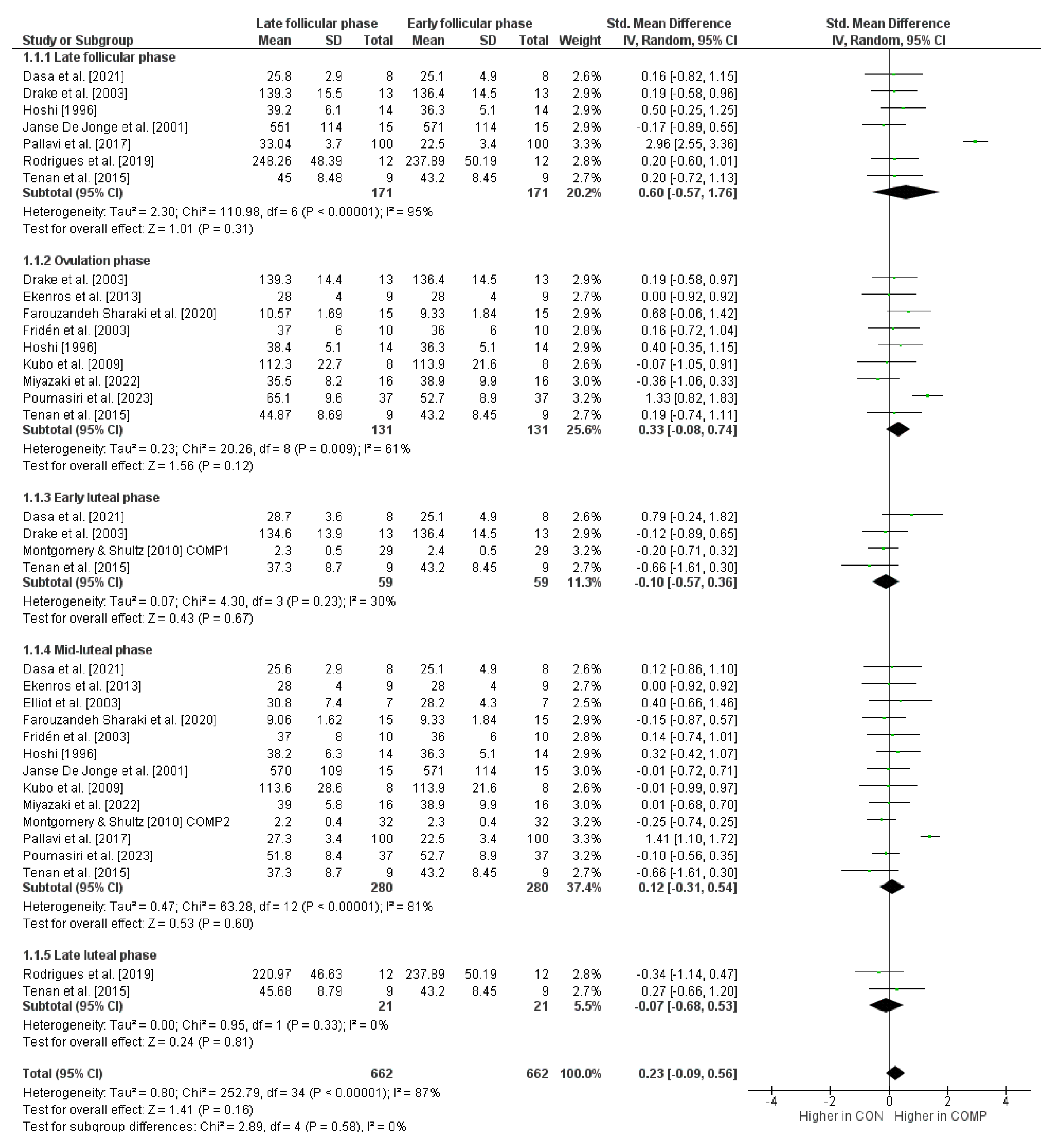
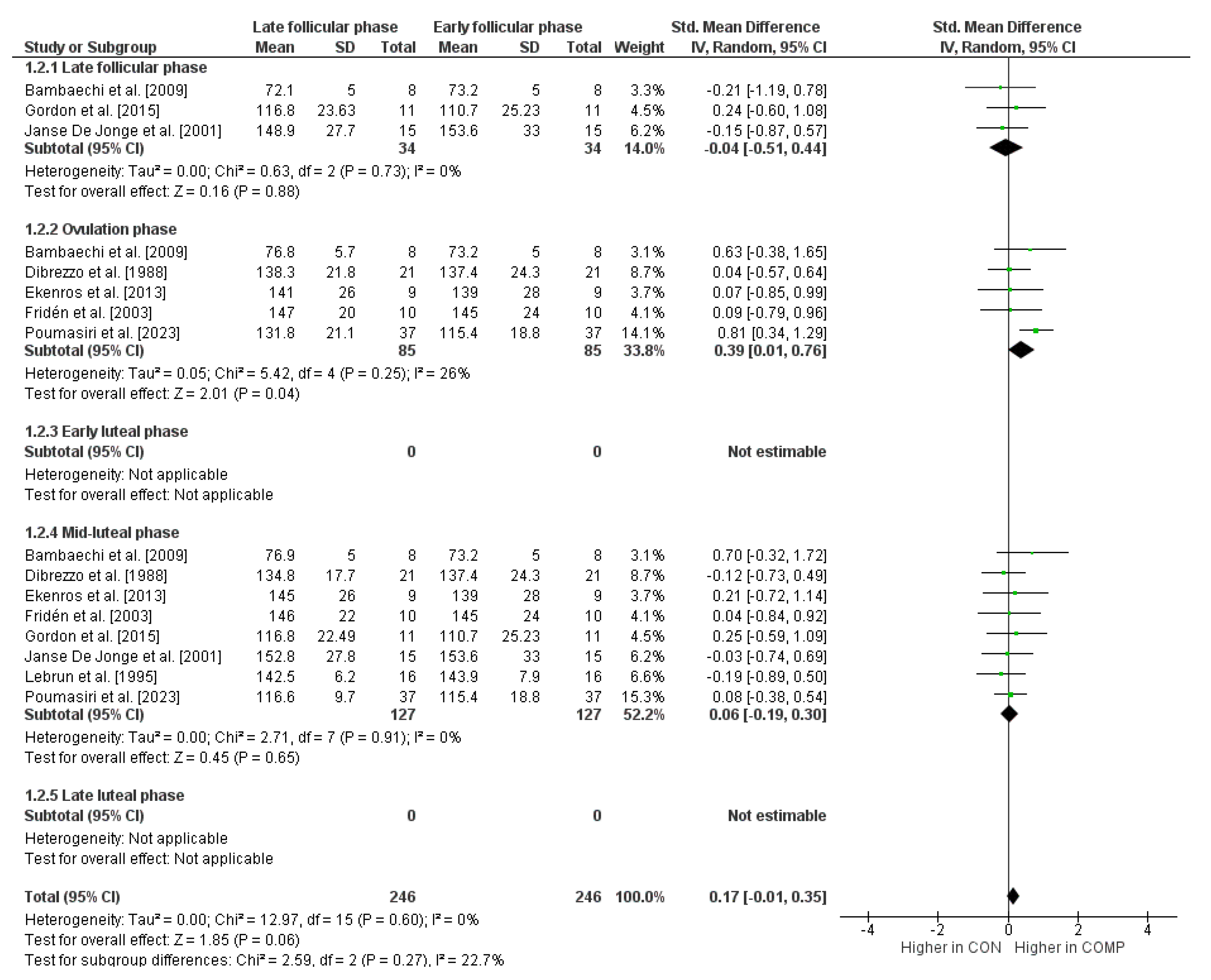
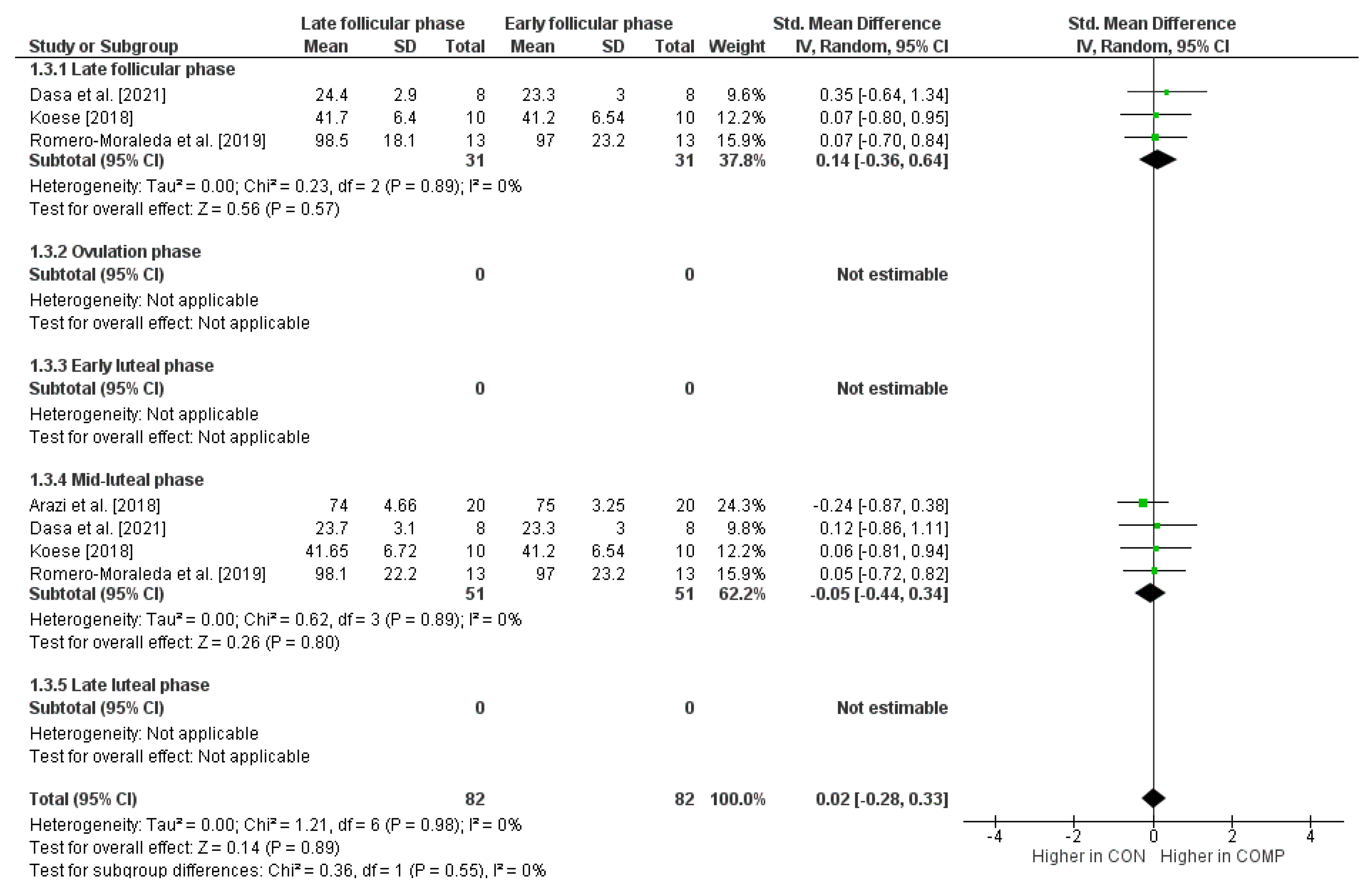
3.4. Influence of the Cycle Phases on Maximal Strength Performance
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Castanier, C.; Bougault, V.; Teulier, C.; Jaffré, C.; Schiano-Lomoriello, S.; Vibarel-Rebot, N.; Villemain, A.; Rieth, N.; Le-Scanff, C.; Buisson, C.; et al. The Specificities of Elite Female Athletes: A Multidisciplinary Approach. Life 2021, 11, 622. [Google Scholar] [CrossRef] [PubMed]
- Janse De Jonge, X.; Thompson, B.; Han, A. Methodological Recommendations for Menstrual Cycle Research in Sports and Exercise. Med. Sci. Sports Exerc. 2019, 51, 2610–2617. [Google Scholar] [CrossRef] [PubMed]
- Sims, S.T.; Heather, A.K. Myths and Methodologies: Reducing Scientific Design Ambiguity in Studies Comparing Sexes and/or Menstrual Cycle Phases. Exp. Physiol. 2018, 103, 1309–1317. [Google Scholar] [CrossRef]
- Sundström Poromaa, I.; Gingnell, M. Menstrual Cycle Influence on Cognitive Function and Emotion Processing-from a Reproductive Perspective. Front. Neurosci. 2014, 8, 380. [Google Scholar] [CrossRef] [PubMed]
- Maïmoun, L.; Georgopoulos, N.A.; Sultan, C. Endocrine Disorders in Adolescent and Young Female Athletes: Impact on Growth, Menstrual Cycles, and Bone Mass Acquisition. J. Clin. Endocrinol. Metab. 2014, 99, 4037–4050. [Google Scholar] [CrossRef] [PubMed]
- Romero-Moraleda, B.; Coso, J.D.; Gutiérrez-Hellín, J.; Ruiz-Moreno, C.; Grgic, J.; Lara, B. The Influence of the Menstrual Cycle on Muscle Strength and Power Performance. J. Hum. Kinet. 2019, 68, 123–133. [Google Scholar] [CrossRef] [PubMed]
- Haff, G.; Triplett, N.T.; National Strength & Conditioning Association (U.S.) (Eds.) Essentials of Strength Training and Conditioning, 4th ed.; Human Kinetics: Champaign, IL, USA, 2016; ISBN 978-1-4925-0162-6. [Google Scholar]
- Zaciorskij, V.M.; Kraemer, W.J. Science and Practice of Strength Training, 2nd ed.; Human Kinetics: Champaign, IL, USA, 2006; ISBN 978-0-7360-5628-1. [Google Scholar]
- Maffiuletti, N.A.; Aagaard, P.; Blazevich, A.J.; Folland, J.; Tillin, N.; Duchateau, J. Rate of Force Development: Physiological and Methodological Considerations. Eur. J. Appl. Physiol. 2016, 116, 1091–1116. [Google Scholar] [CrossRef]
- Andrade, M.D.S.; De Lira, C.A.B.; Koffes, F.D.C.; Mascarin, N.C.; Benedito-Silva, A.A.; Da Silva, A.C. Isokinetic Hamstrings-to-Quadriceps Peak Torque Ratio: The Influence of Sport Modality, Gender, and Angular Velocity. J. Sports Sci. 2012, 30, 547–553. [Google Scholar] [CrossRef]
- Suchomel, T.J.; Nimphius, S.; Bellon, C.R.; Stone, M.H. The Importance of Muscular Strength: Training Considerations. Sports Med. 2018, 48, 765–785. [Google Scholar] [CrossRef]
- Chaudhari, A.M.W.; Zelman, E.A.; Flanigan, D.C.; Kaeding, C.C.; Nagaraja, H.N. Anterior Cruciate Ligament—Injured Subjects Have Smaller Anterior Cruciate Ligaments than Matched Controls: A Magnetic Resonance Imaging Study. Am. J. Sports Med. 2009, 37, 1282–1287. [Google Scholar] [CrossRef]
- Decker, M.J.; Torry, M.R.; Wyland, D.J.; Sterett, W.I.; Richard Steadman, J. Gender Differences in Lower Extremity Kinematics, Kinetics and Energy Absorption during Landing. Clin. Biomech. 2003, 18, 662–669. [Google Scholar] [CrossRef] [PubMed]
- Paterno, M.V.; Rauh, M.J.; Schmitt, L.C.; Ford, K.R.; Hewett, T.E. Incidence of Contralateral and Ipsilateral Anterior Cruciate Ligament (ACL) Injury after Primary ACL Reconstruction and Return to Sport. Clin. J. Sport. Med. 2012, 22, 116–121. [Google Scholar] [CrossRef] [PubMed]
- Elliott-Sale, K.J.; McNulty, K.L.; Ansdell, P.; Goodall, S.; Hicks, K.M.; Thomas, K.; Swinton, P.A.; Dolan, E. The Effects of Oral Contraceptives on Exercise Performance in Women: A Systematic Review and Meta-Analysis. Sports Med. 2020, 50, 1785–1812. [Google Scholar] [CrossRef]
- De Jonge, X.A.J. Effects of the Menstrual Cycle on Exercise Performance. Sports Med. 2003, 33, 833–851. [Google Scholar] [CrossRef]
- Sung, E.-S.; Kim, J.-H. The Difference Effect of Estrogen on Muscle Tone of Medial and Lateral Thigh Muscle during Ovulation. J. Exerc. Rehabil. 2018, 14, 419–423. [Google Scholar] [CrossRef] [PubMed]
- Yim, J.; Petrofsky, J.; Lee, H. Correlation between Mechanical Properties of the Ankle Muscles and Postural Sway during the Menstrual Cycle. Tohoku J. Exp. Med. 2018, 244, 201–207. [Google Scholar] [CrossRef] [PubMed]
- Kokkonen, J.; Nelson, A.G.; Cornwell, A. Acute Muscle Stretching Inhibits Maximal Strength Performance. Res. Q. Exerc. Sport 1998, 69, 411–415. [Google Scholar] [CrossRef]
- Lorimer, A.V.; Hume, P.A. Stiffness as a Risk Factor for Achilles Tendon Injury in Running Athletes. Sports Med. 2016, 46, 1921–1938. [Google Scholar] [CrossRef]
- Romero-Parra, N.; Cupeiro, R.; Alfaro-Magallanes, V.M.; Rael, B.; Rubio-Arias, J.Á.; Peinado, A.B.; Benito, P.J.; on behalf of the IronFEMME Study Group. Exercise-Induced Muscle Damage During the Menstrual Cycle: A Systematic Review and Meta-Analysis. J. Strength. Cond. Res. 2021, 35, 549–561. [Google Scholar] [CrossRef]
- Stachenfeld, N.S. Sex Hormone Effects on Body Fluid Regulation. Exerc. Sport. Sci. Rev. 2008, 36, 152–159. [Google Scholar] [CrossRef]
- Beynnon, B.D.; Bernstein, I.M.; Belisle, A.; Brattbakk, B.; Devanny, P.; Risinger, R.; Durant, D. The Effect of Estradiol and Progesterone on Knee and Ankle Joint Laxity. Am. J. Sports Med. 2005, 33, 1298–1304. [Google Scholar] [CrossRef] [PubMed]
- Herzberg, S.D.; Motu’apuaka, M.L.; Lambert, W.; Fu, R.; Brady, J.; Guise, J.-M. The Effect of Menstrual Cycle and Contraceptives on ACL Injuries and Laxity: A Systematic Review and Meta-Analysis. Orthop. J. Sports Med. 2017, 5, 2325967117718781. [Google Scholar] [CrossRef] [PubMed]
- Benton, M.J.; Hutchins, A.M.; Dawes, J.J. Effect of Menstrual Cycle on Resting Metabolism: A Systematic Review and Meta-Analysis. PLoS ONE 2020, 15, e0236025. [Google Scholar] [CrossRef] [PubMed]
- Oosthuyse, T.; Bosch, A.N. The Effect of the Menstrual Cycle on Exercise Metabolism: Implications for Exercise Performance in Eumenorrhoeic Women. Sports Med. 2010, 40, 207–227. [Google Scholar] [CrossRef] [PubMed]
- McNulty, K.L.; Elliott-Sale, K.J.; Dolan, E.; Swinton, P.A.; Ansdell, P.; Goodall, S.; Thomas, K.; Hicks, K.M. The Effects of Menstrual Cycle Phase on Exercise Performance in Eumenorrheic Women: A Systematic Review and Meta-Analysis. Sports Med. 2020, 50, 1813–1827. [Google Scholar] [CrossRef] [PubMed]
- Tenan, M.S.; Hackney, A.C.; Griffin, L. Maximal Force and Tremor Changes across the Menstrual Cycle. Eur. J. Appl. Physiol. 2016, 116, 153–160. [Google Scholar] [CrossRef]
- McClung, J.M.; Davis, J.M.; Wilson, M.A.; Goldsmith, E.C.; Carson, J.A. Estrogen Status and Skeletal Muscle Recovery from Disuse Atrophy. J. Appl. Physiol. 2006, 100, 2012–2023. [Google Scholar] [CrossRef]
- Smith, M.J.; Adams, L.F.; Schmidt, P.J.; Rubinow, D.R.; Wassermann, E.M. Effects of Ovarian Hormones on Human Cortical Excitability. Ann. Neurol. 2002, 51, 599–603. [Google Scholar] [CrossRef]
- Gordon, D.; Hughes, F.; Young, K.; Scruton, A.; Keiller, D.; Caddy, O.; Baker, J.; Barnes, R. The Effects of Menstrual Cycle Phase on the Development of Peak Torque under Isokinetic Conditions. IES 2013, 21, 285–291. [Google Scholar] [CrossRef]
- Pallavi, L.C.; Souza, D.U.J.; Shivaprakaash, G. Assessment of Musculoskeletal Strength and Levels of Fatigue during Different Phases of Menstrual Cycle in Young Adults. JCDR 2017, 11, CC11–CC13. [Google Scholar] [CrossRef]
- Phillips, S.K.; Sanderson, A.G.; Birch, K.; Bruce, S.A.; Woledge, R.C. Changes in Maximal Voluntary Force of Human Adductor Pollicis Muscle during the Menstrual Cycle. J. Physiol. 1996, 496, 551–557. [Google Scholar] [CrossRef]
- Lowe, D.A.; Baltgalvis, K.A.; Greising, S.M. Mechanisms Behind Estrogen’s Beneficial Effect on Muscle Strength in Females. Exerc. Sport Sci. Rev. 2010, 38, 61–67. [Google Scholar] [CrossRef]
- Baltgalvis, K.A.; Greising, S.M.; Warren, G.L.; Lowe, D.A. Estrogen Regulates Estrogen Receptors and Antioxidant Gene Expression in Mouse Skeletal Muscle. PLoS ONE 2010, 5, e10164. [Google Scholar] [CrossRef]
- Moran, A.L.; Warren, G.L.; Lowe, D.A. Removal of Ovarian Hormones from Mature Mice Detrimentally Affects Muscle Contractile Function and Myosin Structural Distribution. J. Appl. Physiol. 2006, 100, 548–559. [Google Scholar] [CrossRef] [PubMed]
- Crewther, B.T.; Cook, C.; Cardinale, M.; Weatherby, R.P.; Lowe, T. Two Emerging Concepts for Elite Athletes: The Short-Term Effects of Testosterone and Cortisol on the Neuromuscular System and the Dose-Response Training Role of These Endogenous Hormones. Sports Med. 2011, 41, 103–123. [Google Scholar] [CrossRef] [PubMed]
- Cook, C.J.; Kilduff, L.P.; Crewther, B.T. Basal and Stress-Induced Salivary Testosterone Variation across the Menstrual Cycle and Linkage to Motivation and Muscle Power. Scand. J. Med. Sci. Sports 2018, 28, 1345–1353. [Google Scholar] [CrossRef] [PubMed]
- Dougherty, D.; Bjork, J.; Moeller, F.; Swann, A. The Influence of Menstrual-Cycle Phase on the Relationship Between Testosterone and Aggression. Physiol. Behav. 1997, 62, 431–435. [Google Scholar] [CrossRef] [PubMed]
- Willett, H.N.; Koltun, K.J.; Hackney, A.C. Influence of Menstrual Cycle Estradiol-β-17 Fluctuations on Energy Substrate Utilization-Oxidation during Aerobic, Endurance Exercise. Int. J. Environ. Res. Public Health 2021, 18, 7209. [Google Scholar] [CrossRef]
- Tarnopolsky, M.A. Sex Differences in Exercise Metabolism and the Role of 17-Beta Estradiol. Med. Sci. Sports Exerc. 2008, 40, 648–654. [Google Scholar] [CrossRef]
- Lin, G.; Siddiqui, R.; Lin, Z.; Blodgett, J.M.; Patel, S.N.; Truong, K.N.; Mariakakis, A. Blood Glucose Variance Measured by Continuous Glucose Monitors across the Menstrual Cycle. npj Digit. Med. 2023, 6, 140. [Google Scholar] [CrossRef]
- Sylow, L.; Kleinert, M.; Richter, E.A.; Jensen, T.E. Exercise-Stimulated Glucose Uptake—Regulation and Implications for Glycaemic Control. Nat. Rev. Endocrinol. 2017, 13, 133–148. [Google Scholar] [CrossRef] [PubMed]
- Hummel, J.; Benkendorff, C.; Fritsche, L.; Prystupa, K.; Vosseler, A.; Gancheva, S.; Trenkamp, S.; Birkenfeld, A.L.; Preissl, H.; Roden, M.; et al. Brain Insulin Action on Peripheral Insulin Sensitivity in Women Depends on Menstrual Cycle Phase. Nat. Metab. 2023, 5, 1475–1482. [Google Scholar] [CrossRef] [PubMed]
- Justice, J.N.; Pierpoint, L.A.; Mani, D.; Schwartz, R.S.; Enoka, R.M. Motor Function Is Associated with 1,25(OH)2D and Indices of Insulin–Glucose Dynamics in Non-Diabetic Older Adults. Aging Clin. Exp. Res. 2014, 26, 249–254. [Google Scholar] [CrossRef]
- Del Vecchio, A.; Negro, F.; Holobar, A.; Casolo, A.; Folland, J.P.; Felici, F.; Farina, D. You Are as Fast as Your Motor Neurons: Speed of Recruitment and Maximal Discharge of Motor Neurons Determine the Maximal Rate of Force Development in Humans. J. Physiol. 2019, 597, 2445–2456. [Google Scholar] [CrossRef] [PubMed]
- Tenan, M.S.; Peng, Y.-L.; Hackney, A.C.; Griffin, L. Menstrual Cycle Mediates Vastus Medialis and Vastus Medialis Oblique Muscle Activity. Med. Sci. Sports Exerc. 2013, 45, 2151–2157. [Google Scholar] [CrossRef]
- Ansdell, P.; Brownstein, C.G.; Škarabot, J.; Hicks, K.M.; Simoes, D.C.M.; Thomas, K.; Howatson, G.; Hunter, S.K.; Goodall, S. Menstrual Cycle-Associated Modulations in Neuromuscular Function and Fatigability of the Knee Extensors in Eumenorrheic Women. J. Appl. Physiol. 2019, 126, 1701–1712. [Google Scholar] [CrossRef]
- Maciejczyk, M.; Wiecek, M.; Szymura, J.; Szygula, Z.; Brown, L.E. Influence of Increased Body Mass and Body Composition on Cycling Anaerobic Power. J. Strength. Cond. Res. 2015, 29, 58–65. [Google Scholar] [CrossRef] [PubMed]
- Maciejczyk, M.; Wiecek, M.; Szymura, J.; Cempla, J.; Wiecha, S.; Szygula, Z.; Brown, L.E. Effect of Body Composition on Respiratory Compensation Point During an Incremental Test. J. Strength. Cond. Res. 2014, 28, 2071–2077. [Google Scholar] [CrossRef]
- Maciejczyk, M.; Więcek, M.; Szymura, J.; Szyguła, Z.; Wiecha, S.; Cempla, J. The Influence of Increased Body Fat or Lean Body Mass on Aerobic Performance. PLoS ONE 2014, 9, e95797. [Google Scholar] [CrossRef]
- Fruzzetti, F.; Lello, S.; Lazzarini, V.; Fratta, S.; Orrù, M.; Sorge, R.; Minerba, L.; Ricci, C.; Genazzani, A.R.; Melis, G.B.; et al. The Oral Contraceptive Containing 30 Μg of Ethinylestradiol plus 3 Mg of Drospirenone Is Able to Antagonize the Increase of Extracellular Water Occurring in Healthy Young Women during the Luteal Phase of the Menstrual Cycle: An Observational Study. Contraception 2007, 75, 199–203. [Google Scholar] [CrossRef]
- Stachoń, A.J. Menstrual Changes in Body Composition of Female Athletes. Coll. Antropol. 2016, 40, 111–122. [Google Scholar]
- Akturk, M.; Toruner, F.; Aslan, S.; Altinova, A.E.; Cakir, N.; Elbeg, S.; Arslan, M. Circulating Insulin and Leptin in Women with and without Premenstrual Disphoric Disorder in the Menstrual Cycle. Gynecol. Endocrinol. 2013, 29, 465–469. [Google Scholar] [CrossRef] [PubMed]
- Szmuilowicz, E.D.; Adler, G.K.; Williams, J.S.; Green, D.E.; Yao, T.M.; Hopkins, P.N.; Seely, E.W. Relationship between Aldosterone and Progesterone in the Human Menstrual Cycle. J. Clin. Endocrinol. Metab. 2006, 91, 3981–3987. [Google Scholar] [CrossRef]
- Blagrove, R.C.; Bruinvels, G.; Pedlar, C.R. Variations in Strength-Related Measures during the Menstrual Cycle in Eumenorrheic Women: A Systematic Review and Meta-Analysis. J. Sci. Med. Sport. 2020, 23, 1220–1227. [Google Scholar] [CrossRef]
- Carmichael, M.A.; Thomson, R.L.; Moran, L.J.; Wycherley, T.P. The Impact of Menstrual Cycle Phase on Athletes’ Performance: A Narrative Review. Int. J. Env. Res. Public. Health 2021, 18, 1667. [Google Scholar] [CrossRef] [PubMed]
- Massulo, J.D.F.; Nascimento, M.A.D.; Nolêto, D.C.D.S.; Soares, E.D.S.; Lima, G.D.S.O.; Silva, L.P.D.; Coêlho, P.G.D.; Nolêto, V.L.; Silva, A.G.; Lourenço, B.D.S. Influence of the Phases of the Menstrual Cycle on Strength Capacity in Resistance Training. ISHR 2023, 2, 66–77. [Google Scholar] [CrossRef]
- Thompson, B.; Almarjawi, A.; Sculley, D.; Janse De Jonge, X. The Effect of the Menstrual Cycle and Oral Contraceptives on Acute Responses and Chronic Adaptations to Resistance Training: A Systematic Review of the Literature. Sports Med. 2020, 50, 171–185. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, n71. [Google Scholar] [CrossRef]
- Guellich, A.; Schmidtbleicher, D. Struktur Der Kraftfähigkeiten Und Ihrer Trainingsmethoden. Dtsch. Z. Für Sportmed. 1999, 50, 223–234. [Google Scholar]
- Knowles, O.E.; Aisbett, B.; Main, L.C.; Drinkwater, E.J.; Orellana, L.; Lamon, S. Resistance Training and Skeletal Muscle Protein Metabolism in Eumenorrheic Females: Implications for Researchers and Practitioners. Sports Med. 2019, 49, 1637–1650. [Google Scholar] [CrossRef]
- Janicijevic, D.; Knezevic, O.M.; Garcia-Ramos, A.; Cvetic, D.; Mirkov, D.M. Isokinetic Testing: Sensitivity of the Force-Velocity Relationship Assessed through the Two-Point Method to Discriminate between Muscle Groups and Participants’ Physical Activity Levels. Int. J. Environ. Res. Public. Health 2020, 17, 8570. [Google Scholar] [CrossRef]
- Muehlbauer, T.; Granacher, U.; Borde, R.; Hortobágyi, T. Non-Discriminant Relationships between Leg Muscle Strength, Mass and Gait Performance in Healthy Young and Old Adults. Gerontology 2018, 64, 11–18. [Google Scholar] [CrossRef]
- Farouzandeh Shahraki, S.; Minoonejad, H.; Moghadas Tabrizi, Y. Comparison of Some Intrinsic Risk Factors of Shoulder Injury in Three Phases of Menstrual Cycle in Collegiate Female Athletes. Phys. Ther. Sport. 2020, 43, 195–203. [Google Scholar] [CrossRef] [PubMed]
- Croft, P.; Pope, D.; Zonca, M.; O’Neill, T.; Silman, A. Measurement of Shoulder Related Disability: Results of a Validation Study. Ann. Rheum. Dis. 1994, 53, 525–528. [Google Scholar] [CrossRef] [PubMed]
- Nodehi-Moghadam, A.; Nasrin, N.; Kharazmi, A.; Eskandari, Z. A Comparative Study on Shoulder Rotational Strength, Range of Motion and Proprioception between the Throwing Athletes and Non-Athletic Persons. Asian J. Sports Med. 2013, 4, 34–40. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Routledge: New York, NY, USA, 1988; ISBN 978-0-203-77158-7. [Google Scholar]
- Deeks, J.J.; Higgins, J.P.; Altman, D.G.; on behalf of the Cochrane Statistical Methods Group. Analysing Data and Undertaking. Meta-analyses. In Cochrane Handbook for Systematic Reviews of Interventions; Higgins, J., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; Wiley: New York, NY, USA, 2019; pp. 241–284. ISBN 978-1-119-53662-8. [Google Scholar]
- Higgins, J.P.T.; Thompson, S.G. Quantifying Heterogeneity in a Meta-Analysis. Statist. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]
- Bambaeichi, E.; Reilly, T.; Cable, N.T.; Giacomoni, M. The Isolated and Combined Effects of Menstrual Cycle Phase and Time-of-Day on Muscle Strength of Eumenorrheic Females. Chronobiol. Int. 2004, 21, 645–660. [Google Scholar] [CrossRef] [PubMed]
- Dasa, M.S.; Kristoffersen, M.; Ersvær, E.; Bovim, L.P.; Bjørkhaug, L.; Moe-Nilssen, R.; Sagen, J.V.; Haukenes, I. The Female Menstrual Cycles Effect on Strength and Power Parameters in High-Level Female Team Athletes. Front. Physiol. 2021, 12, 600668. [Google Scholar] [CrossRef]
- Drake, S.M.; Evetovich, T.; Eschbach, C.; Webster, M. A Pilot Study on the Effect of Oral Contraceptives on Electromyography and Mechanomyography during Isometric Muscle Actions. J. Electromyogr. Kinesiol. 2003, 13, 297–301. [Google Scholar] [CrossRef]
- Hoshi, A. Changes in Muscular Strength of Women in Different Phases of the Menstrual Cycle. Bull. Nippon. Dent. Univ. 1997, 26, 219–224. [Google Scholar]
- Janse De Jonge, X.A.; Boot, C.R.; Thom, J.M.; Ruell, P.A.; Thompson, M.W. The Influence of Menstrual Cycle Phase on Skeletal Muscle Contractile Characteristics in Humans. J. Physiol. 2001, 530, 161–166. [Google Scholar] [CrossRef] [PubMed]
- Koese, B. Analysis of the Effect of Menstrual Cycle Phases on Aerobic-Anaerobic Capacity and Muscle Strength. JETS 2018, 6, 23. [Google Scholar] [CrossRef]
- Rodrigues, P.; Correia, M.; Wharton, L. Effect of Menstrual Cycle on Muscle Strength. J. Exerc. Physiol. Online 2019, 22, 89–97. [Google Scholar]
- Arazi, H.; Nasiri, S.; Eghbali, E. Is There a Difference toward Strength, Muscular Endurance, Anaerobic Power and Hormonal Changes between the Three Phase of the Menstrual Cycle of Active Girls? Apunts. Med. De. L’esport 2019, 54, 65–72. [Google Scholar] [CrossRef]
- Dibrezzo, R.; Fort, I.L.; Brown, B. Dynamic Strength and Work Variations during Three Stages of the Menstrual Cycle. J. Orthop. Sports Phys. Ther. 1988, 10, 113–116. [Google Scholar] [CrossRef] [PubMed]
- Ekenros, L.; Hirschberg, A.L.; Heijne, A.; Fridén, C. Oral Contraceptives Do Not Affect Muscle Strength and Hop Performance in Active Women. Clin. J. Sport. Med. 2013, 23, 202–207. [Google Scholar] [CrossRef] [PubMed]
- Fridén, C.; Hirschberg, A.L.; Saartok, T. Muscle Strength and Endurance Do Not Significantly Vary Across 3 Phases of the Menstrual Cycle in Moderately Active Premenopausal Women. Clin. J. Sport. Med. 2003, 13, 238–241. [Google Scholar] [CrossRef]
- Kubo, K.; Miyamoto, M.; Tanaka, S.; Maki, A.; Tsunoda, N.; Kanehisa, H. Muscle and Tendon Properties during Menstrual Cycle. Int. J. Sports Med. 2009, 30, 139–143. [Google Scholar] [CrossRef]
- Miyazaki, M.; Maeda, S. Changes in Hamstring Flexibility and Muscle Strength during the Menstrual Cycle in Healthy Young Females. J. Phys. Ther. Sci. 2022, 34, 92–98. [Google Scholar] [CrossRef]
- Pournasiri, F.; Zarei, M.; Mainer-Pardos, E.; Rubio-Morales, A.; Nobari, H. Isometric and Isokinetic Strength of Lower-Limb Muscles in Female Athletes during Different Phases of Menstrual Cycle: A Causal-Comparative Study. BMC Women’s Health 2023, 23, 657. [Google Scholar] [CrossRef]
- Montgomery, M.M.; Shultz, S.J. Isometric Knee-Extension and Knee-Flexion Torque Production during Early Follicular and Postovulatory Phases in Recreationally Active Women. J. Athl. Train. 2010, 45, 586–593. [Google Scholar] [CrossRef] [PubMed]
- Elliott, K.J.; Cable, N.T.; Reilly, T.; Diver, M.J. Effect of Menstrual Cycle Phase on the Concentration of Bioavailable 17-Beta Oestradiol and Testosterone and Muscle Strength. Clin. Sci. 2003, 105, 663–669. [Google Scholar] [CrossRef]
- Lebrun, C.M.; McKenzie, D.C.; Prior, J.C.; Taunton, J.E. Effects of Menstrual Cycle Phase on Athletic Performance. Med. Sci. Sports Exerc. 1995, 27, 437–444. [Google Scholar] [CrossRef] [PubMed]
- Frankovich, R.J.; Lebrun, C.M. Menstrual Cycle, Contraception, And Performance. Clin. Sports Med. 2000, 19, 251–271. [Google Scholar] [CrossRef] [PubMed]
- Gharahdaghi, N.; Phillips, B.E.; Szewczyk, N.J.; Smith, K.; Wilkinson, D.J.; Atherton, P.J. Links Between Testosterone, Oestrogen, and the Growth Hormone/Insulin-Like Growth Factor Axis and Resistance Exercise Muscle Adaptations. Front. Physiol. 2021, 11, 621226. [Google Scholar] [CrossRef] [PubMed]
- Kissow, J.; Jacobsen, K.J.; Gunnarsson, T.P.; Jessen, S.; Hostrup, M. Effects of Follicular and Luteal Phase-Based Menstrual Cycle Resistance Training on Muscle Strength and Mass. Sports Med. 2022, 52, 2813–2819. [Google Scholar] [CrossRef]
- Sung, E.; Han, A.; Hinrichs, T.; Vorgerd, M.; Manchado, C.; Platen, P. Effects of Follicular versus Luteal Phase-Based Strength Training in Young Women. Springerplus 2014, 3, 668. [Google Scholar] [CrossRef]
- Thompson, B.M.; Drover, K.B.; Stellmaker, R.J.; Sculley, D.V.; Janse De Jonge, X.A.K. The Effect of the Menstrual Cycle and Oral Contraceptive Cycle on Muscle Performance and Perceptual Measures. Int. J. Environ. Res. Public Health 2021, 18, 10565. [Google Scholar] [CrossRef]
- Allen, A.M.; McRae-Clark, A.L.; Carlson, S.; Saladin, M.E.; Gray, K.M.; Wetherington, C.L.; McKee, S.A.; Allen, S.S. Determining Menstrual Phase in Human Biobehavioral Research: A Review with Recommendations. Exp. Clin. Psychopharmacol. 2016, 24, 1–11. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Category | Inclusion Criteria | Exclusion Criteria |
|---|---|---|
| Population | women with a regular menstrual cycle | women taking hormonal contraceptives or who had menstrual cycle disorders |
| Intervention | assessment of maximal muscle strength in a clearly defined cycle phase | no measurements of maximal muscle strength or unclearly defined cycle phase |
| Comparator | early follicular phase | studies not including early follicular phase |
| Outcome | maximal isometric, isokinetic, or dynamic muscle strength | muscle power or impulse |
| Study design | longitudinal | between-subjects design, case studies, reviews |
| Category | Preferred Outcome | Alternative Outcome |
| Isometric maximal strength | MVIC knee extension (n = 7) | MVIC handgrip strength (n = 5) MVIC FDI strength (n = 1) MVIC leg press (n = 1) MVIC shoulder internal rotation (n = 1) |
| Isokinetic maximal strength | Peak torque knee extension 60°/s (n = 4) | Peak torque knee extension 120°/s (n = 2) Peak torque knee extension 90°/s (n = 1) Peak torque knee extension 30°/s (n = 1) |
| Dynamic maximal strength | 1RM half-squat (n = 1) | 1RM leg press (n = 1) 1RM bench press (n = 1) |
| References | No. of Subjects (Sex); Activity; Age (Mean ± SD, or Range); Height (Mean ± SD, or Range); Mass (Mean ± SD, or Range); Determination of Cycle Phase | Compared Menstrual Cycle Phases | Muscle Groups or Function Examined; Method; Side | Test Modality; Outcome Measures | Results, Mean (SD) | Level of Evidence |
|---|---|---|---|---|---|---|
| Arazi et al. [78] | 20 (F); recreationally active; 26.27 ± 2.75 yrs; 161 ± 4.25 cm; 60.14 ± 7.60 kg; blood sample | COMP1: ovulation (days 12–14) COMP2: mid-luteal (days 18–25) CON: early follicular (days 3–8) | Leg press; dynamic strength; bilateral | Calculation: 1RM with repetitions until exhaustion | 1RM leg press (kg) COMP1: 72 (5.72) COMP2: 74 (4.66) CON: 75 (3.25) | Low |
| Bambaeichi et al. [71] | 8; sedentary/inactive; 30 ± 5 yrs; 163 ± 6 cm; 66.25 ± 4.6 kg; urine sample | COMP1: late follicular (days 7–9) COMP2: ovulation COMP3: mid-luteal (days 19–21) CON: early follicular (days 1–4) | Knee extension; isokinetic strength; dominant | 1 familiarization trial Warm-up: 5 min cycle ergometer (80–120 W) 3 attempts; 180 s rest between; supine position; knee ROM 90° | Peak torque knee extension at 90°/s (Nm) COMP1: 72.1 (5) COMP2: 76.8 (5.7) COMP3: 76.9 (5) CON: 73.2 (5) | Low |
| Dasa et al. [72] | 8; high-level athletes; 22.5 ± 4.2 yrs; 168.8 ± 8.9 cm; 63.1 ± 9.3 kg; blood sample | COMP1: late follicular (week 2) COMP2: early luteal (week 3) COMP3: mid-luteal (week 4) CON: early follicular (week 1) | Handgrip; isometric strength; dominant | Warm-up: 15 min cycle ergometer (100 W) Handgrip: 2 attempts; seated; 90° elbow flexion; 3–5 s duration; 30 s rest between | MVIC handgrip strength (kg) COMP1: 25.8 (2.9) COMP2: 28.7 (3.6) COMP3: 25.6 (2.9) CON: 25.1 (4.9) | Moderate |
| Dibrezzo et al. [79] | 21; healthy; 18–36 yrs; NA; 65 ± 9 kg; counting days | COMP1: ovulation (days 13–14) COMP2: mid-luteal (day 10 from ovulation) CON: early follicular (day 1) | Knee flexion and extension; isokinetic strength; dominant | 3 familiarization trials 4 attempts; 45 s rest between; velocity 60°/s and 180°/s | Peak torque knee extension at 60°/s (Nm) COMP1: 138.3 (21.8) COMP2: 134.8 (17.7) CON: 137.4 (24.3) | Very low |
| Drake et al. [73] | 13; inactive; 24 ± 1 yrs; 1.68 ± 0.02 m; 70.97 ± 4.81 kg; urine sample | COMP1: late follicular (days 9–11) COMP2: ovulation COMP3: early luteal (5 days after ovulation) CON: early follicular (days 1–3) | Knee extension; isometric strength; dominant | 1 familiarization trial 2 max attempts; highest used for analysis; 3 s duration; 180 s rest between; 45° leg flexion | MVIC knee extension (Nm) COMP1: 139.3 (15.5) COMP2: 139.3 (14.4) COMP3: 134.6 (13.9) CON: 136.4 (14.5) | Very low |
| Ekenros et al. [80] | 9; recreationally active; 27.0 ± 4.8 yrs; 166.8 ± 5.2 cm; 61.8 ± 6.5 kg; blood sample | COMP1: ovulation COMP2: mid-luteal (days 7–8 after ovulation) CON: early follicular (days 2–4) | Hand grip; isometric strength; dominant Knee extension; isokinetic strength; right | 3 familiarization trials Warm-up: 10 min cycle ergometer (150 W) Handgrip strength: 3 attempts; elbow extended, arm beside body Knee extension: 5 attempts; back supporter in 85° angle; velocity 120°/s; knee ROM 90–10° | MVIC handgrip strength (kg) COMP1: 28 (4) COMP2: 28 (4) CON: 28 (4) Peak torque knee extension 120°/s (Nm) COMP1: 141 (26) COMP2: 145 (26) CON: 139 (28) | Moderate |
| Elliot et al. [86] | 7; healthy; 25 ± 5 yrs; 1.6 ± 0.1 m; 62.1 ± 2.7 kg; urine sample | INT: mid-luteal (day 21) CON: early follicular (day 2) | First dorsal interosseus muscle; isometric strength; dominant | 2 familiarization trials Warm-up: hand and forearm with heating pad to 40 °C skin temperature 3 sub-max attempts; 180 s rest between; 3 max attempts for data; 60 s rest between | MVIC FDI strength (N) INT: 30.8 (7.4) CON: 28.2 (4.3) | Low |
| Farouzandeh Sharaki et al. [65] | 15; athletes; 23.27 ± 1.66 yrs; 167 ± 0.05 cm; 57.60 ± 6.75 kg; urine sample | COMP1: ovulation (days 1–2 after ovulation) COMP2: mid-luteal (day 7 after ovulation) CON: early follicular (days 1–3) | Shoulder internal rotation; isometric strength; dominant | 90° angle in the elbow Internal rotation in the supine position | MVIC shoulder internal rotation (kg) COMP1: 10.57 (1.69) COMP2: 9.06 (1.62) CON: 9.33 (1.84) | Low |
| Fridén et al. [81] | 10; recreationally active; 25.3 ± 3.7 yrs; 171 ± 5 cm; 66 ± 7 kg; blood sample | COMP1: ovulation COMP2: mid-luteal (day 7 after ovulation) CON: early follicular (days 3–5) | Handgrip; isometric strength; dominant Knee extension; isokinetic strength; right | 1 familiarization trial Warm-up: 10 min cycle ergometer Handgrip: 3 attempts; elbow extended, arm beside body Knee extension: 5 attempts; back supporter in 85° angle; velocity 120°/s; knee ROM 90–10° | MVIC handgrip strength (kg) COMP1: 37 (6) COMP2: 37 (8) CON: 36 (6) Peak torque knee extension 120°/s (Nm) COMP1: 147 (20) COMP2: 146 (22) CON: 145 (24) | Moderate |
| Gordon et al. [31] | 11; athletes; 20.7 ± 1.4 yrs; 166.8 ± 7.1 cm; 59.2 ± 6.9 kg; saliva sample | COMP1: late follicular (days 9–11) COMP2: mid-luteal (days 19–20) COMP3: late luteal (days 27–28) CON: early follicular (days 1–3) | Knee extension; isokinetic strength; NA | Warm-up: 4 concentric extension/flexions at 60°/s, followed by a 30 s recovery period 5 attempts; 180 s rest between; velocity 60°/s | Peak torque knee extension at 60°/s(Nm) COMP1: 116.8 (23.63) COMP2: 116.8 (22.49) COMP3: 116.2 (22.34) CON: 110.7 (25.23) | Low |
| Hoshi [74] | 14; healthy; 19.6 ± 1 yrs; 162.1 ± 4.3 cm; 46.2 ± 5.5 kg; blood sample | COMP1: late follicular (days 7–12) COMP2: ovulation (days 1–2 after start ovulation) COMP3: mid-luteal (days 7–12 after start of ovulation) CON: early follicular (days 2–5) | Handgrip; isometric strength; NA | No information provided | MVIC handgrip strength (kg) COMP1: 39.2 (6.1) COMP2: 38.4 (5.1) COMP3: 38.2 (6.3) CON: 36.3 (5.1) | Low |
| Janse de Jonge et al. [75] | 15; healthy; 29.9 ± 8.0 yrs; 167 ± 7 cm; 61.4 ± 8.4 kg; blood sample | COMP1: late follicular COMP2: mid-luteal CON: early follicular (days 1–3) | Knee flexion and extension; isometric and isokinetic strength; dominant | Warm-up: 10 min cycle ergometer (50 W) with cadence of 60 rpm Knee extension isometric: 5 attempts; 120 s rest between Knee flexion isokinetic: 5 attempts; 120 s rest between; 60°/s and 240°/s Knee extension isokinetic: 5 attempts; 120 s rest between; 60°/s and 240°/s | MVIC knee extension (N) COMP1: 551 (114) COMP2: 570 (109) CON: 571 (114) Peak torque knee extension at 60°/s (Nm) COMP1: 148.9 (27.7) COMP2: 152.8 (27.8) CON: 153.6 (33.0) | Moderate |
| Koese [76] | 10; athletes; 21.4 ± 2.01 yrs; 169.6 ± 6.14 cm; 63.9 ± 5.76 kg; counting days | COMP1: late follicular (days 8–9) COMP2: mid-luteal (days 22–23) CON: early follicular (days 2–3) | Bench press; dynamic strength; bilateral | 1RM test (until exhaustion with 65% of 1RM) | 1RM bench press (kg) COMP1: 41.7 (6.4) COMP2: 41.65 (6.72) CON: 41.2 (6.54) | Very low |
| Kubo et al. [82] | 8; sedentary; 22.5 ± 0.9 yrs; 160.2 ± 5.1 cm; 56.4 ± 3.7 kg; blood sample | COMP1: ovulation (days 1–2 after ovulation) COMP2: mid-luteal (days 7–10 after ovulation) CON: early follicular (days 1–3) | Knee extension; isometric strength; right | Warm-up: dynamic submaximal knee extension 3 attempts; 5 s duration; 180 s rest between; 90° knee flexion; strong verbal encouragement | MVIC knee extension (Nm) COMP1: 112.3 (22.7) COMP2: 113.6 (28.6) CON: 113.9 (21.6) | Moderate |
| Lebrun et al. [87] | 16; athletes; 27.6 ± 3.8 yrs; 167.9 ± 5.3 cm; 59.6 ± 6.7 kg; blood sample | INT: mid-luteal (days 4–9 after ovulation) CON: early follicular (days 3–8) | Knee flexion and extension; isokinetic; right | Warm-up: short and unspecific 3 attempts; seated | Peak torque knee extension at 30°/s (Nm) INT: 142.5 (6.2) CON: 143.9 (7.9) | Moderate |
| Miyazaki and Maeda [83] | 16; healthy; 21 ± 1 yrs; 159.5 ± 4.7 cm; 52.5 ± 5 kg; urine sample | COMP1: ovulation (days 2–3 after ovulation) COMP2: mid-luteal (days 20–22) CON: early follicular (day 3) | Knee extension; isometric strength; right | 1 attempt; 3 s duration; prone position; 90° knee flexion; verbal encouragement | MVIC knee extension (Nm) COMP1: 35.3 (8.2) COMP2: 39 (5.8) CON: 38.9 (9.9) | Low |
| Montgomery & Shultz [85] | 61; recreationally active; COMP1: 21.5 ± 2.7 yrs; 164.9 ± 7.2 cm; 61.7 ± 9.3 kg; Blood sample COMP2: 21.2 ± 2.4 yrs; 164.0 ± 6.6 cm; 60.8 ± 9.1 kg; blood sample | COMP1 (n = 29): Early luteal (days 10–24) CON1 (n = 29): Early follicular (days 1–3) COMP2 (n = 32): Mid-luteal (days 15–28) CON2 (n = 32): Early follicular (days 1–3) | Knee flexion and extension; isometric strength; dominant | Familiarization trials at 25, 50, 75, and 100% perceived maximal effort Warm-up: 5 min cycle ergometer 3 attempts; 3 s duration; 30 s rest between; 20° knee flexion; strong verbal encouragement | MVIC knee extension (Nm/kg) COMP1: 2.3 (0.5) CON1: 2.4 (0.5) COMP2: 2.2 (0.4) CON2: 2.3 (0.4) | High |
| Pallavi et al. [32] | 100; healthy; 18.4 ± 0.7 yrs; 150 ± 6 cm; 50 ± 4.9 kg; NA | COMP1: late follicular COMP2: mid-luteal CON: Early follicular (day 1) | Handgrip; isometric strength | 3 attempts; verbal encouragement | MVIC handgrip strength (kg) COMP1: 33.04 (3.7) COMP2: 27.3 (3.4) CON: 22.5 (3.4) | Very low |
| Poumasiri et al. [84] | 37; athletes; 21.65 ± 3.5 yrs; 171.14 ± 9.2 cm; 64.07 ± 4.9 kg; self-report | COMP1: ovulation (days 10–14) COMP2: mid-luteal (days 15–28) CON: early follicular (days 1–9) | Knee flexion and extension; isokinetic and isometric strength; dominant | Warm-up: 15 min cycle ergometer 3 attempts; 20 s rest between; back supporter in 70–85° angle; velocity 60°/s; knee ROM 0–90° | Peak torque knee extension at 60°/s (Nm) COMP1: 131.8 (21.1 COMP2: 116.6 (9.7) CON: 115.4 (18.8) MVIC knee extension (Nm2) COMP1: 65.1 (9.6) COMP2: 51.8 (8.4) CON: 52.7 (8.9) | Very low |
| Rodrigues et al. [77] | 12; recreationally active; 27.2 ± 3.4 yrs; 168.62 ± 5.19 cm; 61.37 ± 6.29 kg; counting days | COMP1: late follicular (days 2–3) COMP2: late luteal (days 2–3 before menstruation) CON: early follicular (days 1–2 of menstruation) | Leg press; isometric strength; bilateral | 1 familiarization trial Warm-up: 5 repetitions of leg press with 50% and then 70% 1RM with 2 min set break 3 attempts; 180 s rest between; 45° knee flexion (2–10 reps, with increments of 2, 3 or 4% with more than 10 possible reps | MVIC leg press (kg) COMP1: 248.26 (48.39) COMP2: 220.97 (46.63) CON: 237.89 (50.19) | Very low |
| Romero-Moraleda et al. [6] | 13; athletes; 31.1 ± 5.5 yrs; 166 ± 6 cm; 58.6 ± 7.8 kg; urine sample | COMP1: late follicular (days 8–14) COMP2: mid-luteal (days 15–28) CON: early follicular (days 1–7) | Half squat; dynamic strength; bilateral | 1 familiarization trial 1RM test with loads to 20, 40, 60, and 80% of 1RM, vertical guides regulate the barbell movement | 1RM half-squat (kg) COMP1: 98.5 (18.1) COMP2: 98.1 (22.2) CON: 97 (23.2) | Low |
| Tenan et al. [28] | 9; recreationally active; 24.7 ± 4.5 yrs; body temperature | COMP1: late follicular (days 7–12) COMP2: ovulation (days 13–15) COMP3: early luteal (days 16–22) COMP4: late luteal (days 22–28) CON: early follicular (days 1–6) | Knee extension; isometric strength; dominant | Warm-up: 12 dynamic submaximal knee extension without resistance 3 attempts; 3 s duration; 30 s rest between; seated; 90° knee flexion; strong verbal encouragement | MVIC knee extension (kg) COMP1: 45.0 (8.48) COMP2: 44.87 (8.69) COMP3: 37.3 (8.7) COMP4: 45.68 (8.79) CON: 43.2 (8.45) | Very low |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Niering, M.; Wolf-Belala, N.; Seifert, J.; Tovar, O.; Coldewey, J.; Kuranda, J.; Muehlbauer, T. The Influence of Menstrual Cycle Phases on Maximal Strength Performance in Healthy Female Adults: A Systematic Review with Meta-Analysis. Sports 2024, 12, 31. https://doi.org/10.3390/sports12010031
Niering M, Wolf-Belala N, Seifert J, Tovar O, Coldewey J, Kuranda J, Muehlbauer T. The Influence of Menstrual Cycle Phases on Maximal Strength Performance in Healthy Female Adults: A Systematic Review with Meta-Analysis. Sports. 2024; 12(1):31. https://doi.org/10.3390/sports12010031
Chicago/Turabian StyleNiering, Marc, Nacera Wolf-Belala, Johanna Seifert, Ole Tovar, Jacqueline Coldewey, Jennifer Kuranda, and Thomas Muehlbauer. 2024. "The Influence of Menstrual Cycle Phases on Maximal Strength Performance in Healthy Female Adults: A Systematic Review with Meta-Analysis" Sports 12, no. 1: 31. https://doi.org/10.3390/sports12010031
APA StyleNiering, M., Wolf-Belala, N., Seifert, J., Tovar, O., Coldewey, J., Kuranda, J., & Muehlbauer, T. (2024). The Influence of Menstrual Cycle Phases on Maximal Strength Performance in Healthy Female Adults: A Systematic Review with Meta-Analysis. Sports, 12(1), 31. https://doi.org/10.3390/sports12010031