
Medicalization of Sport? A Mixed-Method Study on the Use of Medications in Elite Ice Hockey


Abstract
1. Introduction
2. Methods
2.1. Quantitative Data from Doping Control Forms
2.2. Qualitative Data: Experimental Approach and Participants
2.3. Qualitative Data Analysis
2.4. Ethical Considerations
3. Results
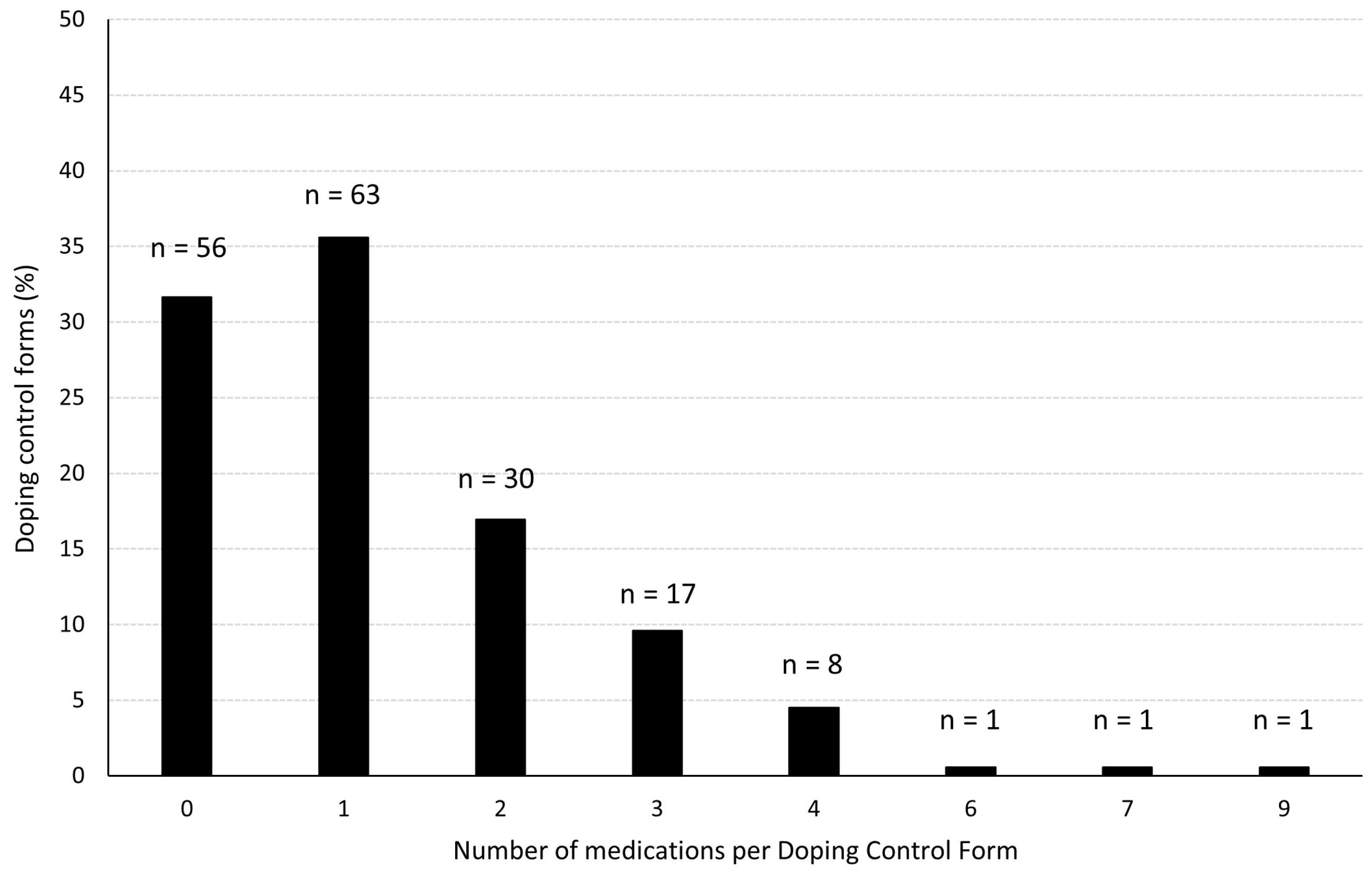
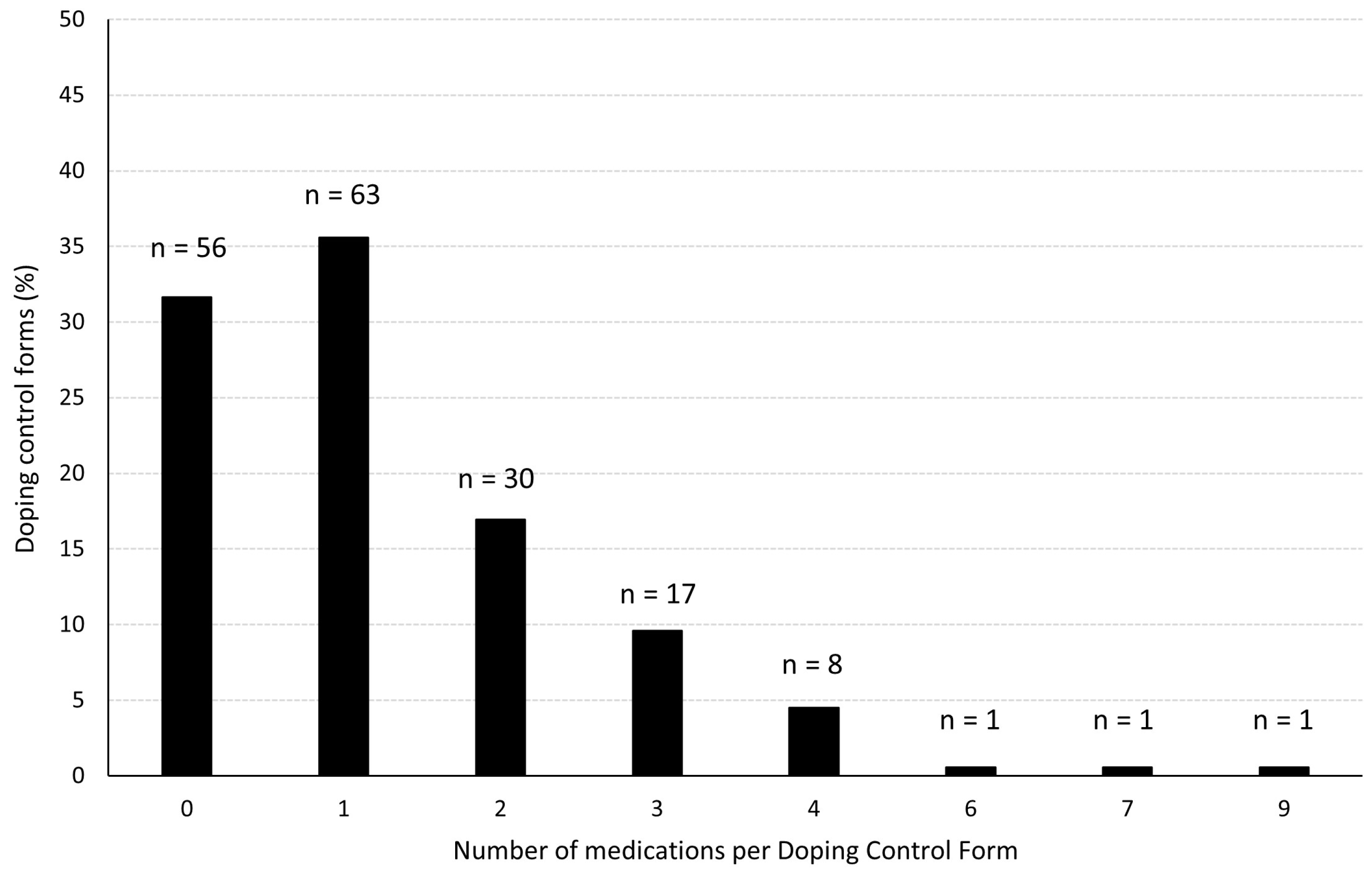
3.1. Quantitative Results—Doping Control Forms
3.2. Qualitative Results—Focus Group Interviews
3.2.1. Use of Analgesics
“Yes, itߣs a bit macho and loose […] But I think the social environment in hockey is a bit like you keep going until it simply doesnߣt work anymore. You donߣt want to lose your position on the team.”(Athlete 11)
“There is a bit of that macho reputation, and the sport also has a bit of that macho reputation. So, I remember even from when I was younger that it was almost tough to play injured, in a way. Then you could almost brag about it to teammates and such: I have an injury, but Iߣm playing.”(Athlete 10)
“To get rid of some pain and inflammation and things like that. Players take a lot of impact damage. And as “athlete 22” says, when there are a lot of matches and such, there is something you can take to get ready. If it’s next Saturday (the match), there might be quick solutions to things.”(Athlete 24)
“Interviewer: Yes, where have you come across local anesthetics?Athlete 17: No, so itߣs something you can take if youߣve gotten an injury. So simply just to play without too much pain. Then you take it. Itߣs quite common, for example, during playoffs and in similar situations. One tries to maybe avoid it during regular league matches. But in the playoffs, itߣs, I think itߣs almost, that it exists in all teams, that everyone plays a bit half-injured, so maybe you put a syringe in the shoulder or in the legs just to play if you have gotten shot (by the hockey puck) there.Interview: Mm. How is this done? Is it done on the sidelines or after the match?Athlete 17: No, it is done before, so that the effect occurs at the right time, so itߣs done before or right after the warm-up or during the break and so on. Since we play three periods, we always have 18-min breaks where it can be done.Interviewer: Yes, is it done nowadays or in the past?Athlete 17: No, itߣs still being done, yes.”
“Toward the playoffs, the threshold for not playing will be extremely high […] If there are six weeks left, you persevere. So, if you have an upcoming surgery after that, if you use somewhat stronger tablets for the six weeks, such a long period before the surgery, then the risk of getting addicted is present. Especially for tramadol and the tablets we are talking about here. But itߣs not very often, but you hear about it sometimes… But there are exceptions. That players are abusing and overusing these drugs during such periods probably happens more often than in other sports because these periods are so intense. Maybe more often in ice hockey than in other sports because itߣs so intense.”(Athlete 6)
3.2.2. Use of Hypnotics
“Iߣve seen some who has used a lot of sleeping pills. Thatߣs probably what sticks out about ice hockey when I think back. Painkillers are ok, I think. But when you start taking sleeping pills, that is worse.”(Athlete 4)
“We have seen examples of that, yes. Eh, weߣve had teammates who today struggle with heavier substances. So, Iߣve seen that.”(Athlete 17)
“It has often been like that, itߣs been a problem with it in (country), but the team physicians have been strict about it. Then you have played in some clubs, you know some physicians, and of course there are some who have been a bit sloppy with it who can give prescriptions elsewhere. Itߣs been a big problem in hockey in general, at least in the leagues Iߣve played. But I havenߣt even seen it here, to be completely honest. But I know there have been challenges associated with this in the past.”(Athlete 17)
“Yes, so the fact that itߣs being used is because we often play late matches. Itߣs also a very adrenaline-filled sport. So, itߣs quite a challenge to fall asleep after matches. A lot of people have it. Then itߣs getting up early the next day, and there is often a tight match schedule.”(Athlete 21)
“Instead of getting to the hotel room at 11:30 p.m. and staying up until three oߣclock without getting any sleep, and you have to wake up at 7 or 8 a.m., you take a sleeping pill when you get to the hotel room or something, then youߣll probably fall asleep at midnight or 12:30 a.m. But you donߣt sleep well, because in a way you are ruining the quality of your sleep. But at least you are able to fall asleep.”(Athlete 7)
“But there are quite a few people who have the problem after matches that they cannot fall asleep, no matter how the match went, because we still have a lot of adrenaline after the match. Letߣs say you play a match at 7 p.m., then youߣre not home until 11 p.m., and you still have some adrenaline, canߣt sleep. Then you have training and work early the next day.”(Athlete 14)
“But then there are perhaps more hockey players than in other team sports who are not quite professional, while in football most are professionals. Here, there are quite a few who have a job on the side. So, yes, but there are a lot of people here who have more on their plate, perhaps. Not getting as much rest.”(Athlete 25)
“I think itߣs a disadvantage that you have in a team a collection of athletes with such a big difference in age. For example, there may be a culture among some older people who use sleeping pills. So, they do that; take some sleeping pills to be able to sleep because they must go to work the next day or have small children. And then the 17-year-old on the team sees that and thinks “Oh, he takes it, it is cool”, they also start taking it, without even needing it. And then it becomes more likely that they may use it in some form (as a recreational drug) to get high, that is what is dangerous. A large group with a large age difference, so itߣs like that. You can never guarantee that it will be used for what itߣs supposed to be used for when so many get access to it. So, I think itߣs much better that itߣs something that everyone must discuss with their physician, rather than that it is, for example, handed out to everyone.”(Athlete 21)
3.2.3. Trust in the Athlete Support Personnel
“A while ago I was given a new medication, and then our physician checked anti-doping (webpage), and confirmed that it was ok to use, so it could be prescribed. So, then it was up to the physician to check it. So, then we don’t have to also check it once the physician has checked it.”(Athlete 18)
“They are a team, right. The physician and Johaug (former Norwegian cross-country skier), they are like a team. You trust that person a lot. You (the interviewer) are the one who knows about it, I have no idea, but you (the interviewer) do. Then he (the physician) says that it is ok. Should you go to someone else who is not on the team to verify it? If he (the other physician) knows it’s allowed but also that it can make you better, then he might say no because he doesn’t want you to get better because he’s on a different team, right. Then I would rather completely trust my own physician.”(Athlete 14)
“I actually got some injections. It happened when I played in X (club). He is quite liberal. Haha (laughs). The physician. I was in so much pain, so he gave me three shots, and then I was completely gone. I believe it was something like local anesthesia. I don’t know… It was during a match, so it was the other team’s physician that helped me.”(Athlete 24)
“I can imagine that if it concerns individual sports and there is a new drug they are going to use, they ask the physician right away, whereas here it’s often the case that I had asked the physician and it’s like yes, it’s probably ok. Even if you have easy access to the physician, you could just send a message, but you don’t have the same relationship as individual athletes do.”(Athlete 20)
4. Discussion
5. Limitations
6. Perspective
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Alaranta, A.; Alaranta, H.; Heliövaara, M.; Airaksinen, M.; Helenius, I. Ample use of physician-prescribed medications in Finnish elite athletes. Int. J. Sports Med. 2006, 27, 919–925. [Google Scholar] [CrossRef] [PubMed]
- Tscholl, P.M.; Vaso, M.; Weber, A.; Dvorak, J. High prevalence of medication use in professional football tournaments including the World Cups between 2002 and 2014: A narrative review with a focus on NSAIDs. Br. J. Sports Med. 2015, 49, 580–582. [Google Scholar] [CrossRef] [PubMed]
- Overbye, M. Walking the line? An investigation into elite athletes’ sport-related use of painkillers and their willingness to use analgesics to train or compete when injured. Int. Rev. Sociol. Sport 2021, 56, 1091–1115. [Google Scholar] [CrossRef]
- Selanne, H.; Ryba, T.V.; Siekkinen, K.; Kyröläinen, H.; Kautiainen, H.; Hakonen, H.; Mikkelsson, M.; Kujala, U.M. The prevalence of musculoskeletal pain and use of painkillers among adolescent male ice hockey players in Finland. Health Psychol. Behav. Med. 2014, 2, 448–454. [Google Scholar] [CrossRef] [PubMed]
- Gjelstad, A.; Herlofsen, T.M.; Bjerke, A.-L.; Lauritzen, F.; Björnsdottir, I. Use of pharmaceuticals amongst athletes tested by Anti-Doping Norway in a five-year period. Front. Sports Act. Living 2023, 5, 1260806. [Google Scholar] [CrossRef] [PubMed]
- Warden, S. Prophylactic misuse and recommended use of non-steroidal anti-inflammatory drugs by athletes. Br. J. Sports Med. 2009, 43, 548–549. [Google Scholar] [CrossRef] [PubMed]
- Manfredini, R.; Manfredini, F.; Conconi, F. Standard melatonin intake and circadian rhythms of elite athletes after a transmeridian flight. J. Int. Med. Res. 2000, 28, 182–186. [Google Scholar] [CrossRef]
- Drawer, S.; Fuller, C.W. Evaluating the level of injury in English professional football using a risk based assessment process. Br. J. Sports Med. 2002, 36, 446–451. [Google Scholar] [CrossRef]
- Cameron, A.F.M.; Perera, N.; Fulcher, M. Professional Athletes Have Poorer Sleep Quality and Sleep Hygiene Compared With an Age-Matched Cohort. Clin. J. Sport Med. 2021, 31, 488–493. [Google Scholar] [CrossRef]
- Burns, J.; Mason, C.; Mueller, N.; Ohlander, J.; Zock, J.P.; Drobnic, F.; Wolfarth, B.; Heinrich, J.; Omenaas, E.; Stensrud, T.; et al. Asthma prevalence in Olympic summer athletes and the general population: An analysis of three European countries. Respir. Med. 2015, 109, 813–820. [Google Scholar] [CrossRef]
- Waddington, I. The Development of Sports Medicine. Sociol. Sport J. 1996, 13, 176–196. [Google Scholar] [CrossRef]
- Kundu, P. A Medical Sociological Perspective of Doping in Sports. Int. J. Phys. Educ. Sports Sci. 2018, 13, 32–37. [Google Scholar] [CrossRef] [PubMed]
- WADA. The Prohibited List. Available online: https://www.wada-ama.org/en/prohibited-list (accessed on 30 November 2023).
- Melzer, M.; Elbe, A.-M.; Strahler, K. Athletes’ use of analgesics is related to doping attitudes, competitive anxiety, and situational opportunity. Front. Sports Act. Living 2022, 4, 849117. [Google Scholar] [CrossRef] [PubMed]
- Thevis, M.; Kuuranne, T.; Fedoruk, M.; Geyer, H. Sports drug testing and the athletes’ exposome. Drug Test. Anal. 2021, 13, 1814–1821. [Google Scholar] [CrossRef] [PubMed]
- Atkinson, M. Sport and Risk Culture. In The Suffering Body in Sport; Research in the Sociology of Sport; Emerald Publishing Limited: Bingley, UK, 2019; Volume 12, pp. 5–21. [Google Scholar]
- Gaetz, M. Substance availability and use in ex-professional ice hockey enforcers. Sci. Rep. 2022, 12, 22204. [Google Scholar] [CrossRef] [PubMed]
- Davies, C.R. Addiction & Substance Abuse in the NHL—It’s Bigger Than the Game. The Hockey Writers, 10 November 2021. [Google Scholar]
- Nimens, R. Pushing through the pain, NHLers say theyߣre regulalry taking painkillers in order to play. CTV News, 23 October 2020. [Google Scholar]
- Basu, A. Paul Byron is looking forward to a life without chronic pain, something that is all too rare in hockey. The Athletic, 4 February 2022. [Google Scholar]
- WADA. International Standard for Testing and Investigations; WADA: Montreal, QC, Canada, 2021. [Google Scholar]
- Lauritzen, F.; Gjelstad, A. Trends in dietary supplement use among athletes selected for doping controls. Front. Nutr. 2023, 10, 1143187. [Google Scholar] [CrossRef]
- Gill, P.; Stewart, K.; Treasure, E.; Chadwick, B. Methods of data collection in qualitative research: Interviews and focus groups. Br. Dent. J. 2008, 204, 291–295. [Google Scholar] [CrossRef]
- Hennink, M.; Kaiser, B.N. Sample sizes for saturation in qualitative research: A systematic review of empirical tests. Soc. Sci. Med. 2022, 292, 114523. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Roderick, M.; Waddington, I.; Parker, G. PLAYING HURT: Managing Injuries in English Professional Football. Int. Rev. Sociol. Sport 2000, 35, 165–180. [Google Scholar] [CrossRef]
- Mayer, J.; Giel, K.E.; Malcolm, D.; Schneider, S.; Diehl, K.; Zipfel, S.; Thiel, A. Compete or rest? Willingness to compete hurt among adolescent elite athletes. Psychol. Sport Exerc. 2018, 35, 143–150. [Google Scholar] [CrossRef]
- Corrigan, B.; Kazlauskas, R. Medication Use in Athletes Selected for Doping Control at the Sydney Olympics (2000). Clin. J. Sport Med. 2003, 13, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Conlan, G.; McLean, B.; Kemp, J.; Duffield, R. Effect of Training/Competition Load and Scheduling on Sleep Characteristics in Professional Rugby League Athletes. J. Strength Cond. Res. 2022, 36, 3390–3397. [Google Scholar] [CrossRef] [PubMed]
- The Norwegian Prescription Database. Available online: https://www.norpd.no/ (accessed on 30 November 2023).
- Schifano, F.; Chiappini, S.; Corkery, J.M.; Guirguis, A. An Insight into Z-Drug Abuse and Dependence: An Examination of Reports to the European Medicines Agency Database of Suspected Adverse Drug Reactions. Int. J. Neuropsychopharmacol. 2019, 22, 270–277. [Google Scholar] [CrossRef]
- Patterson, L.B.; Backhouse, S.H.; Jones, B. The role of athlete support personnel in preventing doping: A qualitative study of a rugby union academy. Qual. Res. Sport Exerc. Health 2023, 15, 70–88. [Google Scholar] [CrossRef]
- Orchard, J.W. Is it Safe to Use Local Anaesthetic Painkilling Injections in Professional Football? Sports Med. 2004, 34, 209–219. [Google Scholar] [CrossRef] [PubMed]
- Orchard, J. The use of local anaesthetic injections in professional football. Br. J. Sports Med. 2001, 35, 212–213. [Google Scholar] [CrossRef]
- Mottram, D.; Chester, N.; Atkinson, G.; Goode, D. Athletes’ Knowledge and Views on OTC Medication. Int. J. Sports Med. 2008, 29, 851–855. [Google Scholar] [CrossRef]
- WADA. World Anti-Doping Code 2021; WADA: Montreal, QC, Canada, 2021. [Google Scholar]
- Dunbarap, G. Ski star Johaug banned from 2018 Olympics in doping case. AP News, 22 August 2017. [Google Scholar]
- Dikic, N.; McNamee, M.; Günter, H.; Markovic, S.S.; Vajgic, B. Sports physicians, ethics and antidoping governance: Between assistance and negligence. Br. J. Sports Med. 2013, 47, 701–704. [Google Scholar] [CrossRef]
- Hughes, D.; Vlahovich, N.; Welvaert, M.; Tee, N.; Harcourt, P.; White, S.; Vernec, A.; Fitch, K.; Waddington, G. Glucocorticoid prescribing habits of sports medicine physicians working in high-performance sport: A 30-nation survey. Br. J. Sports Med. 2020, 54, 402–407. [Google Scholar] [CrossRef]
- Mazanov, J.; Backhouse, S.; Connor, J.; Hemphill, D.; Quirk, F. Athlete support personnel and anti-doping: Knowledge, attitudes, and ethical stance. Scand. J. Med. Sci. Sports 2014, 24, 846–856. [Google Scholar] [CrossRef] [PubMed]
- Tandon, S.; Bowers, L.D.; Fedoruk, M.N. Treating the elite athlete: Anti-doping information for the health professional. Mo. Med. 2015, 112, 122–128. [Google Scholar] [PubMed]

{kind=link}
| Interview Extract | Codes | Subtheme (Main Theme) |
|---|---|---|
| Let’s say we play three matches a week, and then we have a match at 7 p.m., so then we don’t finish until 10 p.m., then we don’t get home until 11 p.m., because we have a late dinner. Then, I think there are many, or I understand why people want sleeping pills to be able to sleep. | Tight program Late-night matches Culture | Reasons for use (Use of hypnotics) |
| I think there may be a little more and closer follow-up in individual sports on a weekly basis about how you feel, so if you have minor injuries, you simply must take that into account. But I think the environment around hockey is a bit like that, that you keep going until it simply doesn’t work. | Individual versus team sports Tolerate pain and injuries | Access to prescribers (Athlete support personnel) Macho culture (Use of analgesics) |
| Pharmaceutical Group | ATC * Code | Usage Areas | Count (n) ** | % of All DCFs ** |
|---|---|---|---|---|
| Other analgesics and antipyretics | N02B | Pain relief | 39 | 22% |
| NSAIDs | M01A | Pain relief | 36 | 20% |
| Hypnotics and sedatives | N05C | Induce, extend, or improve sleep | 34 | 19% |
| Antihistamines for systemic use | R06A | Allergy | 17 | 9.6% |
| Decongestants and other nasal preparations for topical use | R01A | Cold, allergy | 17 | 9.6% |
| Total doping control forms (DCFs) with information about ≥1 medication. | 121 | 68% |
| Main Theme | Subtheme | Codes |
|---|---|---|
| Use of analgesics | Macho culture | Tolerate pain and injury Keep the place on the team It is tough to play injured |
| Removing pain before, during, and after matches | Mechanic impact injuries Injury management | |
| Seasonal-dependent use | Sacrifice your own health More use of analgesics in important parts of the season | |
| Access to analgesics | The accessibility of a physician Used in important matches | |
| Use of hypnotics | Taboo to talk about | More in other clubs More before Aware of the consequences |
| Reasons for use | Traveling Heavy training volume Tight program Late-night matches Adrenaline rush Semi-professional league Culture | |
| Performance | The importance of sleep as an athlete Afraid of too little sleep | |
| Trust in athlete support personnel (ASP) | Athlete and physician as a team | Common goal Trust between physician and athlete |
| ASP’s competence | Control of substances and products Physicians’ competence Division of responsibility | |
| Availability of prescribers | Several prescribers Individual versus team sports Semi-professional league |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Christensen, S.; Gjelstad, A.; Björnsdottir, I.; Lauritzen, F. Medicalization of Sport? A Mixed-Method Study on the Use of Medications in Elite Ice Hockey. Sports 2024, 12, 19. https://doi.org/10.3390/sports12010019
Christensen S, Gjelstad A, Björnsdottir I, Lauritzen F. Medicalization of Sport? A Mixed-Method Study on the Use of Medications in Elite Ice Hockey. Sports. 2024; 12(1):19. https://doi.org/10.3390/sports12010019
Chicago/Turabian StyleChristensen, Sofie, Astrid Gjelstad, Ingunn Björnsdottir, and Fredrik Lauritzen. 2024. "Medicalization of Sport? A Mixed-Method Study on the Use of Medications in Elite Ice Hockey" Sports 12, no. 1: 19. https://doi.org/10.3390/sports12010019
APA StyleChristensen, S., Gjelstad, A., Björnsdottir, I., & Lauritzen, F. (2024). Medicalization of Sport? A Mixed-Method Study on the Use of Medications in Elite Ice Hockey. Sports, 12(1), 19. https://doi.org/10.3390/sports12010019