
Association between Functional Movement Screen Scores and Athletic Performance in Adolescents: A Systematic Review



Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Information Sources
2.3. Search Strategy
2.4. Selection Process
2.5. Data Collection Process
2.6. Data Items
- The report: author, year;
- The study: sample size, country, study design;
- The participants: sex, age, performance status, sport;
- The results: statistical analysis, confidence intervals, effect sizes, FMS© inter-rater reliability, control for maturation.
2.7. Study Risk of Bias Assessment
2.8. Effect Measures
2.9. Synthesis Methods
3. Results
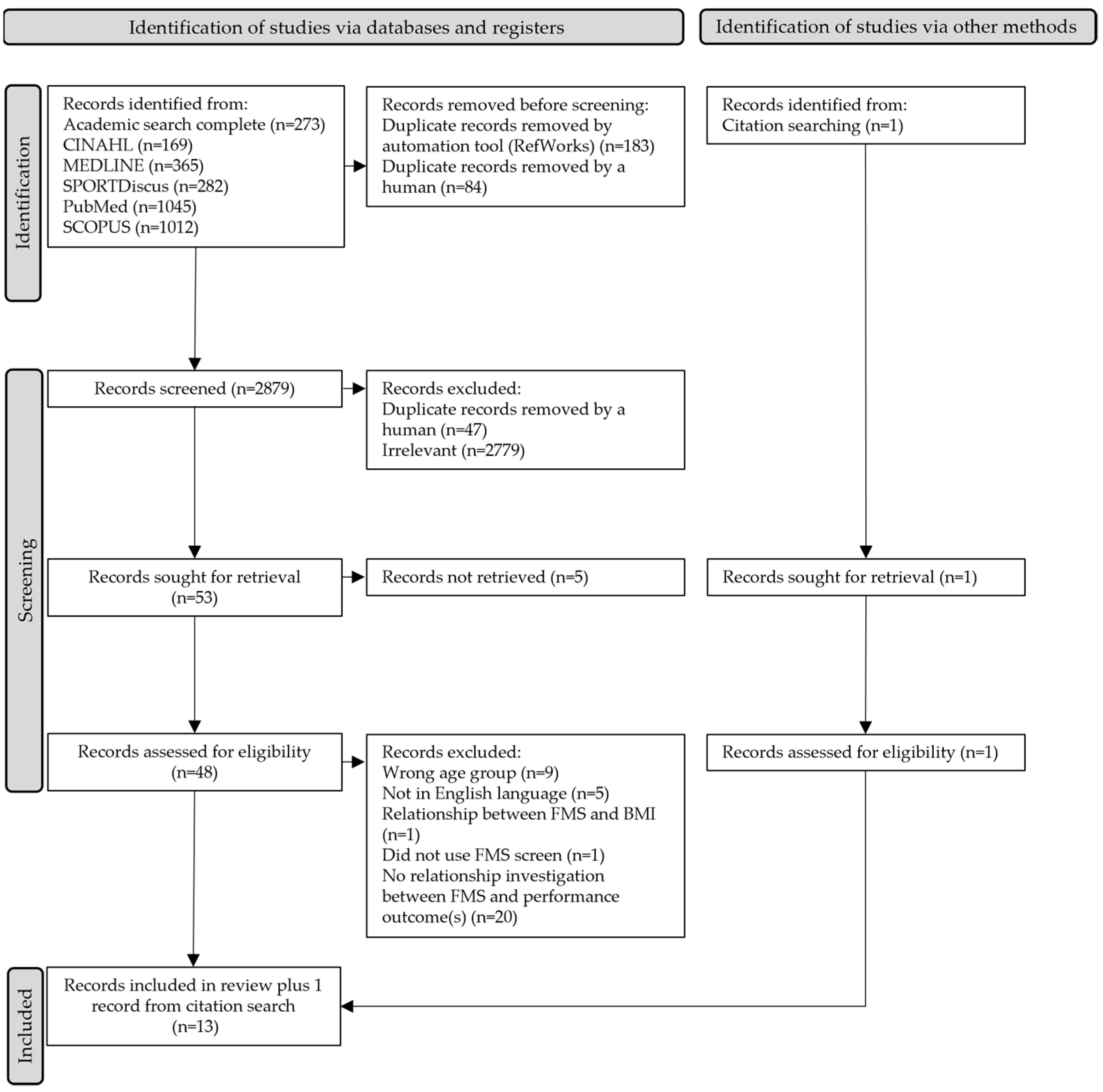
3.1. Study Selection
3.2. Study Characteristics
3.3. Risk of Bias in Studies
3.4. Results of Individual Studies
3.5. Results of Syntheses
3.5.1. Power
3.5.2. Speed
3.5.3. Agility
3.5.4. Strength
3.5.5. Balance
3.5.6. Endurance
3.5.7. Flexibility
3.5.8. Sport-Specific Skills
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Appendix A

{kind=link}
| Grouped FMS© | Individual FMS© | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Outcome by Age | Outcome by Gender | Overall Outcome | ||||||||||||
| Campa et al., 2019 [41] | Bakalľár et al., 2020 [43] | Lloyd et al., 2015 [20] | Silva et al., 2017 [42] | GÜNay et al., 2017 [46] | Kramer et al., 2019 [27] | Pfeifer et al., 2017 [49] | Bond et al., 2015 [48] | Bennett et al., 2021 [40] | Chang et al., 2020 [45] | Krkeljas et al., 2021 [44] | Smith et al., 2017 [50] | Yildiz et al., 2018 [47] | ||
| Total FMS© scores | Elite = 13.50 (2.10) Sub-elite = 12.40 (1.60) | Total | 11 = 15.70 a (1.90) 13 = 16.00 a (1.60) 15 = 17.20 a (1.20) | U11 = 12.00 (1.50) U13 = 12.50 (3.00) U16 = 16.00 (2.00) | U16 = 13.87 (2.93) U19 = 14.96 (2.07) | M = 16.13 (2.32) F = 17.71 (1.65) | M = 12.70 (2.60) F = 14.20 (2.20) | M = 12.62 (3.06) [6–18] F = 14.10 (1.88) [9–18] | 15.90 (1.40) M = 15.20 (0.26) F = 16.30 (0.22) | 13.78 (2.53) | 12.18 (2.02) | 13.50 (8.10) | 16.00 a [9–21] | 15.86 (2.06) |
| FMSmove | Elite = 5.90 (0.80) Sub-elite = 4.80 (0.90) | DS | 11 = 2 13 = 2 15 = 2 | U16 = 2.13 (0.69) U19 = 2.08 (0.40) | M = 2.47 (0.73) F = 2.59 (0.49) | M = 1.70 (0.56) [1–3] F = 1.80 (0.67) [1–3] | 1.65 (0.72) | 1.68 (0.78) | 1.96 | |||||
| HS | 11 = 2 13 = 2 15 = 2 | Right leg U16 = 1.70 (0.47) U19 = 1.84 (0.47) Left leg U16 = 1.57 (0.51) U19 = 1.84 (0.47) | M = 1.93 (0.62) F = 2.12 (0.63) | M = 1.65 (0.54) [0–3] F = 1.91 (0.42) [1–3] | 1.90 (0.52) | 2.32 (0.48) | 2.12 | |||||||
| ILL | 11 = 2 13 = 2 15 = 2 | Right leg U16 = 2.00 (0.80) U19 = 2.52 (0.71) Left leg U16 = 2.04 (0.93) U19 = 2.20 (0.87) | M = 1.93 (0.76) F = 2.12 (0.78) | M = 2.13 (0.66) [1–3] F = 2.32 (0.53) [1–3] | 2.04 (0.58) | 1.45 (0.74) | 1.84 | |||||||
| FMSflex | Elite = 4.30 (0.90) Sub-elite = 3.70 (1.40) | SM | 11 = 3 13 = 3 15 = 3 | Right U16 = 2.17 (0.89) U19 = 2.52 (0.71) Left U16 = 2.04 (0.93) U19 = 2.20 (0.87) | M = 2.36 (0.78) F = 2.61 (0.53) | M = 2.02 (1.00) [0–3] F = 2.68 (0.62) [1–3] | 2.42 (0.91) | 1.64 (1.00) | 2.88 | |||||
| ASLR | 11 = 3 13 = 2 15 = 2.50 | Right U16 = 2.57 (0.66) U19 = 2.60 (0.50) Left U16 = 2.48 (0.59) U19 = 2.60 (0.50) | M = 2.43 (0.97) F = 2.93 (0.24) | M = 1.87 (0.61) [1–3] F = 2.32 (0.75) [1–3] | 2.08 (0.77) | 1.86 (0.35) | 1.84 | |||||||
| FMSstab | Elite = 4.10 (0.10) Sub-elite = 3.80 (0.40) | TSPU | 11 = 2 13 = 3 15 = 3 | U16 = 2.04 (0.82) U19 = 2.20 (0.91) | M = 2.86 (0.35) F = 2.87 (0.66) | M = 1.60 (0.77) [0–3] F = 1.46 (0.77) [1–3] | 1.98 (1.01) | 2.32 (1.09) | 1.92 | |||||
| RS | 11 = 2 13 = 2 15 = 2 | Right U16 = 1.91 (0.42) U19 = 1.92 (0.40) Left U16 = 1.83 (0.49) U19 = 2.00 (0.00) | M = 2.13 (0.67) F = 2.42 (0.57) | M = 1.65 (0.60) [0–3] F = 1.91 (0.38) [1–3] | 1.86 (0.47) | 1.50 (0.80) | 2.00 | |||||||
Appendix B
| Lloyd et al., 2015 [20] | Kramer et al., 2019 [27] | Bennett et al., 2021 [40] | Campa et al., 2019 [41] | GÜNay et al., 2017 [46] | Yildiz et al., 2018 [47] | Bond et al., 2015 [48] | Smith et al., 2017 [50] | |
|---|---|---|---|---|---|---|---|---|
| Total FMS© | Squat jump (r = 0.66, p < 0.01) Reactive strength (r = 0.74, p < 0.01) Reactive agility (r = −0.54, p < 0.01) | M LQYBTL (r = 0.45, p < 0.01) LQYBTT (r = 0.42, p < 0.05) Agility (r = −0.47, p < 0.01) F LQYBTL (r = 0.45, p < 0.05) LQYBTT (r = 0.41, p < 0.05) | 5 m sprint (r = −0.13, p < 0.05) Agility (r = −0.13, p < 0.05) PredV02max (r = 0.22, p < 0.05) | RSAM (r = −0.68, p < 0.001) RSAB (r = −0.58, p < 0.001) | M swim 200 m time (r = 0.014, p = 0.92) F swim 200 m time (r = 0.022, p = 0.89) | Squat jump (r = 0.52, p = 0.002) Sit and reach (r = 0.74, p = 0.000) Crunch (r = 0.75, p = 0.000) Back and leg strength (r = 0.36, p = 0.04) LP-R (r = 0.55, p = 0.001) LP-L (r = 0.57, p = 0.001) Core stability (r = 0.75, p = 0.000) | 100 m freestyle swim (r = −0.333, p < 0.05) Sig. main effect for swim speed (fast v slow) (F = 8.20, p = 0.005) | BESS instrumental (r = 0.058, p = 0.737) BESS clinical (r = 0.145, p = 0.398) Y-Balance right (r = −0.085, p = 0.623) Y-Balance left (r = −0.139, p = 0.42) |
| FMSmove | RSAM (r = −0.36, p < 0.05) RSAB (r = −0.55, p < 0.001) |
Appendix C
| Lloyd et al., 2015 [20] | Kramer et al., 2019 [27] | Bennett et al., 2021 [40] | Campa et al., 2019 [41] | GÜNay et al., 2017 [46] | Yildiz et al., 2018 [47] | Bond et al., 2015 [48] | Smith et al., 2017 [50] | |
|---|---|---|---|---|---|---|---|---|
| Total FMS© | Squat jump (r = 0.66, p < 0.01) Reactive strength (r = 0.74, p < 0.01) Reactive agility (r = −0.54, p < 0.01) | M LQYBTL (r = 0.45, p < 0.01) LQYBTT (r = 0.42, p < 0.05) Agility (r = −0.47, p < 0.01) F LQYBTL (r = 0.45, p < 0.05) LQYBTT (r = 0.41, p < 0.05) | 5 m sprint (r = −0.13, p < 0.05) Agility (r = −0.13, p < 0.05) PredV02max (r = 0.22, p < 0.05) | RSAM (r = −0.68, p < 0.001) RSAB (r = −0.58, p < 0.001) | M swim 200 m time (r = 0.014, p = 0.92) F swim 200 m time (r = 0.022, p = 0.89) | Squat jump (r = 0.52, p = 0.002) Sit and reach (r = 0.74, p = 0.000) Crunch (r = 0.75, p = 0.000) Back and leg strength (r = 0.36, p = 0.04) LP-R (r = 0.55, p = 0.001) LP-L (r = 0.57, p = 0.001) Core stability (r = 0.75, p = 0.000) | 100 m freestyle swim (r = −0.333, p < 0.05) Sig. main effect for swim speed (fast v slow) (F = 8.20, p = 0.005) | BESS instrumental (r =.058, p = 0.737) BESS clinical (r = 0.145, p = 0.398) Y-Balance right (r = −0.085, p = 0.623) Y-Balance left (r = −0.139, p = 0.42) |
| FMSmove | RSAM (r = −0.36, p < 0.05) RSAB (r = −0.55, p < 0.001) |
References
- Barnett, L.M.; Webster, E.K.; Hulteen, R.M.; De Meester, A.; Valentini, N.C.; Lenoir, M.; Pesce, C.; Getchell, N.; Lopes, V.P.; Rodrigues, L.P.; et al. Through the looking glass: A systematic review of longitudinal evidence, providing new insight for motor competence and health. Sports Med. 2021, 1–46. [Google Scholar] [CrossRef]
- Cook, G.; Burton, L.; Hoogenboom, B. Pre-participation screening: The use of fundamental movements as an assessment of function—Part 1. N. Am. J. Sports Phys. Ther. 2006, 1, 62–72. [Google Scholar] [PubMed]
- Cook, G.; Burton, L.; Hoogenboom, B. Pre-participation screening: The use of fundamental movements as an assessment of function—Part 2. N. Am. J. Sports Phys. Ther. 2006, 1, 132–139. [Google Scholar] [PubMed]
- Cliff, D.P.; Okely, A.D.; Morgan, P.J.; Jones, R.A.; Steele, J.R.; Baur, L.A. Proficiency deficiency: Mastery of fundamental movement skills and skill components in overweight and obese children. Obesity 2012, 20, 1024–1033. [Google Scholar] [CrossRef]
- Duncan, M.J.; Stanley, M.; Wright, S.L. The association between functional movement and overweight and obesity in British primary school children. Sports Med. Arthrosc. Rehabil. Ther. Technol. 2013, 5, 11. [Google Scholar] [CrossRef] [Green Version]
- Barnett, L.M.; Stodden, D.; Cohen, K.E.; Smith, J.J.; Lubans, D.; Lenoir, M.; Iivonen, S.; Miller, A.D.; Laukkanen, A.; Dudley, D.; et al. Fundamental Movement Skills: An Important Focus. J. Teach. Phys. Educ. 2016, 35, 219–225. [Google Scholar] [CrossRef]
- Hulteen, R.; Morgan, P.J.; Barnett, L.M.; Stodden, D.F.; Lubans, D. Development of Foundational Movement Skills: A Conceptual Model for Physical Activity across the Lifespan. Sports Med. 2018, 48, 1533–1540. [Google Scholar] [CrossRef]
- Goodway, J.D.; Ozmun, J.C.; Gallahue, D.L. Understanding Motor Development: Infants, Children, Adolescents, Adults; Jones & Bartlett Learning: Burlington, MA, USA, 2019. [Google Scholar]
- Cook, G. Athletic Body in Balance; Human Kinetics: Champaign, IL, USA, 2003. [Google Scholar]
- Kraus, K.; Schutz, E.; Taylor, W.R.; Doyscher, R. Efficacy of the functional movement screen: A review. J. Strength Cond. Res. 2014, 28, 3571–3584. [Google Scholar] [CrossRef]
- Bonazza, N.A.; Smuin, D.; Onks, C.A.; Silvis, M.L.; Dhawan, A. Reliability, Validity, and Injury Predictive Value of the Functional Movement Screen: A Systematic Review and Meta-analysis. Am. J. Sports Med. 2017, 45, 725–732. [Google Scholar] [CrossRef]
- Monaco, J.-T.; Schoenfeld, B.J. A Review of the Current Literature on the Utility of the Functional Movement Screen as a Screening Tool to Identify Athletes’ Risk for Injury. Strength Cond. J. 2019, 41, 17–23. [Google Scholar] [CrossRef]
- Pfeifer, C.E.; Sacko, R.S.; Ortaglia, A.; Monsma, E.V.; Beattie, P.F.; Goins, J.; Stodden, D.F. Functional movement screen in youth sport participants: Evaluating the proficiency barrier for injury. Int. J. Sports Phys. Ther. 2019, 14, 436–444. [Google Scholar] [CrossRef] [PubMed]
- Kuzuhara, K.; Shibata, M.; Iguchi, J.; Uchida, R. Functional Movements in Japanese Mini-Basketball Players. J. Hum. Kinet. 2018, 61, 53–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Padua, D.A.; Marshall, S.W.; Boling, M.C.; Thigpen, C.A.; Garrett, W.E.; Beutler, A.I. The Landing Error Scoring System (LESS) is a valid and reliable clinical assessment tool of jump-landing Biomechanics the JUMP-ACL Study. Am. J. Sports Med. 2009, 37, 1996–2002. [Google Scholar] [CrossRef] [PubMed]
- Dos Santos Bunn, P.; Rodrigues, A.I.; da Silva, E.B. The association between the functional movement screen outcome and the incidence of musculoskeletal injuries: A systematic review with meta-analysis. Phys. Ther. Sport 2019, 35, 146–158. [Google Scholar] [CrossRef]
- Cook, G.; Hoogenboom, B.; Burton, L.; Plisky, P.; Rose, G. Movement: Functional Movement Systems; Lotus Publishing: Chichester, UK, 2010. [Google Scholar]
- Butler, R.J.; Plisky, P.J.; Kiesel, K.B. Interrater Reliability of Videotaped Performance on the Functional Movement Screen Using the 100-Point Scoring Scale. Athl. Train. Sports Health Care J. Pract. Clin. 2012, 4, 103–109. [Google Scholar] [CrossRef]
- Everard, E.M.; Harrison, A.J.; Lyons, M. Examining the Relationship Between the Functional Movement Screen and the Landing Error Scoring System in an Active, Male Collegiate Population. J. Strength Cond. Res. 2017, 31, 1265–1272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lloyd, R.S.; Oliver, J.L.; Radnor, J.M.; Rhodes, B.C.; Faigenbaum, A.D.; Myer, G.D. Relationships between functional movement screen scores, maturation and physical performance in young soccer players. J. Sports Sci. 2015, 33, 11–19. [Google Scholar] [CrossRef]
- Mitchell, U.H.; Johnson, A.W.; Vehrs, P.; Feland, J.; Hilton, S.C. Performance on the Functional Movement Screen in older active adults. J. Sport Health Sci. 2016, 5, 119–125. [Google Scholar] [CrossRef] [Green Version]
- Duncan, M.J.; Stanley, M. Functional Movement Is Negatively Associated with Weight Status and Positively Associated with Physical Activity in British Primary School Children. J. Obes. 2012, 2012, 697563. [Google Scholar] [CrossRef]
- Newell, K.M. What are Fundamental Motor Skills and What is Fundamental About Them? J. Mot. Learn. Dev. 2020, 8, 280. [Google Scholar] [CrossRef]
- Duncan, M.J.; Lawson, C.; Walker, L.J.; Stodden, D.; Eyre, E.L.J. The Utility of the Supine-to-Stand Test as a Measure of Functional Motor Competence in Children Aged 5–9 Years. Sports 2017, 5, 67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Brien, W.; Khodaverdi, Z.; Bolger, L.; Tarantino, G.; Philpott, C.; Neville, R.D. The Assessment of Functional Movement in Children and Adolescents: A Systematic Review and meta-analysis. Sports Med. 2021, 52, 37–53. [Google Scholar] [CrossRef] [PubMed]
- Silva, B.; Rodrigues, L.P.; Clemente, F.M.; Cancela, J.M.; Bezerra, P. Association between motor competence and Functional Movement Screen scores. PeerJ 2019, 7, e7270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Girard, J.; Quigley, M.; Helfst, F. Does the functional movement screen correlate with athletic performance? A systematic review. Phys. Ther. Rev. 2016, 21, 83–90. [Google Scholar] [CrossRef]
- Kramer, T.A.; Sacko, R.S.; Pfeifer, C.E.; Gatens, D.R.; Goins, J.M.; Stodden, D.F. The association between the Functional Movement Screen(TM), Y-balance test, and physical performance test in male and female high school athletes. Int. J. Sports Phys. Ther. 2019, 14, 911–919. [Google Scholar] [CrossRef]
- Balyi, I.; Hamilton, A. Long-term athlete development: Trainability in childhood and adolescence. Olymp. Coach 2004, 16, 4–9. [Google Scholar]
- Lloyd, R.S.; Oliver, J.L. The Youth Physical Development Model. Strength Cond. J. 2012, 34, 61–72. [Google Scholar] [CrossRef] [Green Version]
- Sheppard, J.M.; Young, W.B. Agility literature review: Classifications, training and testing. J. Sports Sci. 2006, 24, 919–932. [Google Scholar] [CrossRef] [Green Version]
- Semenick, D. Tests and measurements: The T-test. Strength Cond. J. 1990, 12, 36–37. [Google Scholar] [CrossRef]
- Isaacs, L.D. Comparison of the vertec and just jump systems for measuring height of vertical jump by young children. Percept. Mot. Ski. 1998, 86, 659–663. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Berk, L. Development through the Lifespan, 7th ed.; Pearson Education: London, UK, 2017; p. 1386. [Google Scholar]
- Chimera, N.J.; Smith, C.A.; Warren, M. Injury History, Sex, and Performance on the Functional Movement Screen and Y Balance Test. J. Athl. Train. 2015, 50, 475–485. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Downes, M.J.; Brennan, M.; Williams, H.C.; Dean, R. Development of a critical appraisal tool to assess the quality of cross-sectional studies (AXIS). BMJ Open 2016, 6, e011458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Molina-Garcia, P.; Migueles, J.H.; Cadenas-Sanchez, C.; Esteban-Cornejo, I.; Mora-Gonzalez, J.; Rodriguez-Ayllon, M.; Plaza-Florido, A.; Molina-Molina, A.; Garcia-Delgado, G.; Ortega, F.B.; et al. Fatness and fitness in relation to functional movement quality in overweight and obese children. J. Sports Sci. 2019, 37, 878–885. [Google Scholar] [CrossRef] [PubMed]
- Klusemann, M.J.; Pyne, D.; Fay, T.S.; Drinkwater, E. Online Video–Based Resistance Training Improves the Physical Capacity of Junior Basketball Athletes. J. Strength Cond. Res. 2012, 26, 2677–2684. [Google Scholar] [CrossRef]
- Bennett, H.; Fuller, J.; Milanese, S.; Jones, S.; Moore, E.; Chalmers, S. Relationship between Movement Quality and Physical Performance in Elite Adolescent Australian Football Players. J. Strength Cond. Res. 2021. Epub ahead of printing. [Google Scholar] [CrossRef]
- Campa, F.; Semprini, G.; Júdice, P.; Messina, G.; Toselli, S. Anthropometry, Physical and Movement Features, and Repeated-sprint Ability in Soccer Players. Int. J. Sports Med. 2019, 40, 100–109. [Google Scholar] [CrossRef]
- Silva, B.; Clemente, F.M.; Camões, M.; Bezerra, P. Functional Movement Screen Scores and Physical Performance among Youth Elite Soccer Players. Sports 2017, 5, 16. [Google Scholar] [CrossRef] [Green Version]
- Bakalľár, I.; Šimonek, J.; Kanásová, J.; Krčmárová, B.; Krčmár, M. Multiple athletic performances, maturation, and Functional Movement Screen total and individual scores across different age categories in young soccer players. J. Exerc. Rehabil. 2020, 16, 432. [Google Scholar] [CrossRef]
- Krkeljas, Z.; Kovac, D. Relationship between functional movement screen, athletic and karate performance in adolescents. Hum. Mov. 2021, 22, 16–21. [Google Scholar] [CrossRef]
- Chang, W.-D.; Chou, L.-W.; Chang, N.-J.; Chen, S. Comparison of Functional Movement Screen, Star Excursion Balance Test, and Physical Fitness in Junior Athletes with Different Sports Injury Risk. BioMed Res. Int. 2020, 2020, 8690540. [Google Scholar] [CrossRef] [PubMed]
- GÜNay, E.; ÜÇEr, O.; Tok, İ.; BedİZ, C.Ş. The relationship between functional movement screen and swimming performance. Sci. Mov. Health 2017, 17 (Suppl. 2), 566–570. [Google Scholar]
- Yıldız, S. Relationship Between Functional Movement Screen and Some Athletic Abilities in Karate Athletes. J. Educ. Train. Stud. 2018, 6, 66–69. [Google Scholar] [CrossRef] [Green Version]
- Bond, D.; Goodson, L.; Oxford, S.W.; Nevill, A.M.; Duncan, M.J. The Association between Anthropometric Variables, Functional Movement Screen Scores and 100 m Freestyle Swimming Performance in Youth Swimmers. Sports 2015, 3, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Pfeifer, C.E. Functional Motor Competence, Health-Related Fitness, and Injury in Youth Sport. Ph.D. Thesis, University of South Carolina, Columbia, SC, USA, 2017. [Google Scholar]
- Smith, L.J.; Creps, J.R.; Bean, R.; Rodda, B.; Alsalaheen, B. Performance of high school male athletes on the Functional Movement Screen™. Phys. Ther. Sport 2017, 27, 17–23. [Google Scholar] [CrossRef]
- Dancey, C.P.; Reidy, J. Statistics without Maths for Psychology; Pearson Education: London, UK, 2007. [Google Scholar]
- Dorrel, B.S.; Long, T.; Shaffer, S.W.; Myer, G.D. Evaluation of the Functional Movement Screen as an Injury Prediction Tool among Active Adult Populations. Sports Health 2015, 7, 532–537. [Google Scholar] [CrossRef] [Green Version]
- Kazman, J.B.; Galecki, J.M.; Lisman, P.; Deuster, P.A.; O’Connor, F.G. Factor Structure of the Functional Movement Screen in Marine Officer Candidates. J. Strength Cond. Res. 2014, 28, 672–678. [Google Scholar] [CrossRef]
- Li, Y.; Wang, X.; Chen, X.; Dai, B. Exploratory factor analysis of the functional movement screen in elite athletes. J. Sports Sci. 2015, 33, 1166–1172. [Google Scholar] [CrossRef]
- Lloyd, R.S.; Oliver, J.L.; Faigenbaum, A.D.; Myer, G.D.; De Ste Croix, M.B. Chronological age vs. biological maturation: Implications for exercise programming in youth. J. Strength Cond. Res. 2014, 28, 1454–1464. [Google Scholar] [CrossRef]
- Alemany, J.A.; Bushman, T.T.; Grier, T.; Anderson, M.; Canham-Chervak, M.; North, W.J.; Jones, B.H. Functional Movement Screen: Pain versus composite score and injury risk. J. Sci. Med. Sport 2017, 20, S40–S44. [Google Scholar] [CrossRef]
- Kiesel, K.; Plisky, P.; Butler, R. Functional movement test scores improve following a standardized off-season intervention program in professional football players. Scand. J. Med. Sci. Sports 2011, 21, 287–292. [Google Scholar] [CrossRef] [PubMed]
- Moran, R.W.; Schneiders, A.G.; Mason, J.; Sullivan, S.J. Do Functional Movement Screen (FMS) composite scores predict subsequent injury? A systematic review with meta-analysis. Br. J. Sports Med. 2017, 51, 1661–1669. [Google Scholar] [CrossRef] [PubMed]
- Hickey, J.N.; Barrett, B.A.; Butler, R.J.; Kiesel, K.B.; Plisky, P.J. Reliability of the Functional Movement Screen using a 100-point grading scale. Med. Sci. Sports Exerc. 2010, 42, 392–405. [Google Scholar] [CrossRef]
- Kiesel, K.B.; Plisky, P.J.; Voight, M.L. Can serious injury in professional football be predicted by a preseason functional movement screen? N. Am. J. Sports Phys. Ther. 2007, 2, 147–157. [Google Scholar]
| Functional Movement (from the FMS©) | Outcomes |
|---|---|
| Total | Composite scores |
| Domain-specific | FMSmove |
| FMSflex | |
| FMSstab | |
| Individual FMS movements | deep squat |
| hurdle step | |
| in-line lunge | |
| shoulder mobility | |
| active straight leg-raise | |
| trunk stability | |
| rotary stability | |
| Athletic performance | |
| jump height or distance | |
| speed | |
| strength | |
| balance | |
| agility | |
| power | |
| fitness | |
| physical performance | |
| athletic performance | |
| muscular endurance | |
| cardiovascular endurance |
| Study | n | Sex (n) | Overall Age Mean ± SD (n) | Min.–Max. Age | Status/Sport | Study Design |
|---|---|---|---|---|---|---|
| Lloyd et al., 2015 [20] | 30 | M | “Under 11”: 11.20 ± 0.50 (10) “Under 13”: 13.20 ± 0.20 (9) “Under 15”: 15.60 ± 0.70 (11) | NR | Professional football club/Soccer | Cross-sectional |
| Kramer et al., 2019 [27] | 56 | M (28) F (28) | 16.40 ± 0.10 | NR | High school students/Sport NR | Cross-sectional |
| Bennett et al., 2021 [40] | 981 | M | 17.40 ± 3.40 | 15–18 | Elite Under 18 competitors/Australian Football | Cross-sectional and longitudinal |
| Campa et al., 2019 [41] | 36 | M | 16.60 ± 50 | NR | Elite and Sub-Elite/Soccer | Observational |
| Silva et al., 2017 [42] | 48 | NR | “Under 16”: 15.78 ± 0.52 (22) “Under 19”: 17.32 ± 0.48 (26) | NR | National competitive players/Soccer | Cross-sectional |
| Bakalľár et al., 2020 [43] | 41 | M | “Under 12”: 11 (15) a “Under 14”: 13 (14) a “Under 16”: 15 (12) a | 11–15 | Local soccer academy/Soccer | Cross-sectional |
| Krkeljas et al., 2021 [44] | 20 | NR | 12.20 ± 1.90 | 10–15 | Belt colour orange to brown/Karate (7.50 ± 4.42 years’ experience) | Cross-sectional |
| Chang et al., 2020 [45] | 32 | NR | 16.06 ± 0.21 | NR | Junior athletes (school sports teams)/Volleyball (n = 11) Basketball (n = 12) Handball (n = 9) | Observational |
| GÜNay et al., 2017 [46] | 93 | M (50) F (43) | NR | NR | Olympic Swimmer Development Camp (National Federation of Swimming)/Swimming | Cross-sectional |
| Yildiz et al., 2018 [47] | 32 | M (20) F (12) | 16.06 ± 0.90 | 15–18 | Blue belt or higher/Karate | Cross-sectional |
| Bond et al., 2015 [48] | 50 | M (21) F (29) | NR | 11–16 | National Amateur Swimming Association beacon squad/Swimming | Cross-sectional |
| Pfeifer et al., 2017 [49] | 136 | M (63) F (73) | 16.01 ± 1.35 | 11–18 | Public/private high schools and local sports organisations/Football (n = 40), Soccer (M = 23, F = 39), Volleyball (F = 18), Lacrosse (F = 10), ‘Other’ (F = 6) | Cross-sectional |
| Smith et al., 2017 [50] | 94 | M | 15.50 ± 1.17 | 13–18 | High school athletes/Football (53), Baseball (1), Soccer (40) | Cross-sectional |
| Studies (Yes/No/Don’t Know/N/A) | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 20 | 27 | 40 | 41 | 42 | 43 | 44 | 45 | 46 | 47 | 48 | 49 | 50 | |
| Introduction | |||||||||||||
| Were the aims/objectives of the study clear | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Methods | |||||||||||||
| Was the study design appropriate for the stated aim(s)? | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Was the sample size justified? | N | N | N | N | N | N | N | Y | N | N | N | N | N |
| Was the target/reference population clearly defined? (Is it clear who the research was about?) | Y | Y | Y | Y | N | N | N | N | Y | N | Y | Y | Y |
| Was the sample frame taken from an appropriate population base so that it closely represented the target/reference population under investigation? | Y | Y | Y | Y | Y | DK | Y | Y | Y | DK | Y | Y | Y |
| Was the selection process likely to select subjects/participants that were representative of the target/reference population under investigation? | Y | Y | Y | Y | Y | DK | Y | Y | Y | DK | Y | Y | Y |
| Were measures undertaken to address and categorise non-responders? | N | N | N | N | N | N | N | N | N | N | N | N | N |
| Were the risk factor and outcome variables measured appropriate to the aims of the study? | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Were the risk factor and outcome variables measured correctly using instruments/measurements that had been trialled, piloted or published previously? | Y | Y | Y | Y | Y | Y | Y | Y | Y | DK | Y | Y | Y |
| Is it clear what was used to determine statistical significance and/or precision estimates? (e.g., p values, CIs) | Y | Y | Y | Y | Y | Y | Y | Y | Y | N | Y | Y | Y |
| Were the methods (including statistical methods) sufficiently described to enable them to be repeated? | Y | N | Y | Y | Y | Y | N | Y | N | N | N | Y | Y |
| Results | |||||||||||||
| Were the basic data adequately described? | Y | Y | Y | Y | Y | Y | Y | N | Y | N | Y | Y | Y |
| Does the response rate raise concerns about non-response bias? | DK | DK | DK | DK | DK | DK | DK | DK | DK | DK | DK | DK | DK |
| If appropriate, was information about non-responders described? | N | N | N | N | N | N | N | N | N | N | N | N | N |
| Were the results internally consistent? | DK | N | DK | DK | DK | Y | DK | Y | N | DK | Y | Y | N |
| Were the results for the analyses described in the methods, presented? | Y | Y | Y | Y | Y | Y | Y | Y | Y | N | Y | Y | Y |
| Discussion | |||||||||||||
| Were the authors’ discussions and conclusions justified by the results? | Y | Y | Y | Y | Y | Y | N | Y | Y | Y | Y | Y | Y |
| Were the limitations of the study discussed? | Y | N | Y | N | Y | Y | N | Y | N | N | Y | Y | Y |
| Other | |||||||||||||
| Were there any funding sources or conflicts of interest that may affect the authors’ interpretation of the results? | N | DK | DK | N | N | N | DK | N | DK | DK | N | DK | N |
| Was ethical approval or consent of participants attained? | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fitton Davies, K.; Sacko, R.S.; Lyons, M.A.; Duncan, M.J. Association between Functional Movement Screen Scores and Athletic Performance in Adolescents: A Systematic Review. Sports 2022, 10, 28. https://doi.org/10.3390/sports10030028
Fitton Davies K, Sacko RS, Lyons MA, Duncan MJ. Association between Functional Movement Screen Scores and Athletic Performance in Adolescents: A Systematic Review. Sports. 2022; 10(3):28. https://doi.org/10.3390/sports10030028
Chicago/Turabian StyleFitton Davies, Katie, Ryan S. Sacko, Mark A. Lyons, and Michael J. Duncan. 2022. "Association between Functional Movement Screen Scores and Athletic Performance in Adolescents: A Systematic Review" Sports 10, no. 3: 28. https://doi.org/10.3390/sports10030028
APA StyleFitton Davies, K., Sacko, R. S., Lyons, M. A., & Duncan, M. J. (2022). Association between Functional Movement Screen Scores and Athletic Performance in Adolescents: A Systematic Review. Sports, 10(3), 28. https://doi.org/10.3390/sports10030028