


Health-Related Physical Fitness in Adolescents from Spain, Estonia and Iceland: A Cross-Sectional, Quantitative Study
 , ,
, ,  ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Measures
2.3. Statistical Analysis
3. Results
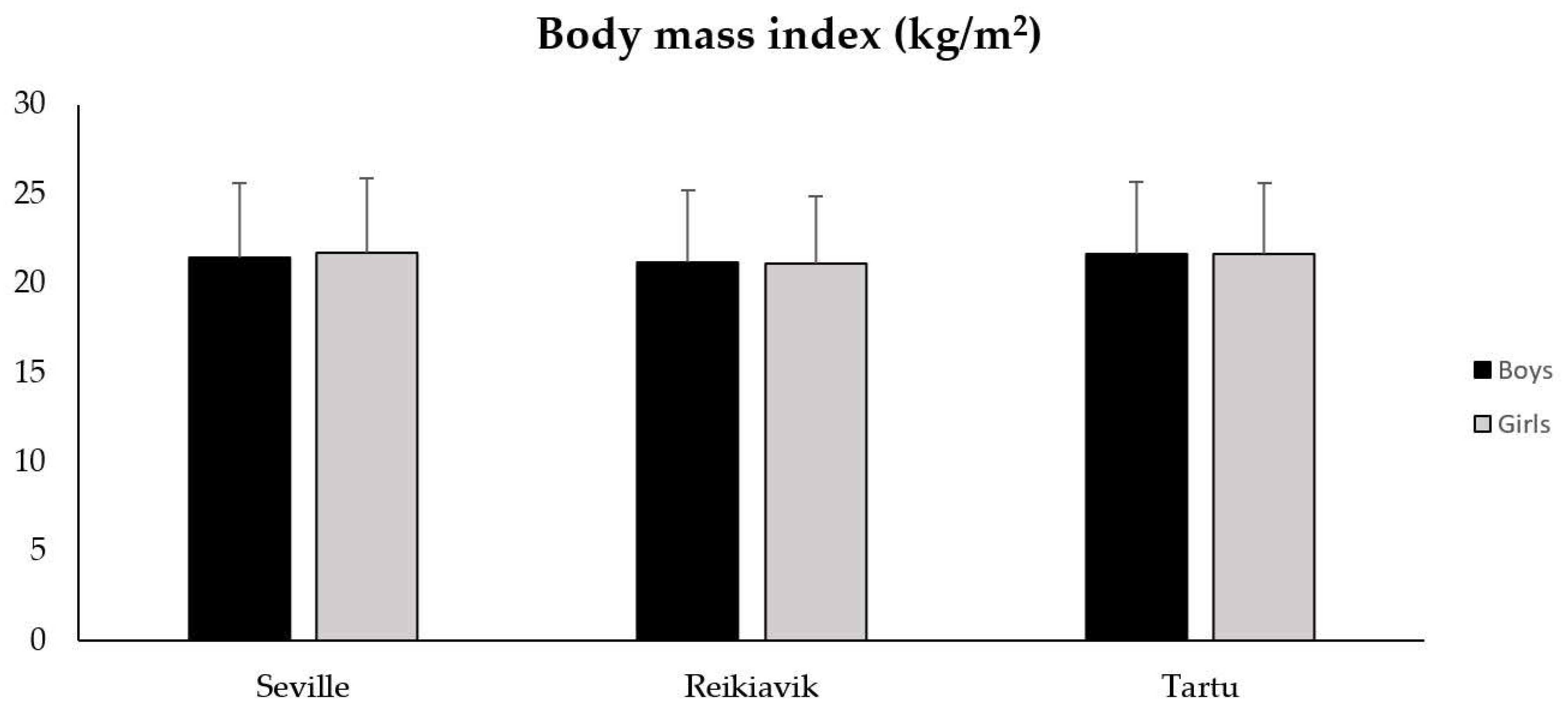
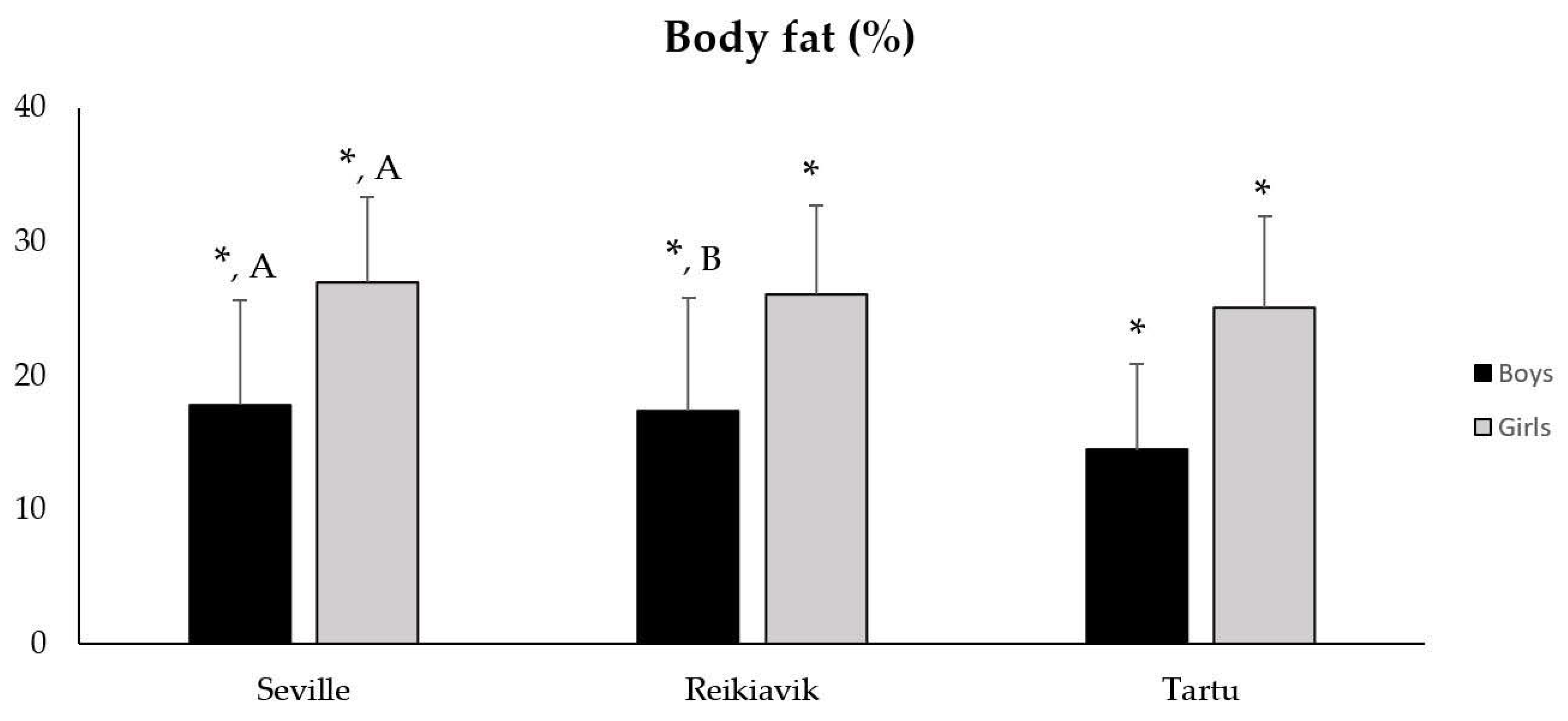
3.1. Body Composition According to City and Gender
3.2. PF According to City and Gender
4. Discussion
4.1. Body Composition According to City and Gender
4.2. PF According to City and Gender
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Myers, J.; Kokkinos, P.; Nyelin, E. Physical Activity, Cardiorespiratory Fitness, and the Metabolic Syndrome. Nutrients 2019, 11, 1652. [Google Scholar] [CrossRef] [PubMed]
- Bell, S.L.; Audrey, S.; Gunnell, D.; Cooper, A.; Campbell, R. The Relationship between Physical Activity, Mental Wellbeing and Symptoms of Mental Health Disorder in Adolescents: A Cohort Study. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 138. [Google Scholar] [CrossRef] [PubMed]
- Carson, V.; Lee, E.Y.; Hewitt, L.; Jennings, C.; Hunter, S.; Kuzik, N.; Stearns, J.A.; Unrau, S.P.; Poitras, V.J.; Gray, C.; et al. Systematic Review of the Relationships between Physical Activity and Health Indicators in the Early Years (0–4 Years). BMC Public Health 2017, 17, 33–63. [Google Scholar] [CrossRef]
- Bedard, C.; Hanna, S.; Cairney, J. A Longitudinal Study of Sport Participation and Perceived Social Competence in Youth. J. Adolesc. Health 2020, 66, 352–359. [Google Scholar] [CrossRef]
- Ortega, F.B.; Ruiz, J.R.; Castillo, M.J. Actividad Física, Condición Física y Sobrepeso En Niños y Adolescentes: Evidencia Procedente de Estudios Epidemiológicos. Endocrinol. y Nutr. 2013, 60, 458–469. [Google Scholar] [CrossRef] [PubMed]
- Sawyer, S.M.; Afifi, R.A.; Bearinger, L.H.; Blakemore, S.J.; Dick, B.; Ezeh, A.C.; Patton, G.C. Adolescence: A Foundation for Future Health. Lancet 2012, 379, 1630–1640. [Google Scholar] [CrossRef]
- Myers, J.; Prakash, M.; Froelicher, V.; Do, D.; Partington, S.; Edwin Atwood, J. Exercise Capacity and Mortality among Men Referred for Exercise Testing. N. Engl. J. Med. 2002, 346, 793–801. [Google Scholar] [CrossRef]
- Ortega, F.B.; Ruiz, J.R.; Castillo, M.J.; Sjöström, M. Physical Fitness in Childhood and Adolescence: A Powerful Marker of Health. Int. J. Obes. 2008, 32, 1–11. [Google Scholar] [CrossRef]
- Lang, J.J.; Tremblay, M.S.; Léger, L.; Olds, T.; Tomkinson, G.R. International Variability in 20 m Shuttle Run Performance in Children and Youth: Who Are the Fittest from a 50-Country Comparison? A Systematic Literature Review with Pooling of Aggregate Results. Br. J. Sports Med. 2018, 52, 276. [Google Scholar] [CrossRef]
- Galan-Lopez, P.; Sánchez-Oliver, A.J.; Ries, F.; González-Jurado, J.A. Mediterranean diet, physical fitness and body composition in sevillian adolescents: A healthy lifestyle. Nutrients. 2019, 11, 2009. [Google Scholar] [CrossRef]
- Mendoza-Muñoz, M.; Adsuar, J.C.; Pérez-Gómez, J.; Muñoz-Bermejo, L.; Garcia-Gordillo, M.Á.; Carlos-Vivas, J. Influence of Body Composition on Physical Fitness in Adolescents. Med. 2020, 56, 328. [Google Scholar] [CrossRef] [PubMed]
- Gralla, M.H.; McDonald, S.M.; Breneman, C.; Beets, M.W.; Moore, J.B. Associations of Objectively Measured Vigorous Physical Activity With Body Composition, Cardiorespiratory Fitness, and Cardiometabolic Health in Youth: A Review. Am. J. Lifestyle Med. 2019, 13, 61–97. [Google Scholar] [CrossRef] [PubMed]
- Thomas, D.M.; Bredlau, C.; Bosy-Westphal, A.; Mueller, M.; Shen, W.; Gallagher, D.; Maeda, Y.; McDougall, A.; Peterson, C.M.; Ravussin, E.; et al. Relationships between Body Roundness with Body Fat and Visceral Adipose Tissue Emerging from a New Geometrical Model. Obesity 2013, 21, 2264–2271. [Google Scholar] [CrossRef] [PubMed]
- Suárez-Carmona, W.; Sánchez-Oliver, A.J.; González-Jurado, J.A. Fisiopatología de La Obesidad: Perspectiva Actual. Rev. Chil. Nutr. 2017, 44, 226–233. [Google Scholar] [CrossRef]
- Piché, M.E.; Poirier, P.; Lemieux, I.; Després, J.P. Overview of Epidemiology and Contribution of Obesity and Body Fat Distribution to Cardiovascular Disease: An Update. Prog. Cardiovasc. Dis. 2018, 61, 103–113. [Google Scholar] [CrossRef]
- Galan-Lopez, P.; Lopez-Cobo, I.; García-Lázaro, I.; Ries, F. Associations between Motives for Physical Exercise, Body Composition and Cardiorespiratory Fitness: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 14128. [Google Scholar] [CrossRef]
- Abdelkarim, O.; Ammar, A.; Trabelsi, K.; Cthourou, H.; Jekauc, D.; Irandoust, K.; Taheri, M.; Bös, K.; Woll, A.; Bragazzi, N.L.; et al. Prevalence of Underweight and Overweight and Its Association with Physical Fitness in Egyptian Schoolchildren. Int. J. Environ. Res. Public Health 2019, 17, 75. [Google Scholar] [CrossRef]
- Ruiz, J.R.; Ortega, F.B.; Gutierrez, A.; Meusel, D.; Sjöström, M.; Castillo, M.J. Health-Related Fitness Assessment in Childhood and Adolescence: A European Approach Based on the AVENA, EYHS and HELENA Studies. J. Public Health 2006, 14, 269–277. [Google Scholar] [CrossRef]
- Arnaoutis, G.; Georgoulis, M.; Psarra, G.; Milkonidou, A.; Panagiotakos, D.B.; Kyriakou, D.; Bellou, E.; Tambalis, K.D.; Sidossis, L.S. Association of Anthropometric and Lifestyle Parameters with Fitness Levels in Greek Schoolchildren: Results from the EYZHN Program. Front. Nutr. 2018, 5, 10. [Google Scholar] [CrossRef] [PubMed]
- Ortega, F.B.; Ruiz, J.R. Fitness in Youth: Methodological Issues and Understanding of Its Clinical Value. Am. J. Lifestyle Med. 2015, 9, 403–408. [Google Scholar] [CrossRef]
- Ruiz, J.R.; Castro-Piñero, J.; España-Romero, V.; Artero, E.G.; Ortega, F.B.; Cuenca, M.A.M.; Enez-Pavón, D.J.; Chillón, P.; Girela-Rejón, M.J.; Mora, J.; et al. Field-Based Fitness Assessment in Young People: The ALPHA Health-Related Fitness Test Battery for Children and Adolescents. Br. J. Sports Med. 2011, 45, 518–524. [Google Scholar] [CrossRef] [PubMed]
- Power, M.L.; Schulkin, J. Sex Differences in Fat Storage, Fat Metabolism, and the Health Risks from Obesity: Possible Evolutionary Origins. Br. J. Nutr. 2008, 99, 931–940. [Google Scholar] [CrossRef] [PubMed]
- Richardson, J.T.E. Eta Squared and Partial Eta Squared as Measures of Effect Size in Educational Research. Educ. Res. Rev. 2011, 6, 135–147. [Google Scholar] [CrossRef]
- Gómez-Martnez, S.; Martnez-Gómez, D.; Perez De Heredia, F.; Romeo, J.; Cuenca-Garcia, M.; Martn-Matillas, M.; Castillo, M.; Rey-López, J.P.; Vicente-Rodriguez, G.; Moreno, L.; et al. Eating Habits and Total and Abdominal Fat in Spanish Adolescents: Influence of Physical Activity. the AVENA Study. J. Adolesc. Health 2012, 50, 403–409. [Google Scholar] [CrossRef] [PubMed]
- Jiménez-Pavón, D.; Castillo, M.J.; Moreno, L.A.; Kafatos, A.; Manios, Y.; Kondaki, K.; Béghin, L.; Zaccaria, M.; De Henauw, S.; Widhalm, K.; et al. Fitness and Fatness Are Independently Associated with Markers of Insulin Resistance in European Adolescents; The HELENA Study. Int. J. Pediatr. Obes. 2011, 6, 253–260. [Google Scholar] [CrossRef]
- Bentham, J.; Di Cesare, M.; Bilano, V.; Bixby, H.; Zhou, B.; Stevens, G.A.; Riley, L.M.; Taddei, C.; Hajifathalian, K.; Lu, Y.; et al. Worldwide Trends in Body-Mass Index, Underweight, Overweight, and Obesity from 1975 to 2016: A Pooled Analysis of 2416 Population-Based Measurement Studies in 128·9 Million Children, Adolescents, and Adults. Lancet 2017, 390, 2627–2642. [Google Scholar] [CrossRef]
- Suárez, W.; Sánchez, J. Índice De Masa Corporal: Ventajas Y Desventajas De Su Uso En La Obesidad. Nutr. Clínica en Med. 2018, 12, 128–139. [Google Scholar] [CrossRef]
- Ross, R.; Neeland, I.J.; Yamashita, S.; Shai, I.; Seidell, J.; Magni, P.; Santos, R.D.; Arsenault, B.; Cuevas, A.; Hu, F.B.; et al. Waist Circumference as a Vital Sign in Clinical Practice: A Consensus Statement from the IAS and ICCR Working Group on Visceral Obesity. Nat. Rev. Endocrinol. 2020, 16, 177–189. [Google Scholar] [CrossRef]
- Pearson, N.; Haycraft, E.; Johnston, J.P.; Atkin, A.J. Sedentary Behaviour across the Primary-Secondary School Transition: A Systematic Review. Prev. Med. (Baltim) 2017, 94, 40–47. [Google Scholar] [CrossRef]
- Barker, A.R.; Gracia-Marco, L.; Ruiz, J.R.; Castillo, M.J.; Aparicio-Ugarriza, R.; González-Gross, M.; Kafatos, A.; Androutsos, O.; Polito, A.; Molnar, D.; et al. Physical Activity, Sedentary Time, TV Viewing, Physical Fitness and Cardiovascular Disease Risk in Adolescents: The HELENA Study. Int. J. Cardiol. 2018, 254, 303–309. [Google Scholar] [CrossRef]
- Moreno, C.; Ramos, P.; Rivera, F.; Jiménez-Iglesias, A.; García-Moya, I.; Moreno-Maldonado, C.; Paniagua, C.; Villafuerte-Díaz, A.; Ciria-Barreiro, E.; Morgan, A.; et al. La Adolescencia En España: Salud, Bienestar, Familia, Vida Académica y Social Resultados Del Estudio HBSC 2018; Ministerio de Sanidad, Consumo y Bienestar Social: Madrid, Spain, 2018. [Google Scholar]
- De Moraes, A.C.F.; Vilanova-Campelo, R.C.; Torres-Leal, F.L.; Carvalho, H.B. Is Self-Reported Physical Fitness Useful for Estimating Fitness Levels in Children and Adolescents? A Reliability and Validity Study. Medicina 2019, 55, 286. [Google Scholar] [CrossRef] [PubMed]
- Tomkinson, G.R.; Carver, K.D.; Atkinson, F.; Daniell, N.D.; Lewis, L.K.; Fitzgerald, J.S.; Lang, J.J.; Ortega, F.B. European Normative Values for Physical Fitness in Children and Adolescents Aged 9-17 Years: Results from 2 779 165 Eurofit Performances Representing 30 Countries. Br. J. Sports Med. 2018, 52, 1445–1456. [Google Scholar] [CrossRef]
- Faigenbaum, A.D.; Rebullido, T.R.; MacDonald, J.P. Pediatric Inactivity Triad: A Risky PIT. Curr. Sports Med. Rep. 2018, 17, 45–47. [Google Scholar] [CrossRef] [PubMed]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Global Trends in Insufficient Physical Activity among Adolescents: A Pooled Analysis of 298 Population-Based Surveys with 1·6 Million Participants. Lancet Child Adolesc. Health 2020, 4, 23–35. [Google Scholar] [CrossRef]
- Lenhart, C.M.; Hanlon, A.; Kang, Y.; Daly, B.P.; Brown, M.D.; Patterson, F. Gender Disparity in Structured Physical Activity and Overall Activity Level in Adolescence: Evaluation of Youth Risk Behavior Surveillance Data. ISRN Public Health 2012, 2012, 674936. [Google Scholar] [CrossRef]
- Tremblay, M.S.; Barnes, J.D.; González, S.A.; Katzmarzyk, P.T.; Onywera, V.O.; Reilly, J.J.; Tomkinson, G.R.; Aguilar-Farias, N.; Akinroye, K.K.; Al-Kuwari, M.G.; et al. Global Matrix 2.0: Report Card Grades on the Physical Activity of Children and Youth Comparing 38 Countries. J. Phys. Act. Health 2016, 13, S343–S366. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Pastor, T.; Salinero, J.J.; Sanz-Frias, D.; Pertusa, G.; Del Coso, J. Body Fat Percentage Is More Associated with Low Physical Fitness than with Sedentarism and Diet in Male and Female Adolescents. Physiol. Behav. 2016, 165, 166–172. [Google Scholar] [CrossRef]
- Albaladejo-Saura, M.; Vaquero-Cristóbal, R.; González-Gálvez, N.; Esparza-Ros, F. Relationship between Biological Maturation, Physical Fitness, and Kinanthropometric Variables of Young Athletes: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 328. [Google Scholar] [CrossRef]
- Hrafnkelsdottir, S.M.; Brychta, R.J.; Rognvaldsdottir, V.; Gestsdottir, S.; Chen, K.Y.; Johannsson, E.; Guðmundsdottir, S.L.; Arngrimsson, S.A. Less Screen Time and More Frequent Vigorous Physical Activity Is Associated with Lower Risk of Reporting Negative Mental Health Symptoms among Icelandic Adolescents. PLoS ONE 2018, 13, e0196286. [Google Scholar] [CrossRef]
- Warburton, D.E.R.; Bredin, S.S.D. Health Benefits of Physical Activity: A Systematic Review of Current Systematic Reviews. Curr. Opin. Cardiol. 2017, 32, 541–556. [Google Scholar] [CrossRef]
- Joensuu, L.; Syväoja, H.; Kallio, J.; Kulmala, J.; Kujala, U.M.; Tammelin, T.H. Objectively Measured Physical Activity, Body Composition and Physical Fitness: Cross-Sectional Associations in 9- to 15-Year-Old Children. Eur. J. Sport Sci. 2018, 18, 882–892. [Google Scholar] [CrossRef] [PubMed]
- Dooley, F.L.; Kaster, T.; Fitzgerald, J.S.; Walch, T.J.; Annandale, M.; Ferrar, K.; Lang, J.J.; Smith, J.J.; Tomkinson, G.R. A Systematic Analysis of Temporal Trends in the Handgrip Strength of 2,216,320 Children and Adolescents Between 1967 and 2017. Sport. Med. 2020, 50, 1129–1144. [Google Scholar] [CrossRef] [PubMed]
- Gísladóttir, T.L.; Matthíasdóttir, Á.; Kristjánsdóttir, H. The Effect of Adolescents’ Sports Clubs Participation on Self-Reported Mental and Physical Conditions and Future Expectations. J. Sports Sci. 2013, 31, 1139–1145. [Google Scholar] [CrossRef] [PubMed]
- Tahira, S. The Association Between Sports Participation and Physical Fitness. Int. J. Sport Stud. Health 2022, 4, e127001. [Google Scholar] [CrossRef]
- Cooper, D.M.; Leu, S.Y.; Taylor-Lucas, C.; Lu, K.; Galassetti, P.; Radom-Aizik, S. Cardiopulmonary Exercise Testing in Children and Adolescents with High Body Mass Index. Pediatr. Exerc. Sci. 2016, 28, 98–108. [Google Scholar] [CrossRef]
- Sayar, I.; Desbiens, J.-F.; Marzougui, M.; Ben Abderrahman, A. Impacts of Teachers Pedagogical Approach on the Inclusion of Adolescents with Exceed Weight into Physical Education and Sports in Emirate of Ajman/United Arab Emirates. Ann. Appl. Sport Sci. 2022, 10, 1–7. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| City | Gender | 13 Years | 14 Years | 15 Years | 16 Years |
|---|---|---|---|---|---|
| Seville (n = 917) | Boys | 113 | 131 | 115 | 99 |
| Girls | 109 | 134 | 121 | 95 | |
| Reikiavik (n = 387) | Boys | 42 | 51 | 47 | 69 |
| Girls | 42 | 43 | 43 | 50 | |
| Tartu (n = 413) | Boys | 50 | 62 | 48 | 73 |
| Girls | 29 | 42 | 53 | 56 | |
| Total (n = 1717) | Boys | 205 | 244 | 210 | 241 |
| Girls | 180 | 219 | 217 | 201 |
| Variable | Gender | Seville (n = 917) | Reykjavík (n = 387) | Tartu (n = 413) | p-Value City | p-Value Gender | p-Value City·Gender |
|---|---|---|---|---|---|---|---|
| Height (m) | Boys | 1.65 ± 0.11 * | 1.67 ± 0.11 * | 1.74 ± 0.09 * | <0.001 | <0.001 | 0.068 |
| Girls | 1.58 ± 0.07 * | 1.61 ±0.08 * | 1.66 ± 0.07 * | ||||
| Weight (kg) | Boys | 59.03 ± 0.62 *, A | 59.20 ± 0.92 *, B | 66.20 ± 0.87 * | <0.001 | <0.001 | 0.272 |
| Girls | 54.72 ± 0.62 *, A | 55.10 ± 1.00 *, B | 59.52 ± 0.99 * | ||||
| Waist Perimeter (cm) | Boys | 74.37 ± 0.45 *, A | 73.94 ± 0.67 *, B | 77.82 ± 0.63 * | <0.001 | <0.001 | 0.189 |
| Girls | 69.68 ± 0.50 * | 69.93 ± 0.72 * | 71.43 ± 0.72 * |
| Variable | Gender | Seville (n = 917) | Reykjavík (n = 387) | Tartu (n = 413) | p-Value City | p-Value Gender | p-Value City·Gender |
|---|---|---|---|---|---|---|---|
| Handgrip Strength (kg) | Boys | 27.07 ± 7.23 * A | 28.18 ± 7.90 * B | 32.87 ± 8.19 * | <0.001 | <0.001 | 0.017 |
| Girls | 21.72 ± 3.94 * A, C | 23.33 ± 4.58 * B | 25.67 ± 5.02 * | ||||
| Jump (m) | Boys | 1.66 ± 0.32 * A, C | 1.83 ± 0.29 * B | 1.92 ± 0.31 * | <0.001 | <0.001 | 0.001 |
| Girls | 1.32 ± 0.25 * A, C | 1.59 ± 0.26 * B | 1.69 ± 0.24 * | ||||
| Speed (s) | Boys | 11.91 ± 1.39 * B | 11.53 ± 1.59 * | 11.68 ± 1.44 * | <0.001 | <0.001 | <0.001 |
| Girls | 13.20 ± 1.34 * A, C | 12.12 ± 1.05 * | 12.18 ± 1.08 * | ||||
| Endurance (stages) | Boys | 6.09 ± 2.37 * A, C | 7.52 ± 2.62 *, B | 6.72 ± 2.46 * | <0.001 | <0.001 | 0.043 |
| Girls | 4.22 ± 1.40 * A, C | 5.80 ± 2.04 * | 5.48 ± 1.73 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Galan-Lopez, P.; Gísladóttir, T.; Pihu, M.; Sánchez-Oliver, A.J.; Ries, F.; Domínguez, R. Health-Related Physical Fitness in Adolescents from Spain, Estonia and Iceland: A Cross-Sectional, Quantitative Study. Sports 2022, 10, 188. https://doi.org/10.3390/sports10120188
Galan-Lopez P, Gísladóttir T, Pihu M, Sánchez-Oliver AJ, Ries F, Domínguez R. Health-Related Physical Fitness in Adolescents from Spain, Estonia and Iceland: A Cross-Sectional, Quantitative Study. Sports. 2022; 10(12):188. https://doi.org/10.3390/sports10120188
Chicago/Turabian StyleGalan-Lopez, Pablo, Thordis Gísladóttir, Maret Pihu, Antonio J. Sánchez-Oliver, Francis Ries, and Raúl Domínguez. 2022. "Health-Related Physical Fitness in Adolescents from Spain, Estonia and Iceland: A Cross-Sectional, Quantitative Study" Sports 10, no. 12: 188. https://doi.org/10.3390/sports10120188
APA StyleGalan-Lopez, P., Gísladóttir, T., Pihu, M., Sánchez-Oliver, A. J., Ries, F., & Domínguez, R. (2022). Health-Related Physical Fitness in Adolescents from Spain, Estonia and Iceland: A Cross-Sectional, Quantitative Study. Sports, 10(12), 188. https://doi.org/10.3390/sports10120188