
Temporary Mechanical Support in Cardiogenic Shock Secondary to Heart Failure: An Evolving Paradigm



Abstract
1. Introduction
2. Materials and Methods
3. Results
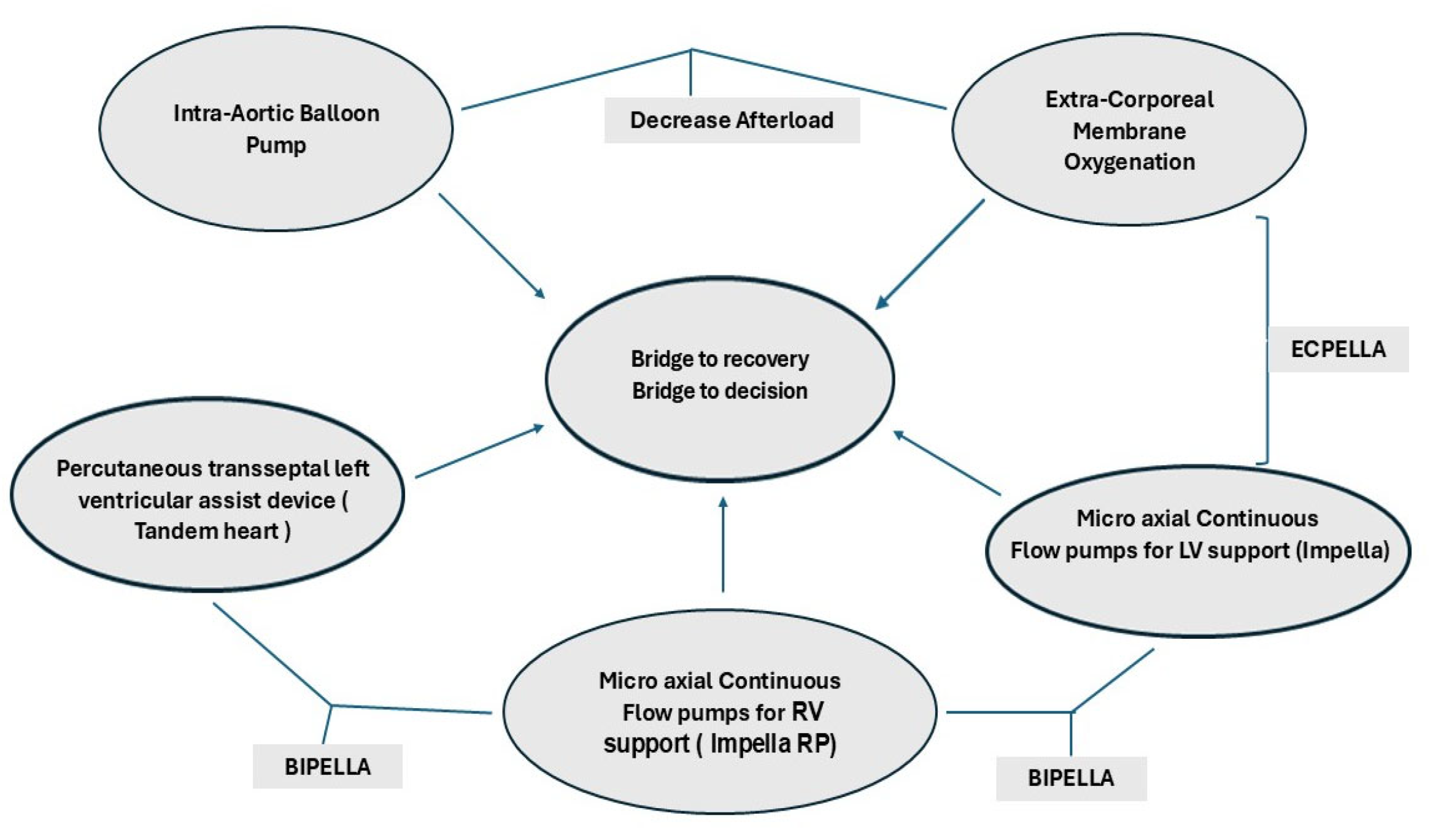
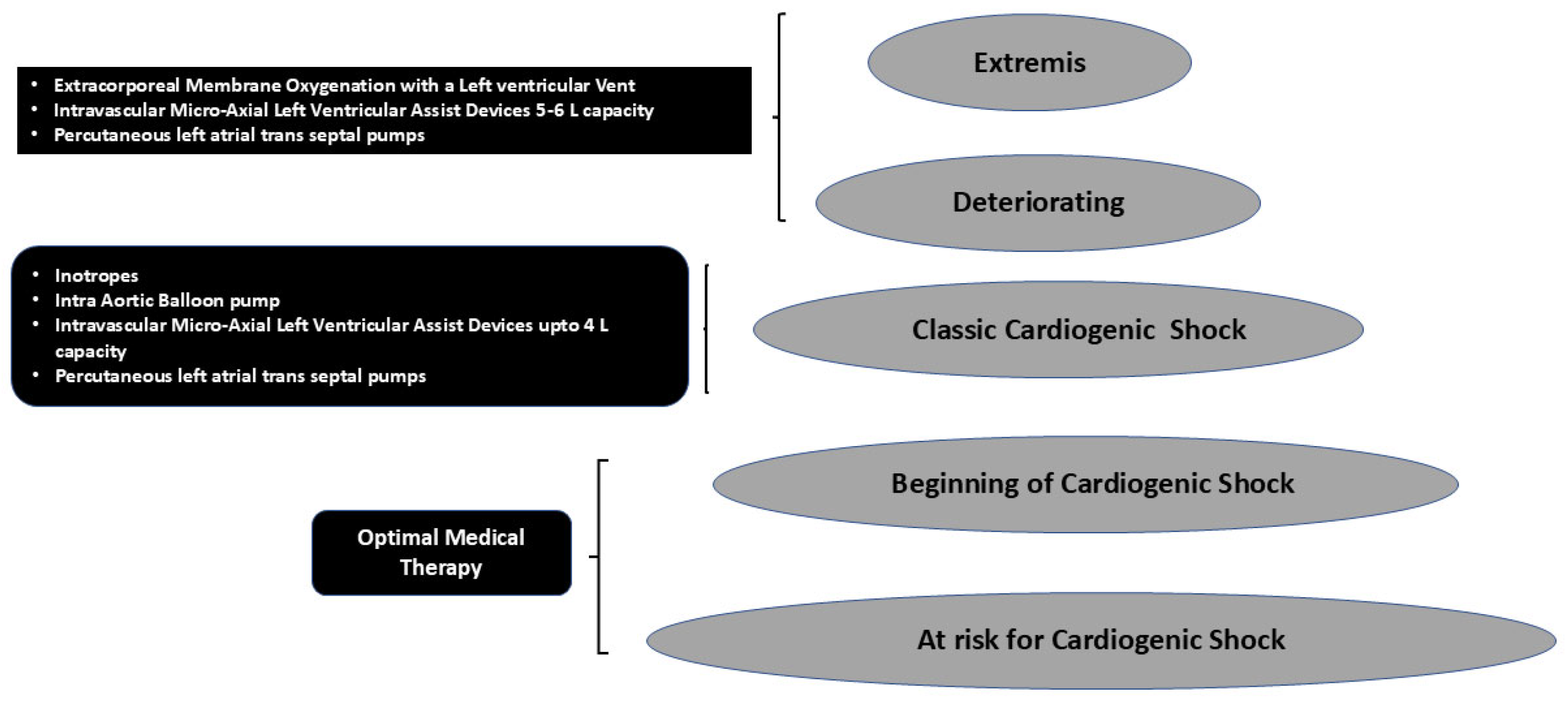
3.1. MCS Use in Different Stages of Cardiogenic Shock
3.2. Differences in Outcomes in Cardiogenic Shock Patients with HF
3.3. Gender Differences in Survival and Outcomes
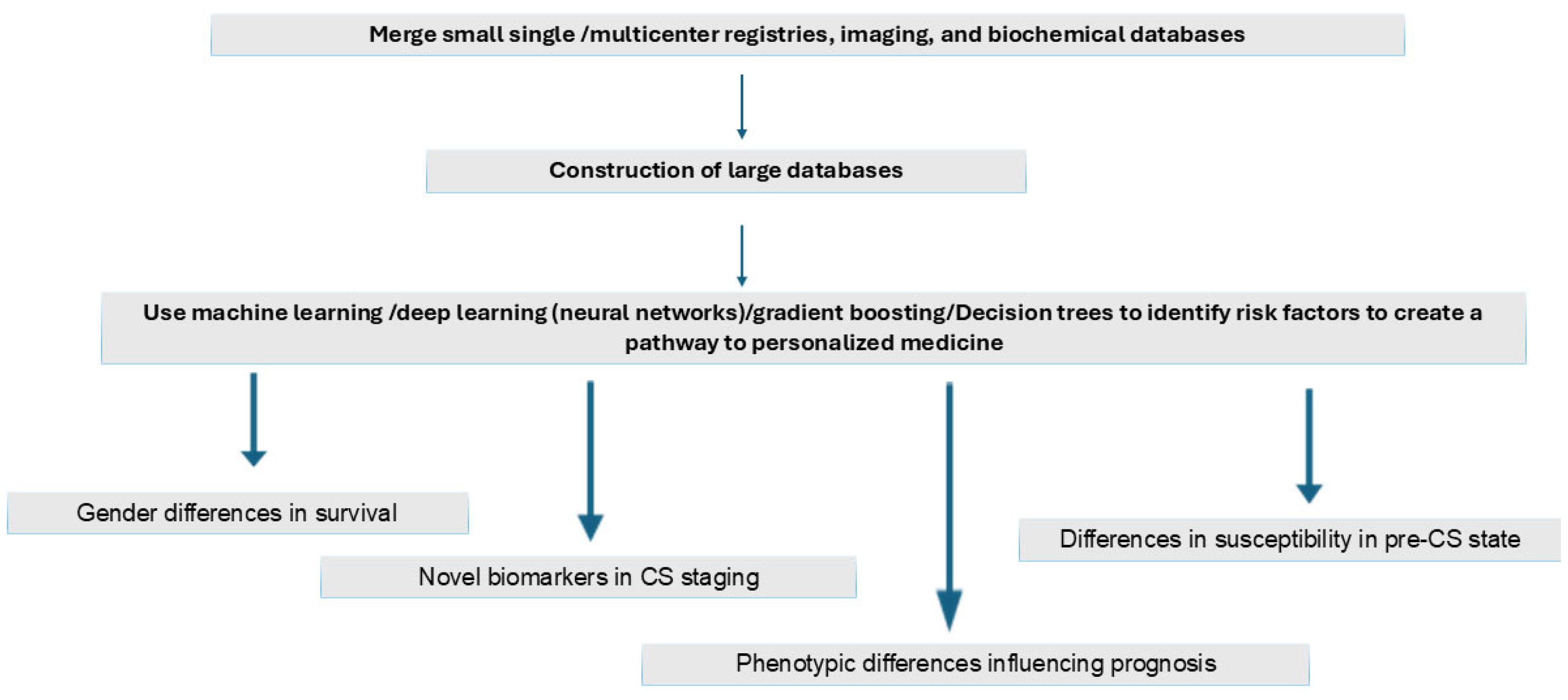
3.4. Use of AI-Driven Technologies to Identify Risk Factors
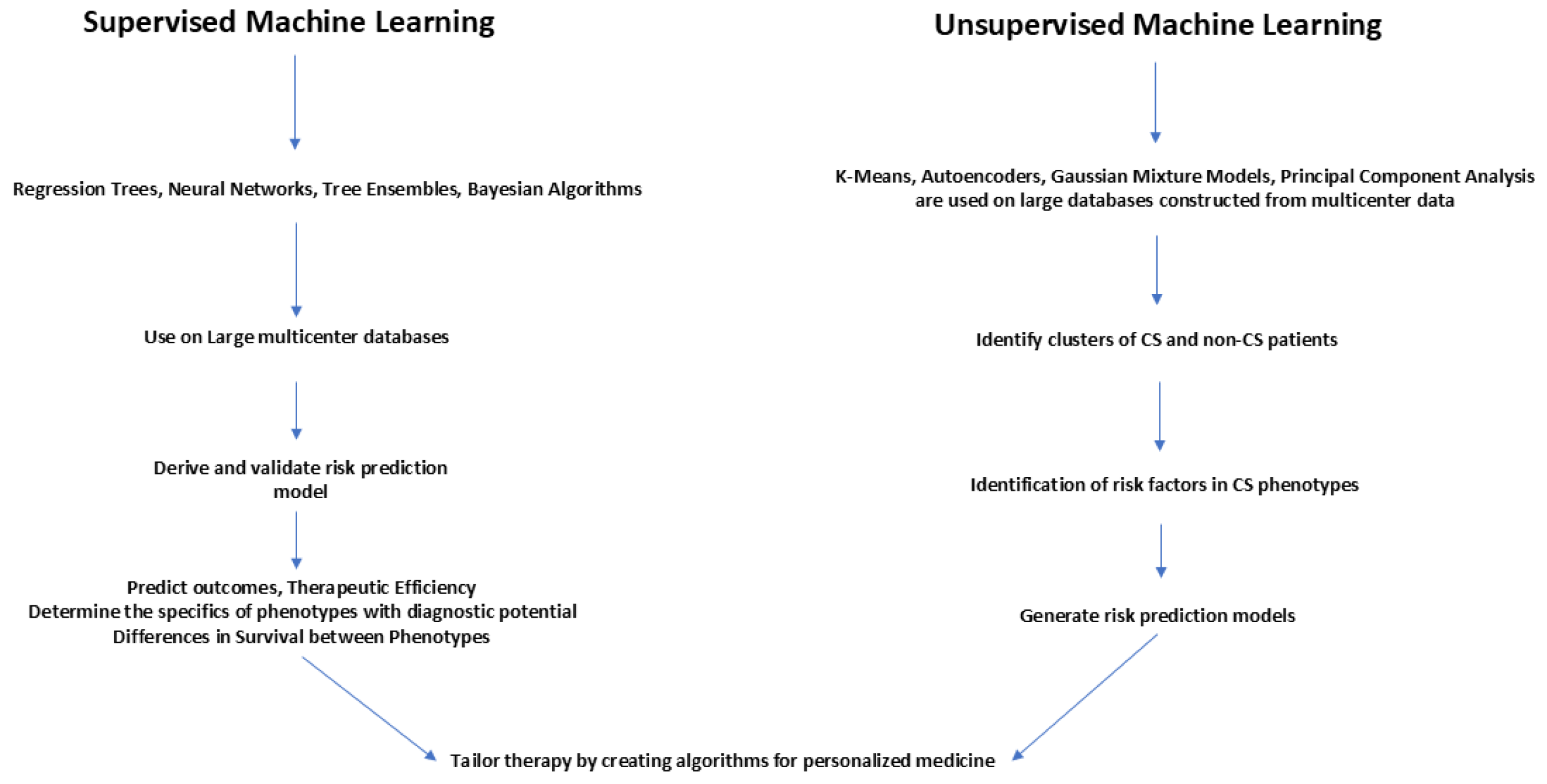
3.5. AI-Driven Strategies to Improve Outcomes in Cardiogenic Shock Secondary to Heart Failure
3.6. Use of Machine Learning in Improving the Management of CS Phenotypes
3.7. Gaps in Knowledge
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CS | Cardiogenic shock |
| ACS | Acute coronary syndrome |
| tMCS | Temporary mechanical circulatory support |
| MCS | Mechanical circulatory support |
References
- Bertaina, M.; Morici, N.; Frea, S.; Garatti, L.; Briani, M.; Sorini, C.; Villanova, L.; Corrada, E.; Sacco, A.; Moltrasio, M.; et al. Differences between cardiogenic shock related to acute decompensated heart failure and acute myocardial infarction. ESC Heart Fail. 2023, 10, 3472–3482. [Google Scholar] [CrossRef] [PubMed]
- Vlachakis, P.K.; Theofilis, P.; Leontsinis, I.; Drakopoulou, M.; Karakasis, P.; Oikonomou, E.; Chrysohoou, C.; Tsioufis, K.; Tousoulis, D. Bridge to Life: Current Landscape of Temporary Mechanical Circulatory Support in Heart-Failure-Related Cardiogenic Shock. J. Clin. Med. 2024, 13, 4120. [Google Scholar] [CrossRef] [PubMed]
- Geller, B.J.; Sinha, S.S.; Kapur, N.K.; Bakitas, M.; Balsam, L.B.; Chikwe, J.; Klein, D.G.; Kochar, A.; Masri, S.C.; Sims, D.B.; et al. Escalating and De-escalating Temporary Mechanical Circulatory Support in Cardiogenic Shock: A Scientific Statement From the American Heart Association. Circulation 2022, 146, E50–E68. [Google Scholar] [CrossRef]
- van Diepen, S.; Katz, J.N.; Albert, N.M.; Henry, T.D.; Jacobs, A.K.; Kapur, N.K.; Kilic, A.; Menon, V.; Ohman, E.M.; Sweitzer, N.K.; et al. Contemporary Management of Cardiogenic Shock: A Scientific Statement From the American Heart Association. Circulation 2017, 136, E232–E268. [Google Scholar] [CrossRef]
- Rihal, C.S.; Naidu, S.S.; Givertz, M.M.; Szeto, W.Y.; Burke, J.A.; Kapur, N.K.; Kern, M.; Garratt, K.N.; Goldstein, J.A.; Dimas, V.; et al. 2015 SCAI/ACC/HFSA/STS Clinical Expert Consensus Statement on the Use of Percutaneous Mechanical Circulatory Support Devices in Cardiovascular Care: Endorsed by the American Heart Assocation, the Cardiological Society of India, and Sociedad Latino Americana de Cardiologia Intervencion; Affirmation of Value by the Canadian Association of Interventional Cardiology-Association Canadienne de Cardiologie d’intervention. J. Am. Coll. Cardiol. 2015, 65, e7–e26. [Google Scholar] [CrossRef]
- Tehrani, B.N.; Truesdell, A.G.; Psotka, M.A.; Rosner, C.; Singh, R.; Sinha, S.S.; Damluji, A.A.; Batchelor, W.B. A Standardized and Comprehensive Approach to the Management of Cardiogenic Shock. JACC Heart Fail. 2020, 8, 879–891. [Google Scholar] [CrossRef]
- Kapur, N.K.; Esposito, M.L.; Bader, Y.; Morine, K.J.; Kiernan, M.S.; Pham, D.T.; Burkhoff, D. Mechanical Circulatory Support Devices for Acute Right Ventricular Failure. Circulation 2017, 136, 314–326. [Google Scholar] [CrossRef]
- Henry, T.D.; Tomey, M.I.; Tamis-Holland, J.E.; Thiele, H.; Rao, S.V.; Menon, V.; Klein, D.G.; Naka, Y.; Piña, I.L.; Kapur, N.K.; et al. Invasive Management of Acute Myocardial Infarction Complicated by Cardiogenic Shock: A Scientific Statement From the American Heart Association. Circulation 2021, 143, e815–e829. [Google Scholar] [CrossRef]
- Lim, H.S.; Howell, N. Cardiogenic Shock Due to End-Stage Heart Failure and Acute Myocardial Infarction: Characteristics and Outcome of Temporary Mechanical Circulatory Support. Shock 2018, 50, 167–172. [Google Scholar] [CrossRef]
- Jones, T.L.; Tan, M.C.; Nguyen, V.; Kearney, K.E.; Maynard, C.C.; Anderson, E.; Mahr, C.; McCabe, J.M. Outcome differences in acute vs. acute on chronic heart failure and cardiogenic shock. ESC Heart Fail. 2020, 7, 1118–1124. [Google Scholar] [CrossRef]
- George, T.J.; Sheasby, J.; DiMaio, J.M.; Kabra, N.; Rawitscher, D.A.; Afzal, A. Outcomes of surgical Impella placement in acute cardiogenic shock. Bayl. Univ. Med. Cent. Proc. 2023, 36, 415–421. [Google Scholar] [CrossRef] [PubMed]
- Hong, Y.; Agrawal, N.; Hess, N.R.; Ziegler, L.A.; Sicke, M.M.; Hickey, G.W.; Ramanan, R.; Fowler, J.A.; Chu, D.; Yoon, P.D.; et al. Outcomes of Impella 5.0 and 5.5 for cardiogenic shock: A single-center 137 patient experience. Artif. Organs 2024, 48, 771–780. [Google Scholar] [CrossRef] [PubMed]
- Balder, J.-W.; Szymanski, M.K.; van Laake, L.W.; van der Harst, P.; Meuwese, C.L.; Ramjankhan, F.Z.; van der Meer, M.G.; Hermens, J.A.J.M.; Voskuil, M.; de Waal, E.E.C.; et al. ECPELLA as a bridge-to-decision in refractory cardiogenic shock: A single-centre experience. Neth. Heart J. 2024, 32, 245–253. [Google Scholar] [CrossRef] [PubMed]
- Mahesh, B.; Peddaayyavarla, P.; Nguyen, K.; Mahesh, A.; Hartford, C.C.; Devich, R.; Dafflisio, G.; Nair, N.; Freundt, M.; Dowling, R.; et al. Use of Intravascular Micro-Axial Left Ventricular Assist Devices as a Bridging Strategy for Cardiogenic Shock: Mid-Term Outcomes. J. Clin. Med. 2024, 13, 6804. [Google Scholar] [CrossRef]
- Ton, V.-K.; Kanwar, M.K.; Li, B.; Blumer, V.; Li, S.; Zweck, E.; Sinha, S.S.; Farr, M.; Hall, S.; Kataria, R.; et al. Impact of Female Sex on Cardiogenic Shock Outcomes: A Cardiogenic Shock Working Group Report. JACC Heart Fail. 2023, 11, 1742–1753. [Google Scholar] [CrossRef]
- Sambola, A.; Elola, F.J.; Buera, I.; Fernández, C.; Bernal, J.L.; Ariza, A.; Brindis, R.; Bueno, H.; Rodríguez-Padial, L.; Marín, F.; et al. Sex bias in admission to tertiary-care centres for acute myocardial infarction and cardiogenic shock. Eur. J. Clin. Investig. 2021, 51, e13526. [Google Scholar] [CrossRef]
- Vallabhajosyula, S.; Ya’qoub, L.; Singh, M.; Bell, M.R.; Gulati, R.; Cheungpasitporn, W.; Sundaragiri, P.R.; Miller, V.M.; Jaffe, A.S.; Gersh, B.J.; et al. Sex Disparities in the Management and Outcomes of Cardiogenic Shock Complicating Acute Myocardial Infarction in the Young. Circ. Heart Fail. 2020, 13, e007154. [Google Scholar] [CrossRef]
- Collado-Lledó, E.; Llaó, I.; Rivas-Lasarte, M.; González-Fernández, V.; Noriega, F.J.; Hernández-Perez, F.J.; Alegre, O.; Sionis, A.; Lidón, R.M.; Viana-Tejedor, A.; et al. Clinical picture, management and risk stratification in patients with cardiogenic shock: Does gender matter? BMC Cardiovasc. Disord. 2020, 20, 189. [Google Scholar] [CrossRef]
- Rubini Gimenez, M.; Zeymer, U.; Desch, S.; de Waha-Thiele, S.; Ouarrak, T.; Poess, J.; Meyer-Saraei, R.; Schneider, S.; Fuernau, G.; Stepinska, J.; et al. Sex-specific management in patients with acute myocardial infarction and cardiogenic shock: A substudy of the CULPRIT-SHOCK trial. Circ. Cardiovasc. Interv. 2020, 13, e008537. [Google Scholar] [CrossRef]
- Epps, K.C.; Tehrani, B.N.; Rosner, C.; Bagchi, P.; Cotugno, A.; Damluji, A.A.; deFilippi, C.; Desai, S.; Ibrahim, N.; Psotka, M.; et al. Sex-related differences in patient characteristics, hemodynamics, and outcomes of cardiogenic shock: INOVA-SHOCK registry. J. Soc. Cardiovasc. Angiogr. Interv. 2023, 2, 100978. [Google Scholar] [CrossRef]
- Yan, I.; Schrage, B.; Weimann, J.; Dabboura, S.; Hilal, R.; Beer, B.N.; Becher, P.M.; Seiffert, M.; Magnussen, C.; Schnabel, R.B.; et al. Sex differences in patients with cardiogenic shock. ESC Heart Fail. 2021, 8, 1775–1783. [Google Scholar] [CrossRef] [PubMed]
- Lozano-Jiménez, S.; Iranzo-Valero, R.; Segovia-Cubero, J.; Gómez-Bueno, M.; Rivas-Lasarte, M.; Mitroi, C.; Escudier-Villa, J.M.; Oteo-Dominguez, J.F.; Vieitez-Florez, J.M.; Villar-García, S.; et al. Gender differences in cardiogenic shock patients: Clinical features, risk prediction, and outcomes in a hub center. Front. Cardiovasc. Med. 2022, 9, 912802. [Google Scholar] [CrossRef] [PubMed]
- Thayer, K.L.; Zweck, E.; Ayouty, M.; Garan, A.R.; Hernandez-Montfort, J.; Mahr, C.; Morine, K.J.; Newman, S.; Jorde, L.; Haywood, J.L.; et al. Invasive hemodynamic assessment and classification of in-hospital mortality risk among patients with cardiogenic shock. Circ. Heart Fail. 2020, 13, e007099. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, A.S.; Berg, D.D.; Bohula, E.A.; Alviar, C.L.; Baird-Zars, V.M.; Barnett, C.F.; Burke, J.A.; Carnicelli, A.P.; Chaudhry, S.-P.; Daniels, L.B.; et al. De novo vs. acute-on-chronic presentations of heart failure-related cardiogenic shock: Insights from the critical care cardiology trials network registry. J. Card. Fail. 2021, 27, 1073–1081. [Google Scholar] [CrossRef]
- Abraham, J.; Blumer, V.; Burkhoff, D.; Pahuja, M.; Sinha, S.S.; Rosner, C.; Vorovich, E.; Grafton, G.; Bagnola, A.; Hernandez-Montfort, J.A.; et al. Heart failure-related cardiogenic shock: Pathophysiology, evaluation and management consid-erations: Review of heart failure-related cardiogenic shock. J. Card. Fail. 2021, 27, 1126–1140. [Google Scholar] [CrossRef]
- Chacko, Y.; Parikh, R.V.; Tremmel, J.A. Vascular access-related complications in women: Temporal trends, emerging data, and the current state of interventional cardiology practice. Curr. Atheroscler. Rep. 2018, 20, 41. [Google Scholar] [CrossRef]
- Alasnag, M.; Truesdell, A.G.; Williams, H.; Martinez, S.C.; Qadri, S.K.; Skendelas, J.P.; Jakobleff, W.A.; Alasnag, M. Mechanical circulatory support: A comprehensive review with a focus on women. Curr. Atheroscler. Rep. 2020, 22, 11. [Google Scholar] [CrossRef]
- Pahuja, M.; Ranka, S.; Chehab, O.; Mishra, T.; Akintoye, E.; Adegbala, O.; Yassin, A.S.; Ando, T.; Thayer, K.L.; Shah, P.; et al. Incidence and clinical outcomes of bleeding complications and acute limb ischemia in STEMI and cardiogenic shock. Catheter. Cardiovasc. Interv. 2021, 97, 1129–1138. [Google Scholar] [CrossRef]
- Patel, N.; Sharma, A.; Dalia, T.; Rali, A.; Earnest, M.; Tadros, P.; Wiley, M.; Hockstad, E.; Mehta, A.; Thors, A.; et al. Vascular complications associated with percutaneous left ventricular assist device placement: A 10-year US perspective. Catheter. Cardiovasc. Interv. 2020, 95, 309–316. [Google Scholar] [CrossRef]
- Joseph, S.M.; Brisco, M.A.; Colvin, M.; Grady, K.L.; Walsh, M.N.; Cook, J.L.; for the genVAD Working Group. Women with cardiogenic shock derive greater benefit from early mechanical circulatory support: An update from the cVAD registry. J. Interv. Cardiol. 2016, 29, 248–256. [Google Scholar] [CrossRef]
- Tran, K.; Dorsey, C.; Lee, J.T.; Chandra, V. Gender-related differences in iliofemoral arterial anatomy among abdominal aortic aneurysm patients. Ann. Vasc. Surg. 2017, 44, 171–178. [Google Scholar] [CrossRef] [PubMed]
- Fisher, T.; Hill, N.; Kalakoutas, A.; Lahlou, A.; Rathod, K.; Proudfoot, A.; Warren, A. Sex differences in treatments and outcomes of patients with cardiogenic shock: A systematic review and epidemiological meta-analysis. Crit. Care 2024, 28, 192. [Google Scholar] [CrossRef] [PubMed]
- Auffret, V.; Cottin, Y.; Leurent, G.; Gilard, M.; Beer, J.-C.; Zabalawi, A.; Chagué, F.; Filippi, E.; Brunet, D.; Hacot, J.-P.; et al. Predicting the development of in-hospital cardiogenic shock in patients with ST-segment elevation myocardial infarction treated by primary percutaneous coronary intervention: The ORBI risk score. Eur. Heart J. 2018, 39, 2090–2102. [Google Scholar] [CrossRef]
- Hasdai, D.; Califf, R.M.; Thompson, T.D.; Hochman, J.S.; Ohman, E.; Pfisterer, M.; Bates, E.R.; Vahanian, A.; Armstrong, P.W.; Criger, D.A.; et al. Predictors of cardiogenic shock after thrombolytic therapy for acute myocardial infarction. J. Am. Coll. Cardiol. 2000, 35, 136–143. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, R.J.; Makam, R.C.P.; Yarzebski, J.; McManus, D.D.; Lessard, D.; Gore, J.M. Decade-long trends (2001–2011) in the incidence and hospital death rates associated with the in-hospital development of cardiogenic shock after acute myocardial infarction. Circ. Cardiovasc. Qual. Outcomes 2016, 9, 117–125. [Google Scholar] [CrossRef]
- Pöss, J.; Köster, J.; Fuernau, G.; Eitel, I.; de Waha, S.; Ouarrak, T.; Lassus, J.; Harjola, V.-P.; Zeymer, U.; Thiele, H.; et al. Risk stratification for patients in cardiogenic shock after acute myocardial infarction. J. Am. Coll. Cardiol. 2017, 69, 1913–1920. [Google Scholar] [CrossRef]
- Obling, L.; Frydland, M.; Hansen, R.; Møller-Helgestad, O.K.; Lindholm, M.G.; Holmvang, L.; Ravn, H.B.; Wiberg, S.; Thomsen, J.H.; Jensen, L.O.; et al. Risk factors of late cardiogenic shock and mortality in ST-segment elevation myocardial infarction patients. Eur. Heart J. Acute Cardiovasc. Care 2018, 7, 7–15. [Google Scholar] [CrossRef]
- Schrage, B.; Weimann, J.; Dabboura, S.; Yan, I.; Hilal, R.; Becher, P.M.; Seiffert, M.; Bernhardt, A.M.; Kluge, S.; Reichenspurner, H.; et al. Patient characteristics, treatment and outcome in non-ischemic vs. ischemic cardiogenic shock. J. Clin. Med. 2020, 9, 931. [Google Scholar] [CrossRef]
- Goldstein, B.A.; Navar, A.M.; Carter, R.E. Moving beyond regression techniques in cardiovascular risk prediction: Applying machine learning to address analytic challenges. Eur. Heart J. 2017, 38, 1805–1814. [Google Scholar] [CrossRef]
- Zweck, E.; Thayer, K.L.; Helgestad, O.K.L.; Kanwar, M.; Ayouty, M.; Garan, A.R.; Hernandez-Montfort, J.; Mahr, C.; Wencker, D.; Sinha, S.S.; et al. Phenotyping cardiogenic shock. J. Am. Heart Assoc. 2021, 10, e020085. [Google Scholar] [CrossRef]
- Bai, Z.; Hu, S.; Wang, Y.; Deng, W.; Gu, N.; Zhao, R.; Zhang, W.; Ma, Y.; Wang, Z.; Liu, Z.; et al. Development of a machine learning model to predict the risk of late cardiogenic shock in patients with ST-segment elevation myocardial infarction. Ann. Transl. Med. 2021, 9, 1162. [Google Scholar] [CrossRef] [PubMed]
- Rahman, F.; Finkelstein, N.; Alyakin, A.; Gilotra, N.A.; Trost, J.; Schulman, S.P.; Saria, S. Using machine learning for early prediction of cardiogenic shock in patients with acute heart failure. J. Soc. Cardiovasc. Angiogr. Interv. 2022, 1, 100308. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.; Antonescu, C.; Ravindranath, S.; Dong, J.; Lu, M.; Vicario, F.; Wondrely, L.; Thompson, P.; Swearingen, D.; Acharya, D. Early Prediction of Cardiogenic Shock Using Machine Learning. Front. Cardiovasc. Med. 2022, 9, 862424. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Zhang, Y.; Yao, R.; Chen, K.; Xu, Q.; Huang, R.; Mao, Z.; Yu, Y. Identification of distinct clinical phenotypes of cardiogenic shock using machine learning consensus clustering approach. BMC Cardiovasc. Disord. 2023, 23, 426. [Google Scholar] [CrossRef]
- Zweck, E.; Li, S.; Burkhoff, D.; Kapur, N.K. Profiling of Cardiogenic Shock: Incorporating Machine Learning Into Bedside Management. J. Soc. Cardiovasc. Angiogr. Interv. 2024, 4, 102047. [Google Scholar] [CrossRef]
- Sinha, S.S.; Morrow, D.A.; Kapur, N.K.; Kataria, R.; Roswell, R.O. 2025 Concise Clinical Guidance: An ACC Expert Consensus Statement on the Evaluation and Management of Cardiogenic Shock: A Report of the American College of Cardiology Solution Set Oversight Committee. J. Am. Coll. Cardiol. 2025, 85, 1618–1641. [Google Scholar] [CrossRef]
- Darlington, A.M.; Lipps, K.M.; Hibbert, B.; Dunlay, S.M.; Dahiya, G.; Jentzer, J.C. Sex-Based Survival Outcomes in Cardiogenic Shock. J. Card. Fail. 2024, 30, 1211–1219. [Google Scholar] [CrossRef]
- Randhawa, V.K.; Baran, D.A.; Kanwar, M.K.; Hernandez-Montfort, J.A.; Sinha, S.S.; Barnett, C.F.; Billia, F. The Comparative Epidemiology, Pathophysiology and Management of Cardiogenic Shock Associated With Acute Myocardial Infarction and Advanced Heart Failure. Can. J. Cardiol. 2025, 41, 573–586. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Study Type/Device Used | Number of Subjects N | End Point | Conclusions |
|---|---|---|---|---|
| George et al., 2023 [11] | Retrospective single-center using Impella 5.0/5.5 | N = 90 | 1-year survival | No change in survival Improved end-organ perfusion Decreased need for vasoactive substances |
| Hong et al., 2024 [12] | Retrospective single-center using Impella 5.0/5.5 | Total N = 137 AMI = 47 HF = 86 Post cardiotomy = 4 | Survival to discharge | Survival to discharge was better in patients with CS secondary to HF |
| Balder et al., 2024 [13] | Retrospective study using ECPELLA | N = 20 | 30-day mortality | 20% mortality at 30 days; 30% cardiac recovery |
| Mahesh et al., 2024 [14] | Impella 5.0/5.5 single-center observational study | N = 107 | 4.5 years | Actuarial survival was 91% in bridge to transplant (n = 34), 79% in BT LVAD (n = 25) and 63% in the post-cardiotomy group (n = 42) |
| Study | Study Type/Device Used | Number of Subjects N | End Point | Conclusions |
|---|---|---|---|---|
| Ton et al., 2023 [15] | Retrospective | 5083 | Survival at discharge | Women with CS secondary to HF had worse outcomes and more vascular complications than their male counterparts |
| Epps et al., 2023 [20] | Retrospective | 520 (151 females and 369 males) | In-hospital mortality | No difference in women with cardiogenic shock secondary to HF versus those secondary to AMI as compared to their male counterparts |
| Fisher et al., 2024 [32] | Meta-analysis | 656,754 females; 1,018,036 males | Combined in-hospital/30-day mortality | After adjusting for confounders, mortality for cardiogenic shock in females is 10% higher than for their male counterparts. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nair, N.; Du, D.; Mahesh, B. Temporary Mechanical Support in Cardiogenic Shock Secondary to Heart Failure: An Evolving Paradigm. J. Pers. Med. 2025, 15, 184. https://doi.org/10.3390/jpm15050184
Nair N, Du D, Mahesh B. Temporary Mechanical Support in Cardiogenic Shock Secondary to Heart Failure: An Evolving Paradigm. Journal of Personalized Medicine. 2025; 15(5):184. https://doi.org/10.3390/jpm15050184
Chicago/Turabian StyleNair, Nandini, Dongping Du, and Balakrishnan Mahesh. 2025. "Temporary Mechanical Support in Cardiogenic Shock Secondary to Heart Failure: An Evolving Paradigm" Journal of Personalized Medicine 15, no. 5: 184. https://doi.org/10.3390/jpm15050184
APA StyleNair, N., Du, D., & Mahesh, B. (2025). Temporary Mechanical Support in Cardiogenic Shock Secondary to Heart Failure: An Evolving Paradigm. Journal of Personalized Medicine, 15(5), 184. https://doi.org/10.3390/jpm15050184