
COVID-19 Pandemic Impacts on STRESS, PTSD, and Prefrontal Cortical Thickness in Pre-Pandemic Trauma Survivors


Abstract
1. Introduction
2. Materials and Methods
2.1. Participants and Processing
2.2. Pandemic Stress Assessment
2.3. PTSD Symptom Assessment and PTSD Diagnosis
2.4. Structural MRI Acquisition, Processing, and Cortical Thickness Measures
2.5. Statistics/Analysis
2.5.1. PTSD vs. Non-PTSD Group Comparison Analyses
2.5.2. Correlation Analyses
2.5.3. Repeated Measures ANCOVA Analysis
3. Results
3.1. Demographics
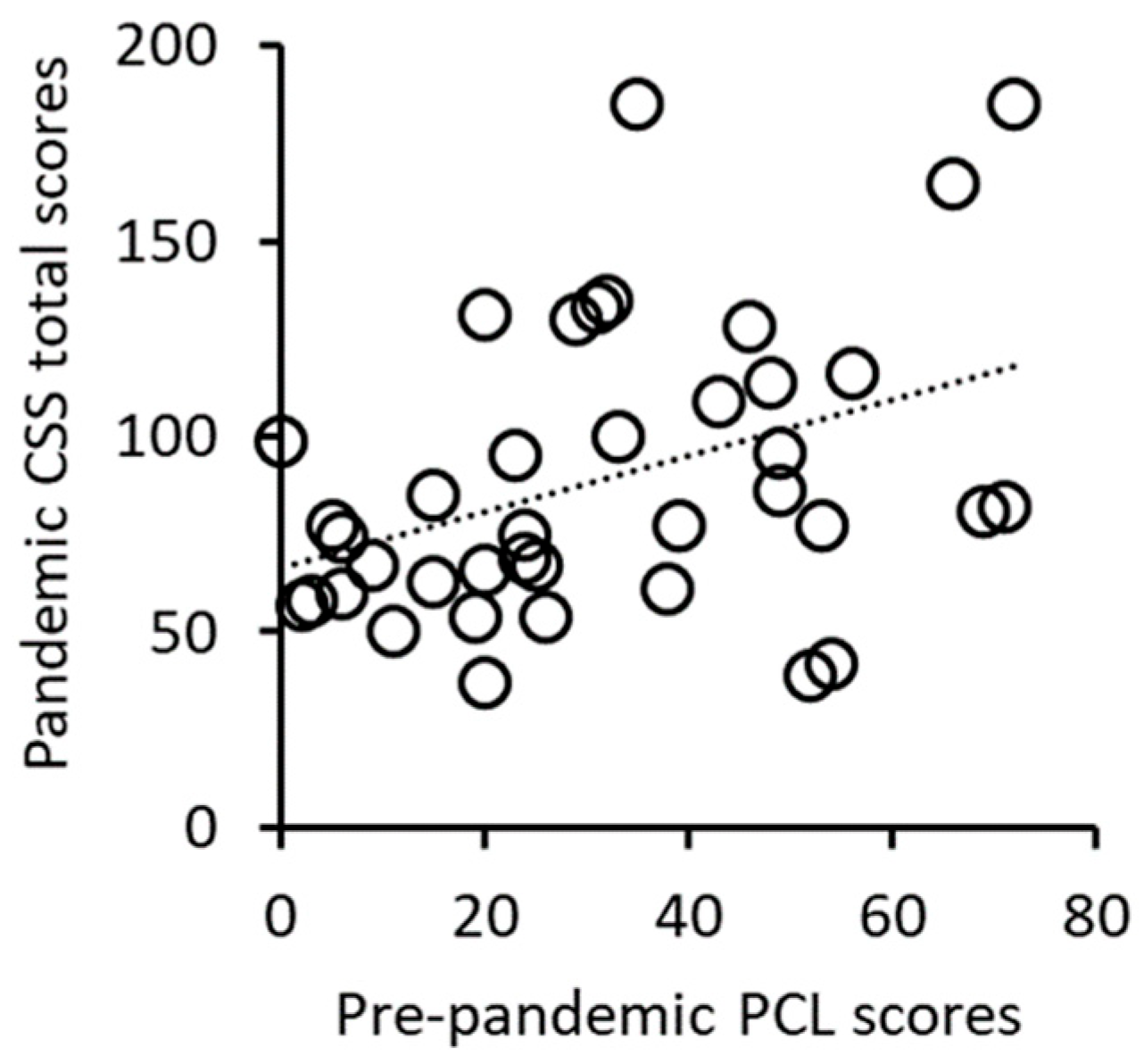
3.2. Correlation Analysis of Pre-Pandemic PCL Scores and Pandemic CSS Scores
3.3. Analyses of Pandemic CSS Scores in Post-Pandemic PTSD vs. Non-PTSD Subjects
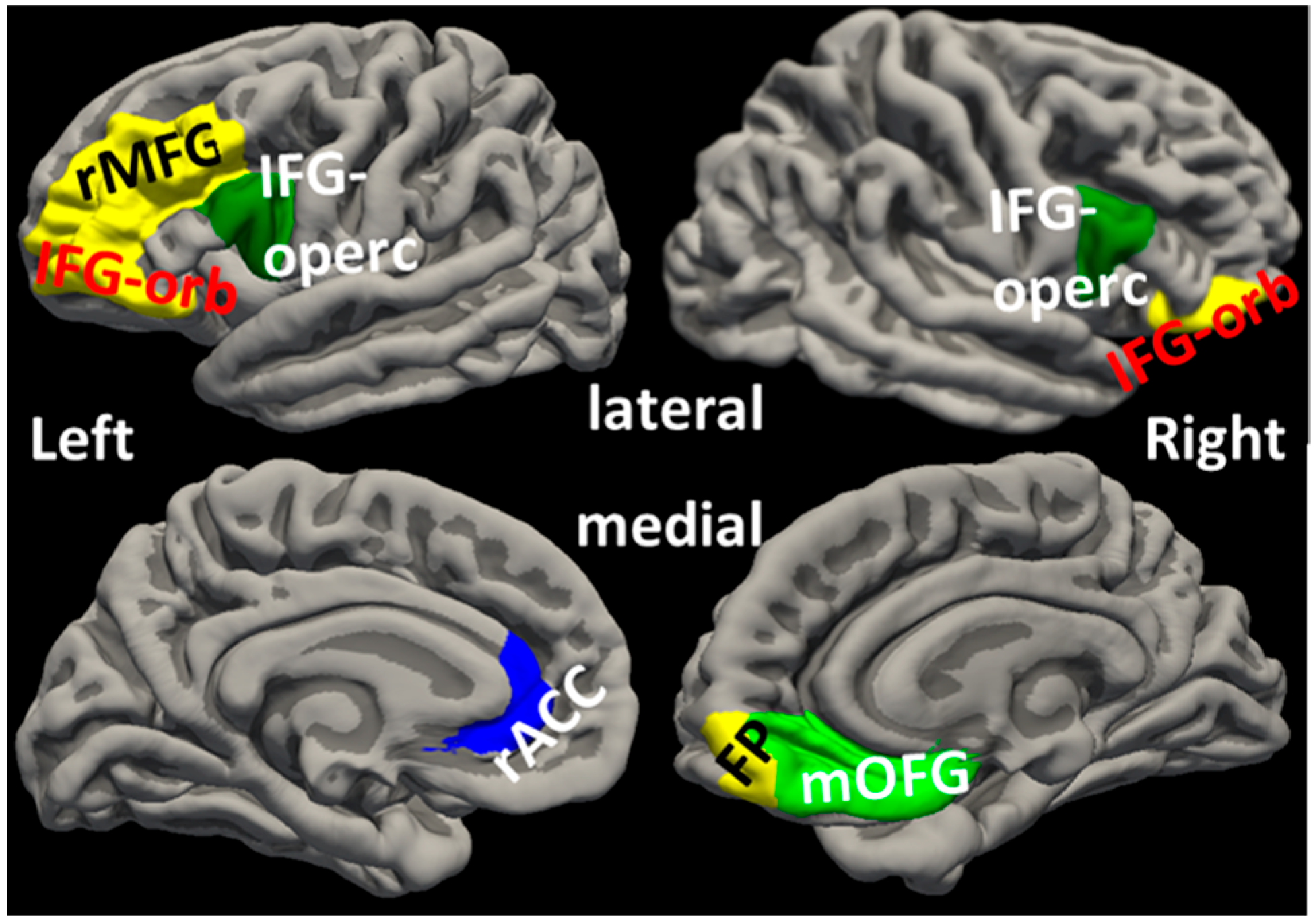
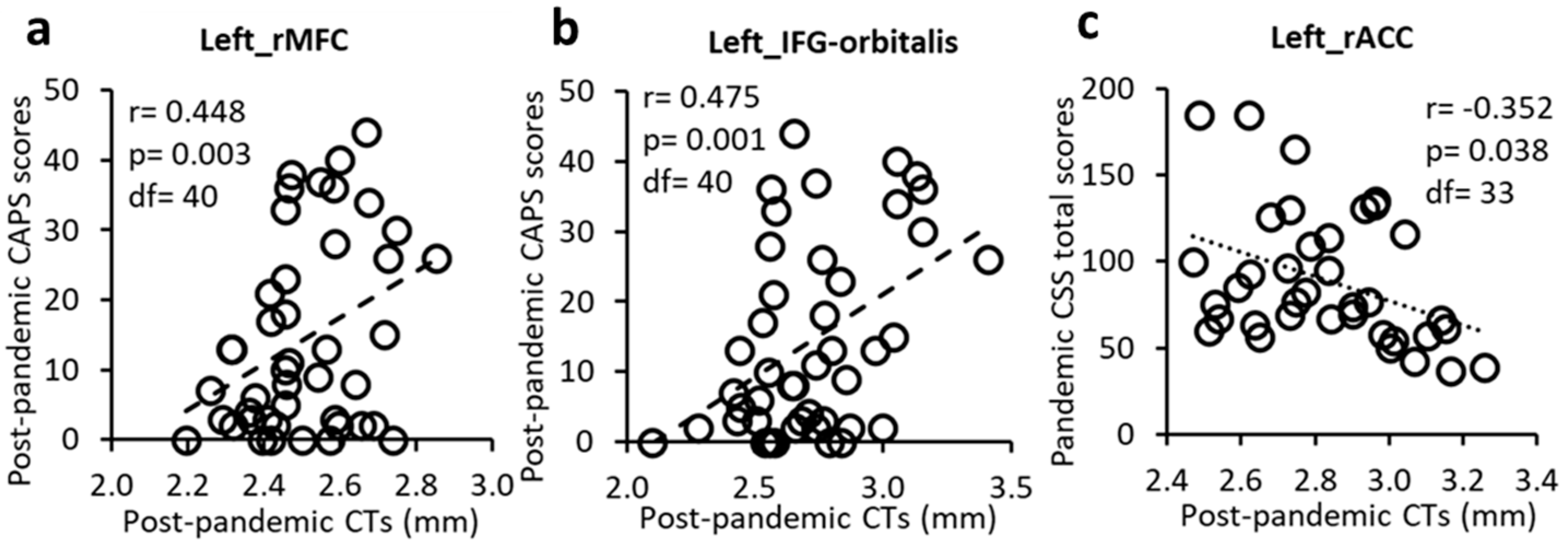
3.4. Correlation Analyses of Post-Pandemic Prefrontal Cortical Thicknesses, PTSD Symptoms, and COVID-19-Related Stress
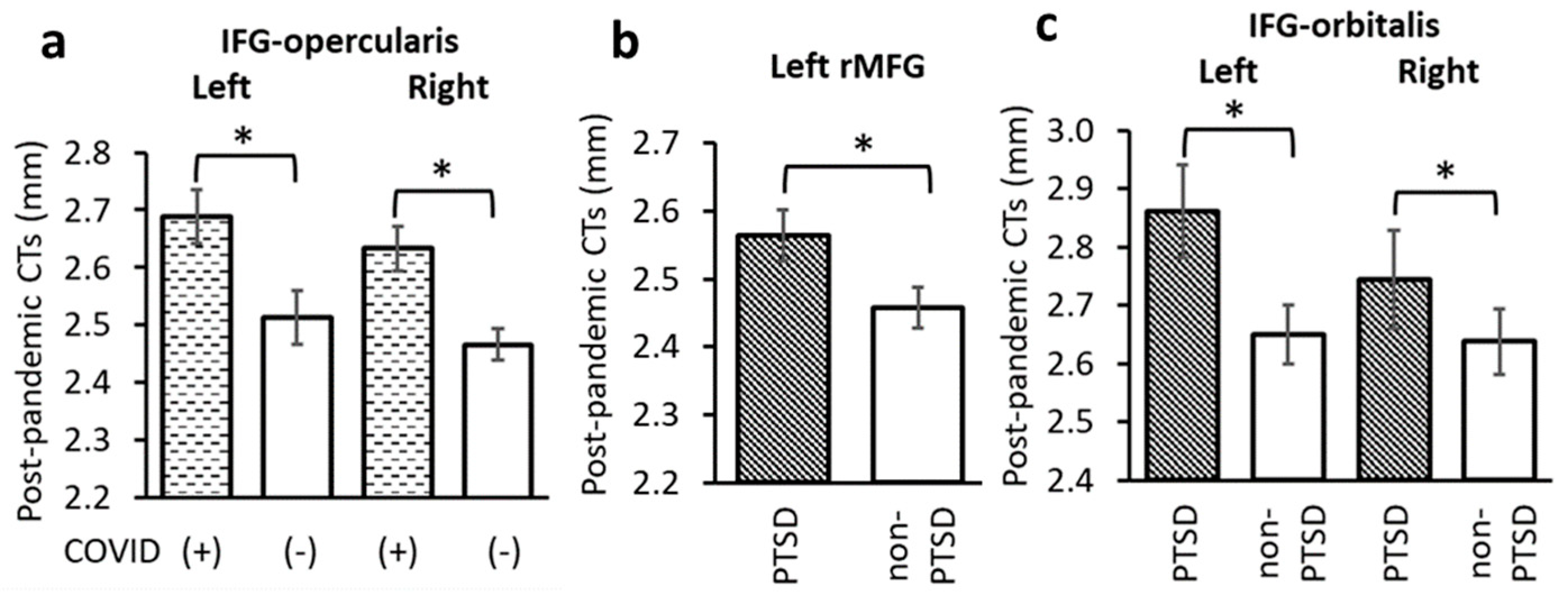
3.5. Effects of COVID-19 Infection and PTSD on Post-Pandemic Prefrontal Cortical Thicknesses
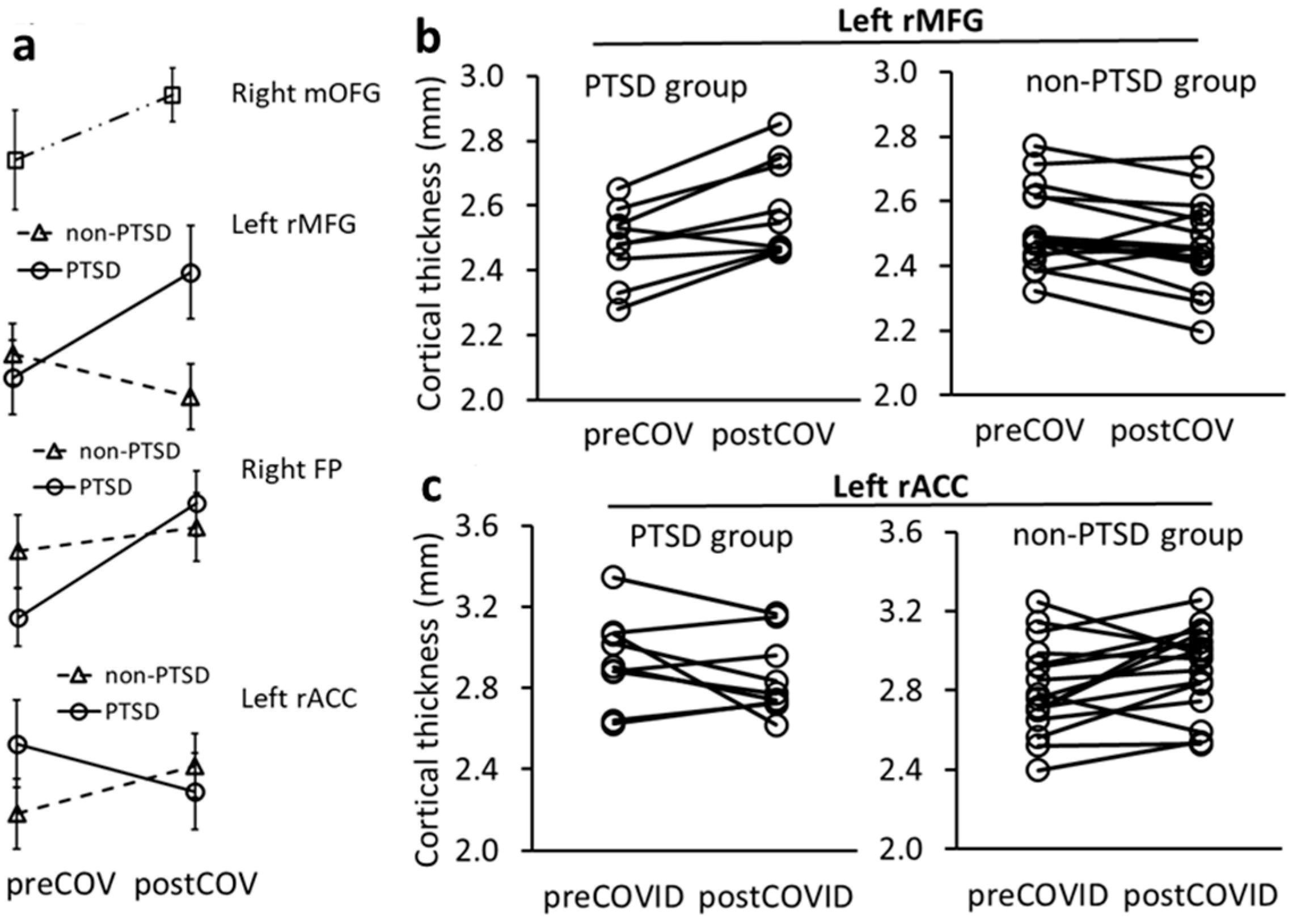
3.6. Changes in Prefrontal Cortical Thickness from Pre- to Post-Pandemic Time and Associations with PTSD and COVID-19 Infection
4. Discussion
4.1. PFC Involvement in Stress and PTSD
4.2. PFC Involvement in COVID-19 Viral Infection
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
Appendix A.1. Assessments
Appendix A.2. Results

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PTSD Group | Non-PTSD Group | Comparison (f, p) | |
|---|---|---|---|
| PSS | 18.2 ± 7.3 | 21.1 ± 7.7 | 1.632, 0.210 |
| Depression mood | 17.0 ± 7.5 | 23.6 ± 8.8 | 3.599, 0.067 |
| Anxiety mood | 16.7 ± 9.8 | 22.2 ± 6.8 | 3.888, 0.057 |
| PFC Cortical Thicknesses | PSS Score | Depression Mood | Anxiety Mood | |
|---|---|---|---|---|
| L_caudalanteriorcingulate | Correlation | 0.189 | −0.344 | −0.258 |
| p | 0.277 | 0.054 | 0.141 | |
| df | 33 | 30 | 32 | |
| L_caudalmiddlefrontal | Correlation | 0.078 | 0.138 | 0.017 |
| p | 0.655 | 0.451 | 0.922 | |
| df | 33 | 30 | 32 | |
| L_lateralorbitofrontal | Correlation | 0.081 | 0.049 | −0.116 |
| p | 0.643 | 0.792 | 0.513 | |
| df | 33 | 30 | 32 | |
| L_medialorbitofrontal | Correlation | 0.134 | −0.228 | −0.201 |
| p | 0.444 | 0.21 | 0.255 | |
| df | 33 | 30 | 32 | |
| L_parsopercularis | Correlation | 0.018 | 0.012 | −0.081 |
| p | 0.918 | 0.946 | 0.651 | |
| df | 33 | 30 | 32 | |
| L_parsorbitalis | Correlation | −0.142 | −0.177 | −0.21 |
| p | 0.416 | 0.332 | 0.232 | |
| df | 33 | 30 | 32 | |
| L_parstriangularis | Correlation | −0.109 | 0.004 | −0.169 |
| p | 0.535 | 0.983 | 0.338 | |
| df | 33 | 30 | 32 | |
| L_rostralanteriorcingulate | Correlation | 0.27 | −0.04 | −0.061 |
| p | 0.117 | 0.828 | 0.734 | |
| df | 33 | 30 | 32 | |
| L_rostralmiddlefrontal | Correlation | −0.084 | −0.008 | −0.084 |
| p | 0.632 | 0.964 | 0.638 | |
| df | 33 | 30 | 32 | |
| L_superiorfrontal | Correlation | 0.063 | −0.007 | −0.067 |
| p | 0.721 | 0.971 | 0.705 | |
| df | 33 | 30 | 32 | |
| L_frontalpole | Correlation | −0.201 | −0.111 | −0.088 |
| p | 0.246 | 0.545 | 0.62 | |
| df | 33 | 30 | 32 | |
| R_caudalanteriorcingulate | Correlation | −0.19 | −0.013 | −0.001 |
| p | 0.275 | 0.945 | 0.994 | |
| df | 33 | 30 | 32 | |
| R_caudalmiddlefrontal | Correlation | 0.232 | 0.204 | 0.079 |
| p | 0.179 | 0.264 | 0.659 | |
| df | 33 | 30 | 32 | |
| R_lateralorbitofrontal | Correlation | 0.099 | 0.066 | −0.02 |
| p | 0.57 | 0.721 | 0.908 | |
| df | 33 | 30 | 32 | |
| R_medialorbitofrontal | Correlation | −0.085 | 0.195 | −0.01 |
| p | 0.627 | 0.285 | 0.955 | |
| df | 33 | 30 | 32 | |
| R_parsopercularis | Correlation | 0.073 | −0.16 | −0.168 |
| p | 0.679 | 0.383 | 0.343 | |
| df | 33 | 30 | 32 | |
| R_parsorbitalis | Correlation | −0.284 | 0.059 | −0.103 |
| p | 0.099 | 0.749 | 0.563 | |
| df | 33 | 30 | 32 | |
| R_parstriangularis | Correlation | −0.008 | −0.121 | −0.161 |
| p | 0.965 | 0.509 | 0.363 | |
| df | 33 | 30 | 32 | |
| R_rostralanteriorcingulate | Correlation | −0.037 | −0.02 | −0.143 |
| p | 0.831 | 0.912 | 0.419 | |
| df | 33 | 30 | 32 | |
| R_rostralmiddlefrontal | Correlation | −0.083 | −0.02 | −0.158 |
| p | 0.634 | 0.915 | 0.373 | |
| df | 33 | 30 | 32 | |
| R_superiorfrontal | Correlation | −0.001 | 0.086 | −0.037 |
| p | 0.995 | 0.64 | 0.834 | |
| df | 33 | 30 | 32 | |
| R_frontalpole | Correlation | 0.001 | −0.001 | 0.026 |
| p | 0.994 | 0.997 | 0.882 | |
| df | 33 | 30 | 32 |
References
- Holmes, E.A.; O’Connor, R.C.; Perry, V.H.; Tracey, I.; Wessely, S.; Arseneault, L.; Ballard, C.; Christensen, H.; Cohen Silver, R.; Everall, I.; et al. Multidisciplinary research priorities for the COVID-19 pandemic: A call for action for mental health science. Lancet Psychiatry 2020, 7, 547–560. [Google Scholar] [CrossRef] [PubMed]
- Vahia, I.V.; Jeste, D.V.; Reynolds, C.F., III. Older Adults and the Mental Health Effects of COVID-19. JAMA 2020, 324, 2253–2254. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Scherer, N.; Felix, L.; Kuper, H. Prevalence of depression, anxiety and post-traumatic stress disorder in health care workers during the COVID-19 pandemic: A systematic review and meta-analysis. PLoS ONE 2021, 16, e0246454. [Google Scholar] [CrossRef]
- Liu, C.H.; Zhang, E.; Wong, G.T.F.; Hyun, S.; Hahm, H.C. Factors associated with depression, anxiety, and PTSD symptomatology during the COVID-19 pandemic: Clinical implications for U.S. young adult mental health. Psychiatry Res. 2020, 290, 113172. [Google Scholar] [CrossRef]
- Calegaro, V.C.; Ramos-Lima, L.F.; Hoffmann, M.S.; Zoratto, G.; Kerber, N.; Costa, F.C.D.; Picinin, V.D.; Köchler, J.; Rodrigues, L.; Maciel, L.; et al. Closed doors: Predictors of stress, anxiety, depression, and PTSD during the onset of COVID-19 pandemic in Brazil. J. Affect. Disord. 2022, 310, 441–451. [Google Scholar] [CrossRef]
- Diniz, C.R.A.F.; Crestani, A.P. The times they are a-changin’: A proposal on how brain flexibility goes beyond the obvious to include the concepts of “upward” and “downward” to neuroplasticity. Mol. Psychiatry 2023, 28, 977–992. [Google Scholar] [CrossRef]
- Huether, G.; Doering, S.; Rüger, U.; Rüther, E.; Schüssler, G. The stress-reaction process and the adaptive modification and reorganization of neuronal networks. Psychiatry Res. 1999, 87, 83–95. [Google Scholar] [CrossRef]
- Cerqueira, J.J.; Almeida, O.F.X.; Sousa, N. The stressed prefrontal cortex. Left? Right! Brain Behav. Immun. 2008, 22, 630–638. [Google Scholar] [CrossRef]
- Girotti, M.; Adler, S.M.; Bulin, S.E.; Fucich, E.A.; Paredes, D.; Morilak, D.A. Prefrontal cortex executive processes affected by stress in health and disease. Prog. Neuropsychopharmacol. Biol. Psychiatry 2018, 85, 161–179. [Google Scholar] [CrossRef]
- Sherin, J.E.; Nemeroff, C.B. Post-traumatic stress disorder: The neurobiological impact of psychological trauma. Dialogues Clin. Neurosci. 2011, 13, 263–278. [Google Scholar] [CrossRef]
- Esagoff, A.I.; Stevens, D.A.; Kosyakova, N.; Woodard, K.; Jung, D.; Richey, L.N.; Daneshvari, N.O.; Luna, L.P.; Bray, M.J.C.; Bryant, B.R.; et al. Neuroimaging Correlates of Post-Traumatic Stress Disorder in Traumatic Brain Injury: A Systematic Review of the Literature. J. Neurotrauma 2023, 40, 1029–1044. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, A.F.; Miskowiak, K.K.; Hyphantis, T.N.; Kohler, C.A.; Alves, G.S.; Bortolato, B.; Sales, P.M.G.; Machado-Vieira, R.; Berk, M.; McIntyre, R.S. Cognitive Dysfunction in Depression—Pathophysiology and Novel Targets. CNS Neurol. Disord. Drug Targets 2014, 13, 1819–1835. [Google Scholar] [CrossRef] [PubMed]
- Ferreri, F.; Lapp, L.K.; Peretti, C.-S. Current research on cognitive aspects of anxiety disorders. Curr. Opin. Psychiatry 2011, 24, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Polak, A.R.; Witteveen, A.B.; Reitsma, J.B.; Olff, M. The role of executive function in posttraumatic stress disorder: A systematic review. J. Affect. Disord. 2012, 141, 11–21. [Google Scholar] [CrossRef]
- Morey, R.A.; Dunsmoor, J.E.; Haswell, C.C.; Brown, V.M.; Vora, A.; Weiner, J.; Stjepanovic, D.; Wagner, H.R.; Brancu, M.; Marx, C.E.; et al. Fear learning circuitry is biased toward generalization of fear associations in posttraumatic stress disorder. Transl. Psychiatry 2015, 5, e700. [Google Scholar] [CrossRef]
- Neelam, K.; Duddu, V.; Anyim, N.; Neelam, J.; Lewis, S. Pandemics and pre-existing mental illness: A systematic review and meta-analysis. Brain Behav. Immun. Health 2021, 10, 100177. [Google Scholar] [CrossRef]
- Arnsten, A.F.T. Stress signalling pathways that impair prefrontal cortex structure and function. Nat. Rev. Neurosci. 2009, 10, 410–422. [Google Scholar] [CrossRef]
- Kredlow, M.A.; Fenster, R.J.; Laurent, E.S.; Ressler, K.J.; Phelps, E.A. Prefrontal cortex, amygdala, and threat processing: Implications for PTSD. Neuropsychopharmacology 2022, 47, 247–259. [Google Scholar] [CrossRef]
- Baldaçara, L.; Zugman, A.; Araújo, C.; Cogo-Moreira, H.; Lacerda, A.L.T.; Schoedl, A.; Pupo, M.; Mello, M.F.; Andreoli, S.B.; de Jesus Mari, J.; et al. Reduction of anterior cingulate in adults with urban violence- related PTSD. J. Affect. Disord. 2014, 168, 13–20. [Google Scholar] [CrossRef]
- Morey, R.A.; Haswell, C.C.; Hooper, S.R.; De Bellis, M.D. Amygdala, Hippocampus, and Ventral Medial Prefrontal Cortex Volumes Differ in Maltreated Youth with and without Chronic Posttraumatic Stress Disorder. Neuropsychopharmacology 2016, 41, 791–801. [Google Scholar] [CrossRef]
- Milad, M.R.; Quinn, B.T.; Pitman, R.K.; Orr, S.P.; Fischl, B.; Rauch, S.L. Thickness of ventromedial prefrontal cortex in humans is correlated with extinction memory. Proc. Natl. Acad. Sci. USA 2005, 102, 10706–10711. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Xie, H.; Chen, T.; Cotton, A.S.; Salminen, L.E.; Logue, M.W.; Clarke-Rubright, E.K.; Wall, J.; Dennis, E.L.; O’Leary, B.M.; et al. Cortical volume abnormalities in posttraumatic stress disorder: An ENIGMA-psychiatric genomics consortium PTSD workgroup mega-analysis. Mol. Psychiatry 2021, 26, 4331–4343. [Google Scholar] [CrossRef] [PubMed]
- Lyoo, I.K.; Kim, J.E.; Yoon, S.J.; Hwang, J.; Bae, S.; Kim, D.J. The Neurobiological Role of the Dorsolateral Prefrontal Cortex in Recovery From Trauma: Longitudinal Brain Imaging Study Among Survivors of the South Korean Subway Disaster. Arch. Gen. Psychiatry 2011, 68, 701–713. [Google Scholar] [CrossRef] [PubMed]
- Sekiguchi, A.; Sugiura, M.; Taki, Y.; Kotozaki, Y.; Nouchi, R.; Takeuchi, H.; Araki, T.; Hanawa, S.; Nakagawa, S.; Miyauchi, C.M.; et al. Brain structural changes as vulnerability factors and acquired signs of post-earthquake stress. Mol. Psychiatry 2013, 18, 618–623. [Google Scholar] [CrossRef]
- Douaud, G.; Lee, S.; Alfaro-Almagro, F.; Arthofer, C.; Wang, C.; McCarthy, P.; Lange, F.; Andersson, J.L.R.; Griffanti, L.; Duff, E.; et al. SARS-CoV-2 is associated with changes in brain structure in UK Biobank. Nature 2022, 604, 697–707. [Google Scholar] [CrossRef]
- Kamaşak Arpaçay, B.; Ulcay, T.; Nisari, M.; Görgülü, Ö.; Akca, V.; Alpaslan, M.; Yetis, A.; Hizmali, L.; Karahocagil, M.; Aycan, K. Effects of COVID-19 on brain and cerebellum: A voxel based morphometrical analysis. Bratisl. Lek. Listy 2023, 124, 442–448. [Google Scholar] [CrossRef]
- Bendella, Z.; Widmann, C.N.; Layer, J.P.; Layer, Y.L.; Haase, R.; Sauer, M.; Bieler, L.; Lehnen, N.C.; Paech, D.; Heneka, M.T.; et al. Brain Volume Changes after COVID-19 Compared to Healthy Controls by Artificial Intelligence-Based MRI Volumetry. Diagnostics 2023, 13, 1716. [Google Scholar] [CrossRef]
- Lu, Y.; Li, X.; Geng, D.; Mei, N.; Wu, P.-Y.; Huang, C.-C.; Jia, T.; Zhao, Y.; Wang, D.; Xiao, A.; et al. Cerebral Micro-Structural Changes in COVID-19 Patients—An MRI-based 3-month Follow-up Study. EClinicalMedicine 2020, 25, 1–12. [Google Scholar] [CrossRef]
- Sanabria-Diaz, G.; Etter, M.M.; Melie-Garcia, L.; Lieb, J.M.; Psychogios, M.-N.; Hutter, G.; Granziera, C. Brain cortical alterations in COVID-19 patients with neurological symptoms. Front. Neurosci. 2022, 16, 992165. [Google Scholar] [CrossRef]
- Du, Y.; Zhao, W.; Huang, S.; Huang, C.; Li, C.; Chen, Y.; Huang, Y.; Yang, L.; Li, C.; Zhang, H.; et al. Gray Matter Thickness and Subcortical Nuclear Volume in Men After SARS-CoV-2 Omicron Infection. JAMA Netw. Open 2023, 6, e2345626. [Google Scholar] [CrossRef]
- Besteher, B.; Machnik, M.; Troll, M.; Toepffer, A.; Zerekidze, A.; Rocktäschel, T.; Heller, C.; Kikinis, Z.; Brodoehl, S.; Finke, K.; et al. Larger gray matter volumes in neuropsychiatric long-COVID syndrome. Psychiatry Res. 2022, 317, 114836. [Google Scholar] [CrossRef] [PubMed]
- Xie, H.; Shih, C.-H.; Aldoohan, S.D.; Wall, J.T.; Wang, X. Hypothalamus volume mediates the association between adverse childhood experience and PTSD development after adulthood trauma. Transl. Psychiatry 2023, 13, 274. [Google Scholar] [CrossRef] [PubMed]
- Taylor, S.; Landry, C.A.; Paluszek, M.M.; Fergus, T.A.; McKay, D.; Asmundson, G.J.G. Development and initial validation of the COVID Stress Scales. J. Anxiety Disord. 2020, 72, 102232. [Google Scholar] [CrossRef] [PubMed]
- Weathers, F.W.; Bovin, M.J.; Lee, D.J.; Sloan, D.M.; Schnurr, P.P.; Kaloupek, D.G.; Keane, T.M.; Marx, B.P. The Clinician-Administered PTSD Scale for DSM–5 (CAPS-5): Development and initial psychometric evaluation in military veterans. Psychol. Assess. 2018, 30, 383–395. [Google Scholar] [CrossRef]
- Mylle, J.; Maes, M. Partial posttraumatic stress disorder revisited. J. Affect. Disord. 2004, 78, 37–48. [Google Scholar] [CrossRef]
- Blevins, C.A.; Weathers, F.W.; Davis, M.T.; Witte, T.K.; Domino, J.L. The Posttraumatic Stress Disorder Checklist for DSM-5 (PCL-5): Development and Initial Psychometric Evaluation. J. Trauma. Stress. 2015, 28, 489–498. [Google Scholar] [CrossRef]
- Fischl, B.; Dale, A.M. Measuring the thickness of the human cerebral cortex from magnetic resonance images. Proc. Natl. Acad. Sci. USA 2000, 97, 11050–11055. [Google Scholar] [CrossRef]
- Spinhoven, P.; Penninx, B.W.; van Hemert, A.M.; de Rooij, M.; Elzinga, B.M. Comorbidity of PTSD in anxiety and depressive disorders: Prevalence and shared risk factors. Child. Abus. Negl. 2014, 38, 1320–1330. [Google Scholar] [CrossRef]
- Lubomirsky, B.; Wang, X.; Xie, H.; Smirnoff, J.B.; Biehn, T.L.; Contractor, A.A.; Elhai, J.D.; Sutu, C.; Brickman, K.R.; Liberzon, I.; et al. Preliminary Study on the Relationship Between Visitation in the Emergency Department and Posttraumatic Mental Health. Soc. Work. Ment. Health 2014, 12, 69–80. [Google Scholar] [CrossRef]
- McEwen, B.S.; Morrison, J.H. The Brain on Stress: Vulnerability and Plasticity of the Prefrontal Cortex over the Life Course. Neuron 2013, 79, 16–29. [Google Scholar] [CrossRef]
- New, A.S.; Fan, J.; Murrough, J.W.; Liu, X.; Liebman, R.E.; Guise, K.G.; Tang, C.Y.; Charney, D.S. A functional magnetic resonance imaging study of deliberate emotion regulation in resilience and posttraumatic stress disorder. Biol. Psychiatry 2009, 66, 656–664. [Google Scholar] [CrossRef] [PubMed]
- Kaul, D.; Schwab, S.G.; Mechawar, N.; Matosin, N. How stress physically re-shapes the brain: Impact on brain cell shapes, numbers and connections in psychiatric disorders. Neurosci. Biobehav. Rev. 2021, 124, 193–215. [Google Scholar] [CrossRef] [PubMed]
- Crocker, L.D.; Heller, W.; Warren, S.L.; O’Hare, A.J.; Infantolino, Z.P.; Miller, G.A. Relationships among cognition, emotion, and motivation: Implications for intervention and neuroplasticity in psychopathology. Front. Hum. Neurosci. 2013, 7, 261. [Google Scholar] [CrossRef] [PubMed]
- Lanius, R.A.; Williamson, P.C.; Boksman, K.; Densmore, M.; Gupta, M.; Neufeld, R.W.; Gati, J.S.; Menon, R.S. Brain activation during script-driven imagery induced dissociative responses in PTSD: A functional magnetic resonance imaging investigation. Biol. Psychiatry 2002, 52, 305–311. [Google Scholar] [CrossRef]
- Lee, H.; Oh, S.; Ha, E.; Joo, Y.; Suh, C.; Kim, Y.; Jeong, H.; Lyoo, I.K.; Yoon, S.; Hong, H. Cerebral cortical thinning in brain regions involved in emotional regulation relates to persistent symptoms in subjects with posttraumatic stress disorder. Psychiatry Res. 2023, 327, 115345. [Google Scholar] [CrossRef]
- Li, L.; Zhang, Y.; Zhao, Y.; Li, Z.; Kemp, G.J.; Wu, M.; Gong, Q. Cortical thickness abnormalities in patients with post-traumatic stress disorder: A vertex-based meta-analysis. Neurosci. Biobehav. Rev. 2022, 134, 104519. [Google Scholar] [CrossRef]
- Raschle, N.M.; Fehlbaum, L.V.; Menks, W.M.; Martinelli, A.; Prätzlich, M.; Bernhard, A.; Ackermann, K.; Freitag, C.; De Brito, S.; Fairchild, G.; et al. Atypical dorsolateral prefrontal activity in female adolescents with conduct disorder during effortful emotion regulation. Biol. Psychiatry Cogn. Neurosci. Neuroimaging 2019, 4, 984–994. [Google Scholar] [CrossRef]
- Michalski, L.J.; Demers, C.H.; Baranger, D.A.A.; Barch, D.M.; Harms, M.P.; Burgess, G.C.; Bogdan, R. Perceived stress is associated with increased rostral middle frontal gyrus cortical thickness: A family-based and discordant-sibling investigation. Genes Brain Behav. 2017, 16, 781–789. [Google Scholar] [CrossRef]
- Tops, M.; Boksem, M.A. A potential role of the inferior frontal gyrus and anterior insula in cognitive control, brain rhythms, and event-related potentials. Front. Psychol. 2011, 2, 330. [Google Scholar] [CrossRef]
- Greenlee, J.D.W.; Oya, H.; Kawasaki, H.; Volkov, I.O.; Severson, M.A., III; Howard, M.A., III; Brugge, J.F. Functional connections within the human inferior frontal gyrus. J. Comp. Neurol. 2007, 503, 550–559. [Google Scholar] [CrossRef]
- Sprengelmeyer, R.; Rausch, M.; Eysel, U.T.; Przuntek, H. Neural structures associated with recognition of facial expressions of basic emotions. Proc. Biol. Sci. 1998, 265, 1927–1931. [Google Scholar] [CrossRef] [PubMed]
- Dapretto, M.; Bookheimer, S.Y. Form and Content: Dissociating Syntax and Semantics in Sentence Comprehension. Neuron 1999, 24, 427–432. [Google Scholar] [CrossRef] [PubMed]
- Hampshire, A.; Chamberlain, S.R.; Monti, M.M.; Duncan, J.; Owen, A.M. The role of the right inferior frontal gyrus: Inhibition and attentional control. Neuroimage 2010, 50, 1313–1319. [Google Scholar] [CrossRef] [PubMed]
- Rolls, E.T.; Hornak, J.; Wade, D.; McGrath, J. Emotion-related learning in patients with social and emotional changes associated with frontal lobe damage. J. Neurol. Neurosurg. Psychiatry 1994, 57, 1518–1524. [Google Scholar] [CrossRef]
- Quidé, Y.; O’Reilly, N.; Watkeys, O.J.; Carr, V.J.; Green, M.J. Effects of childhood trauma on left inferior frontal gyrus function during response inhibition across psychotic disorders. Psychol. Med. 2018, 48, 1454–1463. [Google Scholar] [CrossRef]
- van Rooij, S.J.H.; Rademaker, A.R.; Kennis, M.; Vink, M.; Kahn, R.S.; Geuze, E. Impaired right inferior frontal gyrus response to contextual cues in male veterans with PTSD during response inhibition. J. Psychiatry Neurosci. 2014, 39, 330–338. [Google Scholar] [CrossRef]
- Bush, G.; Luu, P.; Posner, M.I. Cognitive and emotional influences in anterior cingulate cortex. Trends Cogn. Sci. 2000, 4, 215–222. [Google Scholar] [CrossRef]
- Mueller, S.G.; Ng, P.; Neylan, T.; Mackin, S.; Wolkowitz, O.; Mellon, S.; Yan, X.; Flory, J.; Yehuda, R.; Marmar, C.R.; et al. Evidence for disrupted gray matter structural connectivity in posttraumatic stress disorder. Psychiatry Res. Neuroimaging 2015, 234, 194–201. [Google Scholar] [CrossRef]
- Qi, S.; Mu, Y.; Liu, K.; Zhang, J.; Huan, Y.; Tan, Q.; Shi, M.; Wang, Q.; Chen, Y.; Wang, H.; et al. Cortical inhibition deficits in recent onset PTSD after a single prolonged trauma exposure. Neuroimage Clin. 2013, 3, 226–233. [Google Scholar] [CrossRef]
- Kaye, R.; Chang, C.W.D.; Kazahaya, K.; Brereton, J.; Denneny, J.C., III. COVID-19 Anosmia Reporting Tool: Initial Findings. Otolaryngol.–Head. Neck Surg. 2020, 163, 132–134. [Google Scholar] [CrossRef]
- Santos, R.E.A.; da Silva, M.G.; do Monte Silva, M.C.B.; Barbosa, D.A.M.; Gomes, A.L.d.V.; Galindo, L.C.M.; da Silva Aragão, R.; Ferraz-Pereira, K.N. Onset and duration of symptoms of loss of smell/taste in patients with COVID-19: A systematic review. Am. J. Otolaryngol. 2021, 42, 102889. [Google Scholar] [CrossRef] [PubMed]
- Obiefuna, S.; Donohoe, C. Neuroanatomy, Nucleus Gustatory; StatPearls: Treasure Island, FL, USA, 2023. Available online: https://www.ncbi.nlm.nih.gov/books/NBK554522/ (accessed on 17 January 2025).
- Sun, Z.; Shi, C.; Jin, L. Mechanisms by Which SARS-CoV-2 Invades and Damages the Central Nervous System: Apart from the Immune Response and Inflammatory Storm, What Else Do We Know? Viruses 2024, 16, 663. [Google Scholar] [CrossRef] [PubMed]
- Masala, C.; Porcu, M.; Orofino, G.; Defazio, G.; Pinna, I.; Solla, P.; Ercoli, T.; Suri, J.S.; Spinato, G.; Saba, L. Neuroimaging evaluations of olfactory, gustatory, and neurological deficits in patients with long-term sequelae of COVID-19. Brain Imaging Behav. 2024, 18, 1480–1490. [Google Scholar] [CrossRef] [PubMed]
- Srinivasan, M. Taste Dysfunction and Long COVID-19. Front. Cell. Infect. Microbiol. 2021, 11, 716563. [Google Scholar] [CrossRef]
- Alhazmi, F.H.; Alsharif, W.M.; Alshoabi, S.A.; Gameraddin, M.; Aloufi, K.M.; Abdulaal, O.M.; Qurashi, A.A. Identifying cerebral microstructural changes in patients with COVID-19 using MRI: A systematic review. Brain Circ. 2023, 9, 6–15. [Google Scholar] [CrossRef]
- Du, Y.; Zhao, W.; Huang, S.; Huang, Y.; Chen, Y.; Zhang, H.; Guo, H.; Liu, J. Two-year follow-up of brain structural changes in patients who recovered from COVID-19: A prospective study. Psychiatry Res. 2023, 319, 114969. [Google Scholar] [CrossRef]
- Mukerji, S.S.; Solomon, I.H. What can we learn from brain autopsies in COVID-19? Neurosci. Lett. 2021, 742, 135528. [Google Scholar] [CrossRef]
- Sele, S.; Liem, F.; Mérillat, S.; Jäncke, L. Age-related decline in the brain: A longitudinal study on inter-individual variability of cortical thickness, area, volume, and cognition. Neuroimage 2021, 240, 118370. [Google Scholar] [CrossRef]
| Mean ± SD or N | |
|---|---|
| Age (year, (range)) | 35.1 ± 11.3 (19–55) |
| Time between (days) | |
| pandemic onset to survey | 794 ± 233 |
| pandemic onset to sMRI | 700 ± 261 |
| Days between 2 sMRI scans | 1299 ± 289 |
| Race (N) | |
| White | 19 |
| Black | 27 |
| Asian | 1 |
| Mixed | 2 |
| Unknown | 2 |
| Post-pandemic PTSD (N/total) | 16/44 |
| Positive COVID-19 test (N/total) | 19/49 |
| PTSD:non-PTSD | |
| positive COVID-19 test | 8:10 |
| Negative COVID-19 test | 7:17 |
| χ2, p | 1.046, 0.307 |
| Relationships | Mean ± SD | r, p (df = 34) |
|---|---|---|
| Pre-pandemic PCL score | 31.9 ± 20.3 | |
| CSS-danger | 16.9 ± 7.9 | 0.349, 0.037 * |
| CSS-Economic | 15.6 ± 7.4 | 0.376, 0.024 * |
| CSS-Xenophobia | 11.4 ± 7.0 | 0.276, 0.104 |
| CSS-Contamination | 13.9 ± 6.8 | 0.272, 0.109 |
| CSS-Traumatic | 13.0 ± 7.0 | 0.520, 0.001 * |
| CSS-Compulsive | 18.2 ± 8.0 | 0.365, 0.029 * |
| CSS total score | 88.9 ± 36.7 | 0.429, 0.009 * |
| PTSD Group | Non-PTSD Group | Group Comparison (f, p) | |
|---|---|---|---|
| CSS-Danger | 19.5 ± 9.2 | 14.6 ± 6.6 | 4.217, 0.048 * |
| CSS-Economic | 17.5 ± 8.0 | 13.8 ± 6.7 | 2.509, 0.122 |
| CSS-Xenophobia | 11.9 ± 7.2 | 9.9 ± 5.7 | 2.449, 0.127 |
| CSS-Contamination | 14.4 ± 8.0 | 12.7 ± 5.5 | 1.202, 0.280 |
| CSS-Traumatic | 15.3 ± 7.8 | 11.1 ± 5.5 | 4.732, 0.036 * |
| CSS-Compulsive | 19.3 ± 8.1 | 17.0 ± 7.7 | 0.671, 0.418 |
| CSS total score | 97.9 ± 38.3 | 79.2 ± 27.4 | 3.638, 0.065 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chandra, S.; Amer, A.; Shih, C.-H.; Shao, Q.; Wang, X.; Xie, H. COVID-19 Pandemic Impacts on STRESS, PTSD, and Prefrontal Cortical Thickness in Pre-Pandemic Trauma Survivors. J. Pers. Med. 2025, 15, 127. https://doi.org/10.3390/jpm15040127
Chandra S, Amer A, Shih C-H, Shao Q, Wang X, Xie H. COVID-19 Pandemic Impacts on STRESS, PTSD, and Prefrontal Cortical Thickness in Pre-Pandemic Trauma Survivors. Journal of Personalized Medicine. 2025; 15(4):127. https://doi.org/10.3390/jpm15040127
Chicago/Turabian StyleChandra, Sharad, Atheer Amer, Chia-Hao Shih, Qin Shao, Xin Wang, and Hong Xie. 2025. "COVID-19 Pandemic Impacts on STRESS, PTSD, and Prefrontal Cortical Thickness in Pre-Pandemic Trauma Survivors" Journal of Personalized Medicine 15, no. 4: 127. https://doi.org/10.3390/jpm15040127
APA StyleChandra, S., Amer, A., Shih, C.-H., Shao, Q., Wang, X., & Xie, H. (2025). COVID-19 Pandemic Impacts on STRESS, PTSD, and Prefrontal Cortical Thickness in Pre-Pandemic Trauma Survivors. Journal of Personalized Medicine, 15(4), 127. https://doi.org/10.3390/jpm15040127