
Do Patients with Benign Paroxysmal Positional Vertigo Have a Higher Prevalence of Osteoporosis? A Systematic Review and Meta-Analysis


Abstract
1. Introduction
2. Materials and Methods
2.1. Literature Search
2.2. Study Selection
2.3. Data Extraction
2.4. Risk of Bias Assessment
2.5. Data Synthesis and Statistical Analyses
3. Results
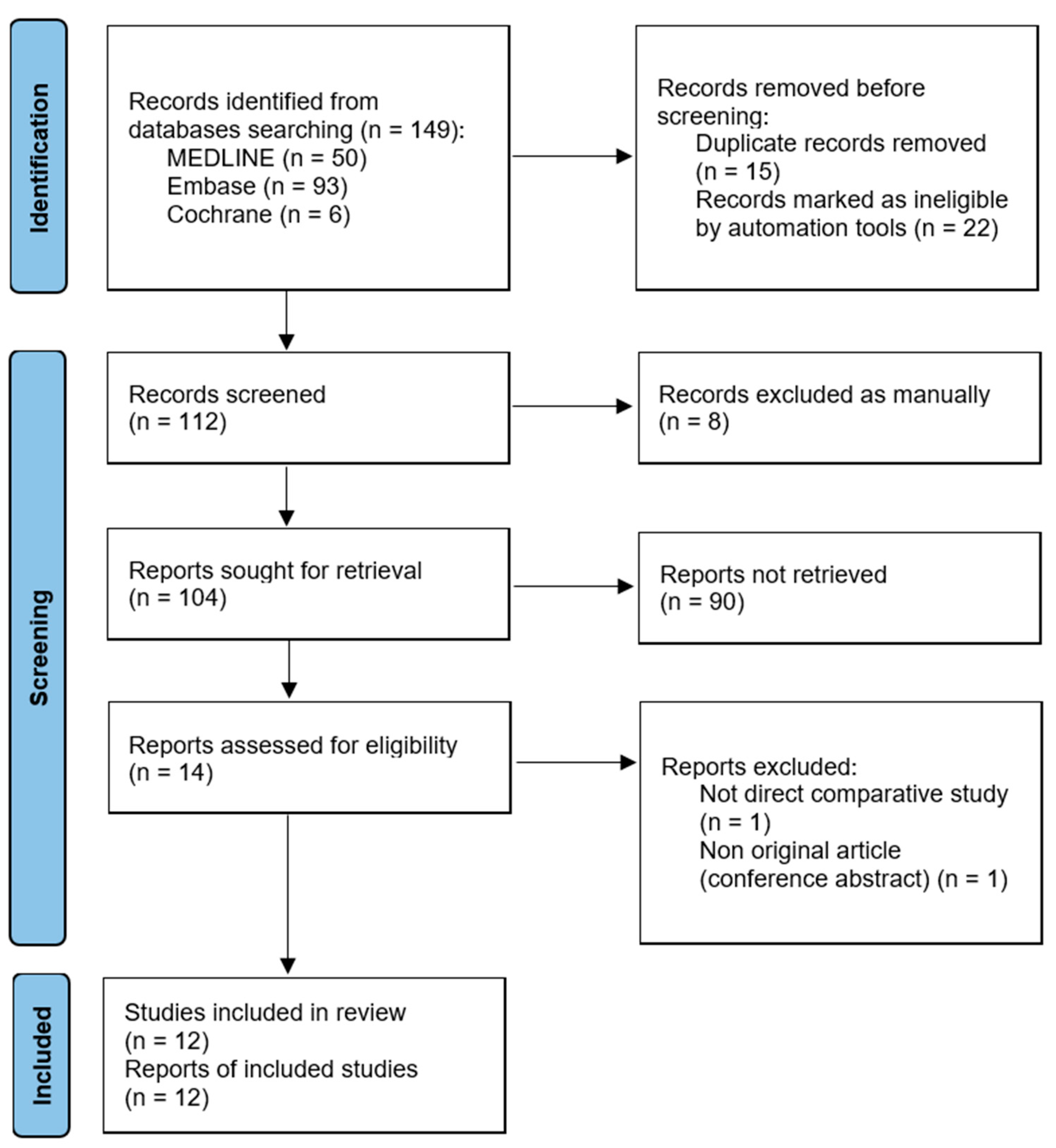
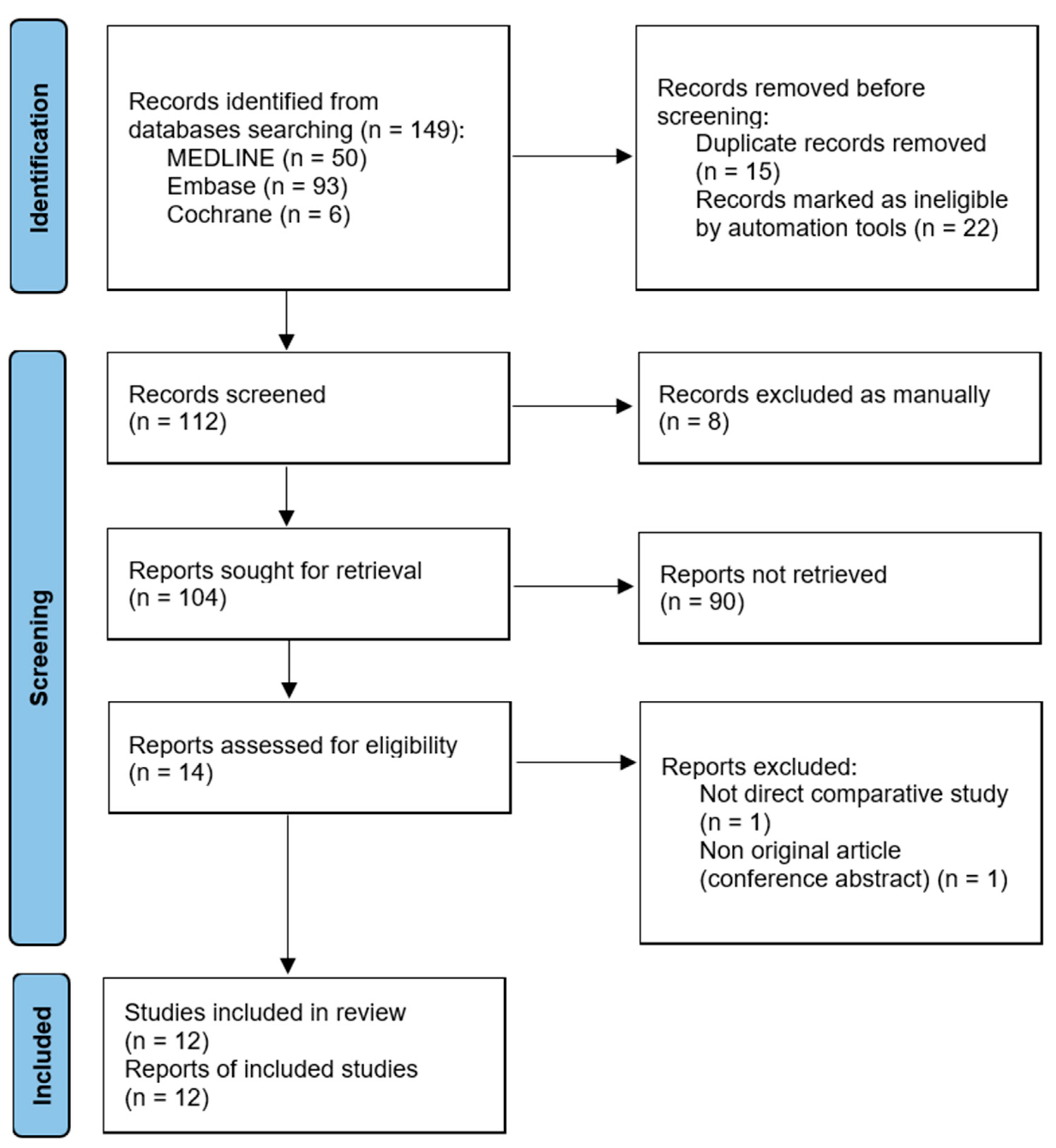
3.1. Article Identification
3.2. Study Characteristics and Qualitative Synthesis
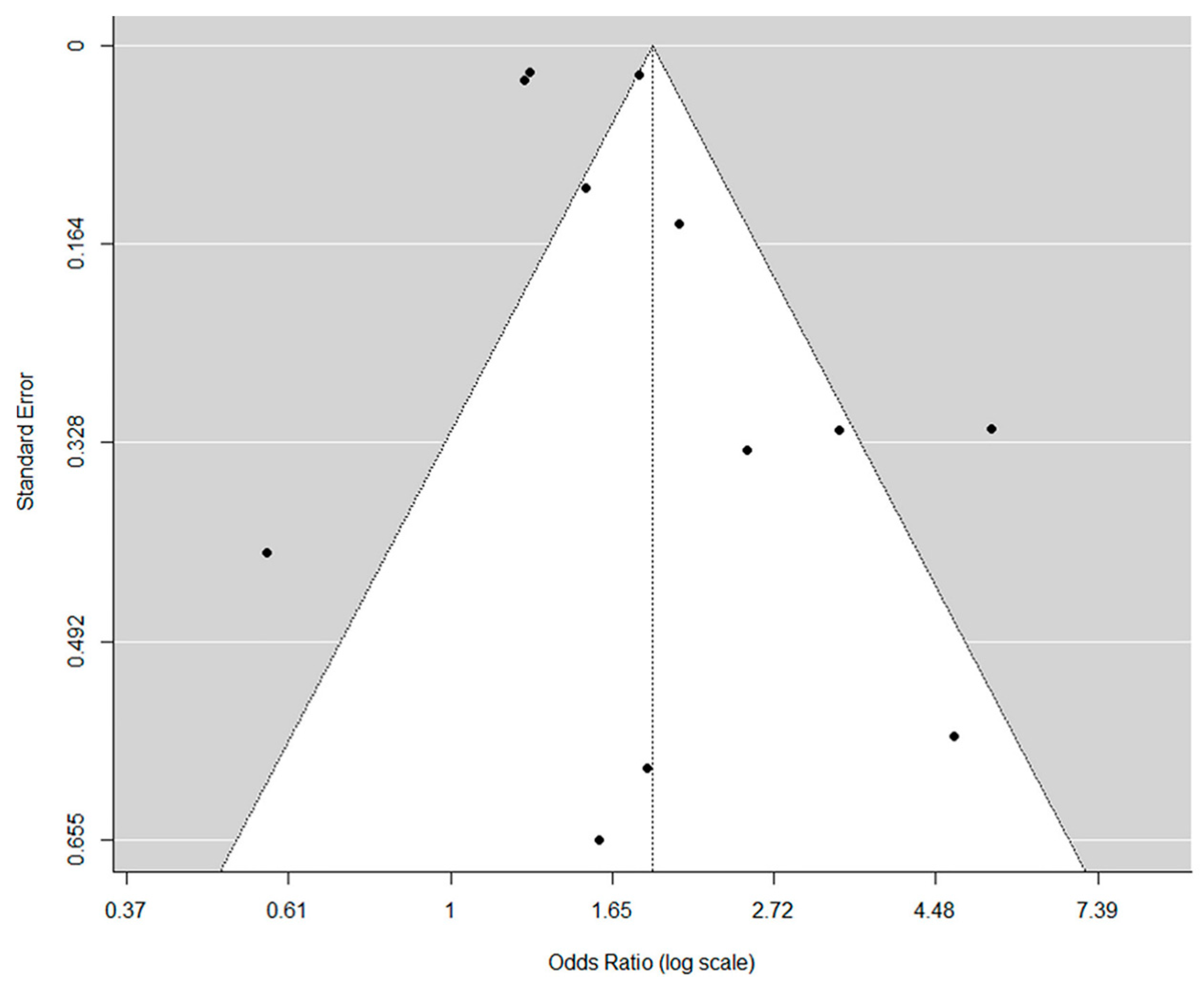
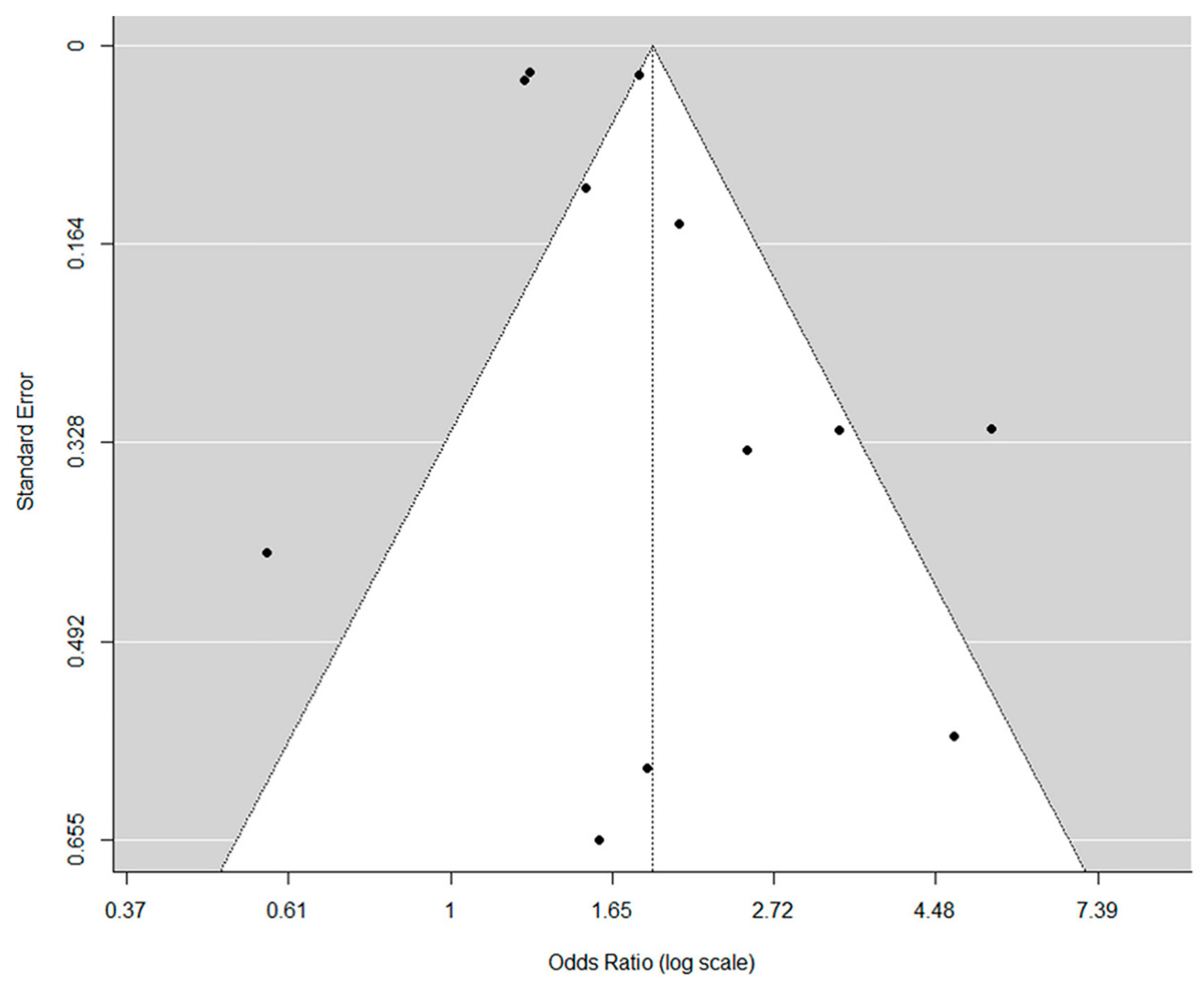
3.3. Risk of Bias Assessment
3.4. Meta-Analysis
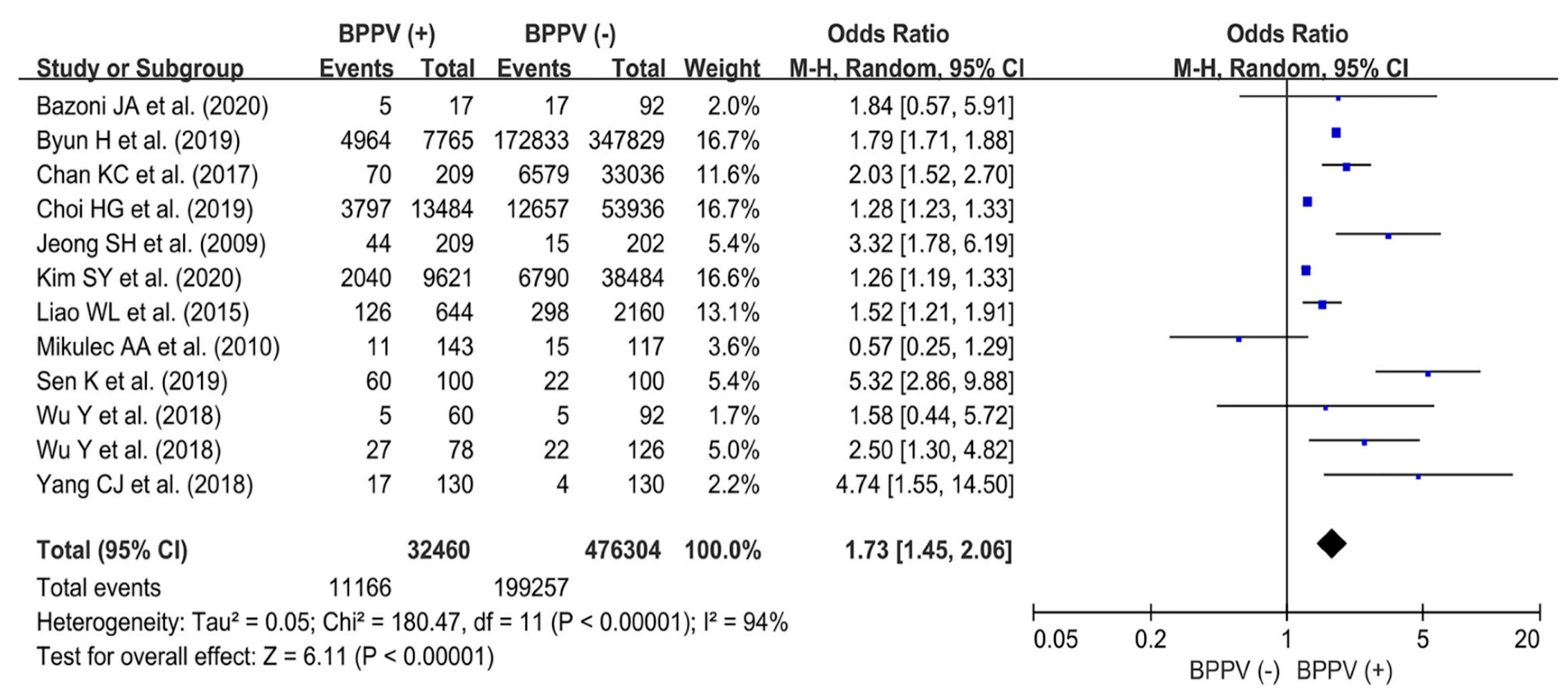
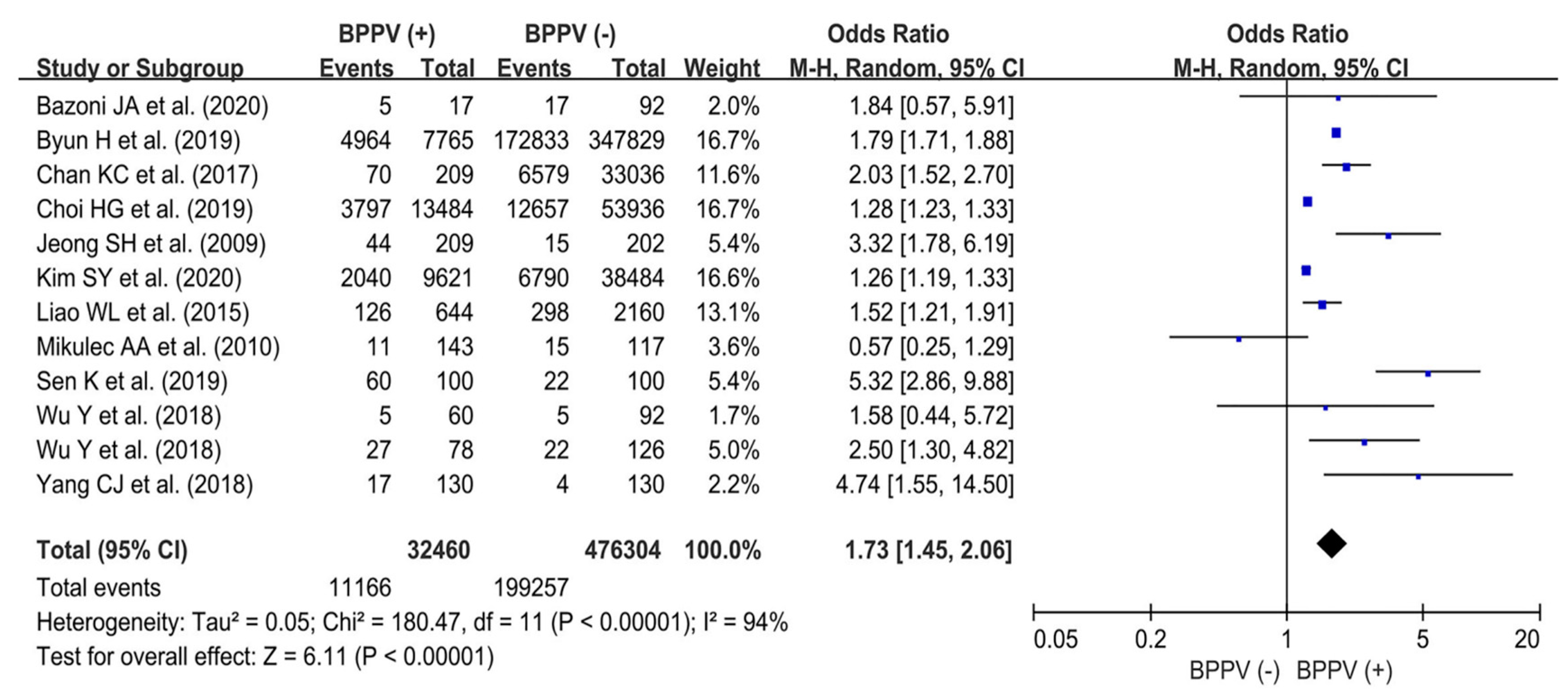
3.4.1. Prevalence of Osteoporosis between BPPV (+) and BPPV (−) Groups: Overall Population
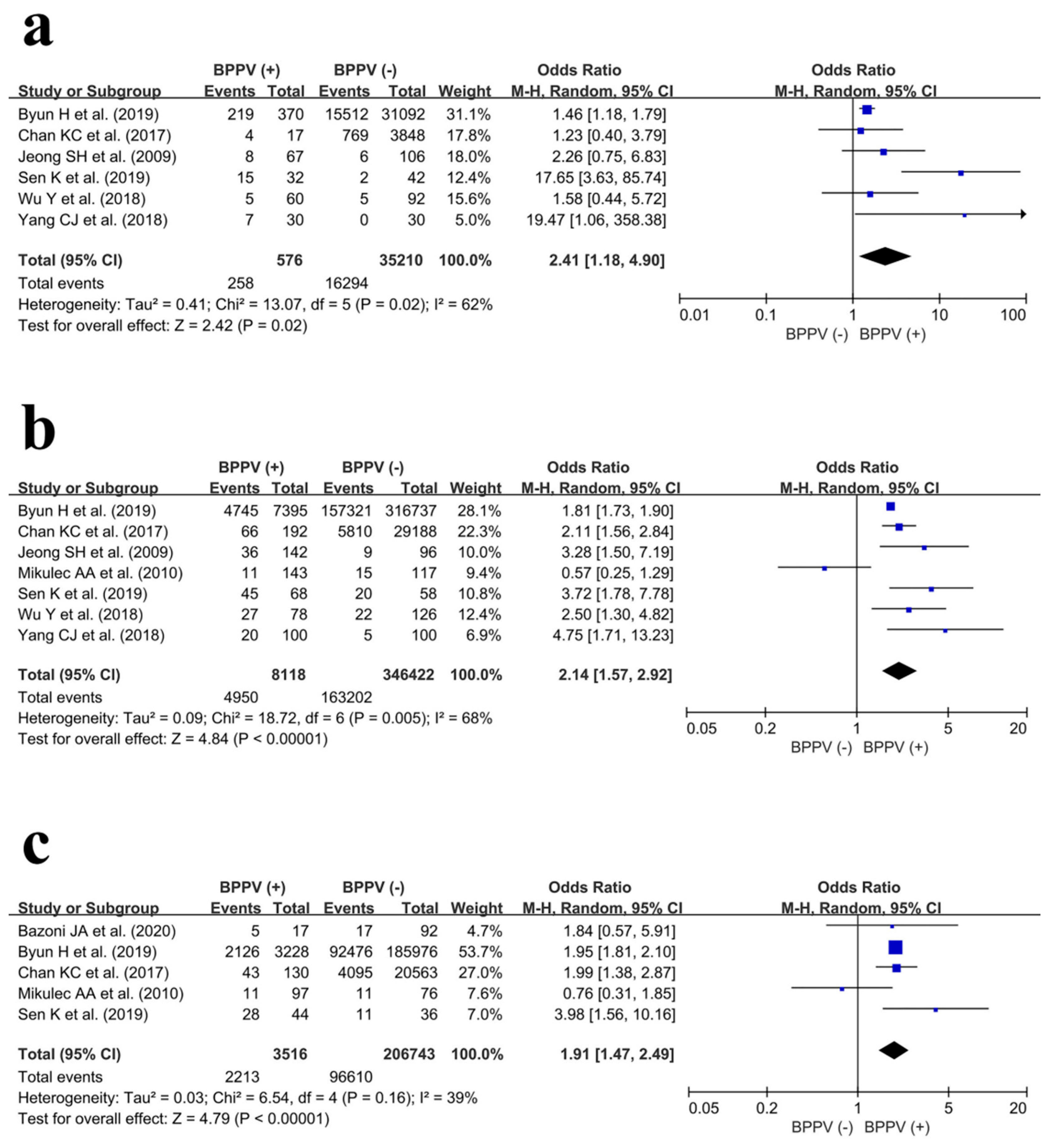
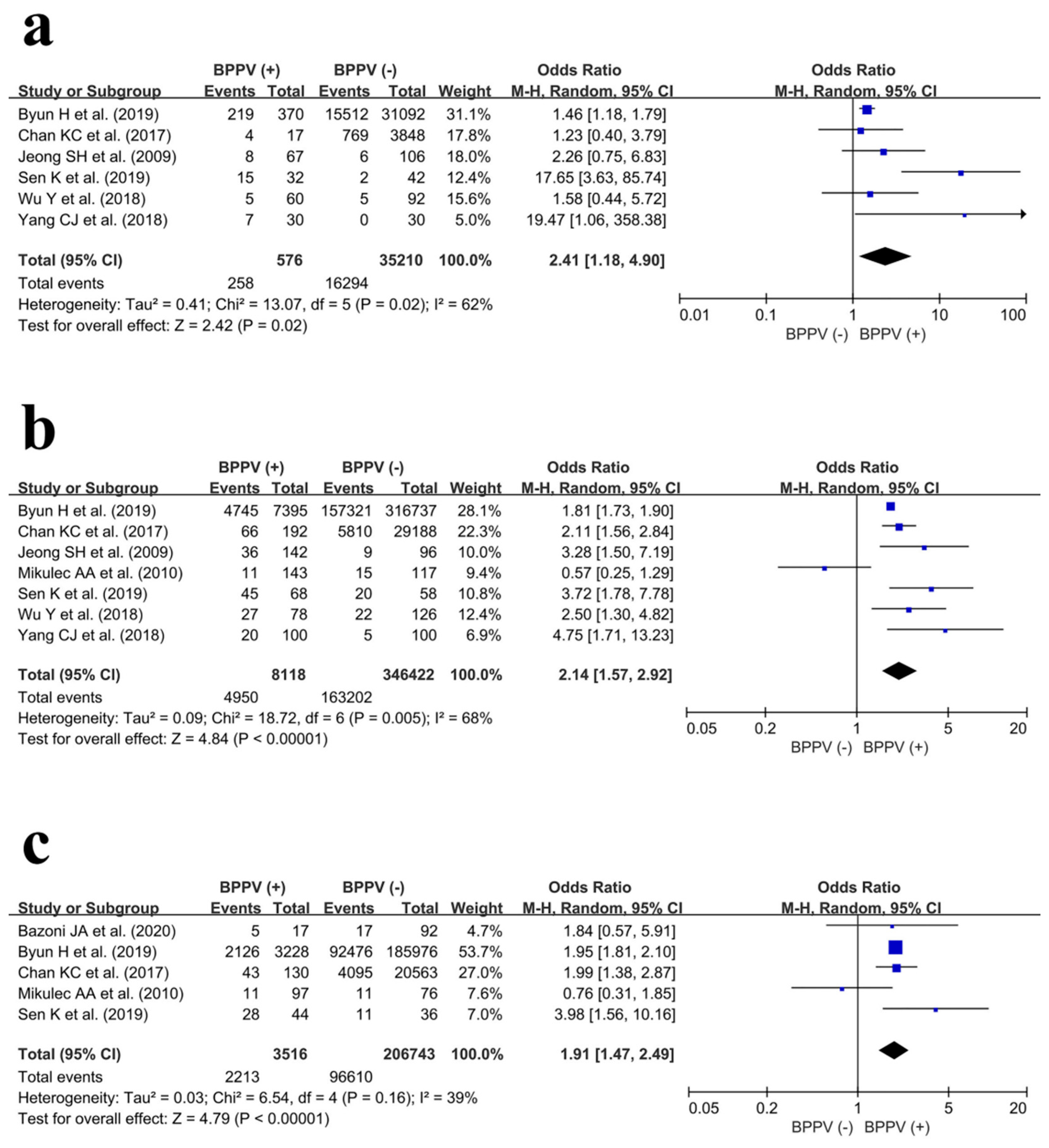
3.4.2. Subgroup Analyses: Male, Female, and Older Patient (Age ≥ 55 Years) Groups
Male Population
Female Population
Older Patients (Age ≥ 55 Years)
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Balatsouras, D.G.; Koukoutsis, G.; Fassolis, A.; Moukos, A.; Apris, A. Benign paroxysmal positional vertigo in the elderly: Current insights. Clin. Interv. Aging 2018, 13, 2251–2266. [Google Scholar] [CrossRef]
- De Stefano, A.; Dispenza, F. Spontaneous nystagmus in horizontal canal benign paroxysmal positional vertigo. Auris Nasus Larynx 2013, 40, 117. [Google Scholar] [CrossRef]
- Palmeri, R.; Kumar, A. Benign Paroxysmal Positional Vertigo. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Byun, H.; Chung, J.H.; Lee, S.H.; Park, C.W.; Kim, E.M.; Kim, I. Increased risk of benign paroxysmal positional vertigo in osteoporosis: A nationwide population-based cohort study. Sci. Rep. 2019, 9, 3469. [Google Scholar] [CrossRef]
- Parham, K.; Leonard, G.; Feinn, R.S.; Lafreniere, D.; Kenny, A.M. Prospective clinical investigation of the relationship between idiopathic benign paroxysmal positional vertigo and bone turnover: A pilot study. Laryngoscope 2013, 123, 2834–2839. [Google Scholar] [CrossRef]
- Jeong, S.H.; Choi, S.H.; Kim, J.Y.; Koo, J.W.; Kim, H.J.; Kim, J.S. Osteopenia and osteoporosis in idiopathic benign positional vertigo. Neurology 2009, 72, 1069–1076. [Google Scholar] [CrossRef]
- Mikulec, A.A.; Kowalczyk, K.A.; Pfitzinger, M.E.; Harris, D.A.; Jackson, L.E. Negative association between treated osteoporosis and benign paroxysmal positional vertigo in women. J. Laryngol. Otol. 2010, 124, 374–376. [Google Scholar] [CrossRef]
- Baek, Y.-H.; Cho, S.W.; Jeong, H.E.; Kim, J.H.; Hwang, Y.; Lange, J.L.; Shin, J.-Y. 10-Year Fracture Risk in Postmenopausal Women with Osteopenia and Osteoporosis in South Korea. Endocrinol. Metab. 2021, 36, 1178–1188. [Google Scholar] [CrossRef]
- Sozen, T.; Ozisik, L.; Basaran, N.C. An overview and management of osteoporosis. Eur. J. Rheumatol. 2017, 4, 46–56. [Google Scholar] [CrossRef]
- Yu, S.; Liu, F.; Cheng, Z.; Wang, Q. Association between osteoporosis and benign paroxysmal positional vertigo: A systematic review. BMC Neurol. 2014, 14, 110. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef]
- Shea, B.J.; Grimshaw, J.M.; Wells, G.A.; Boers, M.; Andersson, N.; Hamel, C.; Porter, A.C.; Tugwell, P.; Moher, D.; Bouter, L.M. Development of AMSTAR: A measurement tool to assess the methodological quality of systematic reviews. BMC Med. Res. Methodol. 2007, 7, 10. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Slim, K.; Nini, E.; Forestier, D.; Kwiatkowski, F.; Panis, Y.; Chipponi, J. Methodological index for non-randomized studies (minors): Development and validation of a new instrument. ANZ J. Surg. 2003, 73, 712–716. [Google Scholar] [CrossRef]
- Schmidt, F.L.; Oh, I.-S.; Hayes, T.L. Fixed- versus random-effects models in meta-analysis: Model properties and an empirical comparison of differences in results. Br. J. Math. Stat. Psychol. 2009, 62, 97–128. [Google Scholar] [CrossRef]
- Cumpston, M.; Li, T.; Page, M.J.; Chandler, J.; Welch, V.A.; Higgins, J.P.; Thomas, J. Updated guidance for trusted systematic reviews: A new edition of the Cochrane Handbook for Systematic Reviews of Interventions. Cochrane Database Syst. Rev. 2019, 10, ED000142. [Google Scholar] [CrossRef]
- Bazoni, J.A.; Ciquinato, D.S.A.; de Souza Marquez, A.; Costa, V.D.S.P.; De Moraes Marchiori, G.; de Moraes Marchiori, L.L. Hypovitaminosis D, low bone mineral density, and diabetes mellitus as probable risk factors for benign paroxysmal positional vertigo in the elderly. Int. Arch. Otorhinolaryngol. 2020, 24, 272–277. [Google Scholar] [CrossRef]
- Chan, K.-C.; Tsai, Y.-T.; Yang, Y.-H.; Chen, P.-C.; Chang, P.-H. Osteoporosis is associated with increased risk for benign paroxysmal positional vertigo: A nationwide population-based study. Arch. Osteoporos. 2017, 12, 106. [Google Scholar] [CrossRef]
- Choi, H.G.; Lee, J.K.; Kong, I.G.; Lim, H.; Kim, S.Y. Osteoporosis increases the risk of benign paroxysmal positional vertigo: A nested case–control study using a national sample cohort. Eur. Arch. Oto-Rhino-Laryngol. 2019, 276, 335–342. [Google Scholar] [CrossRef]
- Kim, S.Y.; Kim, H.-J.; Min, C.; Choi, H.G. Association between benign paroxysmal positional vertigo and osteoporosis: Two nested case-control studies. Osteoporos. Int. 2020, 31, 2017–2024. [Google Scholar] [CrossRef]
- Liao, W.-L.; Chang, T.-P.; Chen, H.-J.; Kao, C.-H. Benign paroxysmal positional vertigo is associated with an increased risk of fracture: A population-based cohort study. J. Orthop. Sports Phys. Ther. 2015, 45, 406–412. [Google Scholar] [CrossRef]
- Sen, K.; Padiyar, B.V.; Arora, G. Association of Benign Paroxysmal Positional Vertigo with Osteoporosis and Vitamin D Deficiency—A Case-Control Study. Dubai Med. J. 2019, 1, 2–5. [Google Scholar] [CrossRef]
- Wu, Y.; Fan, Z.; Jin, H.; Guan, Q.; Zhou, M.; Lu, X.; Li, L.; Yan, W.; Gu, C.; Chen, C.; et al. Assessment of bone metabolism in male patients with benign paroxysmal positional vertigo. Front. Neurol. 2018, 9, 742. [Google Scholar] [CrossRef]
- Wu, Y.; Gu, C.; Han, W.; Lu, X.; Chen, C.; Fan, Z. Reduction of bone mineral density in native Chinese female idiopathic benign paroxysmal positional vertigo patients. Am. J. Otolaryngol.-Head Neck Med. Surg. 2018, 39, 31–33. [Google Scholar] [CrossRef]
- Yang, C.J.; Kim, Y.; Lee, H.S.; Park, H.J. Bone mineral density and serum 25-hydroxyvitamin D in patients with idiopathic benign paroxysmal positional vertigo. J. Vestib. Res. Equilib. Orientat. 2018, 27, 287–294. [Google Scholar] [CrossRef]
- Akkawi, I.; Zmerly, H. Osteoporosis: Current Concepts. Joints 2018, 6, 122–127. [Google Scholar] [CrossRef]
- Labuguen, R.H. Initial evaluation of vertigo. Am. Fam. Physician 2006, 73, 244–251. [Google Scholar]
- Neuhauser, H.K.; Lempert, T. Vertigo: Epidemiologic aspects. Semin. Neurol. 2009, 29, 473–481. [Google Scholar] [CrossRef]
- Oghalai, J.S.; Manolidis, S.; Barth, J.L.; Stewart, M.G.; Jenkins, H.A. Unrecognized benign paroxysmal positional vertigo in elderly patients. Otolaryngol. Head Neck Surg. 2000, 122, 630–634. [Google Scholar] [CrossRef]
- De Stefano, A.; Dispenza, F.; Suarez, H.; Perez-Fernandez, N.; Manrique-Huarte, R.; Ban, J.H.; Kim, M.B.; Strupp, M.; Feil, K.; Oliveira, C.A.; et al. A multicenter observational study on the role of comorbidities in the recurrent episodes of benign paroxysmal positional vertigo. Auris Nasus Larynx 2014, 41, 31–36. [Google Scholar] [CrossRef]
- Lee, S.H.; Kim, M.K.; Cho, K.H.; Kim, J.S. Reversal of initial positioning nystagmus in benign paroxysmal positional vertigo involving the horizontal canal. Ann. N. Y. Acad. Sci. 2009, 1164, 406–408. [Google Scholar] [CrossRef]
- Kim, J.-S.; Zee, D.S. Clinical practice. Benign paroxysmal positional vertigo. N. Engl. J. Med. 2014, 370, 1138–1147. [Google Scholar] [CrossRef] [PubMed]
- Parham, K.; Kuchel, G.A. A Geriatric Perspective on Benign Paroxysmal Positional Vertigo. J. Am. Geriatr. Soc. 2016, 64, 378–385. [Google Scholar] [CrossRef] [PubMed]
- Barnsley, J.; Buckland, G.; Chan, P.E.; Ong, A.; Ramos, A.S.; Baxter, M.; Laskou, F.; Dennison, E.M.; Cooper, C.; Patel, H.P. Pathophysiology and treatment of osteoporosis: Challenges for clinical practice in older people. Aging Clin. Exp. Res. 2021, 33, 759–773. [Google Scholar] [CrossRef] [PubMed]
- Ji, M.X.; Yu, Q. Primary osteoporosis in postmenopausal women. Chronic Dis. Transl. Med. 2015, 1, 9–13. [Google Scholar] [CrossRef]
- Juneja, M.K.; Munjal, S.; Sharma, A.; Gupta, A.K.; Bhadada, S. Audiovestibular functioning of post-menopausal females with osteoporosis and osteopenia. J. Otol. 2021, 16, 27–33. [Google Scholar] [CrossRef]
- Yang, K.; Qiu, X.; Cao, L.; Qiu, S. The role of melatonin in the development of postmenopausal osteoporosis. Front. Pharmacol. 2022, 13, 975181. [Google Scholar] [CrossRef]
- Baytaroglu, B.; Jafarov, S.; Erbek, S.S. The Effect of Postmenopausal Osteoporosis on Middle Ear Resonance Frequency. J. Int. Adv. Otol. 2021, 17, 526–529. [Google Scholar] [CrossRef]
- Lee, S.B.; Lee, C.H.; Kim, Y.J.; Kim, H.-M. Biochemical markers of bone turnover in benign paroxysmal positional vertigo. PLoS ONE 2017, 12, e0176011. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author (year) | Study Design | Country | Sample Size (n) | Characteristics of Control Participants in the Control Group | Mean Age | Female Sex | Diagnosis of BPPV | Subtypes of BPPV | Diagnosis of Osteoporosis | T-Score | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| BPPV Group | Control Group | Years | % | ||||||||
| Bazoni JA et al. (2020) [17] | PCS | Brazil | 17 | 92 | Volunteers of age ≥ 60, both genders | BPPV: 67.0 Control: 68.0 | BPPV: 88.2 Control: 58.7 | Vertigo complaints, audiological anamnesis, and D–H maneuver | N/A | BMD | N/A |
| Byun H et al. (2019) [4] | RCS | Republic of Korea | 7765 | 347,829 | Matched for age, sex, social status, HTN, and DM | 64.5 | BPPV: 91.2 Control: 91.2 | ICD-10 code | N/A | DXA, qCT, peripheral DXA, and qUS | N/A |
| Chan KC et al. (2017) [18] | RCS | Taiwan | 209 | 33,036 | Matched for age and gender | >20 | BPPV: 88.4 Control: 88.4 | ICD-9 code | N/A | DXA | N/A |
| Choi HG et al. (2019) [19] | RCS | Republic of Korea | 13,484 | 53,936 | Matched for age, sex, socioeconomic status, HTN, DM, and dyslipidemia | ≥50 | BPPV: 69.8 Control: 69.8 | ICD-10 code | N/A | DXA and qCT | N/A |
| Jeong SH et al. (2009) [6] | PCS | Republic of Korea | 209 | 202 | Volunteers without dizziness and VCF Hx | BPPV: 59.8 Control: 56.3 | BPPV: 67.9 Control: 47.5 | Vertigo complaints, typical positioning nystagmus, and no other CNS disorders | Horizontal canal, posterior canal, and anterior canal | DXA (LUNAR); T-score ≤ −2.5 from lumbar or femoral areas (WHO definition) | BPPV: −1.7 (female); −1.1 (male). Control: −1.0 (female); −0.7 (male). |
| Kim SY et al. (2020) [20] | RCS | Republic of Korea | 9621 | 38,484 | Matched for age, sex, income, and region of residence | >40 | BPPV: 62.6 Control: 62.6 | ICD-10 code | N/A | DXA and qCT | N/A |
| Liao WL et al. (2015) [21] | RCS | Taiwan | 644 | 2160 | Matched for age and sex; without vertigo Hx | BPPV: 57.1 Control: 56.7 | BPPV: 63.5 Control: 63.5 | ICD-9 code | N/A | N/A (ICD-9 code) | N/A |
| Mikulec AA et al. (2010) [7] | RCS | U.S. | 143 | 117 | Patients without BPPV who visited two otology clinics | 51–80 | 100 | Clinical evaluation; videonystagmography testing | N/A | N/A | N/A |
| Sen K et al. (2019) [22] | PCS | India | 100 | 100 | Healthy volunteers who want to screen for osteoporosis | BPPV: 48.6 Control: 46.2 | BPPV: 68.0 Control: 58.0 | D-H maneuver, P-M maneuver, cephalic hyperextension, and audiological assessment | N/A | DXA (T-score ≤ −2.5 from the lumbar or femoral areas) | BPPV: −2.6. Control: −1.8. |
| Wu Y et al. (2018) [23] | RCS | China | 60 | 92 | Matched for age; healthy controls without vertigo/dizziness history | BPPV: 59.4 Control: 62.1 | 0 | Vertigo complaints, D-H maneuver, and supine roll test | N/A | DXA (LUNAR); T-score ≤ −2.5 from lumbar or femoral areas (WHO definition) | BPPV: 1.101 (spine); 0.966 (hip). Control: 1.128 (spine); 1.000 (hip). |
| Wu Y et al. (2018) [24] | RCS | China | 78 | 126 | Matched for age; healthy controls without vertigo/dizziness history | BPPV: 58.4 Control: 58.5 | 100 | Vertigo complaints, D-H maneuver, and supine roll test | Horizontal canal; posterior canal | DXA (LUNAR); T-score ≤ −2.5 from lumbar or femoral areas (WHO definition) | BPPV: −0.11 to −2.42 (spine); −0.04 to −1.73 (hip). Control: 0.70 to −1.45 (spine); 0.36 to 0.96 (hip). |
| Yang CJ et al. (2018) [25] | RCS | Republic of Korea | 130 | 130 | Matched for age and sex; healthy controls without dizziness or fracture Hx | 54.9 | BPPV: 76.9 Control: 76.9 | Vertigo complaints; D-H maneuver | N/A | DXA (LUNAR); T-score ≤ −2.5 from lumbar or femoral areas (WHO definition) | BPPV: −1.6 (female); −0.9 (male). Control: −1.1 (female); −0.7 (male). |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, C.-H.; Kim, K.; Choi, Y. Do Patients with Benign Paroxysmal Positional Vertigo Have a Higher Prevalence of Osteoporosis? A Systematic Review and Meta-Analysis. J. Pers. Med. 2024, 14, 303. https://doi.org/10.3390/jpm14030303
Kim C-H, Kim K, Choi Y. Do Patients with Benign Paroxysmal Positional Vertigo Have a Higher Prevalence of Osteoporosis? A Systematic Review and Meta-Analysis. Journal of Personalized Medicine. 2024; 14(3):303. https://doi.org/10.3390/jpm14030303
Chicago/Turabian StyleKim, Chul-Ho, Keunho Kim, and Yeonjoo Choi. 2024. "Do Patients with Benign Paroxysmal Positional Vertigo Have a Higher Prevalence of Osteoporosis? A Systematic Review and Meta-Analysis" Journal of Personalized Medicine 14, no. 3: 303. https://doi.org/10.3390/jpm14030303
APA StyleKim, C.-H., Kim, K., & Choi, Y. (2024). Do Patients with Benign Paroxysmal Positional Vertigo Have a Higher Prevalence of Osteoporosis? A Systematic Review and Meta-Analysis. Journal of Personalized Medicine, 14(3), 303. https://doi.org/10.3390/jpm14030303