
Psoriasis and Fibromyalgia: A Systematic Review

 , , ,
, , ,  , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Eligibility Criteria
- -
- Population: adult patients diagnosed with FM or PsO;
- -
- Intervention: not applicable;
- -
- Comparison: healthy controls or no control group;
- -
- Outcome:
- Studies assessing the prevalence of PsO in FM patients.
- Studies assessing the prevalence of FM in PsO patients.
- Studies assessing the association between severity of FM clinical features (composite measures of symptoms severity, pain, tender point count, stiffness, fatigue, physical functioning, sleep, depression, anxiety, cognitive dysfunction, QoL) and outcomes measures in PsO and vice versa.
2.3. Study Selection Process and Data Extraction
2.4. Quality Assessment
3. Results
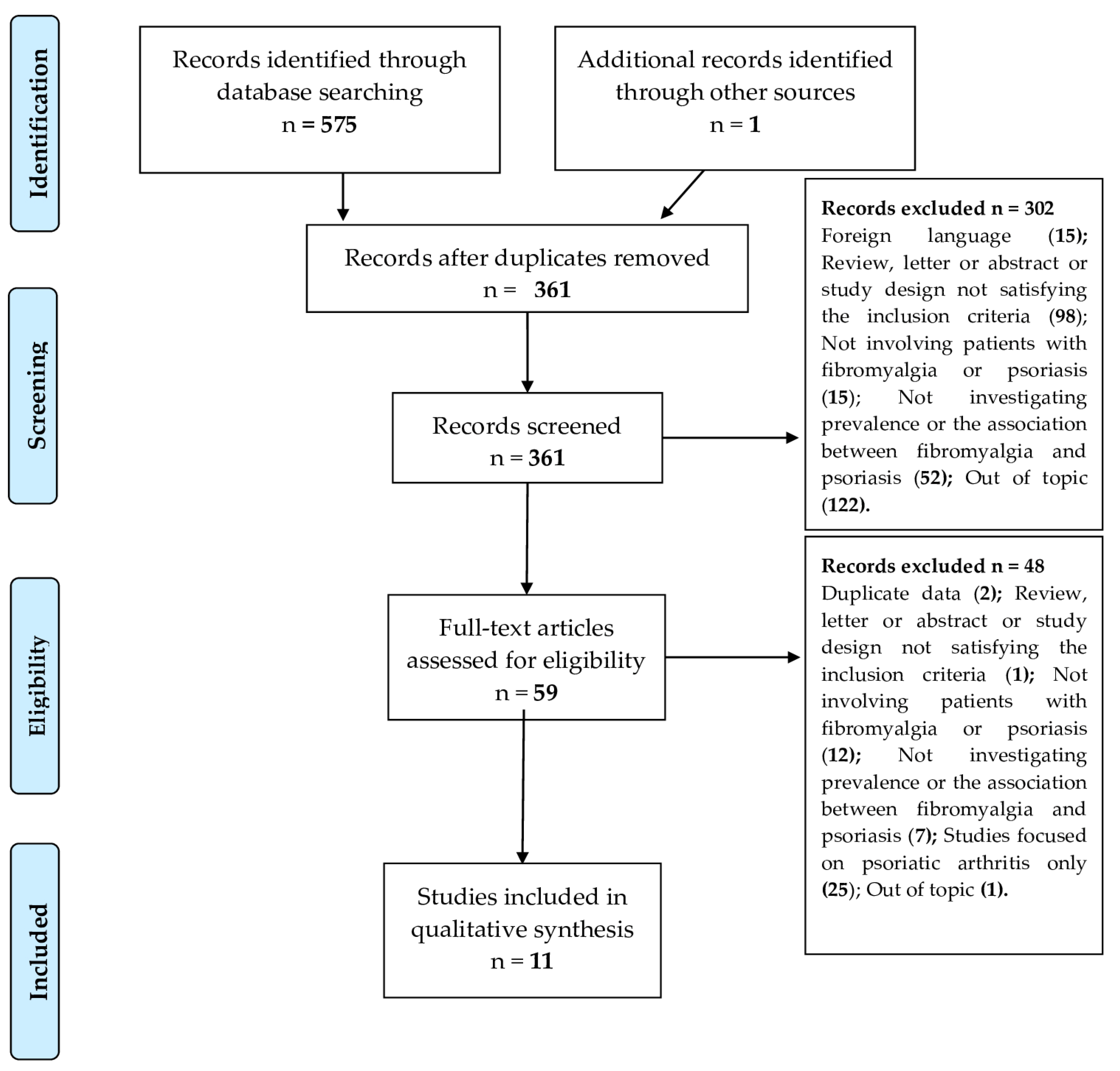
3.1. Results of the Systematic Search
3.2. FM in PsO Patients: Higher Prevalence and Impact on Outcome Measures
3.3. PsO in FM Patients: A Controversial Association
3.4. FM in PsA Patients: Results on PsO Outcome Measures
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bair, M.J.; Krebs, E.E. Fibromyalgia. Ann. Intern. Med. 2020, 172, 33–48. [Google Scholar] [CrossRef]
- Sarzi-Puttini, P.; Giorgi, V.; Marotto, D.; Atzeni, F. Fibromyalgia: An update on clinical characteristics, aetiopathogenesis and treatment. Nat. Rev. Rheumatol. 2020, 16, 645–660. [Google Scholar] [CrossRef]
- D’Onghia, M.; Ciaffi, J.; Ruscitti, P.; Cipriani, P.; Giacomelli, R.; Ablin, J.N.; Ursini, F. The economic burden of fibromyalgia: A systematic literature review. Semin. Arthritis Rheum. 2022, 56, 152060. [Google Scholar] [CrossRef]
- Siracusa, R.; Paola, R.D.; Cuzzocrea, S.; Impellizzeri, D. Fibromyalgia: Pathogenesis, Mechanisms, Diagnosis and Treatment Options Update. Int. J. Mol. Sci. 2021, 22, 3891. [Google Scholar] [CrossRef]
- Fitzcharles, M.A.; Perrot, S.; Hauser, W. Comorbid fibromyalgia: A qualitative review of prevalence and importance. Eur. J. Pain. 2018, 22, 1565–1576. [Google Scholar] [CrossRef] [PubMed]
- Duffield, S.J.; Miller, N.; Zhao, S.; Goodson, N.J. Concomitant fibromyalgia complicating chronic inflammatory arthritis: A systematic review and meta-analysis. Rheumatology 2018, 57, 1453–1460. [Google Scholar] [CrossRef]
- FitzGerald, O.; Ogdie, A.; Chandran, V.; Coates, L.C.; Kavanaugh, A.; Tillett, W.; Leung, Y.Y.; deWit, M.; Scher, J.U.; Mease, P.J. Psoriatic arthritis. Nat. Rev. Dis. Primers 2021, 7, 59. [Google Scholar] [CrossRef]
- Cigolini, C.; Fattorini, F.; Gentileschi, S.; Terenzi, R.; Carli, L. Psoriatic arthritis: One year in review 2022. Clin. Exp. Rheumatol. 2022, 40, 1611–1619. [Google Scholar] [CrossRef] [PubMed]
- Veale, D.J.; Fearon, U. The pathogenesis of psoriatic arthritis. Lancet 2018, 391, 2273–2284. [Google Scholar] [CrossRef] [PubMed]
- Conaghan, P.G.; Alten, R.; Deodhar, A.; Sullivan, E.; Blackburn, S.; Tian, H.; Gandhi, K.; Jugl, S.M.; Strand, V. Relationship of pain and fatigue with health-related quality of life and work in patients with psoriatic arthritis on TNFi: Results of a multi-national real-world study. RMD Open 2020, 6, e001240. [Google Scholar] [CrossRef]
- Marchesoni, A.; De Marco, G.; Merashli, M.; McKenna, F.; Tinazzi, I.; Marzo-Ortega, H.; McGonagle, D.G. The problem in differentiation between psoriatic-related polyenthesitis and fibromyalgia. Rheumatology 2018, 57, 32–40. [Google Scholar] [CrossRef]
- Skoie, I.; Dalen, I.; Ternowitz, T.; Jonsson, G.; Kvivik, I.; Norheim, K.; Omdal, R. Fatigue in psoriasis: A controlled study. Br. J. Dermatol. 2017, 177, 505–512. [Google Scholar] [CrossRef]
- Jensen, P.; Zachariae, C.; Skov, L.; Zachariae, R. Sleep disturbance in psoriasis: A case-controlled study. Br. J. Dermatol. 2018, 179, 1376–1384. [Google Scholar] [CrossRef] [PubMed]
- Gisondi, P.; Sala, F.; Alessandrini, F.; Avesani, V.; Zoccatelli, G.; Beltramello, A.; Moretto, G.; Gambina, G.; Girolomoni, G. Mild cognitive impairment in patients with moderate to severe chronic plaque psoriasis. Dermatology 2014, 228, 78–85. [Google Scholar] [CrossRef]
- Kim, S.H. Skin biopsy findings: Implications for the pathophysiology of fibromyalgia. Med. Hypotheses 2007, 69, 141–144. [Google Scholar] [CrossRef] [PubMed]
- Blanco, I.; Béritze, N.; Argüelles, M.; Cárcaba, V.; Fernández, F.; Janciauskiene, S.; Oikonomopoulou, K.; de Serres, F.J.; Fernández-Bustillo, E.; Hollenberg, M.D. Abnormal overexpression of mastocytes in skin biopsies of fibromyalgia patients. Clin. Rheumatol. 2010, 29, 1403–1412. [Google Scholar] [CrossRef] [PubMed]
- Salemi, S.; Rethage, J.; Wollina, U.; Michel, B.A.; Gay, R.E.; Gay, S.; Sprott, H. Detection of interleukin 1beta (IL-1beta), IL-6, and tumor necrosis factor-alpha in skin of patients with fibromyalgia. J. Rheumatol. 2003, 30, 146–150. [Google Scholar]
- Sprott, H.; Müller, A.; Heine, H. Collagen cross-links in fibromyalgia syndrome. Z. Rheumatol. 1998, 57, S52–S55. [Google Scholar] [CrossRef]
- Greb, J.E.; Goldminz, A.M.; Elder, J.T.; Lebwohl, M.G.; Gladman, D.D.; Wu, J.J.; Mehta, N.N.; Finlay, A.Y.; Gottlieb, A.B. Psoriasis. Nat. Rev. Dis. Primers 2016, 2, 16082. [Google Scholar] [CrossRef]
- Meneguin, S.; de Godoy, N.A.; Pollo, C.F.; Miot, H.A.; de Oliveira, C. Quality of life of patients living with psoriasis: A qualitative study. BMC Dermatol. 2020, 20, 22. [Google Scholar] [CrossRef]
- Boehncke, W.H.; Schön, M.P. Psoriasis. Lancet 2015, 386, 983–994. [Google Scholar] [CrossRef]
- Takeshita, J.; Grewal, S.; Langan, S.M.; Mehta, N.N.; Ogdie, A.; Van Voorhees, A.S.; Gelfand, J.M. Psoriasis and comorbid diseases: Epidemiology. J. Am. Acad. Dermatol. 2017, 76, 377–390. [Google Scholar] [CrossRef] [PubMed]
- De Simone, C.; Calabrese, L.; Balato, A.; Cannavò, S.P.; Dattola, A.; Esposito, M.; Fargnoli, M.C.; Giuffrida, R.; Hansel, K.; Musumeci, M.L.; et al. “Psoriasis in Women of Childbearing Age” Task Force. Psoriasis and its management in women of childbearing age: Tools to increase awareness in dermatologists and patients. G. Ital. Dermatol. Venereol. 2020, 155, 434–440. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. Ann. Intern. Med. 2009, 151, 65–94. [Google Scholar] [CrossRef] [PubMed]
- Wells, A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. 2013. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 27 November 2023).
- Kridin, K.; Vanetik, S.; Damiani, G.; Cohen, A.D. Big data highlights the association between psoriasis and fibromyalgia: A population-based study. Immunol. Res. 2020, 68, 135–140. [Google Scholar] [CrossRef] [PubMed]
- Brikman, S.; Furer, V.; Wollman, J.; Borok, S.; Matz, H.; Polachek, A.; Elalouf, O.; Sharabi, A.; Kaufman, I.; Paran, D.; et al. The Effect of the Presence of Fibromyalgia on Common Clinical Disease Activity Indices in Patients with Psoriatic Arthritis: A Cross-sectional Study. J. Rheumatol. 2016, 43, 1749–1754. [Google Scholar] [CrossRef]
- Elsawy, N.A.; Helal, A.H.; Abd ElHamid, H.A.; Abdel-Fattah, Y.H. Fibromyalgia in patients with psoriatic arthritis: Impact on disease activity indices, fatigue and health-related quality of life. Int. J. Rheum. Dis. 2021, 24, 189–196. [Google Scholar] [CrossRef] [PubMed]
- Erdogan, H.K.; Sas, S.; Acer, E.; Bulur, I.; Altunay, I.K.; Erdem, H.R. Cutaneous findings in fibromyalgia syndrome and their effect on quality of life. Dermatol. Sinica 2016, 34, 131–134. [Google Scholar] [CrossRef]
- Iannone, F.; Nivuori, M.; Fornaro, M.; Venerito, V.; Cacciapaglia, F.; Lopalco, G. Comorbid fibromyalgia impairs the effectiveness of biologic drugs in patients with psoriatic arthritis. Rheumatology 2020, 59, 1599–1606. [Google Scholar] [CrossRef]
- Kancharla, H.; Jain, S.; Mishra, S.; Acharya, N.; Grover, S.; Dogra, S.; Sharma, A. Fibromyalgia influences health-related quality of life and disease activity in psoriatic arthritis. Rheumatol. Int. 2022, 42, 511–517. [Google Scholar] [CrossRef]
- Laniosz, V.; Wetter, D.A.; Godar, D.A. Dermatologic manifestations of fibromyalgia. Clin. Rheumatol. 2014, 33, 1009–1013. [Google Scholar] [CrossRef] [PubMed]
- Mohammed, J.Q.; Mathkhor, A.J.; Abdullah, A.H.; Khudhairy, A.S.; Nasrullah, H.H. Fibromyalgia in patients with psoriasis. World Fam. Med. 2020, 18, 45–49. [Google Scholar] [CrossRef]
- Polachek, A.; Furer, V.; Zureik, M.; Nevo, S.; Mendel, L.; Levartovsky, D.; Wollman, J.; Aloush, V.; Tzemach, R.; Elalouf, O.; et al. Role of ultrasound for assessment of psoriatic arthritis patients with fibromyalgia. Ann. Rheum. Dis. 2021, 80, 1553–1558. [Google Scholar] [CrossRef] [PubMed]
- Thune, P.O. The prevalence of fibromyalgia among patients with psoriasis. Acta Derm. Venereol. 2005, 85, 33–37. [Google Scholar] [CrossRef] [PubMed]
- Ulus, Y.; Akyol, Y.; Bilgici, A.; Kuru, O. The impact of the presence of fibromyalgia on fatigue in patients with psoriatic arthritis: Comparison with controls. Adv. Rheumatol. 2019, 60, 1. [Google Scholar] [CrossRef] [PubMed]
- Wolfe, F.; Smythe, H.A.; Yunus, M.B.; Bennett, R.M.; Bombardier, C.; Goldenberg, D.L.; Tugwell, P.; Campbell, S.M.; Abeles, M.; Clark, P.; et al. The American College of Rheumatology 1990 Criteria for the Classification of Fibromyalgia. Report of the Multicenter Criteria Committee. Arthritis Rheumatol. 1990, 33, 160–172. [Google Scholar] [CrossRef]
- Icen, M.; Crowson, C.S.; McEvoy, M.T.; Dann, F.J.; Gabriel, S.E.; Kremers, H.M. Trends in incidence of adult-onset psoriasis over three decades: A population-based study. J. Am. Acad. Dermatol. 2009, 60, 394–401. [Google Scholar] [CrossRef]
- Moller, A.H.; Erntoft, S.; Vinding, G.R.; Jemec, G.B. A systematic literature review to compare quality of life in psoriasis with other chronic diseases using EQ-5D-derived utility values. Patient Relat. Outcome Meas. 2015, 6, 167–177. [Google Scholar]
- Kim, N.; Thrash, B.; Menter, A. Comorbidities in psoriasis patients. Semin. Cutan. Med. Surg. 2010, 29, 10–15. [Google Scholar] [CrossRef]
- Felbo, S.; Terslev, L.; Sørensen, I.; Skov, L.; Zachariae, C.; Østergaard, M. Musculoskeletal Pain in Patients with Psoriasis and its Influence on Health-related Quality of Life: Results from a Danish Population-based Survey. Acta Derm. Venereol. 2021, 101, adv00553. [Google Scholar] [CrossRef]
- Cohen, H. Controversies and challenges in fibromyalgia: A review and a proposal. Ther. Adv. Musculoskelet. Dis. 2017, 9, 115–127. [Google Scholar] [CrossRef]
- Ljosaa, T.; Rustoen, T.; Mørk, C.; Stubhaug, A.; Miaskowski, C.; Paul, S.; Wahl, A. Skin pain and discomfort in psoriasis: An exploratory study of symptom prevalence and characteristics. Acta Derm. Venereol. 2010, 90, 39–45. [Google Scholar] [CrossRef]
- Patruno, C.; Napolitano, M.; Balato, N.; Ayala, F.; Megna, M.; Patrì, A.; Cirillo, T.; Balato, A. Psoriasis and skin pain: Instrumental and biological evaluations. Acta Derm. Venereol. 2015, 95, 432–438. [Google Scholar] [CrossRef]
- Ayasse, M.T.; Buddenkotte, J.; Alam, M.; Steinhoff, M. Role of neuroimmune circuits and pruritus in psoriasis. Exp. Dermatol. 2020, 29, 414–426. [Google Scholar] [CrossRef]
- Latremoliere, A.; Woolf, C.J. Central sensitization: A generator of pain hypersensitivity by central neural plasticity. J. Pain. 2009, 10, 895–926. [Google Scholar] [CrossRef]
- Lluch Girbes, E.; Nijs, J.; Torres-Cueco, R.; López Cubas, C. Pain treatment for patients with osteoarthritis and central sensitization. Phys. Ther. 2013, 93, 842–851. [Google Scholar] [CrossRef]
- Russell, I.J.; Orr, M.D.; Littman, B.; Vipraio, G.A.; Alboukrek, D.; Michalek, J.E.; Lopez, Y.; Mackillip, F. Elevated cerebrospinal fluid levels of substance P in patients with the fibromyalgia syndrome. Arthritis Rheumatol. 1994, 37, 1593–1601. [Google Scholar] [CrossRef]
- Nakamura, M.; Toyoda, M.; Morohashi, M. Pruritogenic mediators in psoriasis vulgaris: Comparative evaluation of itch-associated cutaneous factors. Br. J. Dermatol. 2003, 149, 718–730. [Google Scholar] [CrossRef] [PubMed]
- O’Mahony, L.F.; Srivastava, A.; Mehta, P.; Ciurtin, C. Is fibromyalgia associated with a unique cytokine profile? A systematic review and meta-analysis. Rheumatology 2021, 60, 2602–2614. [Google Scholar] [CrossRef] [PubMed]
- Coimbra, S.; Oliveira, H.; Reis, F.; Belo, L.; Rocha, S.; Quintanilha, A.; Figueiredo, A.; Teixeira, F.; Castro, E.; Rocha-Pereira, P.; et al. Interleukin (IL)-22, IL-17, IL-23, IL-8, vascular endothelial growth factor and tumour necrosis factor-alpha levels in patients with psoriasis before, during and after psoralen-ultraviolet A and narrowband ultraviolet B therapy. Br. J. Dermatol. 2010, 163, 1282–1290. [Google Scholar] [CrossRef] [PubMed]
- Singh, R.; Koppu, S.; Perche, P.O.; Feldman, S.R. The Cytokine Mediated Molecular Pathophysiology of Psoriasis and Its Clinical Implications. Int. J. Mol. Sci. 2021, 22, 12793. [Google Scholar] [CrossRef] [PubMed]
- Tsilioni, I.; Russell, I.J.; Stewart, J.M.; Gleason, R.M.; Theoharides, T.C. Neuropeptides CRH, SP, HK-1, and Inflammatory Cytokines IL-6 and TNF Are Increased in Serum of Patients with Fibromyalgia Syndrome, Implicating Mast Cells. J. Pharmacol. Exp. Ther. 2016, 356, 664–672. [Google Scholar] [CrossRef] [PubMed]
- Theoharides, T.C.; Tsilioni, I.; Bawazeer, M. Mast Cells, Neuroinflammation and Pain in Fibromyalgia Syndrome. Front. Cell Neurosci. 2019, 13, 353. [Google Scholar] [CrossRef] [PubMed]
- Totsch, S.K.; Sorge, R.E. Immune System Involvement in Specific Pain Conditions. Mol. Pain 2017, 13, 1744806917724559. [Google Scholar] [CrossRef] [PubMed]
- Ohgidani, M.; Kato, T.A.; Hosoi, M.; Tsuda, M.; Hayakawa, K.; Hayaki, C.; Iwaki, R.; Sagata, N.; Hashimoto, R.; Inoue, K.; et al. Fibromyalgia and microglial TNF-α: Translational research using human blood induced microglia-like cells. Sci. Rep. 2017, 7, 11882. [Google Scholar] [CrossRef] [PubMed]
- Pernambuco, A.P.; Schetino, L.P.; Alvim, C.C.; Murad, C.M.; Viana, R.S.; Carvalho, L.S.; Reis, D.Á. Increased levels of IL-17A in patients with fibromyalgia. Clin. Exp. Rheumatol. 2013, 31 (Suppl. S79), S60–S63. [Google Scholar] [PubMed]
- Blauvelt, A.; Chiricozzi, A. The Immunologic Role of IL-17 in Psoriasis and Psoriatic Arthritis Pathogenesis. Clin. Rev. Allergy Immunol. 2018, 55, 379–390. [Google Scholar] [CrossRef]
- Peck, M.M.; Maram, R.; Mohamed, A.; Ochoa Crespo, D.; Kaur, G.; Ashraf, I.; Malik, B.H. The Influence of Pro-inflammatory Cytokines and Genetic Variants in the Development of Fibromyalgia: A Traditional Review. Cureus 2020, 12, e10276. [Google Scholar] [CrossRef]
- Vincent, A.; Benzo, R.P.; O Whipple, M.; McAllister, S.J.; Erwin, P.J.; Saligan, L.N. Beyond pain in fibromyalgia: Insights into the symptom of fatigue. Arthritis Res. Ther. 2013, 15, 221. [Google Scholar] [CrossRef]
- Zambolin, F.; Duro-Ocana, P.; Faisal, A.; Bagley, L.; Gregory, W.J.; Jones, A.W.; McPhee, J.S. Fibromyalgia and Chronic Fatigue Syndromes: A systematic review and meta-analysis of cardiorespiratory fitness and neuromuscular function compared with healthy individuals. PLoS ONE 2022, 17, e0276009. [Google Scholar] [CrossRef]
- Tsai, S.-Y.; Chen, H.-J.; Chen, C.; Lio, C.-F.; Kuo, C.-F.; Leong, K.-H.; Wang, Y.-T.T.; Yang, T.-Y.; You, C.-H.; Wang, W.-S. Increased risk of chronic fatigue syndrome following psoriasis: A nationwide population-based cohort study. J. Transl. Med. 2019, 17, 154. [Google Scholar] [CrossRef]
- Brenu, E.W.; Huth, T.K.; Hardcastle, S.L.; Fuller, K.; Kaur, M.; Johnston, S.; Ramos, S.B.; Staines, D.R.; Marshall-Gradisnik, S.M. Role of adaptive and innate immune cells in chronic fatigue syndrome/myalgic encephalomyelitis. Int. Immunol. 2014, 26, 233–242. [Google Scholar] [CrossRef]
- Dantzer, R.; Kelley, K.W. Twenty years of research on cytokine-induced sickness behavior. Brain Behav. Immun. 2007, 21, 153–160. [Google Scholar] [CrossRef]
- Bigatti, S.M.; Hernandez, A.M.; Cronan, T.A.; Rand, K.L. Sleep disturbances in fibromyalgia syndrome: Relationship to pain and depression. Arthritis Rheum. 2008, 59, 961–967. [Google Scholar] [CrossRef]
- Gupta, M.A.; Simpson, F.C.; Gupta, A.K. Psoriasis and sleep disorders: A systematic review. Sleep. Med. Rev. 2016, 29, 63–75. [Google Scholar] [CrossRef] [PubMed]
- Henao-Pérez, M.; López-Medina, D.C.; Arboleda, A.; Bedoya Monsalve, S.; Zea, J.A. Patients With Fibromyalgia, Depression, and/or Anxiety and Sex Differences. Am. J. Mens. Health 2022, 16, 15579883221110351. [Google Scholar] [CrossRef] [PubMed]
- Holsken, S.; Krefting, F.; Schedlowski, M.; Sondermann, W. Common Fundamentals of Psoriasis and Depression. Acta Derm. Venereol. 2021, 101, adv00609. [Google Scholar] [CrossRef] [PubMed]
- Pinho de Oliveira Ribeiro, N.; Rafael de Mello Schier, A.; Ornelas, A.C.; Pinho de Oliveira, C.M.; Nardi, A.E.; Silva, A.C. Anxiety, depression and suicidal ideation in patients with rheumatoid arthritis in use of methotrexate, hydroxychloroquine, leflunomide and biological drugs. Compr. Psychiatry 2013, 54, 1185–1189. [Google Scholar] [CrossRef] [PubMed]
- Kunz, M.; Simon, J.C.; Saalbach, A. Psoriasis: Obesity and Fatty Acids. Front. Immunol. 2019, 10, 1807. [Google Scholar] [CrossRef] [PubMed]
- Bettelli, E.; Carrier, Y.; Gao, W.; Korn, T.; Strom, T.B.; Oukka, M.; Weiner, H.L.; Kuchroo, V.K. Reciprocal developmental pathways for the generation of pathogenic effector TH17 and regulatory T cells. Nature 2006, 441, 235–238. [Google Scholar] [CrossRef] [PubMed]
- Chehimi, M.; Vidal, H.; Eljaafari, A. Pathogenic Role of IL-17-Producing Immune Cells in Obesity, and Related Inflammatory Diseases. J. Clin. Med. 2017, 6, 68. [Google Scholar] [CrossRef]
- D’Onghia, M.; Ciaffi, J.; Lisi, L.; Mancarella, L.; Ricci, S.; Stefanelli, N.; Meliconi, R.; Ursini, F. Fibromyalgia and obesity: A comprehensive systematic review and meta-analysis. Semin. Arthritis Rheum. 2021, 51, 409–424. [Google Scholar] [CrossRef] [PubMed]
- White, K.P.; Harth, M. Classification, epidemiology, and natural history of fibromyalgia. Curr. Pain Headache Rep. 2001, 5, 320–329. [Google Scholar] [CrossRef] [PubMed]
- Parisi, R.; Symmons, D.P.; Griffiths, C.E.; Ashcroft, D.M. Identification and Management of Psoriasis and Associated ComorbidiTy (IMPACT) project team. Global epidemiology of psoriasis: A systematic review of incidence and prevalence. J. Investig. Dermatol. 2013, 133, 377–385. [Google Scholar] [CrossRef]
- Iskandar, I.Y.K.; Parisi, R.; Griffiths, C.E.M.; Ashcroft, D.M. Global Psoriasis Atlas Systematic review examining changes over time and variation in the incidence and prevalence of psoriasis by age and gender. Br. J. Dermatol. 2021, 184, 243–258. [Google Scholar] [CrossRef] [PubMed]
- Almodóvar, R.; Carmona, L.; Zarco, P.; Collantes, E.; González, C.; Mulero, J.; Sueiro, J.L.F.; Gratacós, J.; Torre-Alonso, J.C.; Juanola, X.; et al. Fibromyalgia in patients with ankylosing spondylitis: Prevalence and utility of the measures of activity, function and radiological damage. Clin. Exp. Rheumatol. 2010, 28 (Suppl. S63), S33–S39. [Google Scholar] [PubMed]
- Marchesoni, A.; Atzeni, F.; Spadaro, A.; Lubrano, E.; Provenzano, G.; Cauli, A.; Olivieri, I.; Melchiorre, D.; Salvarani, C.; Scarpa, R.; et al. Identification of the clinical features distinguishing psoriatic arthritis and fibromyalgia. J. Rheumatol. 2012, 39, 849–855. [Google Scholar] [CrossRef]
- Salaffi, F.; Sarzi-Puttini, P. Old and new criteria for the classification and diagnosis of fibromyalgia: Comparison and evaluation. Clin. Exp. Rheumatol. 2012, 30 (Suppl. S74), 3–9. [Google Scholar]

{kind=link}
| Author, Year | Item S1 | Item S2 | Item S3 | Item S4 | Item C1 | Item E1 | Item E2 | Item E3 | Score |
|---|---|---|---|---|---|---|---|---|---|
| Kridin, 2020 [26] | b * | b | a * | a * | a * | d | a * | c | ****** |
| Brinkman, 2016 [27] | a * | a * | c | c | c | b * | c | c | *** |
| Elsawy, 2021 [28] | a * | a * | c | c | c | b * | c | d | *** |
| Erdogan, 2016 [29] | a * | a * | a * | a * | a * | c | a * | c | ****** |
| Iannone, 2020 [30] | b * | c | c | c | c | a * | a * | d | *** |
| Kancharla, 2022 [31] | a * | a * | c | c | c | b * | c | d | *** |
| Laniosz, 2014 [32] | b | b | c | c | c | d | c | c | - |
| Mathkhor, 2020 [33] | a * | b | a * | a * | a * | c | a * | c | ***** |
| Polachek, 2021 [34] | a * | a * | c | c | c | b * | c | c | *** |
| Thune, 2005 [35] | a * | a * | c | c | c | b * | c | d | *** |
| Ulus, 2019 [36] | a * | b | a * | b | a * | c | a * | c | **** |
| Author, Year | Country | Recruitment | Year | Patients (% F) | Patients Age, Years, Mean (SD) | Controls (%F) | Design | FM Criteria | PsO or PsA Criteria |
|---|---|---|---|---|---|---|---|---|---|
| Thune, 2005 [35] | Norway | Consecutive outpatient | 1997–2000 | 1269 (56) PsO patients | 49.5 (12.8) | NR | Cross sectional | ACR 1990 | Clinical examination |
| Laniosz, 2014 [32] | USA | Outpatient | 2008 | 845 (90.6) FM patients | 48.9 | NR | Cross sectional | ACR 1990/ACR 2010/ACR 2011 | Clinical examination |
| Brinkman, 2016 [27] | Israel | Consecutive outpatient | 2013–2014 | 73 (57.7) PsA patients | 51.7 (13.5) | NR | Cross sectional | ACR 2010/ACR 1990 | CASPAR |
| Erdogan, 2016 [29] | Turkey | Inpatient | NR | 105(100) FM patients | 45.5 (8.7) | 105(100) | Cross sectional | ACR 2010 | Dermatological examination |
| Ulus, 2019 [36] | Turkey | Inpatient | 2017–2018 | 50 (72) PsA patients | 47 (23–64) * | NR | Cross sectional | CASPAR | ACR 2010 |
| Iannone, 2020 [30] | Italy | Outpatient | 2010–2017 | 238 (53) PsA patients | 49.2 (12) | NR | Cohort study | CASPAR | ACR 2010/ACR1990 |
| Kridin, 2020 [26] | Israel | Health Care Database | 2017 | 18,598 (91) FM patients | 56.5 (14.1) | 36,985 (91) | Cross sectional | EHR | EHR |
| Mathkhor, 2020 [33] | Iraq | Outpatient and inpatient | 2018–2020 | 70 (57) PsO patients | 50.7 (7.3) | 70 (57) | Cross sectional | ACR 1990 | Clinical examination |
| Elsawy, 2021 [28] | Egypt | Outpatient consecutive | 2017–2018 | 60 (43.3) PsA patients | 49.30 (11.69) | NR | Cross sectional | CASPAR | ACR 2016 |
| Polacheck, 2021 [34] | Israel | Consecutive outpatient | 2018–2020 | 156 (56) PsA patients | 52.7 (12.7) | NR | Cross sectional | CASPAR | ACR 2016 |
| Kancharla, 2022 [31] | India | Consecutive outpatient | 2014–2015 | 102 (50) PsA patients | 43.4 (12.4) | NR | Cross sectional | CASPAR | ACR 2010 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
D’Onghia, M.; Ursini, F.; Cinotti, E.; Calabrese, L.; Tognetti, L.; Cartocci, A.; Lazzeri, L.; Frediani, B.; Rubegni, P.; Trovato, E. Psoriasis and Fibromyalgia: A Systematic Review. J. Pers. Med. 2024, 14, 165. https://doi.org/10.3390/jpm14020165
D’Onghia M, Ursini F, Cinotti E, Calabrese L, Tognetti L, Cartocci A, Lazzeri L, Frediani B, Rubegni P, Trovato E. Psoriasis and Fibromyalgia: A Systematic Review. Journal of Personalized Medicine. 2024; 14(2):165. https://doi.org/10.3390/jpm14020165
Chicago/Turabian StyleD’Onghia, Martina, Francesco Ursini, Elisa Cinotti, Laura Calabrese, Linda Tognetti, Alessandra Cartocci, Laura Lazzeri, Bruno Frediani, Pietro Rubegni, and Emanuele Trovato. 2024. "Psoriasis and Fibromyalgia: A Systematic Review" Journal of Personalized Medicine 14, no. 2: 165. https://doi.org/10.3390/jpm14020165
APA StyleD’Onghia, M., Ursini, F., Cinotti, E., Calabrese, L., Tognetti, L., Cartocci, A., Lazzeri, L., Frediani, B., Rubegni, P., & Trovato, E. (2024). Psoriasis and Fibromyalgia: A Systematic Review. Journal of Personalized Medicine, 14(2), 165. https://doi.org/10.3390/jpm14020165