
Risk of Type 2 Diabetes in University Students at the University of Extremadura: A Cross-Sectional Study

 , , , , , , and
, , , , , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Research Design
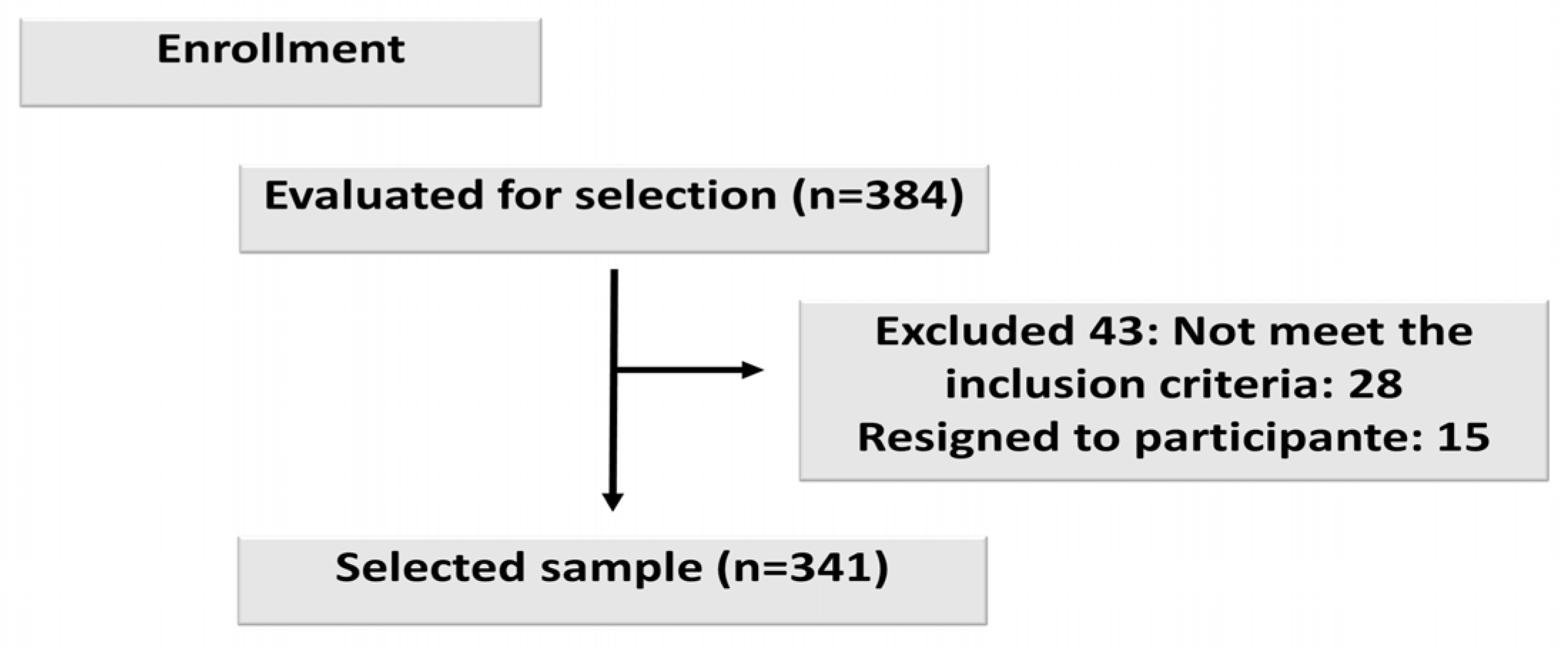
2.2. Participants
2.3. Measuring Instrument and Procedure
2.4. Statistical Analisis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Definition, Diagnosis and Classification of Diabetes Mellitus and Its Complications: Report of a WHO Consultation. Part 1: Diagnosis and Classification of Diabetes Mellitus; World Health Organization: Geneve, Switzerland, 1999. [Google Scholar]
- Extremadura Govern: Integral Plan in Extremadura. 2020–2024. Available online: https://www.fadex.org/bddocumentos/QBDTB-PIDIA-2020-2024.pdf (accessed on 28 May 2023).
- International Diabetes Federation. IDF Diabetes Atlas 2021, 10th ed.; Available online: https://diabetesatlas.org/atlas/tenth-edition/ (accessed on 28 May 2023).
- Formiga, F.; Camafort, M.; Carrasco-Sánchez, F.J. Heart failure and diabetes: The confrontation of two major epidemics of the 21st century. Rev. Clin. Esp. 2020, 220, 135–138. [Google Scholar] [CrossRef] [PubMed]
- Standl, E.; Khunti, K.; Hansen, T.B.; Schnell, O. The global epidemics of diabetes in the 21st century: Current situation and perspectives. Eur. J. Prev. Cardiol. 2019, 26, 7–14. [Google Scholar] [CrossRef]
- American Diabetes Association. Standards of Medical Care in Diabetes 2023. Diabetes Care 2023, 46, S1–S291. Available online: https://diabetesjournals.org/care/issue/46/Supplement_1 (accessed on 30 May 2023). [CrossRef] [PubMed]
- Ezkurra Loiola, P. Fundación Red GDPS. Guía de Actualización en Diabetes Mellitus Tipo 2; Euromedice Vivactis: Badalona, Spain, 2016; Available online: https://redgdps.org/gestor/upload/GUIA2016/Guia_Actualizacion_2016v2.pdf (accessed on 30 May 2023).
- Vermunt, P.W.A.; Milder, I.E.J.; Wielaard, F.; de Vries, J.H.M.; Baan, C.A.; van Oers, J.A.M.; Westert, G.P. A lifestyle intervention to reduce type 2 diabetes risk in Dutch primary care: 2.5-year results of a randomized controlled trial. Diabet. Med. 2012, 29, 223–314. [Google Scholar] [CrossRef]
- Costa, B.; Barrio, F.; Cabré, J.J.; Piñol, J.L.; Cos, X.; Solé, C.; Bolíbar, B.; Basora, J.; Castell, C.; Solà-Morales, O.; et al. Delaying progression to type 2 diabetes among high-risk Spanish individuals is feasible in real-life primary healthcare settings using intensive lifestyle intervention. Diabetologia 2012, 55, 1319–1328. [Google Scholar] [CrossRef] [PubMed]
- Balk, E.M.; Earley, A.; Raman, G.; Avendano, E.A.; Pittas, A.G.; Remington, P.L. Combined diet and physical activity promotion programs to prevent type 2 diabetes among persons at increased risk: A systematic review for the community preventive services task force. Ann. Intern. Med. 2015, 163, 437–451. [Google Scholar] [CrossRef]
- Stevens, J.W.; Khunti, K.; Harvey, R.; Johnson, M.; Preston, L.; Woods, H.B.; Davies, M.; Goyder, E. Preventing the progression to type 2 diabetes mellitus in adults at high risk: A systematic review and network meta-analysis of lifestyle, pharmacological and surgical interventions. Diabetes Res. Clin. Pract. 2015, 107, 320–331. [Google Scholar] [CrossRef]
- UK Prospective Diabetes Study (UKPDS). VIII. Study design, progress and performance. Diabetologia 1999, 34, 877–890. [Google Scholar]
- Rosenbloom, A.L.; Joe, J.R.; Young, R.S.; Winter, W.E. Emerging epidemic of type 2 diabetes in youth. Diabetes Care 1999, 22, 345–354. [Google Scholar] [CrossRef]
- Pettitt, D.J.; Talton, J.; Dabelea, D.; Divers, J.; Imperatore, G.; Lawrence, J.M.; Liese, A.D.; Linder, B.; Mayer-Davis, E.J.; Pihoker, C.; et al. Prevalence of diabetes in U.S. youth in 2009: The SEARCH for diabetes in youth study. Diabetes Care 2014, 37, 402–408. [Google Scholar] [CrossRef]
- Lawrence, J.M.; Imperatore, G.; Pettitt, D.J.; Dabelea, D.; Linder, B.; Mayer-Davis, E.J.; Isom, S.; Pihoker, C.; Standiford, D.A.; Marcovina, S.M.; et al. Incidence of diabetes in United States youth by diabetes type, race/ethnicity, and age, 2008–2009. Diabetes 2014, 63, S407. [Google Scholar]
- Bjornstad, P.; Drews, K.L.; Caprio, S.; Gubitosi-Klug, R.; Nathan, D.M.; Tesfaldet, B.; Tryggestad, J.; White, N.H.; Zeitler, P. TODAY Study Group. Long-Term Complications in Youth-Onset Type 2 Diabetes. N. Engl. J. Med. 2021, 29, 416–426. [Google Scholar]
- Ramírez-Durán, M.d.V.; Basilio-Fernández, B.; Gómez-Luque, A.; Alfageme-García, P.; Clavijo-Chamorro, M.Z.; Jiménez-Cano, V.M.; Fabregat-Fernández, J.; Robles-Alonso, V.; Hidalgo-Ruiz, S. Efficacy of an Online Educational Intervention in Reducing Body Weight in the Pre-Diabetic Population of 18–45 Years Old, a Randomized Trial Protocol. J. Pers. Med. 2022, 12, 1669. [Google Scholar] [CrossRef] [PubMed]
- Soriguer, F.; Valdés, S.; Tapia, M.J.; Esteva, I.; Ruiz De Adana, M.S.; Almaraz, M.C.; Morcillo, S.; Fuentes, E.G.; Rodríguez, F.; Rojo-Martinez, G. Validación del FINDRISC (FINnish Diabetes Risk SCore) para la predicción del riesgo de diabetes tipo 2 en una población del sur de España. Estudio Pizarra. Med. Clin. 2012, 138, 371–376. [Google Scholar] [CrossRef] [PubMed]
- García, J. Guía de Diabetes Tipo 2 Para Clínicos. Recomendaciones de la redGDPS. Fundación redGDPS. 2018. Available online: https://www.redgdps.org/guia-de-diabetes-tipo-2-para-clinicos/introduccion-20180907 (accessed on 30 May 2023).
- Franciosi, M.; De Berardis, G.; Rossi, M.C.; Sacco, M.; Belfiglio, M.; Pellegrini, F.; Tognoni, G.; Valentini, M.; Nicolucci, A. Use of the diabetes risk score for opportunistic screening of undiagnosed diabetes and impaired glucose tolerance: The IGLOO (Impaired Glucose Tolerance and Long-Term Outcomes Observational) study. Diabetes Care 2005, 28, 1187–1194. [Google Scholar] [CrossRef] [PubMed]
- Makrilakis, K.; Liatis, S.; Grammatikou, S.; Perrea, D.; Stathi, C.; Tsiligros, P.; Katsilambros, N. Validation of the Finnish diabetes risk score (FINDRISC) questionnaire for screening for undiagnosed type 2 diabetes, dysglycaemia and the metabolic syndrome in Greece. Diabetes Metab. 2011, 37, 144–151. [Google Scholar] [CrossRef]
- Costa, B.; Barrio, F.; Piñol, J.L.; Cabré, J.J.; Mundet, X.; Sagarra, R.; Salas-Salvadó, J.; Solà-Morales, O. DE-PLAN-CAT/PREDICE Research Group. Shifting from glucose diagnosis to the new HbA1c diagnosis reduces the capability of the Finnish Diabetes Risk Score (FINDRISC) to screen for glucose abnormalities within a real-life primary healthcare preventive strategy. BMC Med. 2013, 11, 45. [Google Scholar] [PubMed]
- Yildiz, T.; Zuhur, S.; Shafi Zuhur, S. Diabetes Risk Assessment and Awareness in a University Academics and Employees. Med. Bull. Sisli Etfal Hosp. 2021, 29, 524–531. [Google Scholar] [CrossRef] [PubMed]
- Vandenbroucke, J.P.; von-Elm, E.; Altman, D.G.; Gøtzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M. STROBE Initiative. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and elaboration. Int. J. Surg. 2014, 12, 1500–1524. [Google Scholar] [CrossRef] [PubMed]
- Lai, K.; Kelley, K. Accuracy in parameter estimation for ANCOVA and ANOVA contrasts: Sample size planning via narrow confidence intervals. Br. J. Math. Stat. Psychol. 2012, 65, 350–370. [Google Scholar] [CrossRef]
- Bergmann, A.; Li, J.; Wang, L.; Schulze, J.; Bornstein, S.R.; Schwarz, P.E. A simplified Finnish diabetes risk score to predict type 2 diabetes risk and disease evolution in a German population. Horm. Metab. Res. 2007, 39, 677–682. [Google Scholar] [CrossRef]
- Schwarz, P.E.; Lindström, J.; Kissimova-Scarbeck, K.; Szybinski, Z.; Barengo, N.C.; Peltonen, M.; Tuomilehto, J. DE-PLAN project. The European perspective of type 2 diabetes prevention: Diabetes in Europe—Prevention using lifestyle, physical activity and nutritional intervention (DE-PLAN) project. Exp. Clin. Endocrinol. Diabetes 2008, 116, 167–172. [Google Scholar] [CrossRef]
- Schwarz, P.E.; Gruhl, U.; Bornstein, S.R.; Landgraf, R.; Hall, M.; Tuomilehto, J. The European Perspective on Diabetes Prevention: Development and Implementation of An European Guideline and training standards for diabetes prevention (IMAGE). Diab. Vasc. Dis. Res. 2007, 4, 353–357. [Google Scholar] [CrossRef]
- Bayındır Çevik, A.; Metin Karaaslan, M.; Koçan, S.; Pekmezci, H.; Baydur Şahin, S.; Kırbaş, A.; Ayaz, T. Prevalence and screening for risk factors of type 2 diabetes in Rize, Nourtheast Turkey: Findings from a population-based study. Prim. Care Diabetes 2016, 10, 10–18. [Google Scholar] [CrossRef]
- Ephraim, R.K.D.; Owusu, V.B.; Asiamah, J.; Mills, A.; Abaka-Yawson, A.; Kpene, G.E.; Kwadzokpui, P.K.; Adusei, S. Predicting type 2 diabetes mellitus among fishermen in Cape Coast: A comparison between the FINDRISC score and the metabolic syndrome. J. Diabetes Metab. Disord. 2020, 19, 1317–1324. [Google Scholar] [CrossRef]
- Meijnikman, A.S.; De Block, C.E.M.; Verrijken, A.; Mertens, I.; Van Gaal, L.F. Predicting type 2 diabetes mellitus: A comparison between the FINDRISC score and the metabolic syndrome. Diabetol. Metab. Syndr. 2018, 1, 10–12. [Google Scholar] [CrossRef]
- International Diabetes Federation. IDF Diabetes Atlas, 10th ed.; International Diabetes Federation: Brussels, Belgium, 2022. [Google Scholar]
- American Diabetes Association. Prevention or delay o diabetes and associated comorbidities: Standars of care in diabetes 2024. Diabetes Care 2024, 47, S43–S51. Available online: https://diabetesjournals.org/care/article/47/Supplement_1/S43/153945/3-Prevention-or-Delay-of-Diabetes-and-Associated (accessed on 11 January 2024). [CrossRef]
- 2018 Physical Activity Guidelines Advisory Committee. 2018 Physical Activity Guidelines Advisory Committee Scientific Report; Department of Health and Human Services: Washington, DC, USA, 2018. Available online: https://health.gov/sites/default/files/2019-09/PAG_Advisory_Committee_Report.pdf (accessed on 11 January 2024).
- Afshin, A.; Forouzanfar, M.H.; Reitsma, M.B.; Sur, P.; Estep, K.; Lee, A. Health Effects of Overweight and Obesity in 195 Countries over 25 Years. N. Engl. J. Med. 2017, 377, 13–27. [Google Scholar]
- Sonmez, A.; Yumuk, V.; Haymana, C.; Demirci, I.; Barcin, C.; Kıyıcı, S.; Güldiken, S.; Örük, G.; Saydam, B.O.; Baldane, S.; et al. Impact of Obesity on the Metabolic Control of Type 2 Diabetes: Results of the Turkish Nationwide Survey of Glycemic and Other Metabolic Parameters of Patients with Diabetes Mellitus (TEMD Obesity Study). Obes. Facts 2019, 12, 167–178. [Google Scholar] [CrossRef]
- Kriska, A. Physical activity and the prevention of type 2 diabetes mellitus. Sports Med. 2000, 29, 147–151. [Google Scholar] [CrossRef]
- Orozco, L.J.; Buchleitner, A.M.; Gimenez-Perez, G.; i Figuls, M.R.; Richter, B.; Mauricio, D. Exercise or exercise and diet for preventing type 2 diabetes mellitus. Cochrane Database Syst. Rev. 2008, 3. [Google Scholar] [CrossRef]
- Feito, Y.; Patel, P.; Sal Redondo, A.; Heinrich, K.M. Effects of eight weeks of high intensity functional training on glucose control and body composition among overweight and obese adults. Sports 2019, 7, 51. [Google Scholar] [CrossRef]
- Zhang, Y.; Pan, X.-F.; Chen, J.; Xia, L.; Cao, A.; Zhang, Y.; Wang, J.; Li, H.; Yang, K.; Guo, K.; et al. Combined lifestyle factors and risk of incident type 2 diabetes and prognosis among individuals with type 2 diabetes: A systematic review and meta-analysis of prospective cohort studies. Diabetologia 2020, 63, 21–33. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. National Diabetes Statistics Report, 2020: Estimates of Diabetes and Its Burden in the United States. Available online: https://www.cdc.gov/diabetes/pdfs/data/statistics/national-diabetes-statistics-report.pdf (accessed on 14 October 2023).
- Kulak, E.; Berber, B.; Temel, H.; Kutluay, S.N.; Yıldırım, M.; Dedeoğlu, F.N.; Cifcili, S. Determining the risk level of type 2 diabetes in individuals applying to family medicine. Türk. Aile. Hek. Derg. 2019, 23, 20–30. [Google Scholar] [CrossRef]
- Qian, F.; Liu, G.; Hu, F.B.; Bhupathiraju, S.N.; Sun, Q. Association between plant-based dietary patterns and risk of type 2 diabetes: A systematic review and meta-analysis. JAMA Intern. Med. 2019, 179, 1335–1344. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6646993/ (accessed on 12 January 2024). [CrossRef]
- Ley, S.H.; Hamdy, O.; Mohan, V.; Hu, F.B. Prevention and management of type 2 diabetes: Dietary components and nutritional strategies. Lancet 2014, 383, 1999–2007. [Google Scholar] [CrossRef]
- Jacobs, S.; Harmon, B.E.; Boushey, C.J.; Morimoto, Y.; Wilkens, L.R.; Le Marchand, L.; Kröger, J.; Schulze, M.B.; Kolonel, L.N.; Maskarinec, G. A priori-defined diet quality indexes and risk of type 2 diabetes: The Multiethenic Cohort. Diabetología 2015, 58, 98–112. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4258157/ (accessed on 12 January 2024). [CrossRef]
- Chiuve, S.E.; Fung, T.T.; Rimm, E.B.; Hu, F.B.; McCullough, M.L.; Wang, M.; Willett, W.C. Alternative dietary indices both strongly predict risk of chronic disease. J. Nutr. 2012, 142, 1009–1018. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3738221/ (accessed on 12 January 2024). [CrossRef]
- Evert, A.B.; Dennison, M.; Gardner, C.D.; Garvey, W.T.; Lau, K.H.K.; MacLeod, J.; Mitri, J.; Pereira, R.F.; Rawlings, K.; Robinson, S.; et al. Nutrition therapy for adults with diabetes or prediabetes: A consensus report. Diabetes Care 2019, 42, 731–754. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7011201/ (accessed on 12 January 2024). [CrossRef]

{kind=link}
| TOTAL SCORE | INTERPRETATION | RESULTS OF OUR RESEARCH |
|---|---|---|
| Less than 7 points | Low risk level | 78.9% |
| From 7 to 11 points | Slightly low risk level | 16.1% |
| From 12 to 14 points | Moderate risk level | 4.4% |
| From 15 to 20 points | High risk level | 0.6% |
| More than 20 points | Very high risk level | 0% |
| QUANTITATIVE VARIABLES | |
|---|---|
| Mean ± SD | |
| Age (years) | 23.54 ± 5.93 |
| Height (cm) | 166.26 ± 9.32 |
| Basal Metabolism (kcal) | 1478.46 ± 275.02 |
| Weight (kg) | 64.50 ± 13.06 |
| % Fat Mass | 25.95 ± 7.40 |
| % Fat-Free Mass | 73.98 ± 7.47 |
| % Lean Mass | 69.48 ± 9.91 |
| Body Water % | 53.25 ± 5.76 |
| Body Mineral % | 3.72 ± 0.53 |
| BMI (kg/m2) | 23.40 ± 4.53 |
| Sarcopenia Index Risk | 7.03 ± 1.21 |
| Visceral Fat Index | 3.08 ± 2.87 |
| Metabolic Rate | 7.66 ± 2.22 |
| Waist Circumference (cm) | 76.83 ± 13.25 |
| Hip Circumference (cm) | 101.09 ± 9.55 |
| Waist/Hip Ratio | 0.76 ± 0.09 |
| Findrisk Score | 4.39 ± 3.25 |
| QUALITATIVE VARIABLES | n (%) |
| SEX | |
| Female | 209 (68.3%) |
| Male | 97 (31.7%) |
| PHYSICAL ACTIVITY | |
| <30 min | 177 (51.9%) |
| >30 min | 164 (48.1%) |
| FRUIT AND VEGETABLES | |
| No todos los días | 144 (42.2%) |
| Todos los días | 197 (57.8%) |
| HYPERTENSION MEDICATION | |
| NO | 335 (98.2%) |
| YES | 6 (1.8%) |
| GLUCOSE | |
| NO | 331 (97.1%) |
| YES | 10 (2.9%) |
| FAMILY HISTORY OF DIABETES | |
| No | 171 (50.3%) |
| Parents, siblings, children, etc. | 36 (10.6%) |
| Grandparents, aunts, uncle, cousins, etc. | 131 (38.5%) |
| Both (grandparents, parents, etc.) | 2 (0.6%) |
| RISK | |
| Low | 269 (78.9%) |
| Slightly Elevated | 55 (16.1%) |
| Moderate | 15 (4.4%) |
| High | 2 (0.6%) |
| Very High | (0%) |
| SCORE | Statistical Test | |||
|---|---|---|---|---|
| Average | Deviation | p-Value | ||
| SEX | Female | 4.61 | 3.12 | <0.01 |
| Male | 3.70 | 3.22 | ||
| PHYSICAL ACTIVITY | <30 min | 5.44 | 2.98 | <0.01 |
| >30 min | 3.26 | 3.14 | ||
| FRUIT AND VEGETABLES | Not every day | 5.16 | 3.01 | <0.01 |
| Every day | 3.83 | 3.31 | ||
| HYPERTENSION MEDICATION | No | 4.33 | 3.22 | >0.05 |
| Yes | 8.00 | 3.16 | ||
| GLUCOSE | No | 4.24 | 3.13 | >0.05 |
| Yes | 9.50 | 3.10 | ||
| FAMILY HISTORY OF DIABETES | No | 2.37 | 2.22 | >0.05 |
| Parents, siblings, children | 8.25 | 2.56 | ||
| grandparents, aunts, uncle, cousins | 5.88 | 2.69 | ||
| Both (grandparents, parents) | 9.50 | 2.12 | ||
| AGE (years) | <25 | 4.01 | 2.99 | <0.01 |
| >25 | 6.00 | 3.26 | ||
| BMI (kg/m2) | Thin | 3.00 | 2.37 | <0.01 |
| Normal weight | 3.56 | 2.58 | ||
| Overweight | 5.72 | 3.31 | ||
| Obese | 10.33 | 2.58 | ||
| BMI | |||||
|---|---|---|---|---|---|
| Thin | Normal Weight | Overweight | Obese | ||
| % of the Row n | % of the Row n | % of the Row n | % of the Row n | ||
| SEX | Female | 9.7% | 67.6% | 17.4% | 5.3% |
| Male | 1.0% | 64.6% | 30.2% | 4.2% | |
| PHYSICAL ACTIVITY | <30 min | 7.7% | 68.6% | 18.6% | 5.1% |
| >30 min | 6.1% | 64.6% | 24.5% | 4.8% | |
| FRUIT VEGETABLES | Not every day | 5.4% | 68.5% | 22.3% | 3.8% |
| Every day | 8.1% | 65.3% | 20.8% | 5.8% | |
| HYPERTENSION MEDICATION | NO | 7.0% | 66.3% | 21.7% | 5.0% |
| YES | 0.0% | 100.0% | 0.0% | 0.0% | |
| GLUCOSE | NO | 6.8% | 66.7% | 21.4% | 5.1% |
| YES | 11.1% | 66.7% | 22.2% | 0.0% | |
| FAMILY HISTORY OF DIABETES | NO | 9.7% | 64.3% | 22.1% | 3.9% |
| Parents, siblings, children | 0.0% | 62.1% | 24.1% | 13.8% | |
| Grandparents, aunts, uncles, cousins | 4.3% | 70.9% | 20.5% | 4.3% | |
| Both (grandparents, parents) | 50.0% | 50.0% | 0.0% | 0.0% | |
| AGE (years) | <25 | 10.5% | 69.8% | 16.7% | 3.1% |
| >25 | 0.0% | 57.1% | 30.4% | 12.5% | |
| SEX | ||||
|---|---|---|---|---|
| Female | Male | |||
| Average | Deviation | Average | Deviation | |
| % Fat mass | 28.56 | 6.34 | 20.27 | 6.30 |
| % Fat-free mass | 71.37 | 6.43 | 79.69 | 6.33 |
| % Lean mass | 67.38 | 7.66 | 74.03 | 12.43 |
| % Body water | 51.32 | 5.17 | 57.41 | 4.68 |
| % Bone mineral | 3.63 | 0.44 | 3.91 | 0.65 |
| BMI (kg/m2) | 23.03 | 4.90 | 24.19 | 3.48 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alfageme-García, P.; Basilio-Fernández, B.; Ramírez-Durán, M.d.V.; Gómez-Luque, A.; Jiménez-Cano, V.M.; Fabregat-Fernández, J.; Alonso, V.R.; Clavijo-Chamorro, M.Z.; Hidalgo-Ruíz, S. Risk of Type 2 Diabetes in University Students at the University of Extremadura: A Cross-Sectional Study. J. Pers. Med. 2024, 14, 146. https://doi.org/10.3390/jpm14020146
Alfageme-García P, Basilio-Fernández B, Ramírez-Durán MdV, Gómez-Luque A, Jiménez-Cano VM, Fabregat-Fernández J, Alonso VR, Clavijo-Chamorro MZ, Hidalgo-Ruíz S. Risk of Type 2 Diabetes in University Students at the University of Extremadura: A Cross-Sectional Study. Journal of Personalized Medicine. 2024; 14(2):146. https://doi.org/10.3390/jpm14020146
Chicago/Turabian StyleAlfageme-García, Pilar, Belinda Basilio-Fernández, María del Valle Ramírez-Durán, Adela Gómez-Luque, Víctor Manuel Jiménez-Cano, Juan Fabregat-Fernández, Vicente Robles Alonso, María Zoraida Clavijo-Chamorro, and Sonia Hidalgo-Ruíz. 2024. "Risk of Type 2 Diabetes in University Students at the University of Extremadura: A Cross-Sectional Study" Journal of Personalized Medicine 14, no. 2: 146. https://doi.org/10.3390/jpm14020146
APA StyleAlfageme-García, P., Basilio-Fernández, B., Ramírez-Durán, M. d. V., Gómez-Luque, A., Jiménez-Cano, V. M., Fabregat-Fernández, J., Alonso, V. R., Clavijo-Chamorro, M. Z., & Hidalgo-Ruíz, S. (2024). Risk of Type 2 Diabetes in University Students at the University of Extremadura: A Cross-Sectional Study. Journal of Personalized Medicine, 14(2), 146. https://doi.org/10.3390/jpm14020146