
Precision Medicine for More Oxygen (P4O2)—Study Design and First Results of the Long COVID-19 Extension
 , , , , ,
, , , , ,  , , ,
, , ,  ,
,  ,
,  ,
,  on behalf of the P4O2 consortiumadd
Show full author list
on behalf of the P4O2 consortiumadd
Show full author list
Abstract
1. Introduction
2. Methods
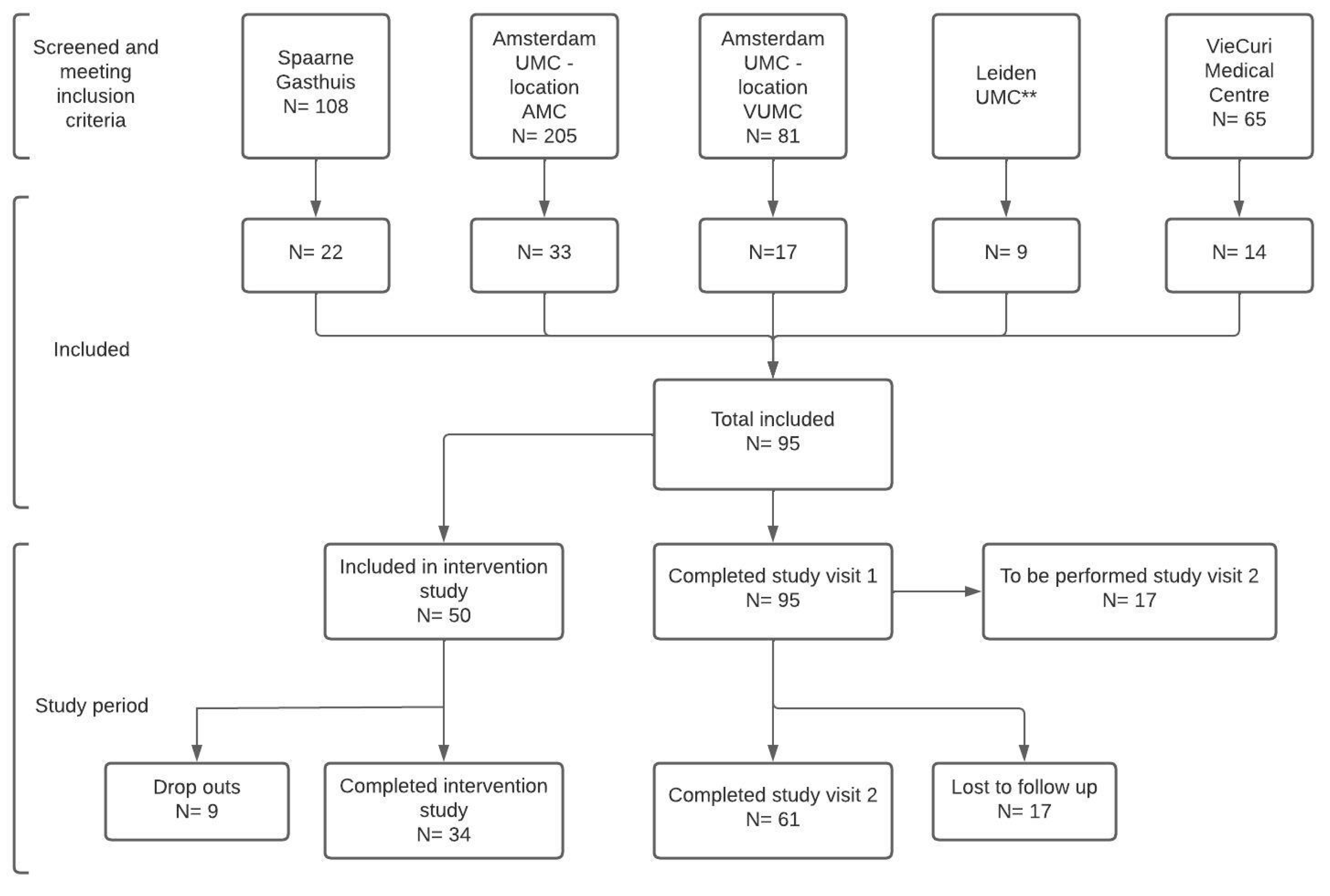
2.1. Study Design and Participants
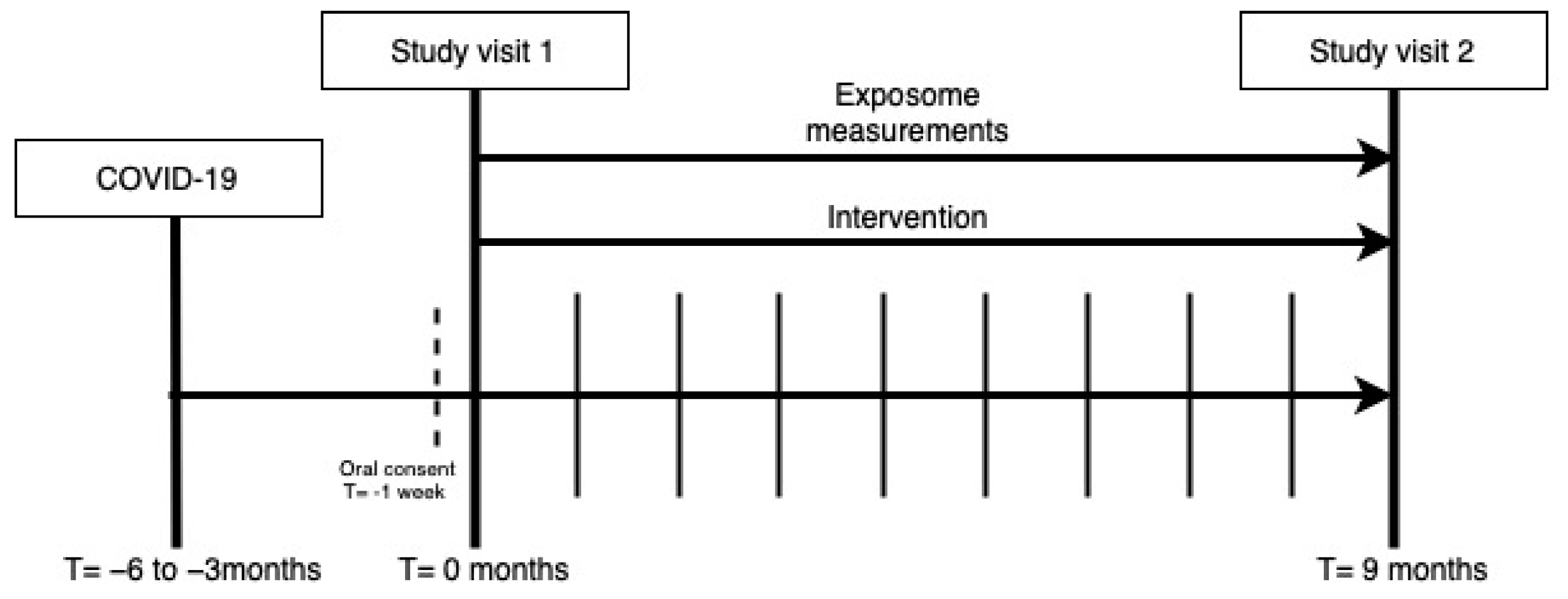
2.2. Study Visits
2.3. Exposome
2.4. Intervention
2.5. Sample Size Determination
2.6. Analysis of Baseline and Long COVID Characteristics
2.6.1. Classification of COVID-19 Severity and Variant
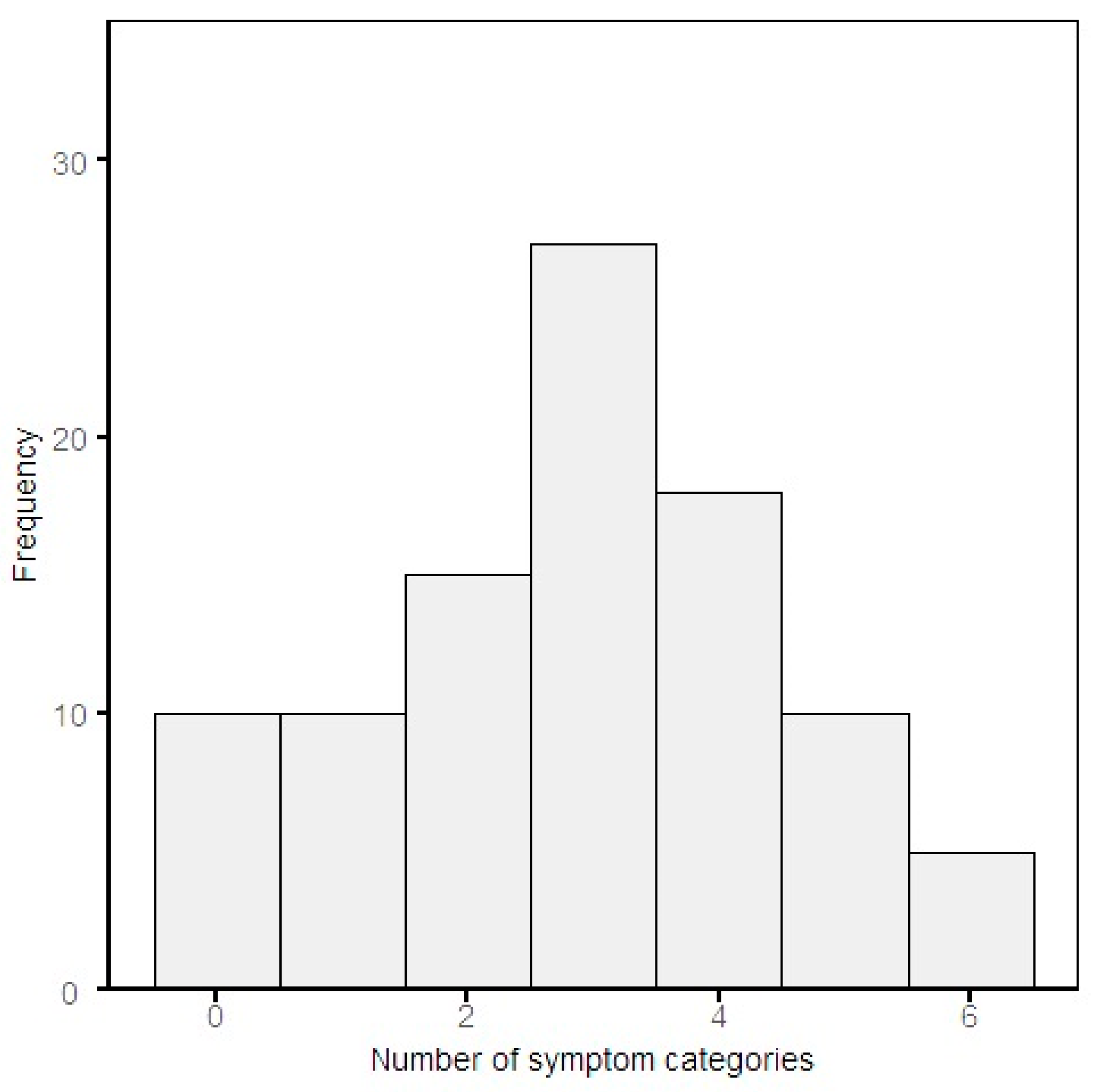
2.6.2. The Number and Classification of Persisting Symptoms
- Fatigue
- Respiratory
- Neurological
- Cardiovascular
- Gastrointestinal
- Other
2.6.3. Pulmonary Function Test and Radiological Abnormalities
2.6.4. Data Management and Statistical Analysis
3. Results
3.1. Baseline Characteristics and Long COVID Symptoms
3.2. Long COVID Symptoms
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| SARS-CoV-2 | severe acute respiratory syndrome coronavirus 2 |
| COVID-19 | coronavirus disease |
| WHO | World Health Organization |
| ACE2 | angiotensin-converting enzyme 2 |
| PASC | post-acute sequelae of COVID-19 |
| P4O2 COVID-19 | Precision Medicine for more Oxygen– COVID-19 study |
| UMC | University Medical Center |
| CO-RADS | COVID-19 Reporting and Data System |
| (q)PCR | (quantitative) polymerase chain reaction |
| DLCO | diffusing capacity of the lungs for carbon monoxide |
| CT | computed tomography |
| NT-PROBNP | N-terminal pro b-type natriuretic peptide |
| eNose | electronic nose |
| VOCs | volatile organic compounds |
| FSS | Fatigue Severity Scale |
| DSQ-2 | DePaul Symptom Questionnaire 2 |
| ME | myalgic encephalomyelitis |
| CFS | chronic fatigue syndrome |
| HADS | Hospital Anxiety and Depression Scale |
| USER-P | Utrecht Scale for Evaluation of Rehabilitation Participations |
| CLC-IC | Checklist for cognitive consequences after an ICU |
| ICU | intensive care unit |
| EQ5D | EuroQol 5D-5L |
| PROMIS | Patient-Reported outcome measurements information system |
| PC-PTSD-5 | Primary Care PTSD Screen for DSM-5 |
| BREQ-2 | Behavioral Regulation in Exercise Questionnaire-2 |
| REBS | Regulation of Eating Behaviors Scale |
| UPAS | Ultrasonic Personal Air Sampler |
| PM | particulate matter |
| EPA | eicosapentaenoic acid |
| DHA | docosahexaenoic acid |
| FVC | forced vital capacity |
| FEV1 | forced expiratory volume |
| OR | odds ratio |
| IQR | interquartile range |
Appendix A
- Study visits
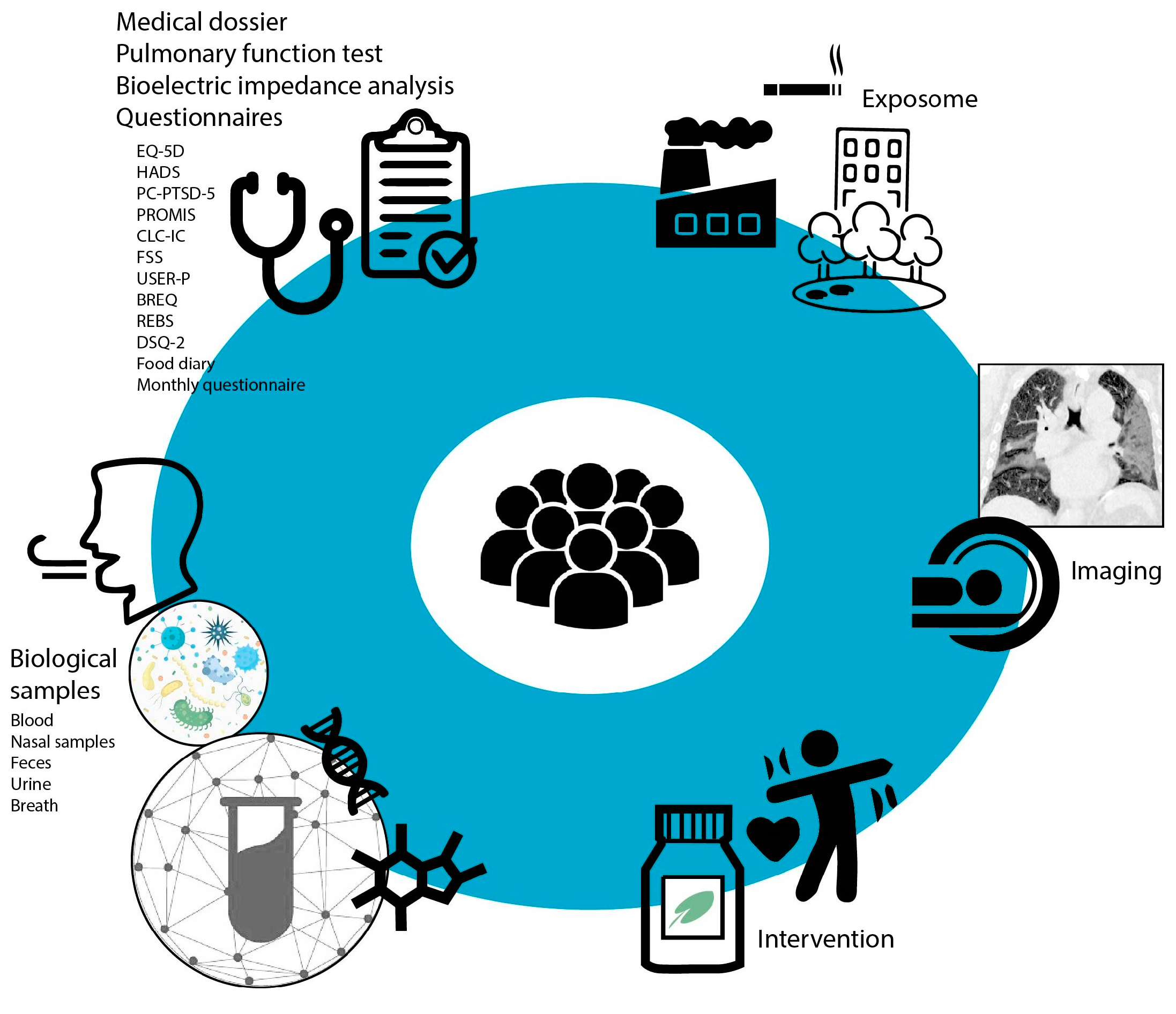
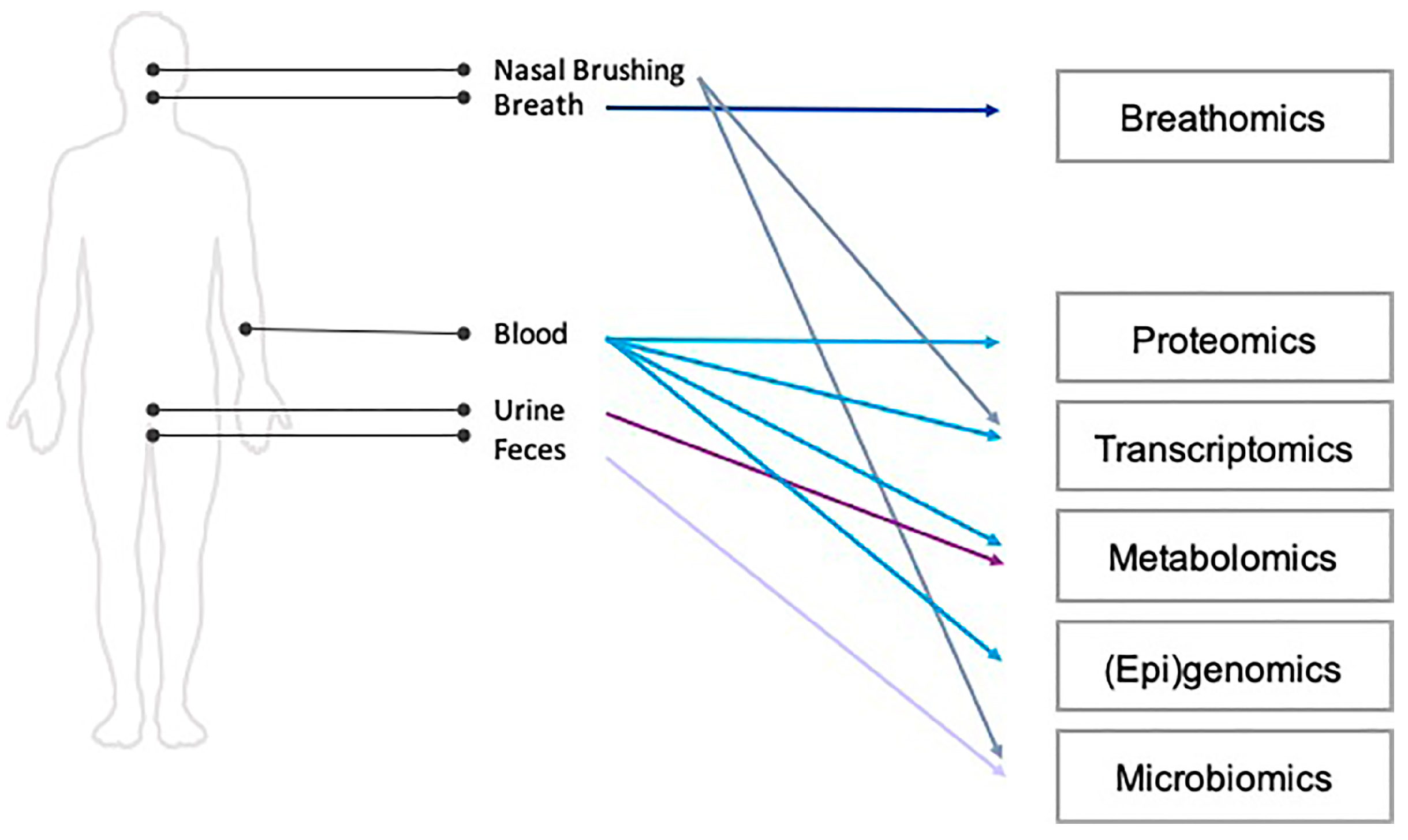
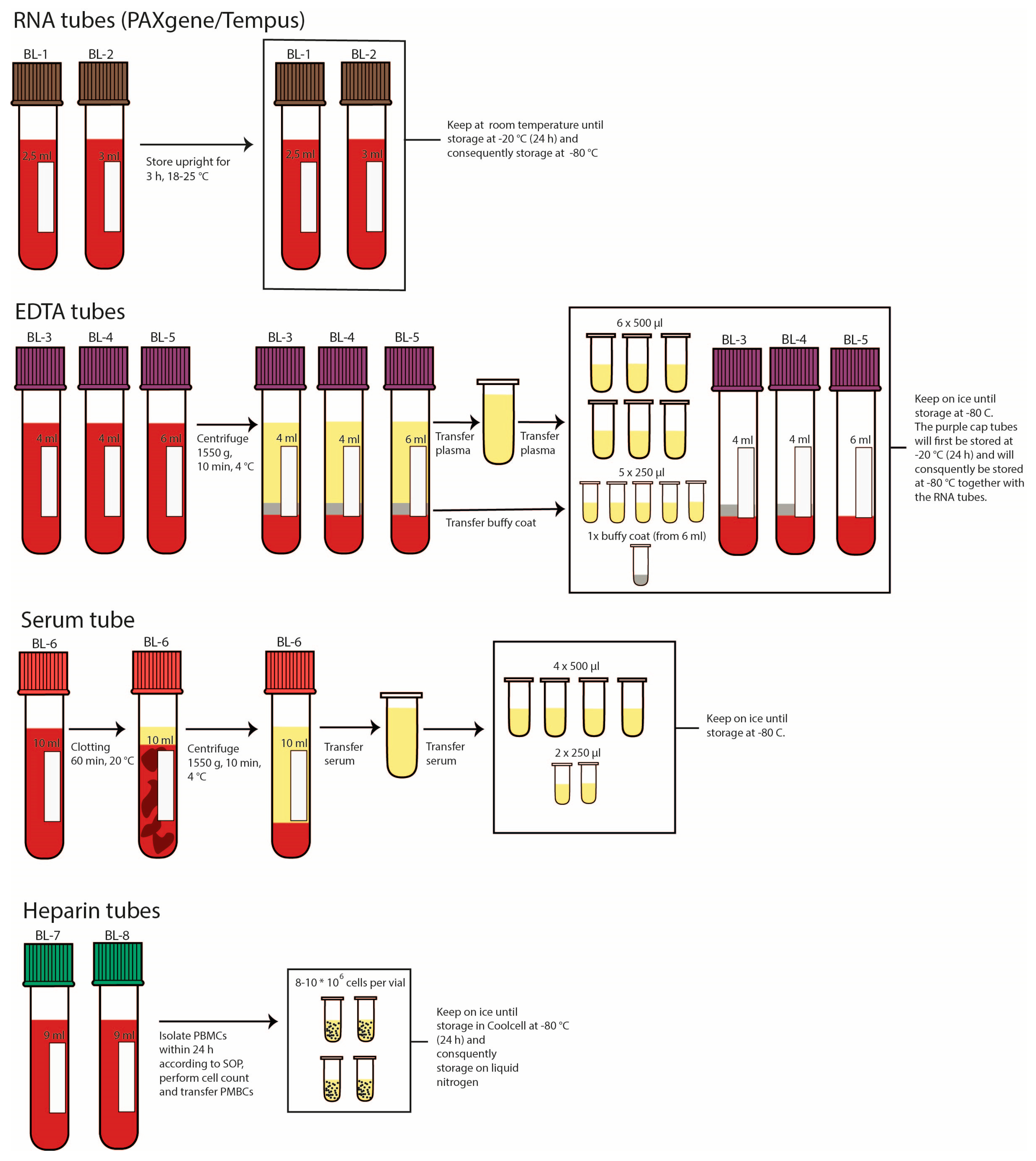
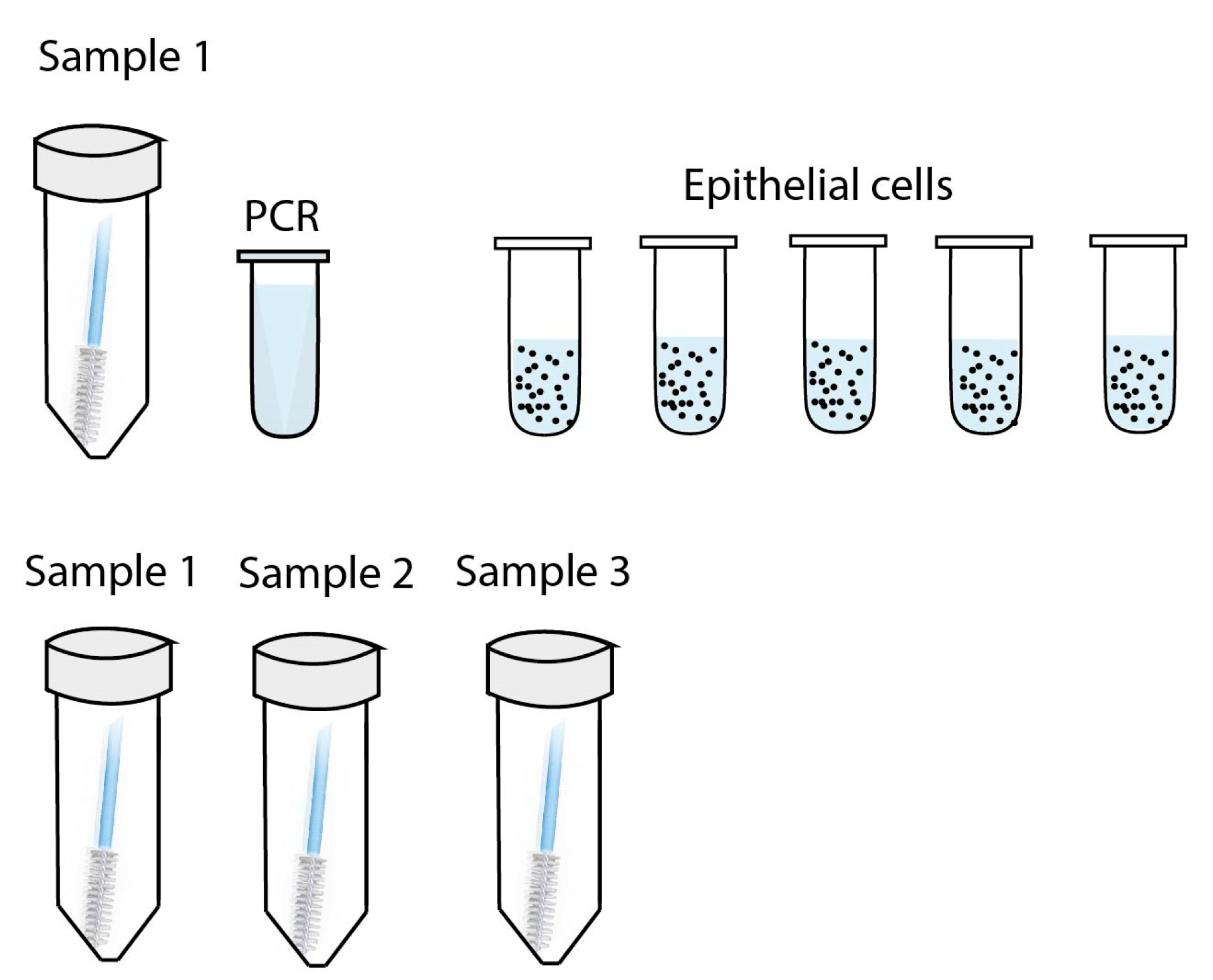
- Biological sample collection and measurements
- Questionnaires
- Exposome
- Intervention
- Personalized counselling intervention
- Nutritional support
- Qualitative analyses

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No Pulmonary Function Test/Radiological Abnormalities (N = 16) | Pulmonary Function Test/Radiological Abnormalities (N = 57) | |
|---|---|---|
| General | ||
| Age (Years) | 51.94 ± 5.80 | 54.14 ± 6.31 |
| Female | 9 (56.2%) | 23 (39.7%) |
| Smoking status | ||
| Current smoker | 0 (0.0%) | 3 (5.2%) |
| Ex-smoker | 9 (56.2%) | 29 (50.0%) |
| Never smoker | 7 (43.8%) | 26 (44.8%) |
| BMI | ||
| Normal | 2 (12.5%) | 6/57 (10.5%) |
| Overweight | 4 (25.0%) | 25/57 (43.9%) |
| Obese | 10 (62.5%) | 26/57 (45.6%) |
| Ethnicity | ||
| Caucasian | 11/15 (73.3%) | 41/52 (78.8%) |
| African | 3/15 (20.0%) | 4/52 (7.7%) |
| Asian | 0/15 (0.0%) | 2/52 (3.8%) |
| Latin-American | 0/15 (0.0%) | 2/52 (3.8%) |
| Other | 1/15 (6.7%) | 3/52 (5.8%) |
| Level of education | ||
| Secondary education | 0/13 (0.0%) | 14/47 (29.8%) |
| Vocational education | 8/13 (61.5%) | 16/47 (34.0%) |
| Bachelor | 4/13 (30.8%) | 11/47 (23.4%) |
| Master | 1/13 (7.7%) | 6/47 (12.8%) |
| Current comorbidities | ||
| Asthma | 0/15 (0.0%) | 0 (0.0%) |
| COPD | 0/15 (0.0%) | 0 (0.0%) |
| Cardiovascular disease | 4/15 (26.7%) | 20 (34.5%) |
| Heart failure | 0/15 (0.0%) | 3 (5.2%) |
| Deep vein thrombosis and pulmonary embolism | 1/15 (6.7%) | 5 (8.6%) |
| Diabetes | 1/15 (6.7%) | 11 (19.0%) |
| Hepatic disease | 0/15 (0.0%) | 5/57 (8.8%) |
| Renal Failure | 1/15 (6.7%) | 4/57 (7.0%) |
| Interstitial lung disease | 0/15 (0.0%) | 0 (0.0%) |
| Neurological disorders | 0/15 (0.0%) | 2 (3.4%) |
| Rheumatic diseases | 2/15 (13.3%) | 4 (6.9%) |
| Acute COVID-19 characteristics | ||
| No hospitalization | 4 (25.0%) | 3 (5.2%) |
| Hospitalization | 12 (75.0%) | 55 (94.8%) |
| Intensive care admission | 3 (18.8%) | 17 (29.3%) |
| Duration of hospitalization | 12; 6.50 (3.00, 8.25) | 54; 10.50 (7.00, 16.00) |
| Thrombosis | 2/15 (13.3%) | 9/55 (16.4%) |
| Pulmonary embolism | 1/15 (6.7%) | 9/56 (16.1%) |
| WHO disease Severity (mild) | 4 (25.0%) | 3 (5.2%) |
| WHO disease Severity (moderate) | 10 (62.5%) | 41 (70.7%) |
| WHO disease Severity (severe) | 2 (12.5%) | 14 (24.1%) |
| Oxygen supplementation and ventilation | ||
| Nasal cannula | 6 (37.5%) | 28 (48.3%) |
| Non-rebreating mask | 3 (18.8%) | 10 (17.2%) |
| Non-invasive ventilation | 0 (0.0%) | 2 (3.4%) |
| Invasive ventilation | 2 (12.5%) | 12 (20.7%) |
| Vaccination status | ||
| No | 5 (31.2%) | 19 (32.8%) |
| Yes, 1 dose | 6 (37.5%) | 12 (20.7%) |
| Yes, 2 or more doses | 5 (31.2%) | 27 (46.6%) |
| Pharmacological treatment during acute COVID-19 | ||
| Antivirals | ⅒ (10.0%) | 0/50 (0.0%) |
| Convalescent plasma | 0/7 (0.0%) | 0/30 (0.0%) |
| Antibiotics | 0/11 (0.0%) | 0/51 (0.0%) |
| Immunosuppressives | 11/12 (91.7%) | 52/54 (96.3%) |
| Other | 12/12 (100.0%) | 48/53 (90.6%) |
| Rest complaints | ||
| Fatigue | 10 (62.5%) | 33 (56.9%) |
| Respiratory | 11 (68.8%) | 43 (74.1%) |
| Neurological | 11 (68.8%) | 37 (63.8%) |
| Cardiovascular | 4 (25.0%) | 13 (22.4%) |
| Gastrointestinal | 5 (31.2%) | 12 (20.7%) |
| Other | 5 (31.2%) | 8 (13.8%) |
| Dominant virus strains | ||
| Beta | 4 (25.0%) | 20 (34.5%) |
| Gamma | 2 (12.5%) | 8 (13.8%) |
| Delta | 8 (50.0%) | 24 (41.4%) |
| Omicron | 2 (12.5%) | 6 (10.3%) |
| Blood tests | ||
| Hemoglobin (mmol/L) | 11; 8.60 (8.45, 9.60) | 39; 8.80 (8.30, 9.50) |
| Hematocrit (L/L) | 9; 0.42 (0.42, 0.47) | 33; 0.43 (0.40, 0.46) |
| Thrombocytes (109/L) | 9; 258.00 (243.00, 265.00) | 36; 261.50 (206.00, 290.75) |
| Leukocytes (109/L) | 9; 6.00 (5.60, 7.70) | 36; 6.45 (5.50, 7.98) |
| Eosinophiles (109/L) | 9; 0.10 (0.08, 0.18) | 31; 0.12 (0.08, 0.17) |
| Basophiles (109/L) | 9; 0.03 (0.02, 0.05) | 31; 0.04 (0.03, 0.06) |
| Neutrophiles (109/L L) | 9; 3.40 (2.98, 3.60) | 28; 3.75 (2.65, 4.49) |
| Lymphocytes (109/L) | 9; 2.16 (1.63, 2.78) | 31; 1.98 (1.73, 2.59) |
| Monocytes (109/L) | 9; 0.47 (0.40, 0.59) | 31; 0.54 (0.43, 0.72) |
| Creatinine (μmol/L) | 10; 72.50 (67.00, 80.75) | 38; 81.50 (70.00, 89.00) |
| EGFR (mL/min/1.73 m2) | 10; 88.50 (86.25, 90.00) | 38; 86.50 (72.25, 90.00) |
| ALAT (U/L) | 9; 23.00 (18.00, 29.00) | 33; 27.00 (20.00, 37.00) |
| ASAT (U/L) | 9; 22.00 (20.00, 29.00) | 32; 23.00 (20.25, 27.00) |
| LDH (U/L) | 9; 170.00 (159.00, 191.00) | 33; 204.00 (179.00, 235.00) |
| CRP (mg/L) | 9; 2.40 (1.00, 3.20) | 34; 2.10 (1.33, 5.88) |
| Glucose (mmol/L) | 6; 5.50 (4.75, 5.50) | 27; 5.70 (5.35, 6.45) |
| Creatine Phosphokinase (U/L) | 6; 91.00 (74.75, 104.25) | 22; 96.50 (67.50, 199.50) |
| NTProBNP (ng/L) | 10; 50.70 (50.00, 73.50) | 29; 50.70 (50.00, 87.00) |


References
- Dixon, B.E.; Wools-Kaloustian, K.; Fadel, W.F.; Duszynski, T.J.; Yiannoutsos, C.; Halverson, P.K.; Menachemi, N. Symptoms and symptom clusters associated with SARS-CoV-2 infection in community-based populations: Results from a statewide epidemiological study. Public Glob. Health 2020, 16, e0241875. [Google Scholar] [CrossRef]
- Tobin, M.J.; Laghi, F.; Jubran, A. Why COVID-19 Silent Hypoxemia Is Baffling to Physicians. Am. J. Respir. Crit. Care Med. 2020, 202, 356–360. [Google Scholar] [CrossRef] [PubMed]
- Shang, J.; Wan, Y.; Luo, C.; Ye, G.; Geng, Q.; Auerbach, A.; Li, F. Cell Entry Mechanisms of SARS-CoV-2. Proc. Natl. Acad. Sci. USA 2020, 117, 11727–11734. [Google Scholar] [CrossRef] [PubMed]
- Hamming, I.; Timens, W.; Bulthuis, M.; Lely, A.; Navis, G.; van Goor, H. Tissue Distribution of ACE2 Protein, the Functional Receptor for SARS Coronavirus. A First Step in Understanding SARS Pathogenesis. J. Pathol. 2004, 203, 631–637. [Google Scholar] [CrossRef]
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons From the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72 314 Cases From the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Huang, L.; Wang, Y.; Li, X.; Ren, L.; Gu, X.; Kang, L.; Guo, L.; Liu, M.; Zhou, X.; et al. 6-Month Consequences of COVID-19 in Patients Discharged from Hospital: A Cohort Study. Lancet 2021, 397, 220–232. [Google Scholar] [CrossRef]
- Carfì, A.; Bernabei, R.; Landi, F.; for the Gemelli against COVID-19 Post-Acute Care Study Group. Persistent Symptoms in Patients After Acute COVID-19. JAMA 2020, 324, 603. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. A Clinical Case Definition of Post COVID-19 Condition by a Delphi Consensus; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Taquet, M.; Dercon, Q.; Luciano, S.; Geddes, J.R.; Husain, M.; Harrison, P.J. Incidence, Co-Occurrence, and Evolution of Long-COVID Features: A 6-Month Retrospective Cohort Study of 273,618 Survivors of COVID-19. PLoS Med. 2021, 18, e1003773. [Google Scholar] [CrossRef]
- Groff, D.; Sun, A.; Ssentongo, A.E.; Ba, D.M.; Parsons, N.; Poudel, G.R.; Lekoubou, A.; Oh, J.S.; Ericson, J.E.; Ssentongo, P.; et al. Short-Term and Long-Term Rates of Postacute Sequelae of SARS-CoV-2 Infection: A Systematic Review. JAMA Netw Open 2021, 4, e2128568. [Google Scholar] [CrossRef]
- World Health Organization. At Least 17 Million People in the WHO European Region Experienced Long COVID in the First Two Years of the Pandemic; Millions May Have to Live with It for Years to Come. Available online: https://www.who.int/europe/news/item/13-09-2022-at-least-17-million-people-in-the-who-european-region-experienced-long-covid-in-the-first-two-years-of-the-pandemic--millions-may-have-to-live-with-it-for-years-to-come (accessed on 6 June 2022).
- Logue, J.K.; Franko, N.M.; McCulloch, D.J.; McDonald, D.; Magedson, A.; Wolf, C.R.; Chu, H.Y. Sequelae in Adults at 6 Months After COVID-19 Infection. JAMA Netw Open 2021, 4, e210830. [Google Scholar] [CrossRef]
- Goërtz, Y.M.J.; Van Herck, M.; Delbressine, J.M.; Vaes, A.W.; Meys, R.; Machado, F.V.C.; Houben-Wilke, S.; Burtin, C.; Posthuma, R.; Franssen, F.M.E.; et al. Persistent Symptoms 3 Months after a SARS-CoV-2 Infection: The Post-COVID-19 Syndrome? ERJ Open Res. 2020, 6, 00542–02020. [Google Scholar] [CrossRef] [PubMed]
- Crook, H.; Raza, S.; Nowell, J.; Young, M.; Edison, P. Long Covid—Mechanisms, Risk Factors, and Management. BMJ 2021, 374, n1648. [Google Scholar] [CrossRef] [PubMed]
- Bannister, B.A. Post-Infectious Disease Syndrome. Postgrad. Med. J. 1988, 64, 559–567. [Google Scholar] [CrossRef] [PubMed]
- Ortona, E.; Malorni, W. Long COVID: To Investigate Immunological Mechanisms and Sex/Gender Related Aspects as Fundamental Steps for Tailored Therapy. Eur. Respir. J 2022, 59, 2102245. [Google Scholar] [CrossRef] [PubMed]
- Proal, A.D.; VanElzakker, M.B. Long COVID or Post-Acute Sequelae of COVID-19 (PASC): An Overview of Biological Factors That May Contribute to Persistent Symptoms. Front. Microbiol. 2021, 12, 698169. [Google Scholar] [CrossRef]
- Su, Y.; Yuan, D.; Chen, D.G.; Ng, R.H.; Wang, K.; Choi, J.; Li, S.; Hong, S.; Zhang, R.; Xie, J.; et al. Multiple Early Factors Anticipate Post-Acute COVID-19 Sequelae. Cell 2022, 185, 881–895.e20. [Google Scholar] [CrossRef]
- Vijayakumar, B.; Boustani, K.; Ogger, P.P.; Papadaki, A.; Tonkin, J.; Orton, C.M.; Ghai, P.; Suveizdyte, K.; Hewitt, R.J.; Desai, S.R.; et al. Immuno-Proteomic Profiling Reveals Aberrant Immune Cell Regulation in the Airways of Individuals with Ongoing Post-COVID-19 Respiratory Disease. Immunity 2022, 55, 542–556.e5. [Google Scholar] [CrossRef]
- Eroğlu, İ.; Eroğlu, B.Ç.; Güven, G.S. Altered Tryptophan Absorption and Metabolism Could Underlie Long-Term Symptoms in Survivors of Coronavirus Disease 2019 (COVID-19). Nutrition 2021, 90, 111308. [Google Scholar] [CrossRef]
- Nemeth, H.; Toldi, J.; Vecsei, L. Role of Kynurenines in the Central and Peripherial Nervous Systems. CNR 2005, 2, 249–260. [Google Scholar] [CrossRef]
- CDC. Exposome and Exposomics | NIOSH | CDC. Available online: https://www.cdc.gov/niosh/topics/exposome/default.html (accessed on 22 June 2022).
- La Rosa, P.S.; Brooks, J.P.; Deych, E.; Boone, E.L.; Edwards, D.J.; Wang, Q.; Sodergren, E.; Weinstock, G.; Shannon, W.D. Hypothesis Testing and Power Calculations for Taxonomic-Based Human Microbiome Data. PLoS ONE 2012, 7, e52078. [Google Scholar] [CrossRef] [PubMed]
- Nyamundanda, G.; Gormley, I.C.; Fan, Y.; Gallagher, W.M.; Brennan, L. MetSizeR: Selecting the Optimal Sample Size for Metabolomic Studies Using an Analysis Based Approach. BMC Bioinform. 2013, 14, 338. [Google Scholar] [CrossRef]
- Blaise, B.J.; Correia, G.; Tin, A.; Young, J.H.; Vergnaud, A.-C.; Lewis, M.; Pearce, J.T.M.; Elliott, P.; Nicholson, J.K.; Holmes, E.; et al. Power Analysis and Sample Size Determination in Metabolic Phenotyping. Anal. Chem. 2016, 88, 5179–5188. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO R&D Blueprint Novel Coronavirus COVID-19 Therapeutic Trial Synopsis; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- RIVM. Variants of the Coronavirus SARS-CoV-2. Available online: https://www.rivm.nl/en/coronavirus-covid-19/virus/variants (accessed on 30 June 2022).
- CDC. Long COVID or Post-COVID Conditions. Available online: https://www.cdc.gov/coronavirus/2019-ncov/long-term-effects/index.html (accessed on 6 June 2022).
- Ghayda, R.A.; Lee, K.H.; Kim, J.S.; Lee, S.; Hong, S.H.; Kim, K.S.; Kim, K.E.; Seok, J.; Kim, H.; Seo, J.; et al. Chest CT Abnormalities in COVID-19: A Systematic Review. Int. J. Med. Sci. 2021, 18, 3395–3402. [Google Scholar] [CrossRef] [PubMed]
- Kanne, J.P.; Little, B.P.; Schulte, J.J.; Haramati, A.; Haramati, L.B. Long-Term Lung Abnormalities Associated with COVID-19 Pneumonia. Radiology 2022, 306, 221806. [Google Scholar] [CrossRef]
- Lemhöfer, C.; Sturm, C.; Loudovici-Krug, D.; Best, N.; Gutenbrunner, C. The Impact of Post-COVID-Syndrome on Functioning—Results from a Community Survey in Patients after Mild and Moderate SARS-CoV-2-Infections in Germany. J. Occup. Med. Toxicol. 2021, 16, 45. [Google Scholar] [CrossRef] [PubMed]
- Jacobson, K.B.; Rao, M.; Bonilla, H.; Subramanian, A.; Hack, I.; Madrigal, M.; Singh, U.; Jagannathan, P.; Grant, P. Patients With Uncomplicated Coronavirus Disease 2019 (COVID-19) Have Long-Term Persistent Symptoms and Functional Impairment Similar to Patients with Severe COVID-19: A Cautionary Tale During a Global Pandemic. Clin. Infect. Dis. 2021, 73, e826–e829. [Google Scholar] [CrossRef]
- Davis, M.M. Flexibility for Specificity. Science 2015, 347, 371–372. [Google Scholar] [CrossRef]
- Arnold, D.T.; Hamilton, F.W.; Milne, A.; Morley, A.J.; Viner, J.; Attwood, M.; Noel, A.; Gunning, S.; Hatrick, J.; Hamilton, S.; et al. Patient Outcomes after Hospitalisation with COVID-19 and Implications for Follow-up: Results from a Prospective UK Cohort. Thorax 2021, 76, 399–401. [Google Scholar] [CrossRef]
- Ali, S.T.; Kang, A.K.; Patel, T.R.; Clark, J.R.; Perez-Giraldo, G.S.; Orban, Z.S.; Lim, P.H.; Jimenez, M.; Graham, E.L.; Batra, A.; et al. Evolution of Neurologic Symptoms in Non-hospitalized COVID-19 “Long Haulers”. Ann. Clin. Transl. Neurol. 2022, 9, 950–961. [Google Scholar] [CrossRef]
- Bai, F.; Tomasoni, D.; Falcinella, C.; Barbanotti, D.; Castoldi, R.; Mulè, G.; Augello, M.; Mondatore, D.; Allegrini, M.; Cona, A.; et al. Female Gender Is Associated with Long COVID Syndrome: A Prospective Cohort Study. Clin. Microbiol. Infect. 2022, 28, 611.e9–611.e16. [Google Scholar] [CrossRef]
- Dryden, M.; Mudara, C.; Vika, C.; Blumberg, L.; Mayet, N.; Cohen, C.; Tempia, S.; Parker, A.; Nel, J.; Perumal, R.; et al. Post-COVID-19 Condition 3 Months after Hospitalisation with SARS-CoV-2 in South Africa: A Prospective Cohort Study. Lancet Glob. Health 2022, 10, e1247–e1256. [Google Scholar] [CrossRef] [PubMed]
- Pelà, G.; Goldoni, M.; Solinas, E.; Cavalli, C.; Tagliaferri, S.; Ranzieri, S.; Frizzelli, A.; Marchi, L.; Mori, P.A.; Majori, M.; et al. Sex-Related Differences in Long-COVID-19 Syndrome. J. Women’s Health 2022, 31, 620–630. [Google Scholar] [CrossRef] [PubMed]
- Sudre, C.H.; Murray, B.; Varsavsky, T.; Graham, M.S.; Penfold, R.S.; Bowyer, R.C.; Pujol, J.C.; Klaser, K.; Antonelli, M.; Canas, L.S.; et al. Attributes and Predictors of Long COVID. Nat. Med. 2021, 27, 626–631. [Google Scholar] [CrossRef] [PubMed]
- the European Network on ME/CFS (EUROMENE); Rasa, S.; Nora-Krukle, Z.; Henning, N.; Eliassen, E.; Shikova, E.; Harrer, T.; Scheibenbogen, C.; Murovska, M.; Prusty, B.K. Chronic Viral Infections in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS). J. Transl. Med. 2018, 16, 268. [Google Scholar] [CrossRef]
- Kedor, C.; Freitag, H.; Meyer-Arndt, L.; Wittke, K.; Hanitsch, L.G.; Zoller, T.; Steinbeis, F.; Haffke, M.; Rudolf, G.; Heidecker, B.; et al. A Prospective Observational Study of Post-COVID-19 Chronic Fatigue Syndrome Following the First Pandemic Wave in Germany and Biomarkers Associated with Symptom Severity. Nat. Commun. 2022, 13, 5104. [Google Scholar] [CrossRef]
- Bellan, M.; Soddu, D.; Balbo, P.E.; Baricich, A.; Zeppegno, P.; Avanzi, G.C.; Baldon, G.; Bartolomei, G.; Battaglia, M.; Battistini, S.; et al. Respiratory and Psychophysical Sequelae Among Patients With COVID-19 Four Months After Hospital Discharge. JAMA Netw Open 2021, 4, e2036142. [Google Scholar] [CrossRef]
- Magnúsdóttir, I.; Lovik, A.; Unnarsdóttir, A.B.; McCartney, D.; Ask, H.; Kõiv, K.; Christoffersen, L.A.N.; Johnson, S.U.; Hauksdóttir, A.; Fawns-Ritchie, C.; et al. Acute COVID-19 Severity and Mental Health Morbidity Trajectories in Patient Populations of Six Nations: An Observational Study. Lancet Public Health 2022, 7, e406–e416. [Google Scholar] [CrossRef]
- Trimbos Instituut. Neerslachtiger, Meer Slaapproblemen En Gedachten Aan de Dood Door Corona. Available online: https://www.trimbos.nl/actueel/nieuws/neerslachtiger-meer-slaapproblemen-en-gedachten-aan-de-dood-door-corona/ (accessed on 7 July 2022).
- Centraal Bureau voor de Statistiek. Meer Volwassenen Met Ernstig Overgewicht Tevreden Met Gewicht. Available online: https://www.cbs.nl/nl-nl/nieuws/2021/34/meer-volwassenen-met-ernstig-overgewicht-tevreden-met-gewicht (accessed on 8 July 2022).
- Venkatakrishnan, A.J.; Pawlowski, C.; Zemmour, D.; Hughes, T.; Anand, A.; Berner, G.; Kayal, N.; Puranik, A.; Conrad, I.; Bade, S.; et al. Mapping Each Pre-Existing Condition’s Association to Short-Term and Long-Term COVID-19 Complications. npj Digit. Med. 2021, 4, 117. [Google Scholar] [CrossRef]
- Antonelli, M.; Pujol, J.C.; Spector, T.D.; Ourselin, S.; Steves, C.J. Risk of Long COVID Associated with Delta versus Omicron Variants of SARS-CoV-2. Lancet 2022, 399, 2263–2264. [Google Scholar] [CrossRef]
- So, M.; Kabata, H.; Fukunaga, K.; Takagi, H.; Kuno, T. Radiological and Functional Lung Sequelae of COVID-19: A Systematic Review and Meta-Analysis. BMC Pulm. Med. 2021, 21, 97. [Google Scholar] [CrossRef]
- Lehmann, A.; Gysan, M.; Bernitzky, D.; Bal, C.; Prosch, H.; Zehetmayer, S.; Milos, R.-I.; Vonbank, K.; Pohl, W.; Idzko, M.; et al. Comparison of Pulmonary Function Test, Diffusion Capacity, Blood Gas Analysis and CT Scan in Patients with and without Persistent Respiratory Symptoms Following COVID-19. BMC Pulm. Med. 2022, 22, 196. [Google Scholar] [CrossRef]
- Shahid, A.; Wilkinson, K.; Marcu, S.; Shapiro, C.M. Fatigue Severity Scale (FSS). In STOP, THAT and One Hundred Other Sleep Scales; Shahid, A., Wilkinson, K., Marcu, S., Shapiro, C.M., Eds.; Springer: New York, NY, USA, 2011; pp. 167–168. ISBN 978-1-4419-9892-7. [Google Scholar]
- Bedree, H.; Sunnquist, M.; Jason, L.A. The DePaul Symptom Questionnaire-2: A Validation Study. Fatigue Biomed. Health Behav. 2019, 7, 166–179. [Google Scholar] [CrossRef] [PubMed]
- Bourmistrova, N.W.; Solomon, T.; Braude, P.; Strawbridge, R.; Carter, B. Long-Term Effects of COVID-19 on Mental Health: A Systematic Review. J. Affect. Disord. 2022, 299, 118–125. [Google Scholar] [CrossRef] [PubMed]
- Stern, A.F. The Hospital Anxiety and Depression Scale. Occup. Med. 2014, 64, 393–394. [Google Scholar] [CrossRef] [PubMed]
- Post, M.W.M.; van der Zee, C.H.; Hennink, J.; Schafrat, C.G.; Visser-Meily, J.M.A.; van Berlekom, S.B. Validity of the Utrecht Scale for Evaluation of Rehabilitation-Participation. Disabil. Rehabil. 2012, 34, 478–485. [Google Scholar] [CrossRef] [PubMed]
- van Hout, B.; Janssen, M.F.; Feng, Y.-S.; Kohlmann, T.; Busschbach, J.; Golicki, D.; Lloyd, A.; Scalone, L.; Kind, P.; Pickard, A.S. Interim Scoring for the EQ-5D-5L: Mapping the EQ-5D-5L to EQ-5D-3L Value Sets. Value Health 2012, 15, 708–715. [Google Scholar] [CrossRef]
- Hays, R.D.; Bjorner, J.B.; Revicki, D.A.; Spritzer, K.L.; Cella, D. Development of Physical and Mental Health Summary Scores from the Patient-Reported Outcomes Measurement Information System (PROMIS) Global Items. Qual. Life Res. 2009, 18, 873–880. [Google Scholar] [CrossRef]
- Prins, A.; Bovin, M.J.; Smolenski, D.J.; Marx, B.P.; Kimerling, R.; Jenkins-Guarnieri, M.A.; Kaloupek, D.G.; Schnurr, P.P.; Kaiser, A.P.; Leyva, Y.E.; et al. The Primary Care PTSD Screen for DSM-5 (PC-PTSD-5): Development and Evaluation Within a Veteran Primary Care Sample. J. Gen. Intern. Med. 2016, 31, 1206–1211. [Google Scholar] [CrossRef]
- Murcia, J.a.M.; Gimeno, E.C.; Camacho, A.M. Measuring Self-Determination Motivation in a Physical Fitness Setting: Validation of the Behavioral Regulation in Exercise Questionnaire-2 (BREQ-2) in a Spanish Sample. J. Sport. Med. Phys. Fit. 2007, 47, 366–374. [Google Scholar]
- Pelletier, L.G.; Dion, S.C.; Slovinec-D’Angelo, M.; Reid, R. Why Do You Regulate What You Eat? Relationships Between Forms of Regulation, Eating Behaviors, Sustained Dietary Behavior Change, and Psychological Adjustment. Motiv. Emot. 2004, 28, 245–277. [Google Scholar] [CrossRef]
- SODAQ. SODAQ Snifferbike—SODAQ. Available online: https://old.sodaq.com/sodaq-snifferbike/ (accessed on 6 June 2022).
- O’Connell, S.G.; Kincl, L.D.; Anderson, K.A. Silicone Wristbands as Personal Passive Samplers. Environ. Sci. Technol. 2014, 48, 3327–3335. [Google Scholar] [CrossRef]
- van de Bool, C.; Rutten, E.P.A.; van Helvoort, A.; Franssen, F.M.E.; Wouters, E.F.M.; Schols, A.M.W.J. A Randomized Clinical Trial Investigating the Efficacy of Targeted Nutrition as Adjunct to Exercise Training in COPD: Targeted Nutrition in COPD Patients with Low Muscle Mass. J. Cachexia Sarcopenia Muscle 2017, 8, 748–758. [Google Scholar] [CrossRef] [PubMed]
- van Beers, M.; Rutten-van Mölken, M.P.M.H.; van de Bool, C.; Boland, M.; Kremers, S.P.J.; Franssen, F.M.E.; van Helvoort, A.; Gosker, H.R.; Wouters, E.F.; Schols, A.M.W.J. Clinical Outcome and Cost-Effectiveness of a 1-Year Nutritional Intervention Programme in COPD Patients with Low Muscle Mass: The Randomized Controlled NUTRAIN Trial. Clin. Nutr. 2020, 39, 405–413. [Google Scholar] [CrossRef]
- Laviano, A.; Calder, P.C.; Schols, A.; Lonnqvist, F.; Bech, M.; Dorkhan, M.; Muscaritoli, M. Targeted Medical Nutrition in Pre-Cachectic Patients with Non-Small-Cell Lung Cancer: A Subgroup Analysis. Nutr. Cancer 2021, 73, 899–900. [Google Scholar] [CrossRef] [PubMed]
- Calder, P.C.; Laviano, A.; Lonnqvist, F.; Muscaritoli, M.; Öhlander, M.; Schols, A. Targeted Medical Nutrition for Cachexia in Chronic Obstructive Pulmonary Disease: A Randomized, Controlled Trial: Cachexia in COPD: TMN RCT. J. Cachexia Sarcopenia Muscle 2018, 9, 28–40. [Google Scholar] [CrossRef] [PubMed]
- Laviano, A.; Calder, P.C.; Schols, A.M.W.J.; Lonnqvist, F.; Bech, M.; Muscaritoli, M. Safety and Tolerability of Targeted Medical Nutrition for Cachexia in Non-Small-Cell Lung Cancer: A Randomized, Double-Blind, Controlled Pilot Trial. Nutr. Cancer 2020, 72, 439–450. [Google Scholar] [CrossRef]
- Jensen, G.L.; Cederholm, T.; Correia, M.I.T.D.; Gonzalez, M.C.; Fukushima, R.; Higashiguchi, T.; Baptista, G.A.; Barazzoni, R.; Blaauw, R.; Coats, A.J.S.; et al. GLIM Criteria for the Diagnosis of Malnutrition: A Consensus Report From the Global Clinical Nutrition Community. J. Parenter. Enter. Nutr. 2019, 43, 32–40. [Google Scholar] [CrossRef]





| Data (N = 95) | |
|---|---|
| General | |
| Age | 54.15 ± 6.18 |
| Female | 47 (49.5%) |
| Smoking status | |
| Current smoker | 4 (4.2%) |
| Ex-smoker | 51 (53.7%) |
| Never smoker | 40 (42.1%) |
| BMI | |
| Normal | 10/94 (10.6%) |
| Overweight | 35/94 (37.2%) |
| Obese | 49/94 (52.1%) |
| Ethnicity | |
| Caucasian | 66/86 (76.7%) |
| African | 8/86 (9.3%) |
| Asian | 3/86 (3.5%) |
| Latin-American | 3/86 (3.5%) |
| Other | 6/86 (7.0%) |
| Level of education | |
| Secondary education | 19/79 (24.1%) |
| Vocational education | 33/79 (41.8%) |
| Bachelor | 19/79 (24.1%) |
| Master | 8/79 (10.1%) |
| Current comorbidities | |
| Asthma | 16/94 (17.0%) |
| COPD | 6/94 (6.4%) |
| Cardiovascular disease | 27/93 (29.0%) |
| Heart failure | 6/94 (6.4%) |
| Deep vein thrombosis and pulmonary embolism | 10/94 (10.6%) |
| Diabetes | 15/94 (16.0%) |
| Hepatic disease | 6/93 (6.5%) |
| Renal Failure | 7/92 (7.6%) |
| Interstitial lung disease | 2/94 (2.1%) |
| Neurological disorders | 3/94 (3.2%) |
| Rheumatic diseases | 9/94 (9.6%) |
| Acute COVID-19 characteristics | |
| No hospitalization | 10 (10.5%) |
| Hospitalization | 85 (89.5%) |
| Intensive care admission | 27 (28.4%) |
| Duration of hospitalization | 84; 8.50 (6.00, 16.00) |
| Thrombosis | 14/91 (15.4%) |
| Pulmonary embolism | 15/92 (16.3%) |
| WHO disease Severity (mild) | 10 (10.5%) |
| WHO disease Severity (moderate) | 61 (64.2%) |
| WHO disease Severity (severe) | 24 (25.3%) |
| Oxygen supplementation and ventilation | |
| Nasal cannula | 40 (42.1%) |
| Non-rebreathing mask | 16 (16.8%) |
| Non-invasive ventilation | 5 (5.3%) |
| Invasive ventilation | 19 (20.0%) |
| Vaccination status | |
| No | 28 (29.5%) |
| Yes, 1 dose | 24 (25.3%) |
| Yes, 2 or more doses | 43 (45.3%) |
| Pharmacological treatment during acute COVID-19 | |
| Antivirals | 1/75 (1.3%) |
| Convalescent plasma | 0/45 (0.0%) |
| Antibiotics | 0/77 (0.0%) |
| Immunosuppressives | 78/83 (94.0%) |
| Other | 74/81 (91.4%) |
| Rest complaints | |
| Fatigue | 64 (67.4%) |
| Respiratory | 75 (78.9%) |
| Neurological | 65 (68.4%) |
| Cardiovascular | 25 (26.3%) |
| Gastrointestinal | 26 (27.4%) |
| Other | 18 (18.9%) |
| Dominant virus strains | |
| Beta | 27 (28.4%) |
| Gamma | 14 (14.7%) |
| Delta | 43 (45.3%) |
| Omicron | 11 (11.6%) |
| Blood tests | |
| Hemoglobin (mmol/L) | 68; 8.70 (8.30, 9.50) |
| Hematocrit (L/L) | 58; 0.42 (0.40, 0.46) |
| Thrombocytes (109/L) | 62; 259.00 (206.50, 295.25) |
| Leukocytes (109/L) | 62; 6.70 (5.62, 8.38) |
| Eosinophiles (109/L) | 55; 0.12 (0.08, 0.20) |
| Basophiles (109/L) | 54; 0.04 (0.03, 0.06) |
| Neutrophiles (109/L) | 49; 3.65 (2.98, 4.62) |
| Lymphocytes (109/L) | 54; 2.04 (1.70, 2.54) |
| Monocytes (109/L) | 54; 0.55 (0.45, 0.70) |
| Creatinine (μmol/L) | 63; 79.00 (66.00, 88.00) |
| EGFR (mL/min/1.73 m2) | 63; 89.00 (72.50, 90.00) |
| ALAT (U/L) | 56; 25.50 (18.75, 35.25) |
| ASAT (U/L) | 53; 22.00 (19.00, 27.00) |
| LDH (U/L) | 55; 198.00 (168.00, 234.50) |
| CRP (mg/L) | 55; 2.20 (1.30, 6.00) |
| Glucose (mmol/L) | 39; 5.70 (5.25, 6.45) |
| Creatine Phosphokinase (U/L) | 34; 89.50 (66.25, 179.00) |
| Data (N = 95) | |
|---|---|
| Abnormalities | |
| Ground glass opacities/consolidations | 54 (56.8%) |
| Bronchiectasis | 19 (20.0%) |
| Subpleural reticulation | 23 (24.2%) |
| Honeycombing | 2 (2.1%) |
| Lymphadenopathy | 9 (9.5%) |
| Air trapping | 10 (10.5%) |
| Symptoms in 2 or Fewer Categories (N = 35) | Symptoms in More than 2 Categories (N = 60) | No Pulmonary Function Test/Radiological Abnormalities (N = 14) | Pulmonary Function Test/ Radiological Abnormalities (N = 78) | |
|---|---|---|---|---|
| General | ||||
| Age (Years) | 53.66 ± 6.24 | 54.43 ± 6.18 | 51.64 ± 5.62 | 54.56 ± 6.13 |
| Female | 10 (28.6%) | 37 (61.7%) | 9 (64.3%) | 36 (46.2%) |
| Smoking status | ||||
| Current smoker | 1 (2.9%) | 3 (5.0%) | 0 (0.0%) | 4 (5.1%) |
| Ex-smoker | 17 (48.6%) | 34 (56.7%) | 9 (64.3%) | 40 (51.3%) |
| Never smoker | 17 (48.6%) | 23 (38.3%) | 5 (35.7%) | 34 (43.6%) |
| BMI | ||||
| Normal | 3/34 (8.8%) | 7 (11.7%) | 2 (14.3%) | 8/77 (10.4%) |
| Overweight | 14/34 (41.2%) | 21 (35.0%) | 2 (14.3%) | 32/77 (41.6%) |
| Obese | 17/34 (50.0%) | 32 (53.3%) | 10 (71.4%) | 37/77 (48.1%) |
| Ethnicity | ||||
| Caucasian | 19/28 (67.9%) | 47/58 (81.0%) | 13 (92.9%) | 52/69 (75.4%) |
| African | 3/28 (10.7%) | 5/58 (8.6%) | 0 (0.0%) | 6/69 (8.7%) |
| Asian | 1/28 (3.6%) | 2/58 (3.4%) | 0 (0.0%) | 3/69 (4.3%) |
| Latin-American | 1/28 (3.6%) | 2/58 (3.4%) | 0 (0.0%) | 3/69 (4.3%) |
| Other | 4/28 (14.3%) | 2/58 (3.4%) | 1 (7.1%) | 5/69 (7.2%) |
| Level of education | ||||
| Secondary education | 7/26 (26.9%) | 12/53 (22.6%) | 0/13 (0.0%) | 18/63 (28.6%) |
| Vocational education | 7/26 (26.9%) | 26/53 (49.1%) | 7/13 (53.8%) | 24/63 (38.1%) |
| Bachelor | 6/26 (23.1%) | 13/53 (24.5%) | 5/13 (38.5%) | 14/63 (22.2%) |
| Master | 6/26 (23.1%) | 2/53 (3.8%) | 1/13 (7.7%) | 7/63 (11.1%) |
| Current comorbidities | ||||
| Asthma | 3 (8.6%) | 13/59 (22.0%) | 2/13 (15.4%) | 13 (16.7%) |
| COPD | 0 (0.0%) | 6/59 (10.2%) | 0/13 (0.0%) | 5 (6.4%) |
| Cardiovascular disease | 15 (42.9%) | 12/58 (20.7%) | 2/13 (15.4%) | 25/77 (32.5%) |
| Heart failure | 3 (8.6%) | 3/59 (5.1%) | 0/13 (0.0%) | 6 (7.7%) |
| Deep vein thrombosis and pulmonary embolism | 3 (8.6%) | 7/59 (11.9%) | 1/13 (7.7%) | 8 (10.3%) |
| Diabetes | 10 (28.6%) | 5/59 (8.5%) | 0/13 (0.0%) | 14 (17.9%) |
| Hepatic disease | 4/34 (11.8%) | 2/59 (3.4%) | 0/13 (0.0%) | 6/77 (7.8%) |
| Renal Failure | 4/33 (12.1%) | 3/59 (5.1%) | 0/13 (0.0%) | 6/76 (7.9%) |
| Interstitial lung disease | 0 (0.0%) | 2/59 (3.4%) | 0/13 (0.0%) | 2 (2.6%) |
| Neurological disorders | 2 (5.7%) | 1/59 (1.7%) | 0/13 (0.0%) | 3 (3.8%) |
| Rheumatic diseases | 1 (2.9%) | 8/59 (13.6%) | 2/13 (15.4%) | 7 (9.0%) |
| Acute COVID-19 characteristics | ||||
| No hospitalization | 2 (5.7%) | 8 (13.3%) | 5 (35.7%) | 4 (5.1%) |
| Hospitalization | 33 (94.3%) | 52 (86.7%) | 9 (64.3%) | 74 (94.9%) |
| Intensive care admission | 13 (37.1%) | 14 (23.3%) | 2 (14.3%) | 24 (30.8%) |
| Duration of hospitalization | 33; 12.00 (7.00, 21.00) | 51; 8.00 (4.50, 16.00) | 9; 7.00 (3.00, 8.00) | 73; 10.00 (6.00, 16.00) |
| Thrombosis | 8/34 (23.5%) | 6/57 (10.5%) | 2/13 (15.4%) | 12/75 (16.0%) |
| Pulmonary embolism | 5/34 (14.7%) | 10/58 (17.2%) | 1/13 (7.7%) | 14/76 (18.4%) |
| WHO disease Severity (mild) | 2 (5.7%) | 8 (13.3%) | 5 (35.7%) | 4 (5.1%) |
| WHO disease Severity (moderate) | 23 (65.7%) | 38 (63.3%) | 8 (57.1%) | 52 (66.7%) |
| WHO disease Severity (severe) | 10 (28.6%) | 14 (23.3%) | 1 (7.1%) | 22 (28.2%) |
| Oxygen supplementation and ventilation | ||||
| Nasal cannula | 14 (40.0%) | 26 (43.3%) | 4 (28.6%) | 36 (46.2%) |
| Non-rebreathing mask | 7 (20.0%) | 9 (15.0%) | 3 (21.4%) | 12 (15.4%) |
| Non-invasive ventilation | 2 (5.7%) | 3 (5.0%) | 0 (0.0%) | 5 (6.4%) |
| Invasive ventilation | 8 (22.9%) | 11 (18.3%) | 1 (7.1%) | 17 (21.8%) |
| Vaccination status | ||||
| No | 11 (31.4%) | 17 (28.3%) | 4 (28.6%) | 23 (29.5%) |
| Yes, 1 dose | 11 (31.4%) | 13 (21.7%) | 4 (28.6%) | 20 (25.6%) |
| Yes, 2 or more doses | 13 (37.1%) | 30 (50.0%) | 6 (42.9%) | 35 (44.9%) |
| Pharmacological treatment during acute COVID-19 | ||||
| Antivirals | 0/29 (0.0%) | 1/46 (2.2%) | 0/7 (0.0%) | 1/66 (1.5%) |
| Convalescent plasma | 0/17 (0.0%) | 0/28 (0.0%) | 0/5 (0.0%) | 0/39 (0.0%) |
| Antibiotics | 0/31 (0.0%) | 0/46 (0.0%) | 0/8 (0.0%) | 0/67 (0.0%) |
| Immunosuppressives | 32/33 (97.0%) | 46/50 (92.0%) | 8/9 (88.9%) | 68/72 (94.4%) |
| Other | 30/32 (93.8%) | 44/49 (89.8%) | 9/9 (100.0%) | 63/70 (90.0%) |
| Rest complaints | ||||
| Fatigue | 7 (20.0%) | 57 (95.0%) | 10 (71.4%) | 52 (66.7%) |
| Respiratory | 18 (51.4%) | 57 (95.0%) | 10 (71.4%) | 63 (80.8%) |
| Neurological | 11 (31.4%) | 54 (90.0%) | 10 (71.4%) | 53 (67.9%) |
| Cardiovascular | 1 (2.9%) | 24 (40.0%) | 3 (21.4%) | 21 (26.9%) |
| Gastrointestinal | 1 (2.9%) | 25 (41.7%) | 5 (35.7%) | 20 (25.6%) |
| Other | 2 (5.7%) | 16 (26.7%) | 4 (28.6%) | 13 (16.7%) |
| Dominant virus strains | ||||
| Beta | 15 (42.9%) | 12 (20.0%) | 1 (7.1%) | 25 (32.1%) |
| Gamma | 5 (14.3%) | 9 (15.0%) | 3 (21.4%) | 11 (14.1%) |
| Delta | 11 (31.4%) | 32 (53.3%) | 7 (50.0%) | 34 (43.6%) |
| Omicron | 4 (11.4%) | 7 (11.7%) | 3 (21.4%) | 8 (10.3%) |
| Blood tests | ||||
| Hemoglobin (mmol/L) | 24; 9.05 (8.38, 9.60) | 44; 8.55 (8.28, 8.93) | 9; 8.60 (8.30, 9.50) | 57; 8.70 (8.30, 9.50) |
| Hematocrit (L/L) | 19; 0.46 (0.43, 0.47) | 39; 0.42 (0.40, 0.44) | 7; 0.42 (0.40, 0.44) | 49; 0.42 (0.41, 0.46) |
| Thrombocytes (109/L) | 22; 246.50 (178.00, 273.75) | 40; 265.00 (236.75, 296.00) | 7; 265.00 (235.00, 302.00) | 53; 258.00 (206.00, 293.00) |
| Leukocytes (109/L) | 22; 7.15 (6.12, 8.88) | 40; 6.10 (5.50, 7.90) | 7; 7.00 (5.85, 7.80) | 53; 6.80 (5.60, 8.50) |
| Eosinophiles (109/L) | 19; 0.15 (0.10, 0.18) | 36; 0.11 (0.08, 0.19) | 7; 0.10 (0.08, 0.20) | 46; 0.13 (0.08, 0.20) |
| Basophiles (109/L) | 18; 0.04 (0.03, 0.07) | 36; 0.04 (0.02, 0.06) | 7; 0.05 (0.02, 0.08) | 45; 0.04 (0.03, 0.06) |
| Neutrophiles (109/L) | 15; 3.89 (3.44, 4.50) | 34; 3.57 (2.69, 4.59) | 6; 3.70 (3.45, 4.32) | 41; 3.85 (2.98, 4.83) |
| Lymphocytes (109/L) | 18; 2.39 (1.96, 3.14) | 36; 1.94 (1.55, 2.39) | 7; 1.90 (1.66, 2.50) | 45; 2.07 (1.70, 2.56) |
| Monocytes (109/L) | 18; 0.69 (0.52, 0.85) | 36; 0.50 (0.44, 0.60) | 7; 0.59 (0.53, 0.60) | 45; 0.54 (0.46, 0.71) |
| Creatinine (μmol/L) | 23; 84.00 (74.50, 101.50) | 40; 73.00 (65.75, 83.25) | 8; 70.50 (64.75, 76.50) | 53; 81.00 (68.00, 89.00) |
| EGFR (mL/min/1.73 m2) | 23; 87.00 (69.00, 90.00) | 40; 90.00 (75.25, 90.00) | 8; 88.50 (83.50, 90.00) | 53; 89.00 (72.00, 90.00) |
| ALAT (U/L) | 19; 29.00 (20.50, 35.50) | 37; 23.00 (18.00, 35.00) | 6; 21.50 (17.25, 28.00) | 48; 24.50 (19.75, 36.25) |
| ASAT (U/L) | 18; 23.00 (18.75, 25.50) | 35; 22.00 (19.50, 27.00) | 6; 21.00 (20.00, 23.50) | 45; 22.00 (18.00, 27.00) |
| LDH (U/L) | 18; 200.50 (182.00, 218.75) | 37; 194.00 (161.00, 242.00) | 6; 173.00 (170.00, 197.75) | 47; 202.00 (168.00, 237.00) |
| CRP (mg/L) | 17; 3.20 (2.00, 6.00) | 38; 2.00 (1.30, 6.00) | 7; 2.40 (1.50, 7.00) | 46; 2.10 (1.33, 6.00) |
| Glucose (mmol/L) | 14; 5.90 (5.32, 6.80) | 25; 5.50 (5.20, 6.30) | 2; 5.00 (4.75, 5.25) | 35; 5.70 (5.35, 6.45) |
| Creatine Phosphokinase (U/L) | 11; 115.00 (69.50, 221.00) | 23; 86.00 (66.50, 123.50) | 2; 91.00 (88.50, 93.50) | 30; 84.00 (66.00, 179.00) |
| NTProBNP (ng/L) | 17; 50.70 (50.00, 82.00) | 33; 50.70 (50.00, 99.90) | 7; 75.00 (50.70, 109.20) | 41; 50.70 (50.00, 87.00) |
| Score | # Abnormal (%) | |
|---|---|---|
| Physical function | ||
| PROMIS | 82; 28.72 ± 8.03 | 14/82 (17.1%) |
| Fatigue | ||
| FSS | 87; 5.56 (4.17, 6.28) | 66/87 (75.9%) |
| Cognitive functioning | ||
| CLC-IC | 80; 5.00 (2.00, 8.00) | 61/80 (76.3%) |
| Psychological functioning | ||
| HADS anxiety | 28; 4.00 (3.00, 10.25) | 11/28 (39.3%) |
| HADS depression | 27; 5.00 (1.50, 8.00) | 8/27 (29.6%) |
| PC-PTSD-5 | 83; 1.00 (0.00, 2.00) | 23/83 (27.7%) |
| Self care | ||
| EQ-5D, mobility | 84; 1.00 (1.00, 3.00) | 36/84 (42.7%) |
| EQ-5D, self-care | 84; 1.00 (1.00, 1.00) | 13/84 (15.5%) |
| EQ-5D, daily activities | 84; 2.00 (1.00, 3.00) | 57/84 (67.9%) |
| EQ-5D, pain/discomfort | 84; 2.00 (1.00, 3.00) | 55/84 (65.5%) |
| EQ-5D, anxiety/depression | 83; 1.00 (1.00, 2.00) | 30/83 (36.1%) |
| Participation | ||
| USER-P | 83; 80.00 (60.00, 96.82) | 22/83 (26.5%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baalbaki, N.; Blankestijn, J.M.; Abdel-Aziz, M.I.; de Backer, J.; Bazdar, S.; Beekers, I.; Beijers, R.J.H.C.G.; van den Bergh, J.P.; Bloemsma, L.D.; Bogaard, H.J.; et al. Precision Medicine for More Oxygen (P4O2)—Study Design and First Results of the Long COVID-19 Extension. J. Pers. Med. 2023, 13, 1060. https://doi.org/10.3390/jpm13071060
Baalbaki N, Blankestijn JM, Abdel-Aziz MI, de Backer J, Bazdar S, Beekers I, Beijers RJHCG, van den Bergh JP, Bloemsma LD, Bogaard HJ, et al. Precision Medicine for More Oxygen (P4O2)—Study Design and First Results of the Long COVID-19 Extension. Journal of Personalized Medicine. 2023; 13(7):1060. https://doi.org/10.3390/jpm13071060
Chicago/Turabian StyleBaalbaki, Nadia, Jelle M. Blankestijn, Mahmoud I. Abdel-Aziz, Jan de Backer, Somayeh Bazdar, Inés Beekers, Rosanne J. H. C. G. Beijers, Joop P. van den Bergh, Lizan D. Bloemsma, Harm Jan Bogaard, and et al. 2023. "Precision Medicine for More Oxygen (P4O2)—Study Design and First Results of the Long COVID-19 Extension" Journal of Personalized Medicine 13, no. 7: 1060. https://doi.org/10.3390/jpm13071060
APA StyleBaalbaki, N., Blankestijn, J. M., Abdel-Aziz, M. I., de Backer, J., Bazdar, S., Beekers, I., Beijers, R. J. H. C. G., van den Bergh, J. P., Bloemsma, L. D., Bogaard, H. J., van Bragt, J. J. M. H., van den Brink, V., Charbonnier, J. P., Cornelissen, M. E. B., Dagelet, Y., Davies, E. H., van der Does, A. M., Downward, G. S., van Drunen, C. M., ... Maitland-van der Zee, A. H., on behalf of the P4O2 consortium. (2023). Precision Medicine for More Oxygen (P4O2)—Study Design and First Results of the Long COVID-19 Extension. Journal of Personalized Medicine, 13(7), 1060. https://doi.org/10.3390/jpm13071060