Abstract
There are a number of devastating complications associated with peripheral artery disease, including limb amputations and acute limb ischemia. Despite the overlap, atherosclerotic diseases have distinct causes that need to be differentiated and managed appropriately. In coronary atherosclerosis, thrombosis is often precipitated by rupture or erosion of fibrous caps around atheromatous plaques, which leads to acute coronary syndrome. Regardless of the extent of atherosclerosis, peripheral artery disease manifests itself as thrombosis. Two-thirds of patients with acute limb ischemia have thrombi associated with insignificant atherosclerosis. A local thrombogenic or remotely embolic basis of critical limb ischemia may be explained by obliterative thrombi in peripheral arteries of patients without coronary artery-like lesions. Studies showed that thrombosis of the above-knee arteries was more commonly due to calcified nodules, which are the least common cause of luminal thrombosis associated with acute coronary events in patients with acute coronary syndrome. Cardiovascular mortality was higher in peripheral artery disease without myocardial infarction/stroke than in myocardial infarction/stroke without peripheral artery disease. The aim of this paper is to gather published data regarding the disparities of acute coronary syndrome with and without peripheral artery disease in terms of pathophysiology and mortality.
1. Introduction
More than 200 million adults suffer from peripheral artery disease in their lower extremities, which increases their risk of cardiovascular events (such as coronary heart disease, strokes, and leg amputations). Globally and in the United States, peripheral artery disease has gone underdiagnosed and undertreated due to a lack of awareness [1]. Generally speaking, lower-extremity peripheral artery disease refers to atherosclerotic diseases of the arteries supplying the limbs, from the aortoiliac segments to the pedal arteries. Even though this disease is associated with adverse clinical outcomes, impaired physical function, and reduced physical activity, it has been understudied and underrecognized compared with other atherosclerotic diseases such as myocardial infarction. In recent years, there has been mounting evidence that peripheral artery disease is significantly linked to mortality, primarily as a risk factor for future myocardial infarctions and strokes. Also, peripheral artery disease can cause devastating complications that result in limb amputations and acute limb ischemia. Despite the overlap, the causes of atherosclerotic diseases are not the same and the need for the appropriate diagnosis and treatment remains a major concern for medicine. Clinically, peripheral artery disease and coronary artery disease overlap due to their shared risk factors. In these patients, hyperlipidemia and type II diabetes mellitus were significant comorbidities. In addition to accelerating atherosclerosis development, diabetes mellitus affects the characteristic of atherosclerotic lesions in the lower extremities [2,3]. Compared with patients with PAD (peripheral artery disease) and without diabetes mellitus, patients who have PAD and coexisting diabetes mellitus have more arteries below the knee that are affected and more multilevel lesions [4,5,6]. Although patients with diabetes mellitus benefit from medical and endovascular procedures to manage atherosclerotic cardiovascular diseases, restenosis is a significant factor that may worsen the prognosis and may be associated with the necessity of reintervention [7]. The presence of dyslipidemia is associated with both changes in basic lipid parameters and modified lipoproteins, which are not routinely measured in clinical practice. Nitrated lipoproteins are oxidatively modified lipoproteins discussed in the context of cardiovascular dysfunction development. However, their role remains unclear at this time [8]. Many studies have found that coronary artery disease and peripheral artery disease are frequently coexisting conditions. Saleh et al. suggested that there was a significant increase in peripheral artery disease prevalence among those with coronary artery disease compared with those with normal coronaries [9]. Despite being under the care of a cardiovascular specialist, studies have shown that one out of six patients with coronary artery disease had an unrecognized peripheral artery disease [10].
The ankle-brachial index’s high positive predictive value and the high prevalence of peripheral artery disease with coronary artery disease suggest a high degree of suspicion for, and pretest probability for, coronary artery disease in a patient with peripheral artery disease. Coronary artery disease diagnosis is highly dependent on cardiac imaging tests such as electrocardiograms, stress electrocardiograms, myocardial perfusion imaging, and coronary angiographies. Kumar et al. say pretest probabilities can be increased through the ankle-brachial index, but it cannot replace the above testing methods [11].
Many factors contribute to this lack of knowledge about peripheral artery disease. Various nomenclatures and definitions have been used to describe peripheral artery disease, making effective communication challenging [12]. It is also likely that the clinical presentation of peripheral artery disease contributes to confusion regarding peripheral artery disease. A small percentage of patients are diagnosed with intermittent claudication, with either no exertional leg symptoms (up to 50%) or atypical leg symptoms (almost 50%) [13]. Patients may experience leg pain that begins at rest, or that does not interfere with walking, or that resolves with rest. These symptoms can be confused with arthritis or degenerative spinal disease. Various adverse outcomes can occur as a result of peripheral artery disease. To improve overall outcomes among this growing and undertreated population, increasing awareness about the definition, diagnosis, clinical manifestations, and complications of peripheral artery disease is critical.
Coronary atherosclerosis often manifests as an acute coronary syndrome, where thrombosis is precipitated by rupture or erosion of the fibrous caps of atheromatous plaques. It is common for plaque ruptures to have large necrotic cores, as well as thin, inflamed fibrous caps. Regardless of the extent of atherosclerosis, peripheral artery disease manifests as thrombosis. In peripheral arteries with significant stenosis, approximately 75% of them are blocked by thrombi. Two-thirds of them also have thrombi associated with insignificant atherosclerosis. A local thrombogenic or remotely embolic basis of critical limb ischemia may be explained by obliterative thrombi in peripheral arteries of patients without coronary artery-like lesions [14].
This study aims to study the prevalence of peripheral arterial disease and its correlation with the severity and characteristics of patients’ coronary disease, as well as its impact on in-hospital mortality and major adverse cardiac. The prevalence of peripheral arterial disease varies in the studies carried out so far.
2. Anatomy of Coronary Arteries: Normal and Pathological Aspects
The epicardial coronary artery systems are the left and right coronary arteries, which normally arise from the left and right ostia, located in the sinuses of Valsalva [15,16]. A separate ostium in the right sinus gives rise to the “third coronary artery” in about half of humans [17]. Several smaller ostia can be found in the right sinus, giving rise to multiple right ventricular branches [18,19].
The right coronary artery travels down the right atrioventricular groove, toward the crux of the heart. In addition to supplying blood to the right ventricle, the right coronary artery supplies 25% to 35% of the left ventricle. The main branches of the right coronary artery are the following: the conus artery, the sinoatrial nodal artery, the acute marginal artery, and the posterior descending artery [20].
The left main coronary artery has an overall mean length of 10.5 ± 4 mm for men and 10 ± 3 mm for women, it enters the coronary sulcus after passing between the main pulmonary artery and the left auricle, and bifurcates into the left anterior descending artery and the left circumflex [21].
From the bifurcation of the left main coronary artery, the left anterior descending artery continues around the left side of the pulmonary artery and descends in the epicardial fat into the anterior interventricular sulcus of the heart; its normal length is from 10 cm to 13 cm [22]. There are three segments of the left anterior descendent artery: a proximal segment (from the origin to the first septal artery), a middle segment (from the first septal to the origin of the first diagonal branch), and a distal segment (from the origin of the first diagonal artery to the apex). There are a number of diagonal branches of the left anterior descending artery, one or two large branches that are usually present along the anterior surface of the left ventricle, and the septal perforator branches, which supply the anterior 2/3 of the basal interventricular septum and the entire septum at its mid and apical levels [20,22,23].
From the left main coronary artery bifurcation, the left circumflex artery traverses the coronary sulcus and the diaphragmatic surface before terminating at the posterior interventricular sulcus. In contrast with the right coronary artery and left anterior descending arteries, the circumflex artery has only two segments, called the proximal segment and distal segment [24]. Its normal length is from 5 cm to 8 cm. There are several branches that originate from the left circumflex artery, including the left marginal artery, the posterolateral branch, and the obtuse marginal branch, which supplies a portion of the inferior wall [20,23].
3. Anatomy of Lower Extremity Arteries: Normal Aspects
To maintain the body’s mobility, lower extremity arteries supply oxygenated blood to muscles, tendons, and nerves. Several diseases can affect these arteries, which inhibit the optimal function of the limb. Lower-extremity arteries originate from the iliac artery at the point where the abdominal aorta is divided into the two common iliac arteries and the median sacral artery, approximately at the fourth lumbar vertebral body [25,26].
There are two branches of the common iliac artery, the internal and the external. A portion of the external iliac artery runs down into the lower limbs and becomes the common femoral artery [27]. Among the small branches of the common femoral artery, there are the superficial epigastric artery, external pudendal artery, and superficial circumflex artery. The common femoral artery divides into the superficial and deep femoral arteries.
Through Hunter’s canal, the superficial femoral artery travels along the medial side of the thigh. Once it exits the adductor canal, the superficial femoral artery courses posteriorly, where it is called the popliteal artery after it passes through the adductor hiatus. Approximately at the level of the proximal tibiofibular joint, the popliteal artery divides into the anterior tibial artery and the tibioperoneal trunk [28]. The anterior tibial artery runs along the anterior surface of the interosseus membrane, and there is a continuation of this artery in the foot as the dorsalis pedis artery. Located along the posteromedial aspect of the leg, the tibioperoneal trunk further divides into the peroneal artery and posterior tibial artery [25]. There are two arches on the medial and lateral surfaces of the plantar surface, formed by the posterior tibial artery. Besides giving rise to the metatarsals, the plantar arch is also responsible for producing the plantar digital arteries. Above the ankle joint, the peroneal artery divides into two calcaneal branches, one on the medial side and one on the lateral side. As a result of free communication with the dorsalis pedis artery and posterior tibial artery, these branches assist in the collateralization of the foot when it is sick or injured [29].
4. Atherosclerosis
Atherosclerosis is a chronic inflammatory disease with complex etiopathogenesis, which results in the development of atherosclerotic plaques, leading to the formation of narrowing and/or occlusion of the arteries [30,31]. This clinically may lead to the development of ischemic heart disease, cerebrovascular disease, or peripheral arterial disease [32,33,34,35]. In clinical practice, lowering the level of LDL cholesterol (low-density lipoprotein cholesterol) is the primary therapeutic objective of lipid-lowering therapy due to the role that oxidatively modified LDL particles play in atherosclerosis [36,37,38]. Additionally, we observe patients with advanced atherosclerosis and normal LDL concentrations in clinical practice, and such patients are also eligible for statin therapy. There are many pleiotropic effects associated with statins, which are mainly used for lowering cholesterol, and thus they are not only lipid-lowering drugs [37]. To achieve a target level for LDL cholesterol, statins and PCSK9 inhibitors (proprotein convertase subtilisin/kexin type 9) are effective [39,40,41]. There is no doubt that both of them are effective in controlling LDL cholesterol and reducing major adverse cardiovascular events by about 50% [42]. After controlling LDL cholesterol, the remaining risk for major adverse cardiovascular events is believed to be due to inflammation. As part of the CANTOS trial, it was shown that canakinumab, an antibody that blocks IL-1β (interleukin-1β), reduces major adverse cardiovascular events [43,44,45,45,46,47].
As a result of atherosclerosis, there is an autoimmune response to LDL and other antigens which could lead to an escalation or amelioration of the disease’s progression. There have been some recent advances in immunotherapy and vaccination that have shown promise in curbing atherosclerosis in animal models [48]. Based on the theory of the modulation of atherogenesis by adaptive immune responses, especially the CD4+ T cells that recognize self-antigens, a novel type of therapy that targets the adaptive immune response has been developed to address this phenomenon [49].
4.1. Pathogenesis of Atherosclerosis
Early-stage atherosclerosis is characterized by cell formation which is the result of lipid accumulation in the cells [50,51,52]. Inflammatory cytokines are released by damaged endothelial cells, which recruit monocytes through the endothelium and then differentiate into macrophages. Differentiated macrophages consume oxidized low-density lipoprotein (ox-LDL) through the scavenger receptors LOX-1, CD36, and SR-A1, which hydrolyze cholesteryl esters within lysosomes. By contrast, free cholesterol is esterified by acyl-CoA cholesterol acyltransferase 1 (ACAT1), while cholesteryl ester is hydrolyzed by neutral cholesteryl ester hydrolase (nCEH) and cholesteryl ester hydrolase (CEH) [51,53]. A large amount of free cholesterol is toxic to cells, so it must be efficiently removed from cells by ABCA1 and ABCG1 transporters [54,55]. When the above cholesterol homeostasis is disturbed, excessive cholesterol ester or free cholesterol will accumulate, causing foam cell formation or cell necrosis.
4.2. Immune Response in Atherosclerosis
Atherosclerotic plaques can become unstable, rupture, or erode over time, causing major cardiovascular complications [55,56,57,58,59]. There is a direct correlation between plaque stability and the level of inflammatory cells as well as the thickness of the cap of the plaque. Plaques that have thin caps and are full of immune cells are referred to as soft or vulnerable plaques. To initiate immune cell infiltration, chemokines and adhesion molecules play a major role. An antigen-presenting cell is a cell that generates major histocompatibility complex molecules, costimulatory molecules, and cytokines upon the presence of antigens that are produced by pathogens, bacteria, or altered self to determine the polarization of the adaptive immune response.
In the arterial adventitia and neointima, there are macrophages and dendritic cells that are activated by TLR ligands (Toll-like receptors) and scavenger receptors [60]. As inflammation cytokines increase in amount and intensity, atherosclerosis gets worse, and more immune cells are attracted to the area. The inflammatory cytokine IL-1β is an effective target for the treatment of atherosclerosis and other vascular diseases [58].
Marchini et al. suggested that at the maturation stage of atherosclerotic plaque, atherosclerosis-antigen-specific T cells release cytokines, perpetuate inflammation, and help an immune cell infiltrate develop over time [61] (Figure 1).
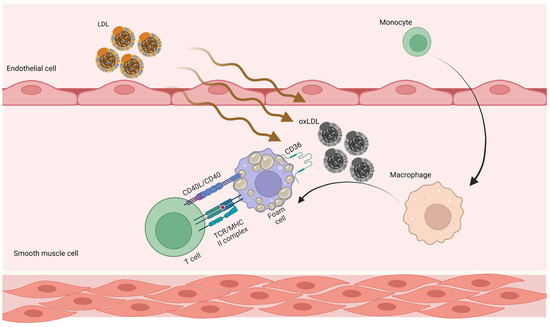
Figure 1.
Adaptive immune responses in atherosclerosis. LDL penetrates the artery wall and experiences modification by oxidative and enzymatic processes. The modified LDL molecules promote the expression of leukocyte adhesion molecules. Monocytes invade the vascular wall and mature into macrophages, differentiating into foam cells after taking up large volumes of oxidized LDL. T cells become active throughout this process and release mediators, which subsequently increase the immune reaction and lead to atherogenesis. LDL, low-density lipoprotein; oxLDL, oxidized low-density lipoprotein [62].
There is always an autoimmune response associated with atherosclerosis. There are antibodies to oxidized (oxLDL) LDL that are produced by plasma cells derived from the B cell, and these antibodies can be detected in the serum of humans and animals suffering from atherosclerosis. The presence of T cells against antigens associated with atherosclerosis is also found. For some time now, regulating CD4+ T cells (Tregs) have been shown to protect mice from atherosclerosis in animal models [63]. Our recent studies showed that CD4+ T cells specific for the core lipoprotein ApoB (apolipoprotein B), which is involved in LDL, very low-density lipoproteins, and chylomicron, are mostly Tregs in people without cardiovascular disease, but assume mixed and effector phenotypes in those with cardiovascular disease [49,64]. There is some evidence that atheroprotection may involve other T- and B-cell subsets, and this is an area of active research.
4.3. Atherosclerosis and Autoreactive CD4+ T cells
A majority of CD4+ T cells present in atherosclerotic lesions are memory T cells (CD45RO+) and are responsible for producing inflammatory cytokines in response to oxLDL. Several immunogenic epitopes have been identified and used as vaccine antigens against atherosclerosis in animal models derived from mouse ApoB (Apolipoprotein B).
Until recently, there has not been any direct proof that CD4+ T cells specific for ApoB epitopes exist in the body. To answer this question, scientists developed MHC-II tetramers for detecting such cells in mice as well as humans. ApoB epitope P18 is identical in mice (ApoB) and humans (APOB). P18 binds the mouse MHC-II allele I-Ab and DRB1*07:01 (presented in about 8% of humans). To detect APOB-specific CD4+ T cells, scientists created human APOB-peptide P18:DRB1*07:01 tetramers and found that P18-recognizing CD4+ T cells exist in human peripheral blood mononuclear cells. The presence of these cells was found in subjects both with and without subclinical cardiovascular disease [49]. The results of this study are the first in a series of studies to demonstrate that there are self-peptide-recognizing CD4+ T cells within human peripheral blood mononuclear cells. During the progression of atherosclerosis, the phenotypes of these cells seem to change [64,65,66,67,68,69].
4.4. Future Atherosclerosis Prevention
There is no doubt that vaccination is one of the most successful interventions in medicine. In recent years, vaccine development has moved from vaccine development for infectious diseases to vaccine development for non-communicable diseases, such as cancer, atherosclerosis, hypertension, Alzheimer’s disease, and diabetes mellitus. Identifying vaccine antigens is the first step in developing an atherosclerosis vaccine. PCSK9 (proprotein convertase subtilisin/kexin type 9), HSP65, and ApoB are some of the possible antigens that may be used as atherosclerosis vaccine antigens [70]. There are already antibodies against PCSK9 that are being used in clinical trials. As far as targeting PCSK9 is concerned, it is known to be safe because humans with null mutations in PCSK9 are asymptomatic except for the fact that they are resistant to atherosclerosis [71].
There is currently no information available regarding how long vaccination-induced atheroprotection lasts, how often the vaccine needs to be administered, and what would be the most effective dose, formulation, and route of administration for this vaccine.
5. Diagnostic Approach to Coronary Artery Disease
The first step is to evaluate the patient’s general condition and quality of life by assessing the comorbidities, symptoms, and signs. While physical examination findings generally do not indicate that acute coronary syndromes are present, thorough patient evaluation is essential for assessing immediate risk, recognizing hemodynamic collapse, and identifying mechanical complications associated with myocardial infarction. The presence of a tachycardia, narrow pulse pressure, hypotension, and signs of congestion (for example, pulmonary oedema) or inadequate perfusion (for example, cool extremities) are all indicators of a high clinical risk. With the Killip classification, patients with acute coronary syndromes are classified according to the degree of clinical heart failure, ranging from no signs of congestive heart failure (Class I) to cardiogenic shock (Class IV), and this classification is highly predictive of mortality [72,73]. Typically, mechanical complications from myocardial infarction are accompanied by abrupt haemodynamic deterioration and a loud holosystolic murmur in the left parasternal region in cases of acute ventricular septal rupture, soft systolic murmurs in cases of acute mitral regurgitation, and signs of tamponade when free wall rupture occurs [74].
The diagnosis of acute coronary syndrome is based on clinical presentation, ECG (electrocardiogram) findings, and biochemical evidence of myocardial injury. In the immediate context of a patient suspected of having acute coronary syndrome, it is important to rule out the presence or absence of ST-segment elevations on a 12-lead electrocardiogram [75,76].
Since the development of high-sensitivity troponin (hsTn), the diagnosis of NSTEACS (non-ST-elevation acute coronary syndromes), which include unstable angina and NSTEMI (non-ST segment elevation myocardial infarction), has advanced significantly. NSTEACS may present with T-wave inversions or ST-segment depressions on the ECG, but these findings are not necessary for diagnosis. NSTEMI is distinguished from unstable angina by elevated levels of myocardial necrosis markers such as cardiac troponin I and T (cTnI and cTnT) or creatine kinase-myocardial band (CK-MB). This is usually accompanied by an initial rise and a peak, followed by a fall in the concentration of the biomarker [77,78].
The most recent European and American guidelines emphasize the importance of emergent reperfusion therapy for patients who manifest ST-segment elevation infarction [76,79]. If a patient presents to a hospital that has the capability of performing percutaneous coronary intervention (PCI), immediate coronary angiography should be performed with a goal of limiting the time from first medical contact to the insertion of the device to less than 60–90 min. Unless PCI is possible within this timeframe, fibrinolysis should be administered if not contraindicated, and a pharmaco-invasive approach should be considered, in which fibrinolytic therapy is followed by invasive angiography within 24 h [76,79].
In regard to NSTEACS, the optimal time for catheterization continues to be debated. In the most critical cases (such as those with hemodynamic instability, chest discomfort that persists or arrhythmia that poses a life-threatening danger), emergent angiography should be performed within two hours of hospital admission. Those with a high risk of coronary heart disease (e.g., GRACE scores >140) will undergo catheterization within 24 h, while those with a low risk will undergo selective procedures [76].
The electrocardiogram and the assessment of the function of the left ventricle are included in the basic testing. All patients should undergo a resting transthoracic echocardiogram to rule out alternative causes of angina, to detect regional wall motion abnormalities indicative of coronary artery disease, to assess left ventricle ejection fraction for risk-stratification purposes, and to assess diastolic function [80].
In patients with suspected or established CCS (chronic coronary syndrome), the following clinical scenarios are most frequently encountered: patients with suspected CAD (coronary artery disease) and stable anginal symptoms and/or dyspnoea; patients with new onset of heart failure or left ventricular dysfunction and suspected CAD; asymptomatic and symptomatic patients with stabilized symptoms < 1 year after an ACS; patients with recent revascularization; asymptomatic and symptomatic patients > 1 year after initial diagnosis or revascularization; patients with angina and suspected vasospastic or microvascular disease; and asymptomatic subjects in whom CAD is detected at screening [1].
Based on recent meta-analyses of the performance of diagnostic tests for the detection of anatomically (>50%) and functionally significant coronary artery disease, there is different sensitivity and specificity between computed tomography angiography, positron emission tomography, single-photon emission computed tomography (exercise with or without dipyridamole or adenosine), stress cardiac magnetic resonance, stress echo exercise, stress echocardiography, and invasive angiography [80].
The presence of peripheral artery disease (PAD) is an essential factor to consider when discussing the outcomes of percutaneous coronary intervention (PCI) and coronary artery bypass grafting (CABG) for patients with acute coronary syndrome (ACS). Patients with PAD face unique challenges when undergoing these procedures, making outcomes assessment particularly significant.
The extent of PAD can significantly influence the treatment of ACS and can affect the outcomes of PCI and CABG. Patients with PAD may have a higher risk of adverse events following PCI, including mortality, major bleeding, and urgent revascularization [81]. Likewise, CABG may be associated with higher stroke rates and re-operation in PAD patients. As such, it is essential to consider the presence of PAD when assessing PCI and CABG outcomes for ACS patients [82]. This may involve additional risk stratification, pre-procedural testing, and post-procedural monitoring [83].
6. Diagnostic Approach to Peripheral Artery Disease
As a result of technological advances over the past decade, noninvasive imaging has become a very effective tool for assessing the anatomy and severity of arterial stenosis in patients with peripheral artery disease. The main advantages of this technology are its ability to image distal vessels with calcification, a lower contrast dose, and a higher spatial resolution, among others [84].
Patients with peripheral arterial disease often experience intermittent claudication. Intermittent claudication occurs when blood circulation to the muscles is blocked due to obstruction to arterial flow during exercise, resulting in pain in the calves and less commonly the hips and buttocks. There is a range of severity for symptoms, which is summarized on Fontaine’s scale (Table 1) and Rutherford’s scale (Table 2) [85,86].

Table 1.
The Fontaine classification.
Table 2.
The Rutherford classification.
This first-line noninvasive diagnostic method is based on the ratio of ankle-to-brachial systolic blood pressure, a measurement that requires standard measurement methodology. The presence of peripheral artery disease is determined by an ankle-to-brachial index ≤0.90 [87]. There are many cases of peripheral arterial stenosis even when the ABI is normal or elevated; in such cases the toe-brachial-index (TBI) should be used. To calculate TBI, it is commonly recommended to use the great toe artery pressure since the vessels of the toes are not usually affected by media sclerosis [88]. TBI’s utility in diabetic patients makes it the method of choice to evaluate lower-limb perfusion when there is overt arterial wall calcification. According to the algorithm devised by Park et al., wound management is recommended if the ABI is less than 0.9 or if the TBI is less than 0.6 after angiography. Further, if the TBI was less than 0.6 in patients with normal ABI values, angiography was performed prior to wound treatment. In patients with diabetic gangrene, this treatment algorithm will allow more rapid detection of PAD, improving wound management and reducing hospitalizations [89].
The definition of chronic limb-threatening ischemia (CLTI), the most severe form of peripheral arterial disease, should encompass a broader and more heterogeneous group of patients with varying degrees of ischemia that may delay wound healing and increase the risk of amputation. A clearer concept of CLTI needs to be developed by excluding the following individuals from the population as defined by the guideline document: patients with purely venous ulcers, acute limb ischemia (ALI), acute trash foot, ischemia caused by emboli, acute trauma, or mangled extremities, as well as those with wounds associated with non-atherosclerotic conditions [14,90,91]. In order to establish a diagnosis of CLTI, an objectively documented atherosclerotic PAD must be associated with ischemic rest pain or tissue loss (ulceration or gangrene) [92]. Ischemic rest pain should persist for at least two weeks and be associated with at least one abnormal hemodynamic parameter: (ABI) < 0.4, absolute highest AP (ankle pressure) < 50 mm Hg, absolute TP (posterior tibial artery) < 30 mm Hg, transcutaneous partial pressure of oxygen (TcPo2) < 30 mm Hg, or flat or minimally pulsatile pulse volume recording (PVR) waveforms. Since the 1950s, a number of different classification systems for lower-limb ischemia and wounds have been developed and promulgated [91]. Among the most widely accepted classifications are the Fontaine and Rutherford classifications [86].
Acute limb ischemia (ALI) refers to a rapid decrease in lower-limb blood flow caused by an acute occlusion of a peripheral artery or bypass graft, and the prognosis is poor unless the condition is treated quickly and appropriately. Embolizations and thromboses are the most common etiologies, with a variety of comorbidities [92]. The symptoms of ALI are abrupt and include pain, numbness, and coldness of the lower limbs, along with paresthesia, contracture, and irreversible purpura. There are several treatments available for ALI, including open surgical revascularization, endovascular revascularization, and heparin administration within a short period of time. As a result of the poor prognosis for limb recovery, limb amputation should be performed without hesitation if the limb is irreversible [93,94,95,96].
Duplex ultrasound, computer tomographic angiography, magnetic resonance angiography, and invasive angiography have a different sensibility and specificity for detecting peripheral artery disease. For example, when comparing multidetector computer tomography with angiography, the sensitivity and specificity of multidetector computer tomography for detecting peripheral artery disease is 90% [97,98,99].
However, to diagnose peripheral artery disease, catheter-based angiography remains the gold standard, although it is now limited to patients who are receiving endovascular revascularization as part of the process [100].
7. Pathology of Coronary Artery Disease and Acute Coronary Events
Approximately two-thirds of all acute coronary events are caused by the rupture of the thin-capped fibroatheromas in the plaque, while one-third are caused by plaque erosion caused by pathological intimal thickening or fibroatheroma in the plaque. The calcification of a nodule can sometimes penetrate beyond the fibrous cap and result in the formation of a thrombus. As a result of plaque rupture, a loss of integrity occurs in the fibrous cap, which is responsible for separating the necrotic core in the lumen of the artery from the blood. This defect is the primary cause of coronary thrombosis present in autopsies of patients who died unexpectedly [101,102]. During the rupture of the plaques, the necrotic cores constituted more than 30% of the plaque area. Several macrophages and a few smooth muscle cells were also present in the thick fibrous cap covering the plaques. There was a tendency for such plaques to be accompanied by spotty calcification, and the plaque cores often showed that hemorrhage had occurred.
Kolofgie et al. suggested that plaque hemorrhage is the result of leaky neovasculature caused by proliferating adventitial vessels, resulting in proliferating adventitial vasa vasorum, which further expands the plaque core, as the erythrocyte membranes are rich in free cholesterol [56].
There is a risk of large intraplaque hemorrhages due to neovessel ruptures. A plaque rupture can also result in luminal blood being able to reach the necrotic core of the plaque, contributing to the enlargement of the plaque, especially in the event of silent ruptures. There is intense inflammation within the disrupted plaques, which stretches from the fibrous cap to the necrosis and adventitious layer of the vessel wall [103]. As observed in this study, fibrous cap attenuation was one of the strongest predictors of high-risk plaques. It was found that stable plaques had a fibrous cap thickness of 85 microns, and disrupted and vulnerable plaques had a fibrous cap thickness of 55 microns [104,105]. Two other characteristics distinguished this type of plaque from others: the extent of inflammation within the plaque and the extent of necrosis within the plaque. Furthermore, the plaque was more likely to become unstable, as a result of a greater degree of luminal obstruction.
8. Pathology of Peripheral Artery Disease
In patients with coronary artery disease, sudden cardiac death and myocardial infarction are the most common adverse events that occur. When these situations occur, the underlying pathology is in situ thrombosis, which is primarily caused by rupture of the atherosclerotic plaque of the underlying atherosclerotic artery, and rarely by erosion of the plaque itself. In similar ways, acute limb ischemia is characterized by sudden decreases in perfusion in the limbs that can lead to tissue loss and may require early intervention to prevent further complications.
Acute limb ischemia in peripheral artery disease is, however, very different from acute coronary events wherein the underlying pathology is atherothrombosis. This is due to in situ thrombosis, embolisms from the heart and proximal vessels, and graft occlusion as well [106]. In general, ALI progresses into advanced limb ischemia within two weeks of its acute onset, and it is associated with a mortality rate of 15–20% due to concurrent illnesses, such as cardiovascular disease and ischemia–reperfusion injury [107]. Acute limb ischemia, excluding trauma, is generally classified as embolism and thrombosis. A recent report found that embolisms, thromboses caused by occlusive atherosclerotic lesions, complex factors, and stent or graft-related thromboses occur at rates of 46%, 24%, 20%, and 10%, respectively [107]. It is not uncommon for ALIs to occur due to peripheral embolisms caused by aneurysms of the popliteal artery and thrombotic occlusion of aneurysms.
Thrombosis occurs when chronic stenotic lesions in occlusive atherosclerosis break down, fail to circulate, or become hypercoagulable. There is often difficulty distinguishing embolism from thrombosis in the presence of stenotic arteriosclerosis obliterans lesions [107].
According to Narula et al., 239 arteries were pathologically examined in 75 patients with critical limb ischemia who had undergone 98 amputations above the knee and below the knee [108]. According to our study, one-fourth of the arteries with luminal stenosis of at least 70% had stenosis due to significant atherosclerosis without thrombi in the arteries. It has been reported that thrombi contributed to luminal compromise in two-thirds of patients, with only one-third of these having significant atherosclerosis associated with it and the remainder having nonsignificant atherosclerosis associated with it. It is important to note that luminal thrombi associated with significant atherosclerosis were considered in situ thrombi possibly related to plaque rupture, erosion, or calcified nodules, whereas luminal thrombi associated with insignificant atherosclerosis suggest that they may be associated with thromboembolism. There was medial calcification in more than 70% of all arteries. While it is suggested that luminal thrombi associated with insignificant atherosclerosis are likely thromboembolic, it has also been suggested that the non-compliant vessels with medial calcification could have also contributed to luminal thrombi caused by the stasis of blood owing to the lack of mobility, infection, and non-compliant vessels [91].
9. Pathological Comparison of Arteries of Patients with Coronary Artery Disease and Peripheral Artery Disease
There are several clinical implications related to the pathological changes in the lower extremity arteries of patients with peripheral artery disease, specifically those who suffer from major adverse limb events. Among the most serious adverse limb events occur when the limb is severely ischemic and thus requires intervention or amputation due to vascular damage. Occlusion of large arteries by thrombus without significant atherosclerosis and the occlusion of small subcutaneous arteries by thrombus suggest the possibility of thromboembolism. It has been observed that repeated, layered thrombi are present in several arteries that are free of significant atherosclerosis, thus supporting the idea that emboli are repeated over time [91,109,110,111,112,113]. To further understand the factors that contribute to the development of thrombotic lesions, in addition to alterations in the coagulation cascade, infection, diminished mobility, and non-compliant vessels, additional studies are required. Acute coronary syndrome, on the other hand, is commonly associated with in situ luminal thrombus caused by the rupture of the thin-capped fibroatheroma plaque [114,115,116].
Torii et al. studied 3000 serial autopsies and showed that thrombosis of the above-knee arteries was more commonly due to calcified nodules, which are the least common cause of luminal thrombosis associated with acute coronary events in patients with acute coronary syndrome [110,117]. There is a higher prevalence of fibrocalcific plaques in the lower extremities as compared with the coronary arteries [110,118]. In patients with peripheral artery disease, calcification of the middle layers of arterial walls is common, but it is rare in the coronary arteries unless the patient also has advanced kidney disease [119]. Several pathological factors could contribute to the failure of any artery revascularization procedure, such as rigid, non-expansive, noncompliant large and small arteries with medial calcification of the intermediate vessels and distal vessel thrombosis [120].
In conclusion, occlusive complications caused by atherosclerotic lesions can occur locally or distally, depending on the extent of the disease. A plaque rupture, plaque erosion, or calcium-rich nodules protruding through the plaque surface are generally responsible for local complications. There is no better example than what we see in the presence of coronary artery disease [121,122,123]. There is, however, the possibility of embolic compromise in distal territories, whereby aortic, iliac, and femoral plaques can impair infra-popliteal arterial supply and result in critical limb ischemia.
10. Mortality and Cardiovascular Outcomes
When it comes to mortality in patients with peripheral artery disease, The Ankle to Brachial Cohort Study found a strong association between low (0.90) and high (>1.40) ankle-to-brachial results and all-cause and cardiovascular mortality [124]. The mortality rate was doubled in those with an ankle-to-brachial index between 0.81 and 0.90, while the mortality rate was quadrupled in those with an ankle-to-brachial index between 0.70 and 0.80. There has been evidence in multiple studies from a variety of populations demonstrating that persons with peripheral artery disease are more likely to develop other cardiovascular diseases as well, such as coronary heart disease, strokes, and aneurysms of the abdominal aorta [125,126].
Recent research has shown that peripheral artery disease is becoming increasingly important in the context of polyvascular disease. An example of this is a subset of patients with multiple vascular beds affected by atherosclerosis, including peripheral arterial disease. According to the FOURIER trial, peripheral artery disease in combination with myocardial infarction or stroke had the highest risk of major adverse cardiovascular events (cardiovascular mortality, myocardial infarction, and stroke) over 2.5 years, with a risk of 14.9% [127,128,129,130,131] (Figure 2).
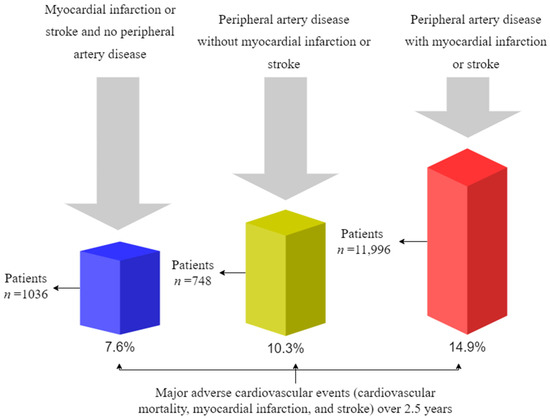
Figure 2.
Cumulative incidence of major adverse cardiovascular events in the placebo group according to CVD status at baseline [127]. CVD indicates cardiovascular disease.
There is an interesting finding in this study that peripheral artery disease without myocardial infarction/stroke was associated with a higher risk of major adverse cardiovascular events (10.3%) than myocardial infarction/stroke without peripheral artery disease (7.6%) [132,133,134,135,136].
Numerous studies have demonstrated a correlation between peripheral artery disease and increased mortality (Table 3) [127,137,138,139,140].
Table 3.
Studies examining the relationship between peripheral arterial disease and mortality.
The mortality and adverse outcomes associated with acute coronary syndrome and peripheral artery disease are not only unfortunate consequences of the natural progression of these diseases but can also result from medical, endovascular, or surgical interventions [141]. While potentially beneficial, these interventions can have unintended consequences that may result in death or other adverse outcomes.
11. Conclusions
Overall mortality rates for acute coronary syndromes and acute limb ischemia have declined in most developed countries by 24–50%. It is estimated that approximately half of this reduction in cardiovascular mortality can be attributed to changes in therapy, including secondary preventive measures following myocardial infarction and revascularization. Initial treatments, advancements in heart failure treatments, and revascularization for chronic angina contributed to this drop. The other half of the effect was caused by changes in risk factors, including reductions in total cholesterol, systolic blood pressure, smoking, and physical inactivity. In addition, detecting peripheral arterial disease and developing novel treatments can improve our therapeutic options.
Slowing the progression of peripheral artery disease is key to decreasing cardiovascular mortality. For now, lifestyle changes, dietary changes, and conventional therapies may seem like a winning combination, but vaccines might be the medicine of the future.
Author Contributions
Conceptualization, F.-A.G., D.B. and M.-R.P.; methodology, F.-A.G., D.B. and M.-R.P.; writing—original draft preparation, F.-A.G., D.B. and M.-R.P.; writing—review and editing, F.-A.G., D.B. and M.-R.P.; visualization, F.-A.G., D.B. and M.-R.P.; supervision, D.B. and M.-R.P.; project administration, F.-A.G. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
Publication of this paper was supported by the University of Medicine and Pharmacy Carol Davila, through the institutional program Publish not Perish.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Neumann, F.J.; Sechtem, U.; Banning, A.P.; Bonaros, N.; Bueno, H.; Bugiardini, R.; Chieffo, A.; Crea, F.; Czerny, M.; Delgado, V.; et al. 2019 ESC Guidelines for the Diagnosis and Management of Chronic Coronary SyndromesThe Task Force for the Diagnosis and Management of Chronic Coronary Syndromes of the European Society of Cardiology (ESC). Eur. Heart J. 2020, 41, 407–477. [Google Scholar] [CrossRef]
- Verner, V.A.; Mel’Nik, M.V.; Knjazeva, S.A. Cardio-Ankle Vascular Index (CAVI) in Diagnostics, Risk and Severity Evaluation of Magistral Vessels Lesion in Patients with Cardio-Vascular Diseases and Type 2 Diabetes. Ter. Arkhiv 2021, 93, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Thiruvoipati, T.; Kielhorn, C.E.; Armstrong, E.J. Peripheral Artery Disease in Patients with Diabetes: Epidemiology, Mechanisms, and Outcomes. World J. Diabetes 2015, 6, 961–969. [Google Scholar] [CrossRef] [PubMed]
- Foussard, N.; Dari, L.; Ducasse, E.; Rigalleau, V.; Mohammedi, K.; Caradu, C. Lower-Limb Peripheral Arterial Disease and Amputations in People with Diabetes: Risk Factors, Prognostic Value and Management. Presse Med. 2023, 52, 104164. [Google Scholar] [CrossRef]
- Chun, D.I.; Kim, S.; Kim, J.; Yang, H.J.; Kim, J.H.; Cho, J.H.; Yi, Y.; Kim, W.J.; Won, S.H. Epidemiology and Burden of Diabetic Foot Ulcer and Peripheral Arterial Disease in Korea. J. Clin. Med. 2019, 8, 748. [Google Scholar] [CrossRef] [PubMed]
- Jakubiak, G.K.; Pawlas, N.; Cieślar, G.; Stanek, A. Chronic Lower Extremity Ischemia and Its Association with the Frailty Syndrome in Patients with Diabetes. Int. J. Environ. Res. Public Health 2020, 17, 9339. [Google Scholar] [CrossRef]
- Jakubiak, G.K.; Pawlas, N.; Cieślar, G.; Stanek, A. Pathogenesis and Clinical Significance of In-Stent Restenosis in Patients with Diabetes. Int. J. Environ. Res. Public Health 2021, 18, 11970. [Google Scholar] [CrossRef]
- Aday, A.W.; Everett, B.M. Dyslipidemia Profiles in Patients with Peripheral Artery Disease. Curr. Cardiol. Rep. 2019, 21, 42. [Google Scholar] [CrossRef]
- Saleh, A.; Makhamreh, H.; Qoussoos, T.; Alawwa, I.; Alsmady, M.; Salah, Z.A.; Shakhatreh, A.; Alhazaymeh, L.; Jabber, M. Prevalence of Previously Unrecognized Peripheral Arterial Disease in Patients Undergoing Coronary Angiography. Medicine 2018, 97, 11519. [Google Scholar] [CrossRef]
- Moussa, I.D.; Jaff, M.R.; Mehran, R.; Gray, W.; Dangas, G.; Lazic, Z.; Moses, J.W. Prevalence and Prediction of Previously Unrecognized Peripheral Arterial Disease in Patients with Coronary Artery Disease: The Peripheral Arterial Disease in Interventional Patients Study. Catheter. Cardiovasc. Interv. 2009, 73, 719–724. [Google Scholar] [CrossRef]
- Kumar, A.; Bano, S.; Bhurgri, U.; Kumar, J.; Ali, A.; Dembra, S.; Kumar, L.; Shahid, S.; Khalid, D.; Rizwan, A.; et al. Peripheral Artery Disease as a Predictor of Coronary Artery Disease in Patients Undergoing Coronary Angiography. Cureus 2021, 13, 15094. [Google Scholar] [CrossRef] [PubMed]
- Aursulesei Onofrei, V.; Ceasovschih, A.; Marcu, D.T.M.; Adam, C.A.; Mitu, O.; Mitu, F. Mortality Risk Assessment in Peripheral Arterial Disease—The Burden of Cardiovascular Risk Factors over the Years: A Single Center’s Experience. Diagnostics 2022, 12, 2499. [Google Scholar] [CrossRef] [PubMed]
- Hirsch, A.T.; Criqui, M.H.; Treat-Jacobson, D.; Regensteiner, J.G.; Creager, M.A.; Olin, J.W.; Krook, S.H.; Hunninghake, D.B.; Comerota, A.J.; Walsh, M.E.; et al. Peripheral Arterial Disease Detection, Awareness, and Treatment in Primary Care. J. Am. Med. Assoc. 2001, 286, 1317–1324. [Google Scholar] [CrossRef] [PubMed]
- Hirsch, A.T.; Haskal, Z.J.; Hertzer, N.R.; Bakal, C.W.; Creager, M.A.; Halperin, J.L.; Hiratzka, L.F.; Murphy, W.R.C.; Olin, J.W.; Puschett, J.B.; et al. ACC/AHA 2005 Guidelines for the Management of Patients with Peripheral Arterial Disease (Lower Extremity, Renal, Mesenteric, and Abdominal Aortic): Executive Summary a Collaborative Report from the American Association for Vascular Surgery/Society for Vascular Surgery, Society for Cardiovascular Angiography and Interventions, Society for Vascular Medicine and Biology, Society of Interventional Radiology, and the ACC/AHA Task Force on Practice Guidelines (Writing Committee to Develop Guidelines f. J. Am. Coll. Cardiol. 2006, 47, 1239–1312. [Google Scholar] [CrossRef] [PubMed]
- Loukas, M.; Sharma, A.; Blaak, C.; Sorenson, E.; Mian, A. The Clinical Anatomy of the Coronary Arteries. J. Cardiovasc. Transl. Res. 2013, 6, 197–207. [Google Scholar] [CrossRef] [PubMed]
- Kosar, P.; Ergun, E.; Öztürk, C.; Kosar, U. Anatomic Variations and Anomalies of the Coronary Arteries: 64-Slice CT Angiographic Appearance. Diagn. Interv. Radiol. 2009, 15, 275–283. [Google Scholar] [CrossRef]
- Alexander, R.W.; Griffith, G.C. Anomalies of the Coronary Arteries and Their Clinical Significance. Circulation 1956, 14, 800–805. [Google Scholar] [CrossRef]
- Rabin, D.N.; Rabin, S.; Mintzer, R.A. A Pictorial Review of Coronary Artery Anatomy on Spiral CT. Chest 2000, 118, 488–491. [Google Scholar] [CrossRef][Green Version]
- Woodhouse, C.; Janowitz, W.; Viamonte, M. Coronary Arteries: Retrospective Cardiac Gating Technique to Reduce Cardiac Motion Artifact at Spiral CT. Radiology 1997, 204, 566–569. [Google Scholar] [CrossRef]
- Von Lüdinghausen, M. The Clinical Anatomy of Coronary Arteries. In Advances in Anatomy, Embryology and Cell Biology; Springer: Berlin/Heidelberg, Germany, 2003; Volume 167, ISBN 978-3-540-43689-8. [Google Scholar]
- De Cecco, C.N.; Bastarrika, G.; Arraiza, M.; Maurizi Enrici, M.; Pueyo, J.; Muscogiuri, G.; Fina, P.; Anselmi, A.; Di Girolamo, M.; David, V. Dual Source CT: State of the Art in the Depiction of Coronary Arteries Anatomy, Anatomical Variants and Myocardial Segments. Minerva Cardioangiol. 2012, 60, 133–146. [Google Scholar]
- Young, P.M.; Gerber, T.C.; Williamson, E.E.; Julsrud, P.R.; Herfkens, R.J. Cardiac Imaging: Part 2, Normal, Variant, and Anomalous Configurations of the Coronary Vasculature. Am. J. Roentgenol. 2012, 197, 816–826. [Google Scholar] [CrossRef] [PubMed]
- Medrano-Gracia, P.; Ormiston, J.; Webster, M.; Beier, S.; Young, A.; Ellis, C.; Wang, C.; Smedby, Ö.; Cowan, B. A Computational Atlas of Normal Coronary Artery Anatomy. EuroIntervention 2016, 12, 845–854. [Google Scholar] [CrossRef] [PubMed]
- Randhawa, A.; Saini, A.; Aggarwal, A.; Gupta, T.; Saikia, U.N.; Rohit, M.K.; Sahni, D. Variant Origin and Course of Left Circumflex Coronary Artery. Surg. Radiol. Anat. SRA 2017, 39, 333–336. [Google Scholar] [CrossRef] [PubMed]
- Qazi, E.; Wilting, J.; Patel, N.R.; Alenezi, A.O.; Kennedy, S.A.; Tan, K.T.; Jaberi, A.; Mafeld, S. Arteries of the Lower Limb-Embryology, Variations, and Clinical Significance. Can. Assoc. Radiol. J. 2022, 73, 259–270. [Google Scholar] [CrossRef]
- Chen, Q.; Shi, Y.; Wang, Y.; Li, X. Patterns of Disease Distribution of Lower Extremity Peripheral Arterial Disease. Angiology 2015, 66, 211–218. [Google Scholar] [CrossRef]
- Xie, D.; Na, J.; Zhang, M.; Dong, S.; Xiao, X. CT Angiography of the Lower Extremity and Coronary Arteries Using 256-Section CT: A Preliminary Study. Clin. Radiol. 2015, 70, 1281–1288. [Google Scholar] [CrossRef]
- Kropman, R.H.J.; Kiela, G.; Moll, F.L.; De Vries, J.P.P.M. Variations in Anatomy of the Popliteal Artery and Its Side Branches. Vasc. Endovasc. Surg. 2011, 45, 536–540. [Google Scholar] [CrossRef]
- Shah, S.; Fischman, A.; Marin, M.; Won, J. Spontaneous Tibioperoneal Trunk and Anterior Tibial Artery Pseudoaneurysms. Vasc. Med. 2012, 17, 164–167. [Google Scholar] [CrossRef]
- Pedro-Botet, J.; Climent, E.; Benaiges, D. Atherosclerosis and Inflammation. New Therapeutic Approaches. Med. Clin. 2020, 155, 256–262. [Google Scholar] [CrossRef]
- Zárate, A.; Manuel-Apolinar, L.; Basurto, L.; De la Chesnaye, E.; Saldívar, I. Cholesterol and Atherosclerosis. Historical Considerations and Treatment. Arch. Cardiol. Mex. 2016, 86, 163–169. [Google Scholar] [CrossRef]
- Sarmah, D.; Datta, A.; Raut, S.; Sarkar, A.; Shah, B.; Bohra, M.; Singh, U.; Jagtap, P.; Baidya, F.; Kalia, K.; et al. The Role of Inflammasomes in Atherosclerosis and Stroke Pathogenesis. Curr. Pharm. Des. 2020, 26, 4234–4245. [Google Scholar] [CrossRef]
- Shi, Y.; Guo, L.; Chen, Y.; Xie, Q.; Yan, Z.; Liu, Y.; Kang, J.; Li, S. Risk Factors for Ischemic Stroke: Differences between Cerebral Small Vessel and Large Artery Atherosclerosis Aetiologies. Folia Neuropathol. 2021, 59, 378–385. [Google Scholar] [CrossRef]
- Razavi, A.C.; Agatston, A.S.; Shaw, L.J.; De Cecco, C.N.; van Assen, M.; Sperling, L.S.; Bittencourt, M.S.; Daubert, M.A.; Nasir, K.; Blumenthal, R.S.; et al. Evolving Role of Calcium Density in Coronary Artery Calcium Scoring and Atherosclerotic Cardiovascular Disease Risk. Cardiovasc. Imaging 2022, 15, 1648–1662. [Google Scholar] [CrossRef]
- Fioranelli, M.; Bottaccioli, A.G.; Bottaccioli, F.; Bianchi, M.; Rovesti, M.; Roccia, M.G. Stress and Inflammation in Coronary Artery Disease: A Review Psychoneuroendocrineimmunology-Based. Front. Immunol. 2018, 9, 2031. [Google Scholar] [CrossRef] [PubMed]
- Weitgasser, R.; Ratzinger, M.; Hemetsberger, M.; Siostrzonek, P. LDL-Cholesterol and Cardiovascular Events: The Lower the Better? Wien. Med. Wochenschr. 2018, 168, 108–120. [Google Scholar] [CrossRef] [PubMed]
- Oesterle, A.; Laufs, U.; Liao, J.K. Pleiotropic Effects of Statins on the Cardiovascular System. Circ. Res. 2017, 120, 229–243. [Google Scholar] [CrossRef] [PubMed]
- Kroon, A.A.; Stalenhoef, A.F.H. LDL-Cholesterol Lowering and Atherosclerosis—Clinical Benefit and Possible Mechanisms: An Update. Neth. J. Med. 1997, 51, 16–27. [Google Scholar] [CrossRef]
- Gencer, B.; Marston, N.A.; Im, K.A.; Cannon, C.P.; Sever, P.; Keech, A.; Braunwald, E.; Giugliano, R.P.; Sabatine, M.S. Efficacy and Safety of Lowering LDL Cholesterol in Older Patients: A Systematic Review and Meta-Analysis of Randomised Controlled Trials. Lancet 2020, 396, 1637–1643. [Google Scholar] [CrossRef]
- Stoekenbroek, R.M.; Lambert, G.; Cariou, B.; Hovingh, G.K. Inhibiting PCSK9—Biology beyond LDL Control. Nat. Rev. Endocrinol. 2018, 15, 52–62. [Google Scholar] [CrossRef]
- Rosenson, R.S.; Hegele, R.A.; Fazio, S.; Cannon, C.P. The Evolving Future of PCSK9 Inhibitors. J. Am. Coll. Cardiol. 2018, 72, 314–329. [Google Scholar] [CrossRef]
- Ridker, P.M.; Danielson, E.; Fonseca, F.A.; Genest, J.; Gotto, A.M.; Kastelein, J.J.; Koenig, W.; Libby, P.; Lorenzatti, A.J.; MacFadyen, J.G.; et al. Reduction in C-Reactive Protein and LDL Cholesterol and Cardiovascular Event Rates after Initiation of Rosuvastatin: A Prospective Study of the JUPITER Trial. Lancet 2009, 373, 1175–1182. [Google Scholar] [CrossRef] [PubMed]
- Ridker, P.M.; Everett, B.M.; Thuren, T.; MacFadyen, J.G.; Chang, W.H.; Ballantyne, C.; Fonseca, F.; Nicolau, J.; Koenig, W.; Anker, S.D.; et al. Antiinflammatory Therapy with Canakinumab for Atherosclerotic Disease. N. Engl. J. Med. 2017, 377, 1119–1131. [Google Scholar] [CrossRef] [PubMed]
- Ridker, P.M. Closing the Loop on Inflammation and Atherothrombosis: Why Perform the CIRT and CANTOS Trials? Trans. Am. Clin. Climatol. Assoc. 2013, 124, 174–190. [Google Scholar] [PubMed]
- Kirii, H.; Niwa, T.; Yamada, Y.; Wada, H.; Saito, K.; Iwakura, Y.; Asano, M.; Moriwaki, H.; Seishima, M. Lack of Interleukin-1beta Decreases the Severity of Atherosclerosis in ApoE-Deficient Mice. Arterioscler. Thromb. Vasc. Biol. 2003, 23, 656–660. [Google Scholar] [CrossRef]
- Merhi-Soussi, F.; Kwak, B.R.; Magne, D.; Chadjichristos, C.; Berti, M.; Pelli, G.; James, R.W.; MacH, F.; Gabay, C. Interleukin-1 Plays a Major Role in Vascular Inflammation and Atherosclerosis in Male Apolipoprotein E-Knockout Mice. Cardiovasc. Res. 2005, 66, 583–593. [Google Scholar] [CrossRef]
- Isoda, K.; Sawada, S.; Ishigami, N.; Matsuki, T.; Miyazaki, K.; Kusuhara, M.; Iwakura, Y.; Ohsuzu, F. Lack of Interleukin-1 Receptor Antagonist Modulates Plaque Composition in Apolipoprotein E-Deficient Mice. Arterioscler. Thromb. Vasc. Biol. 2004, 24, 1068–1073. [Google Scholar] [CrossRef]
- Kimura, T.; Tse, K.; Sette, A.; Ley, K. Vaccination to Modulate Atherosclerosis. Autoimmunity 2015, 48, 152–160. [Google Scholar] [CrossRef]
- Kimura, T.; Kobiyama, K.; Winkels, H.; Tse, K.; Miller, J.; Vassallo, M.; Wolf, D.; Ryden, C.; Orecchioni, M.; Dileepan, T.; et al. Regulatory CD4+ T Cells Recognize Major Histocompatibility Complex Class II Molecule–Restricted Peptide Epitopes of Apolipoprotein B. Circulation 2018, 138, 1130–1143. [Google Scholar] [CrossRef]
- Davignon, J.; Ganz, P. Role of Endothelial Dysfunction in Atherosclerosis. Circulation 2004, 109, III-27–III-32. [Google Scholar] [CrossRef]
- Sekiya, M.; Osuga, J.; Nagashima, S.; Ohshiro, T.; Igarashi, M.; Okazaki, H.; Takahashi, M.; Tazoe, F.; Wada, T.; Ohta, K.; et al. Ablation of Neutral Cholesterol Ester Hydrolase 1 Accelerates Atherosclerosis. Cell Metab. 2009, 10, 219–228. [Google Scholar] [CrossRef]
- Sukhorukov, V.N.; Khotina, V.A.; Chegodaev, Y.S.; Ivanova, E.; Sobenin, I.A.; Orekhov, A.N. Lipid Metabolism in Macrophages: Focus on Atherosclerosis. Biomedicines 2020, 8, 262. [Google Scholar] [CrossRef] [PubMed]
- Yu, X.; Fu, Y.; Zhang, D.; Yin, K.; Tang, C. Foam Cells in Atherosclerosis. Clin. Chim. Acta 2013, 424, 245–252. [Google Scholar] [CrossRef]
- Chistiakov, D.A.; Bobryshev, Y.V.; Orekhov, A.N. Macrophage-mediated Cholesterol Handling in Atherosclerosis. J. Cell. Mol. Med. 2016, 20, 17–28. [Google Scholar] [CrossRef] [PubMed]
- Cagnina, A.; Chabot, O.; Davin, L.; Lempereur, M.; Maréchal, P.; Oury, C.; Lancellotti, P. Atherosclerosis—An Inflammatory Disease. N. Engl. J. Med. 1999, 340, 302–309. [Google Scholar] [CrossRef]
- Kolodgie, F.D.; Gold, H.K.; Burke, A.P.; Fowler, D.R.; Kruth, H.S.; Weber, D.K.; Farb, A.; Guerrero, L.J.; Hayase, M.; Kutys, R.; et al. Intraplaque Hemorrhage and Progression of Coronary Atheroma. N. Engl. J. Med. 2003, 349, 2316–2325. [Google Scholar] [CrossRef]
- Ma, J.; Luo, J.; Sun, Y.; Zhao, Z. Cytokines Associated with Immune Response in Atherosclerosis. Am. J. Transl. Res. 2022, 14, 6424–6444. [Google Scholar] [PubMed]
- Tsioufis, P.; Theofilis, P.; Tsioufis, K.; Tousoulis, D. The Impact of Cytokines in Coronary Atherosclerotic Plaque: Current Therapeutic Approaches. Int. J. Mol. Sci. 2022, 23, 15937. [Google Scholar] [CrossRef]
- Creager, M.A.; Belkin, M.; Bluth, E.I.; Casey, D.E.; Chaturvedi, S.; Dake, M.D.; Fleg, J.L.; Hirsch, A.T.; Jaff, M.R.; Kern, J.A.; et al. 2012 ACCF/AHA/ACR/SCAI/SIR/STS/SVM/SVN/SVS Key Data Elements and Definitions for Peripheral Atherosclerotic Vascular Disease: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Clinical Data Standards (Writing Committee to Develop Clinical Data Standards for Peripheral Atherosclerotic Vascular Disease). Circulation 2012, 125, 395–467. [Google Scholar] [CrossRef]
- Lundberg, A.M.; Hansson, G.K. Innate Immune Signals in Atherosclerosis. Clin. Immunol. 2010, 134, 5–24. [Google Scholar] [CrossRef]
- Marchini, T.; Mitre, L.S.; Wolf, D. Inflammatory Cell Recruitment in Cardiovascular Disease. Front. Cell Dev. Biol. 2021, 9, 207. [Google Scholar] [CrossRef]
- Kobiyama, K.; Ley, K. Atherosclerosis. Circ. Res. 2018, 123, 1118–1120. [Google Scholar] [CrossRef] [PubMed]
- Ait-Oufella, H.; Salomon, B.L.; Potteaux, S.; Robertson, A.K.L.; Gourdy, P.; Zoll, J.; Merval, R.; Esposito, B.; Cohen, J.L.; Fisson, S.; et al. Natural Regulatory T Cells Control the Development of Atherosclerosis in Mice. Nat. Med. 2006, 12, 178–180. [Google Scholar] [CrossRef] [PubMed]
- Saleheen, D.; Haycock, P.C.; Zhao, W.; Rasheed, A.; Taleb, A.; Imran, A.; Abbas, S.; Majeed, F.; Akhtar, S.; Qamar, N.; et al. Apolipoprotein(a) Isoform Size, Lipoprotein(a) Concentration, and Coronary Artery Disease: A Mendelian Randomisation Analysis. Lancet Diabetes Endocrinol. 2017, 5, 524–533. [Google Scholar] [CrossRef]
- Sarwar, N.; Butterworth, A.S.; Freitag, D.F.; Gregson, J.; Willeit, P.; Gorman, D.N.; Gao, P.; Saleheen, D.; Rendon, A.; Nelson, C.P.; et al. Interleukin-6 Receptor Pathways in Coronary Heart Disease: A Collaborative Meta-Analysis of 82 Studies. Lancet 2012, 379, 1205–1213. [Google Scholar] [CrossRef]
- Swerdlow, D.I.; Holmes, M.V.; Kuchenbaecker, K.B.; Engmann, J.E.L.; Shah, T.; Sofat, R.; Guo, Y.; Chung, C.; Peasey, A.; Pfister, R.; et al. The Interleukin-6 Receptor as a Target for Prevention of Coronary Heart Disease: A Mendelian Randomisation Analysis. Lancet 2012, 379, 1214–1224. [Google Scholar] [CrossRef] [PubMed]
- Cai, T.; Zhang, Y.; Ho, Y.L.; Link, N.; Sun, J.; Huang, J.; Cai, T.A.; Damrauer, S.; Ahuja, Y.; Honerlaw, J.; et al. Association of Interleukin 6 Receptor Variant with Cardiovascular Disease Effects of Interleukin 6 Receptor Blocking Therapy: A Phenome-Wide Association Study. JAMA Cardiol. 2018, 3, 849–857. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.; Kishimoto, T. Interplay between Interleukin-6 Signaling and the Vascular Endothelium in Cytokine Storms. Exp. Mol. Med. 2021, 53, 1116–1123. [Google Scholar] [CrossRef]
- Shuvalova, Y.A.; Kaminnaya, V.; Kaminnyi, A.I. Contribution of Interleukin-6 System Genes Polymorphisms to the Development of Coronary Atherosclerosis. Gene 2023, 861, 147253. [Google Scholar] [CrossRef]
- Ortega-Rivera, O.A.; Shin, M.D.; Moreno-Gonzalez, M.A.; Pokorski, J.K.; Steinmetz, N.F. A Single-Dose Qβ VLP Vaccine against S100A9 Protein Reduces Atherosclerosis in a Preclinical Model. Adv. Ther. 2022, 5, 2200092. [Google Scholar] [CrossRef]
- Ahamad, S.; Bhat, S.A. Recent Update on the Development of PCSK9 Inhibitors for Hypercholesterolemia Treatment. J. Med. Chem. 2022, 65, 15513–15539. [Google Scholar] [CrossRef]
- Ramonfaur, D.; Hinojosa-González, D.E.; Paredes-Vázquez, J.G. Killip-Kimball Classification in Octogenarians with Acute Coronary Syndrome: An 11-Year Experience. Arch. Cardiol. Mex. 2022, 92, 425–430. [Google Scholar] [CrossRef] [PubMed]
- Killip, T.; Kimball, J.T. Treatment of Myocardial Infarction in a Coronary Care Unit. A Two Year Experience with 250 Patients. Am. J. Cardiol. 1967, 20, 457–464. [Google Scholar] [CrossRef] [PubMed]
- Zeymer, U.; Bueno, H.; Granger, C.B.; Hochman, J.; Huber, K.; Lettino, M.; Price, S.; Schiele, F.; Tubaro, M.; Vranckx, P.; et al. Acute Cardiovascular Care Association Position Statement for the Diagnosis and Treatment of Patients with Acute Myocardial Infarction Complicated by Cardiogenic Shock: A Document of the Acute Cardiovascular Care Association of the European Society of Cardiology. Eur. Heart J. 2020, 9, 183–197. [Google Scholar] [CrossRef]
- Bergmark, B.A.; Mathenge, N.; Merlini, P.A.; Lawrence-Wright, M.B.; Giugliano, R.P. Acute Coronary Syndromes. Lancet 2022, 399, 1347–1358. [Google Scholar] [CrossRef]
- Collet, J.-P.; Thiele, H.; Barbato, E.; Barthélémy, O.; Bauersachs, J.; Bhatt, D.L.; Dendale, P.; Dorobantu, M.; Edvardsen, T.; Folliguet, T.; et al. 2020 ESC Guidelines for the Management of Acute Coronary Syndromes in Patients Presenting without Persistent ST-Segment ElevationThe Task Force for the Management of Acute Coronary Syndromes in Patients Presenting without Persistent ST-Segment Elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2021, 42, 1289–1367. [Google Scholar] [CrossRef]
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Chaitman, B.R.; Bax, J.J.; Morrow, D.A.; White, H.D. Fourth Universal Definition of Myocardial Infarction (2018). Circulation 2018, 138, e618–e651. [Google Scholar] [CrossRef]
- Neumann, J.; Twerenbold, R.; Ojeda, F.; Sörensen, N.A.; Chapman, A.R.; Shah, A.S.V.; Anand, A.; Boeddinghaus, J.; Nestelberger, T.; Badertscher, P.; et al. Application of High-Sensitivity Troponin in Suspected Myocardial Infarction. N. Engl. J. Med. 2019, 380, 2529–2540. [Google Scholar] [CrossRef]
- Lawton, J.S.; Tamis-Holland, J.E.; Bangalore, S.; Bates, E.R.; Beckie, T.M.; Bischoff, J.M.; Bittl, J.A.; Cohen, M.G.; Dimaio, J.M.; Don, C.W.; et al. 2021 ACC/AHA/SCAI Guideline for Coronary Artery Revascularization: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2022, 145, E18–E114. [Google Scholar] [CrossRef]
- Saraste, A.; Knuuti, J. ESC 2019 Guidelines for the Diagnosis and Management of Chronic Coronary Syndromes: Recommendations for Cardiovascular Imaging. Herz 2020, 45, 409–420. [Google Scholar] [CrossRef]
- Matetzky, S.; Natanzon, S.S.; Shlomo, N.; Atar, S.; Pollak, A.; Yosefy, C.; Zahger, D.; Fefer, P.; Iakobishvili, Z.; Mazin, I.; et al. Peripheral Arterial Disease in Patients With Acute Coronary Syndrome: Results From a Large Real-World Registry. Heart Lung Circ. 2022, 31, 1093–1101. [Google Scholar] [CrossRef]
- Bonacchi, M.; Parise, O.; Matteucci, F.; Tetta, C.; Moula, A.I.; Micali, L.R.; Dokollari, A.; Martino, M.D.; Sani, G.; Grasso, A.; et al. Is Peripheral Artery Disease an Independent Predictor of Isolated Coronary Artery Bypass Outcome? Heart Lung Circ. 2020, 29, 1502–1510. [Google Scholar] [CrossRef] [PubMed]
- Attar, R.; Wu, A.; Wojdyla, D.; Jensen, S.E.; Andell, P.; Mahaffey, K.W.; Roe, M.T.; James, S.K.; Wallentin, L.; Vemulapalli, S.; et al. Outcomes After Acute Coronary Syndrome in Patients With Diabetes Mellitus and Peripheral Artery Disease (from the TRACER, TRILOGY-ACS, APPRAISE-2, and PLATO Clinical Trials). Am. J. Cardiol. 2022, 178, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Misra, S.; Shishehbor, M.H.; Takahashi, E.A.; Aronow, H.D.; Brewster, L.P.; Bunte, M.C.; Kim, E.S.H.; Lindner, J.R.; Rich, K. Perfusion Assessment in Critical Limb Ischemia: Principles for Understanding and the Development of Evidence and Evaluation of Devices: A Scientific Statement from the American Heart Association. Circulation 2019, 140, E657–E672. [Google Scholar] [CrossRef] [PubMed]
- Cassar, K. Intermittent Claudication. BMJ 2006, 333, 1002–1005. [Google Scholar] [CrossRef] [PubMed]
- Hardman, R.L.; Jazaeri, O.; Yi, J.; Smith, M.; Gupta, R. Overview of Classification Systems in Peripheral Artery Disease. Semin. Interv. Radiol. 2014, 31, 378–388. [Google Scholar] [CrossRef] [PubMed]
- Kieback, A.G.; Gähwiler, R.; Thalhammer, C. PAD Screening: Why? Whom? When? How?—A Systematic Review. Vasa 2021, 50, 85–91. [Google Scholar] [CrossRef]
- Marco, M.; Valentina, I.; Daniele, M.; Valerio, D.R.; Andrea, P.; Roberto, G.; Laura, G.; Luigi, U. Peripheral Arterial Disease in Persons with Diabetic Foot Ulceration: A Current Comprehensive Overview. Curr. Diabetes Rev. 2021, 17, 474–485. [Google Scholar] [CrossRef]
- Park, S.C.; Choi, C.Y.; Ha, Y.I.; Yang, H.E. Utility of Toe-Brachial Index for Diagnosis of Peripheral Artery Disease. Arch. Plast. Surg. 2012, 39, 227–231. [Google Scholar] [CrossRef]
- Mills, J.L.; Conte, M.S.; Armstrong, D.G.; Pomposelli, F.B.; Schanzer, A.; Sidawy, A.N.; Andros, G. The Society for Vascular Surgery Lower Extremity Threatened Limb Classification System: Risk Stratification Based on Wound, Ischemia, and Foot Infection (WIfI). J. Vasc. Surg. 2014, 59, 220–234. [Google Scholar] [CrossRef]
- Conte, M.S.; Bradbury, A.W.; Kolh, P.; White, J.V.; Dick, F.; Fitridge, R.; Mills, J.L.; Ricco, J.B.; Suresh, K.R.; Murad, M.H.; et al. Global Vascular Guidelines on the Management of Chronic Limb-Threatening Ischemia. J. Vasc. Surg. 2019, 69, 3S–125S.e40. [Google Scholar] [CrossRef]
- Obara, H.; Matsubara, K.; Kitagawa, Y. Acute Limb Ischemia. Ann. Vasc. Dis. 2018, 11, 443–448. [Google Scholar] [CrossRef] [PubMed]
- Yusrizal, T.; Dewi, I.P.; Wardhani, L.F.K.; Lefi, A. Massive Thrombosis in Elderly with Acute Limb Ischemia: Lessons Learned from Difficult Case. Vis. J. Emerg. Med. 2021, 25, 101173. [Google Scholar] [CrossRef]
- Roush, W.P.; Peters, A.; Vogel, T.R.; Balasundaram, N.; Bath, J. Balloon-Assisted Endovascular Thrombectomy for Tibial Thromboembolism. Ann. Vasc. Surg. 2022, 79, 440.e1–440.e5. [Google Scholar] [CrossRef]
- King, E.G.; Farber, A. What Is the Best Treatment for Acute Limb Ischemia? Adv. Surg. 2022, 56, 287–304. [Google Scholar] [CrossRef] [PubMed]
- McNally, M.M.; Univers, J. Acute Limb Ischemia. Surg. Clin. N. Am. 2018, 98, 1081–1096. [Google Scholar] [CrossRef] [PubMed]
- Buls, N.; de Brucker, Y.; Aerden, D.; Devos, H.; Van Gompel, G.; Boonen, P.T.; Nieboer, K.; Leiner, T.; de Mey, J. Improving the Diagnosis of Peripheral Arterial Disease in Below-the-Knee Arteries by Adding Time-Resolved CT Scan Series to Conventional Run-off CT Angiography. First Experience with a 256-Slice CT Scanner. Eur. J. Radiol. 2019, 110, 136–141. [Google Scholar] [CrossRef]
- AbuRahma, A.F.; Campbell, J.E. Overview of Peripheral Arterial Disease of the Lower Extremity. In Noninvasive Vascular Diagnosis: A Practical Textbook for Clinicians; AbuRahma, A.F., Perler, B.A., Eds.; Springer International Publishing: Cham, Switzerland, 2022; pp. 449–488. ISBN 978-3-030-60626-8. [Google Scholar]
- Metaxas, V.I.; Dimitroukas, C.P.; Efthymiou, F.O.; Zampakis, P.E.; Panayiotakis, G.S.; Kalogeropoulou, C.P. Patient Dose in CT Angiography Examinations: An Institutional Survey. Radiat. Phys. Chem. 2022, 195, 110083. [Google Scholar] [CrossRef]
- Gerhard-Herman, M.D.; Gornik, H.L.; Barrett, C.; Barshes, N.R.; Corriere, M.A.; Drachman, D.E.; Fleisher, L.A.; Fowkes, F.G.R.; Hamburg, N.M.; Kinlay, S.; et al. 2016 AHA/ACC Guideline on the Management of Patients with Lower Extremity Peripheral Artery Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2017, 135, e726–e779. [Google Scholar] [CrossRef]
- Buckler, A.J.; Gotto, A.M.; Rajeev, A.; Nicolaou, A.; Sakamoto, A.; Pierre, S.S.; Phillips, M.; Virmani, R.; Villines, T.C. Atherosclerosis Risk Classification with Computed Tomography Angiography: A Radiologic-Pathologic Validation Study. Atherosclerosis 2023, 366, 42–48. [Google Scholar] [CrossRef]
- van Zandvoort, L.J.C.; Otsuka, K.; Villiger, M.; Neleman, T.; Dijkstra, J.; Zijlstra, F.; van Mieghem, N.M.; Bouma, B.E.; Daemen, J. Polarimetric Signatures of Coronary Thrombus in Patients with Acute Coronary Syndrome. Circ. J. 2021, 85, 1806–1813. [Google Scholar] [CrossRef]
- Falk, E.; Shah, P.K.; Fuster, V. Coronary Plaque Disruption. Circulation 1995, 92, 657–671. [Google Scholar] [CrossRef] [PubMed]
- Medaković, P.; Jukić, M.; Biloglav, Z. Vulnerable Plaque Characteristics at Coronary Computed Tomography Angiography. Cardiol. Croat. 2023, 18, 7–21. [Google Scholar] [CrossRef]
- Jebari-Benslaiman, S.; Galicia-García, U.; Larrea-Sebal, A.; Olaetxea, J.R.; Alloza, I.; Vandenbroeck, K.; Benito-Vicente, A.; Martín, C. Pathophysiology of Atherosclerosis. Int. J. Mol. Sci. 2022, 23, 3346. [Google Scholar] [CrossRef] [PubMed]
- Creager, M.A.; Kaufman, J.A.; Conte, M.S. Clinical Practice. Acute Limb Ischemia. N. Engl. J. Med. 2012, 366, 2198–2206. [Google Scholar] [CrossRef] [PubMed]
- Howard, D.P.J.; Banerjee, A.; Fairhead, J.F.; Hands, L.; Silver, L.E.; Rothwell, P.M. Population-Based Study of Incidence, Risk Factors, Outcome, and Prognosis of Ischemic Peripheral Arterial Events: Implications for Prevention. Circulation 2015, 132, 1805–1815. [Google Scholar] [CrossRef]
- Narula, N.; Olin, J.W.; Narula, N. Pathologic Disparities between Peripheral Artery Disease and Coronary Artery Disease. Arterioscler. Thromb. Vasc. Biol. 2020, 40, 1982–1989. [Google Scholar] [CrossRef]
- Kuyama, N.; Kaikita, K.; Ishii, M.; Mitsuse, T.; Nakanishi, N.; Fujisue, K.; Otsuka, Y.; Hanatani, S.; Sueta, D.; Takashio, S.; et al. Increased Thrombogenicity Is Associated with Revascularization Outcomes in Patients with Chronic Limb-Threatening Ischemia. J. Vasc. Surg. 2022, 76, 513–522.e3. [Google Scholar] [CrossRef]
- Torii, S.; Mustapha, J.A.; Narula, J.; Mori, H.; Saab, F.; Jinnouchi, H.; Yahagi, K.; Sakamoto, A.; Romero, M.E.; Narula, N.; et al. Histopathologic Characterization of Peripheral Arteries in Subjects With Abundant Risk Factors: Correlating Imaging With Pathology. JACC Cardiovasc. Imaging 2019, 12, 1501–1513. [Google Scholar] [CrossRef]
- Soor, G.S.; Vukin, I.; Leong, S.W.; Oreopoulos, G.; Butany, J. Peripheral Vascular Disease: Who Gets It and Why? A Histomorphological Analysis of 261 Arterial Segments from 58 Cases. Pathology 2008, 40, 385–391. [Google Scholar] [CrossRef]
- Narula, J.; Ibáñez, B.; Fuster, V. From Heart to Head, Thrombi to Emboli, and Inferences to Extrapolation. J. Am. Coll. Cardiol. 2019, 73, 1000–1003. [Google Scholar] [CrossRef]
- Ho, C.Y.; Shanahan, C.M. Medial Arterial Calcification: An Overlooked Player in Peripheral Arterial Disease. Arterioscler. Thromb. Vasc. Biol. 2016, 36, 1475–1482. [Google Scholar] [CrossRef] [PubMed]
- Zhuo, M.F.; Zhang, K.L.; Shen, X.B.; Lin, W.C.; Hu, B.; Cai, H.P.; Huang, G. Retrospective Study Postoperative Adverse Cardiac Events in Acute Myocardial Infarction with High Thrombus Load and Best Time for Stent Implantation. World J. Clin. Cases 2022, 10, 2106–2114. [Google Scholar] [CrossRef]
- Yoshida, K.; Yang, T.; Yamamoto, Y.; Kurosaki, Y.; Funaki, T.; Kikuchi, T.; Ishii, A.; Kataoka, H.; Miyamoto, S. Expansive Carotid Artery Remodeling: Possible Marker of Vulnerable Plaque. J. Neurosurg. 2019, 133, 1435–1440. [Google Scholar] [CrossRef] [PubMed]
- Okada, K.; Hibi, K. Intravascular Ultrasound in Vulnerable Plaque and Acute Coronary Syndrome. Interv. Cardiol. Clin. 2023, 12, 155–165. [Google Scholar] [CrossRef] [PubMed]
- Schantl, A.E.; Ivarsson, M.E.; Leroux, J.C. Investigational Pharmacological Treatments for Vascular Calcification. Adv. Ther. 2019, 2, 1800094. [Google Scholar] [CrossRef]
- Anand, S.S.; Caron, F.; Eikelboom, J.W.; Bosch, J.; Dyal, L.; Aboyans, V.; Abola, M.T.; Branch, K.R.H.; Keltai, K.; Bhatt, D.L.; et al. Major Adverse Limb Events and Mortality in Patients With Peripheral Artery Disease: The COMPASS Trial. J. Am. Coll. Cardiol. 2018, 71, 2306–2315. [Google Scholar] [CrossRef]
- Nakamura, S.; Ishibashi-Ueda, H.; Niizuma, S.; Yoshihara, F.; Horio, T.; Kawano, Y. Coronary Calcification in Patients with Chronic Kidney Disease and Coronary Artery Disease. Clin. J. Am. Soc. Nephrol. 2009, 4, 1892–1900. [Google Scholar] [CrossRef]
- Rerkasem, A.; Nopparatkailas, R.; Nantakool, S.; Rerkasem, R.; Chansakaow, C.; Apichartpiyakul, P.; Phrommintikul, A.; Rerkasem, K. The Ability of Clinical Decision Rules to Detect Peripheral Arterial Disease: A Narrative Review. Int. J. Low. Extrem. Wounds 2022, 15347346221104590. [Google Scholar] [CrossRef]
- Sakamoto, A.; Virmani, R.; Finn, A.V.; Gupta, A. Calcified Nodule as the Cause of Acute Coronary Syndrome: Connecting Bench Observations to the Bedside. Cardiology 2018, 139, 101–104. [Google Scholar] [CrossRef]
- Eligini, S.; Gianazza, E.; Mallia, A.; Ghilardi, S.; Banfi, C. Macrophage Phenotyping in Atherosclerosis by Proteomics. Int. J. Mol. Sci. 2023, 24, 2613. [Google Scholar] [CrossRef]
- Kitada, R.; Otsuka, K.; Fukuda, D. Role of Plaque Imaging for Identification of Vulnerable Patients beyond the Stage of Myocardial Ischemia. Front. Cardiovasc. Med. 2023, 10, 1095806. [Google Scholar] [CrossRef] [PubMed]
- Fowkes, G.; Fowkes, F.G.R.; Murray, G.D.; Butcher, I.; Heald, C.L.; Lee, R.J.; Chambless, L.E.; Folsom, A.R.; Hirsch, A.T.; Dramaix, M.; et al. Ankle Brachial Index Combined With Framingham Risk Score to Predict Cardiovascular Events and Mortality: A Meta-Analysis. JAMA 2008, 300, 197–208. [Google Scholar] [CrossRef] [PubMed]
- Grenon, S.M.; Hiramoto, J.; Smolderen, K.G.; Vittinghoff, E.; Whooley, M.A.; Cohen, B.E. Association between Depression and Peripheral Artery Disease: Insights from the Heart and Soul Study. J. Am. Heart Assoc. 2012, 1, e002667. [Google Scholar] [CrossRef]
- Wickström, J.E.; Laivuori, M.; Aro, E.; Sund, R.T.; Hautero, O.; Venermo, M.; Jalkanen, J.; Hakovirta, H. Toe Pressure and Toe Brachial Index Are Predictive of Cardiovascular Mortality, Overall Mortality, and Amputation Free Survival in Patients with Peripheral Artery Disease. Eur. J. Vasc. Endovasc. Surg. 2017, 53, 696–703. [Google Scholar] [CrossRef] [PubMed]
- Bonaca, M.P.; Nault, P.; Giugliano, R.P.; Keech, A.C.; Pineda, A.L.; Kanevsky, E.; Kuder, J.; Murphy, S.A.; Jukema, J.W.; Lewis, B.S.; et al. Low-Density Lipoprotein Cholesterol Lowering with Evolocumab and Outcomes in Patients with Peripheral Artery Disease: Insights from the FOURIER Trial (Further Cardiovascular Outcomes Research with PCSK9 Inhibition in Subjects with Elevated Risk). Circulation 2018, 137, 338–350. [Google Scholar] [CrossRef]
- Sabatine, M.S.; Giugliano, R.P.; Wiviott, S.D.; Raal, F.J.; Blom, D.J.; Robinson, J.; Ballantyne, C.M.; Somaratne, R.; Legg, J.; Wasserman, S.M.; et al. Efficacy and Safety of Evolocumab in Reducing Lipids and Cardiovascular Events. N. Engl. J. Med. 2015, 372, 1500–1509. [Google Scholar] [CrossRef]
- Sacks, C.A.; Avorn, J.; Kesselheim, A.S. The Failure of Solanezumab—How the FDA Saved Taxpayers Billions. N. Engl. J. Med. 2017, 376, 1706–1708. [Google Scholar] [CrossRef]
- Cannon, C.P.; Braunwald, E.; McCabe, C.H.; Rader, D.J.; Rouleau, J.L.; Belder, R.; Joyal, S.V.; Hill, K.A.; Pfeffer, M.A.; Skene, A.M. Intensive versus Moderate Lipid Lowering with Statins after Acute Coronary Syndromes. N. Engl. J. Med. 2004, 350, 1495–1504. [Google Scholar] [CrossRef]
- Robinson, J.G.; Farnier, M.; Krempf, M.; Bergeron, J.; Luc, G.; Averna, M.; Stroes, E.S.; Langslet, G.; Raal, F.J.; El Shahawy, M.; et al. Efficacy and Safety of Alirocumab in Reducing Lipids and Cardiovascular Events. N. Engl. J. Med. 2015, 372, 1489–1499. [Google Scholar] [CrossRef]
- Cohen, J.C.; Boerwinkle, E.; Mosley, T.H., Jr.; Hobbs, H.H. Sequence Variations in PCSK9, Low LDL, and Protection against Coronary Heart Disease. N. Engl. J. Med. 2006, 354, 1264–1272. [Google Scholar] [CrossRef]
- Dullaart, R.P.F. PCSK9 Inhibition to Reduce Cardiovascular Events. N. Engl. J. Med. 2017, 376, 1790–1791. [Google Scholar] [CrossRef] [PubMed]
- Kathiresan, S. A PCSK9 Missense Variant Associated with a Reduced Risk of Early-Onset Myocardial Infarction. N. Engl. J. Med. 2008, 358, 2299–2300. [Google Scholar] [CrossRef] [PubMed]
- La Rosa, J.C.; Conti, C.R. Intensive Lipid Lowering with Atorvastatin in Patients with Stable Coronary Disease. ACC Cardiosource Rev. J. 2006, 15, 97–99. [Google Scholar] [CrossRef]
- Sabatine, M.S.; Giugliano, R.P.; Keech, A.C.; Honarpour, N.; Wiviott, S.D.; Murphy, S.A.; Kuder, J.F.; Wang, H.; Liu, T.; Wasserman, S.M.; et al. Evolocumab and Clinical Outcomes in Patients with Cardiovascular Disease. N. Engl. J. Med. 2017, 376, 1713–1722. [Google Scholar] [CrossRef] [PubMed]
- Hiatt, W.R.; Fowkes, F.G.R.; Heizer, G.; Berger, J.S.; Baumgartner, I.; Held, P.; Katona, B.G.; Mahaffey, K.W.; Norgren, L.; Jones, W.S.; et al. Ticagrelor versus Clopidogrel in Symptomatic Peripheral Artery Disease. N. Engl. J. Med. 2017, 376, 32–40. [Google Scholar] [CrossRef]
- Bundó Vidiella, M.; Pérez Pérez, C.; Montero Alia, J.J.; Cobos Solórzano, M.D.; Aubà Llambrich, J.; Cabezas Peña, C. Peripheral Artery Disease of the Lower Limbs and Morbidity/Mortality in Type 2 Diabetics. Atención Primaria 2006, 38, 139–144. [Google Scholar] [CrossRef][Green Version]
- Mueller, T.; Hinterreiter, F.; Poelz, W.; Haltmayer, M.; Dieplinger, B. Mortality Rates at 10 Years Are Higher in Diabetic than in Non-Diabetic Patients with Chronic Lower Extremity Peripheral Arterial Disease. Vasc. Med. 2016, 21, 445–452. [Google Scholar] [CrossRef]
- Schuyler Jones, W.; Patel, M.R.; Dai, D.; Vemulapalli, S.; Subherwal, S.; Stafford, J.; Peterson, E.D. High Mortality Risks after Major Lower Extremity Amputation in Medicare Patients with Peripheral Artery Disease. Am. Heart J. 2013, 165, 809–815.e1. [Google Scholar] [CrossRef]
- Voci, D.; Fedeli, U.; Valerio, L.; Schievano, E.; Righini, M.; Kucher, N.; Spirk, D.; Barco, S. Mortality Rate Related to Peripheral Arterial Disease: A Retrospective Analysis of Epidemiological Data (Years 2008–2019). Nutr. Metab. Cardiovasc. Dis. 2023, 33, 516–522. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).