

Analysis of Clinical Trials and Review of Recent Advances in Therapy Decisions for Locally Advanced Prostate Cancer


Abstract
1. Introduction
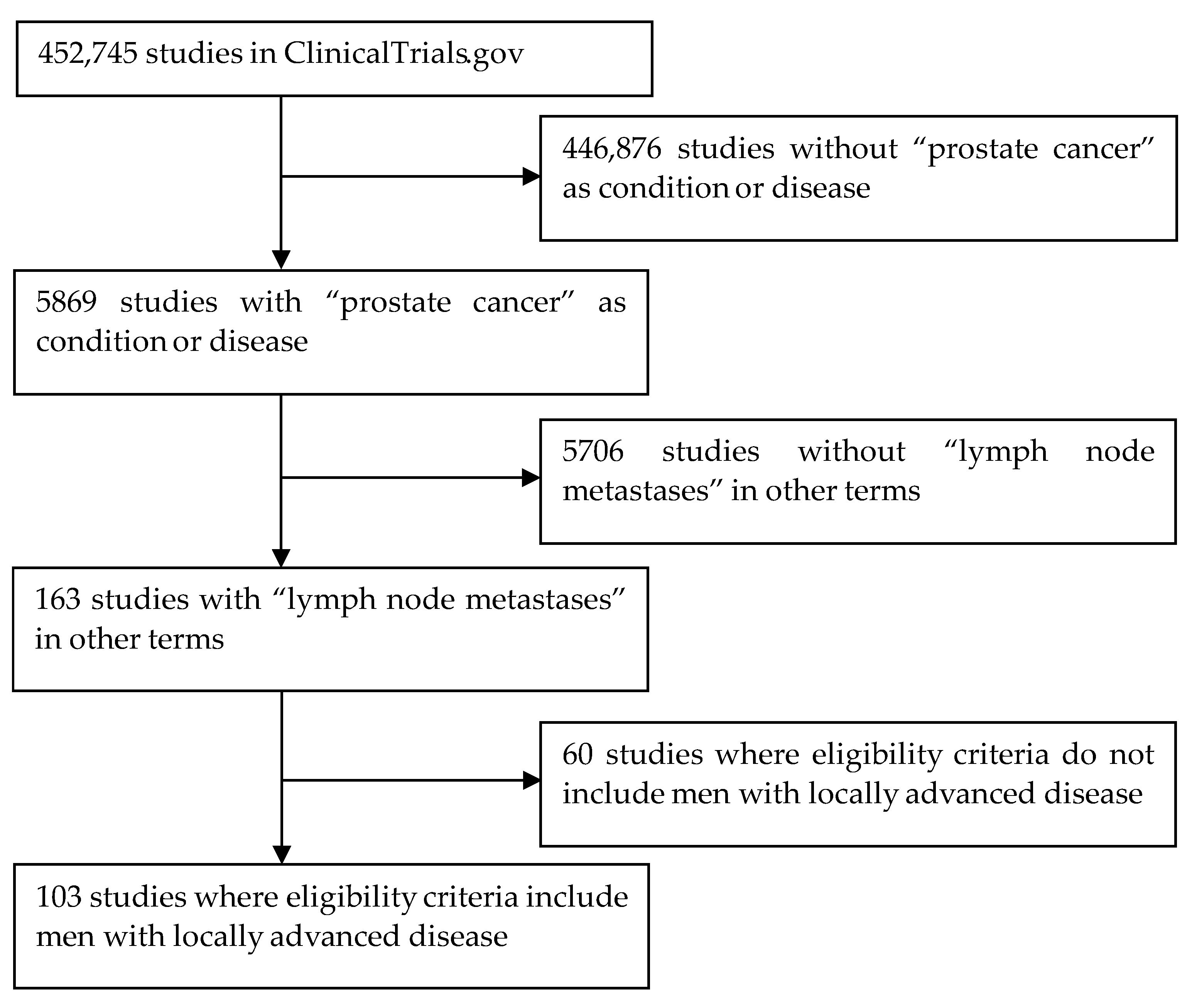
2. Materials and Methods
3. Results
3.1. Analysis of Studies Reported in ClinicalTrials.gov
3.1.1. Geographic Distribution
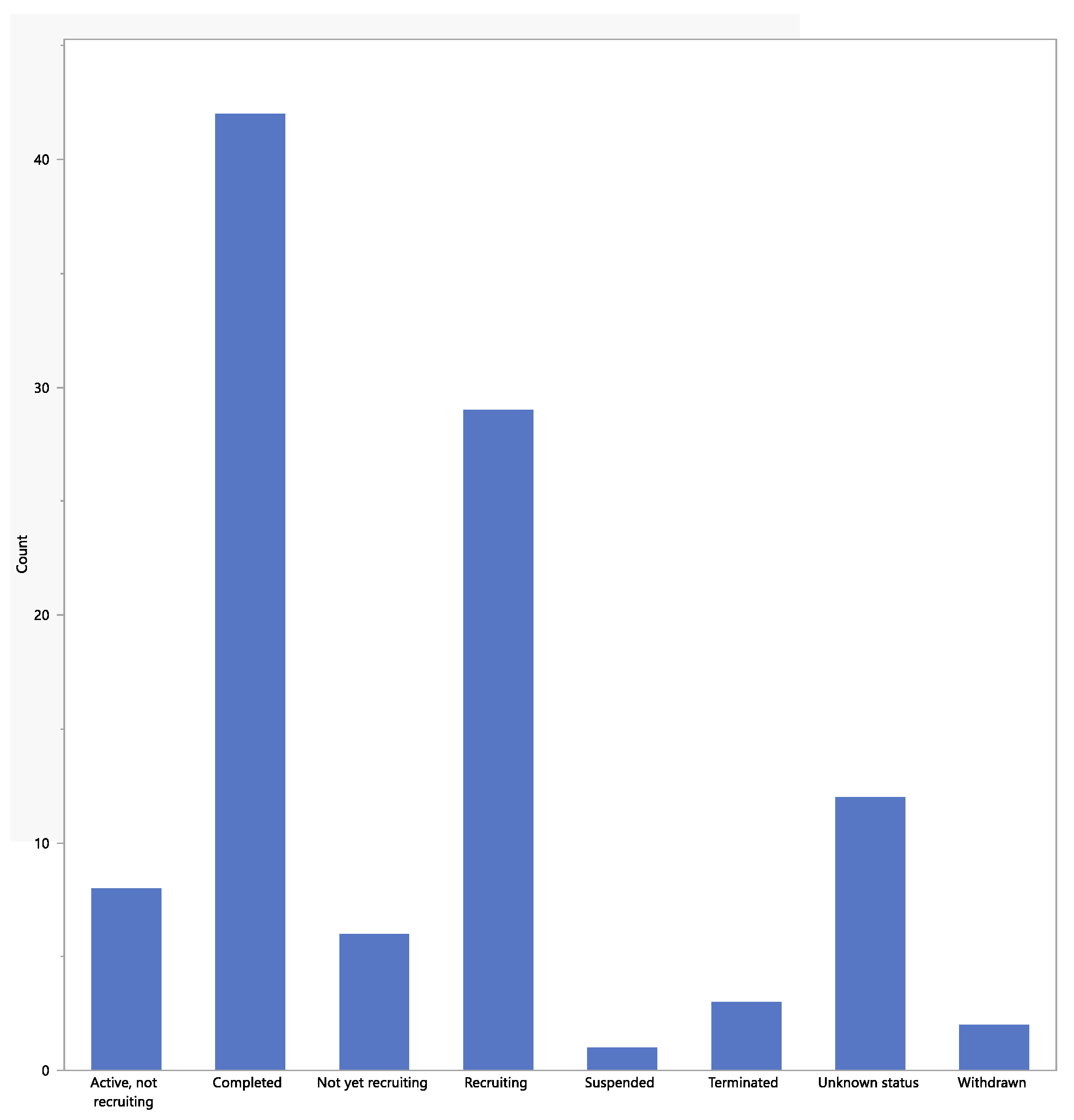
3.1.2. Status of Studies
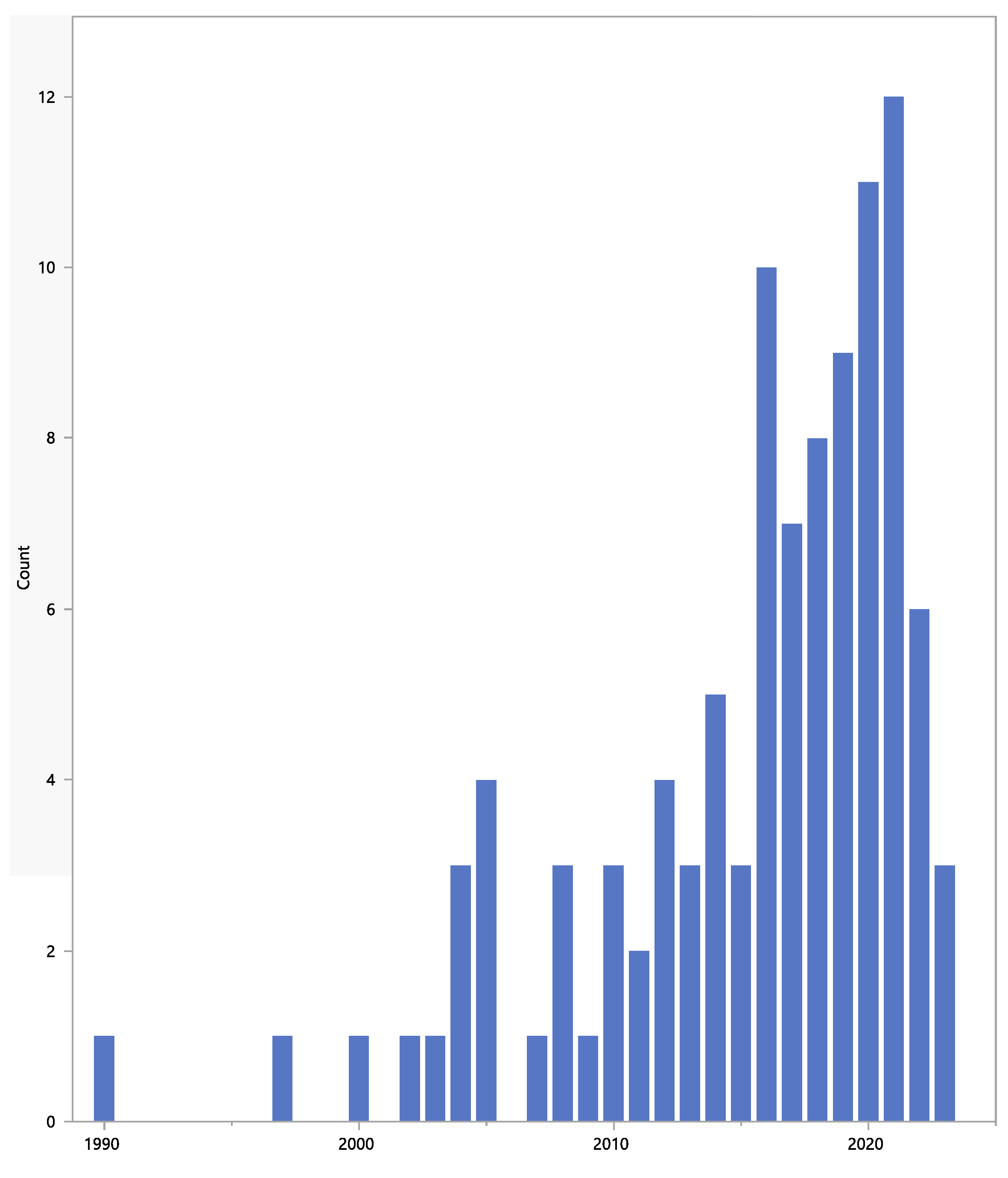
3.1.3. Start Date
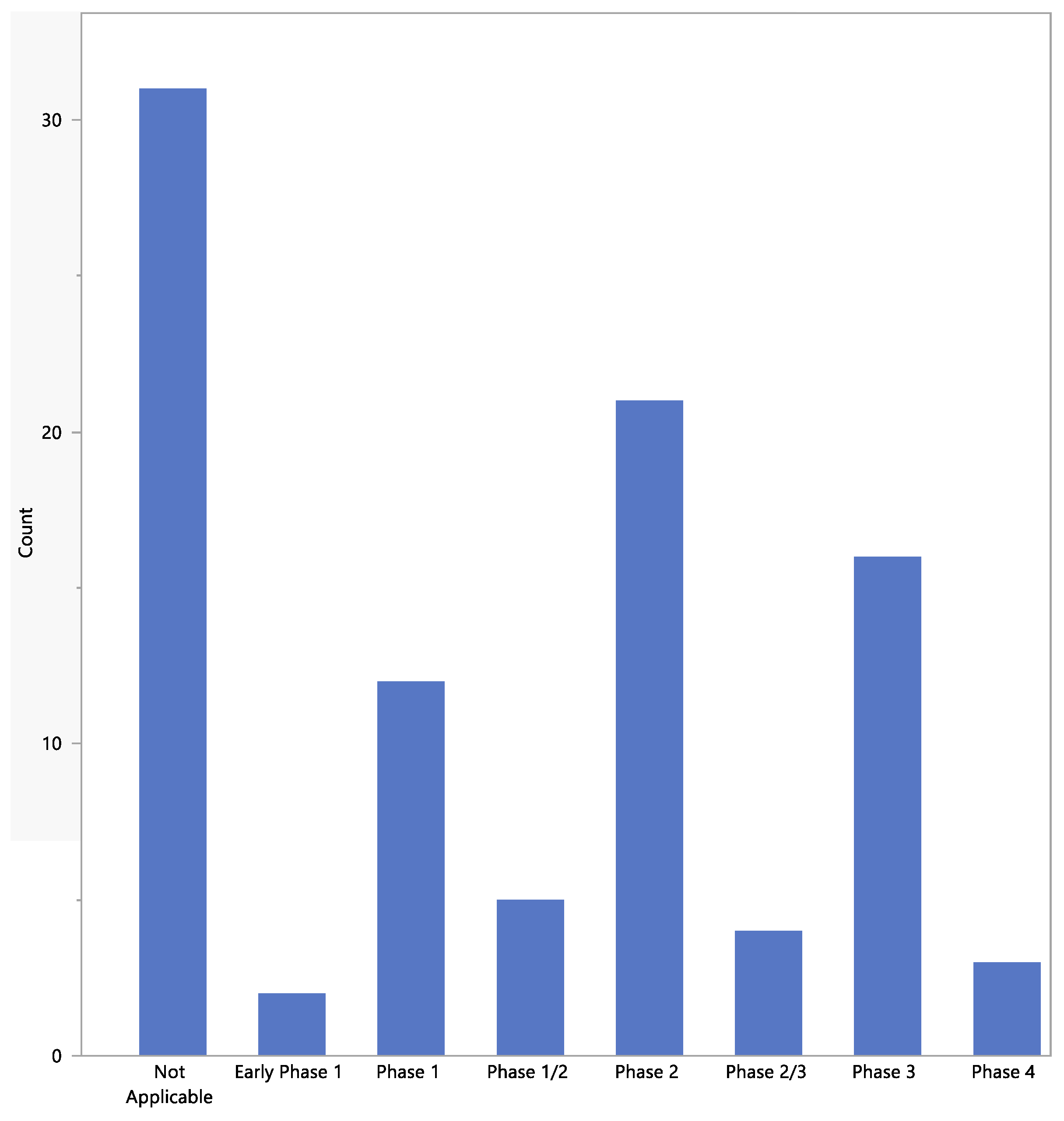
3.1.4. Phases of Studies
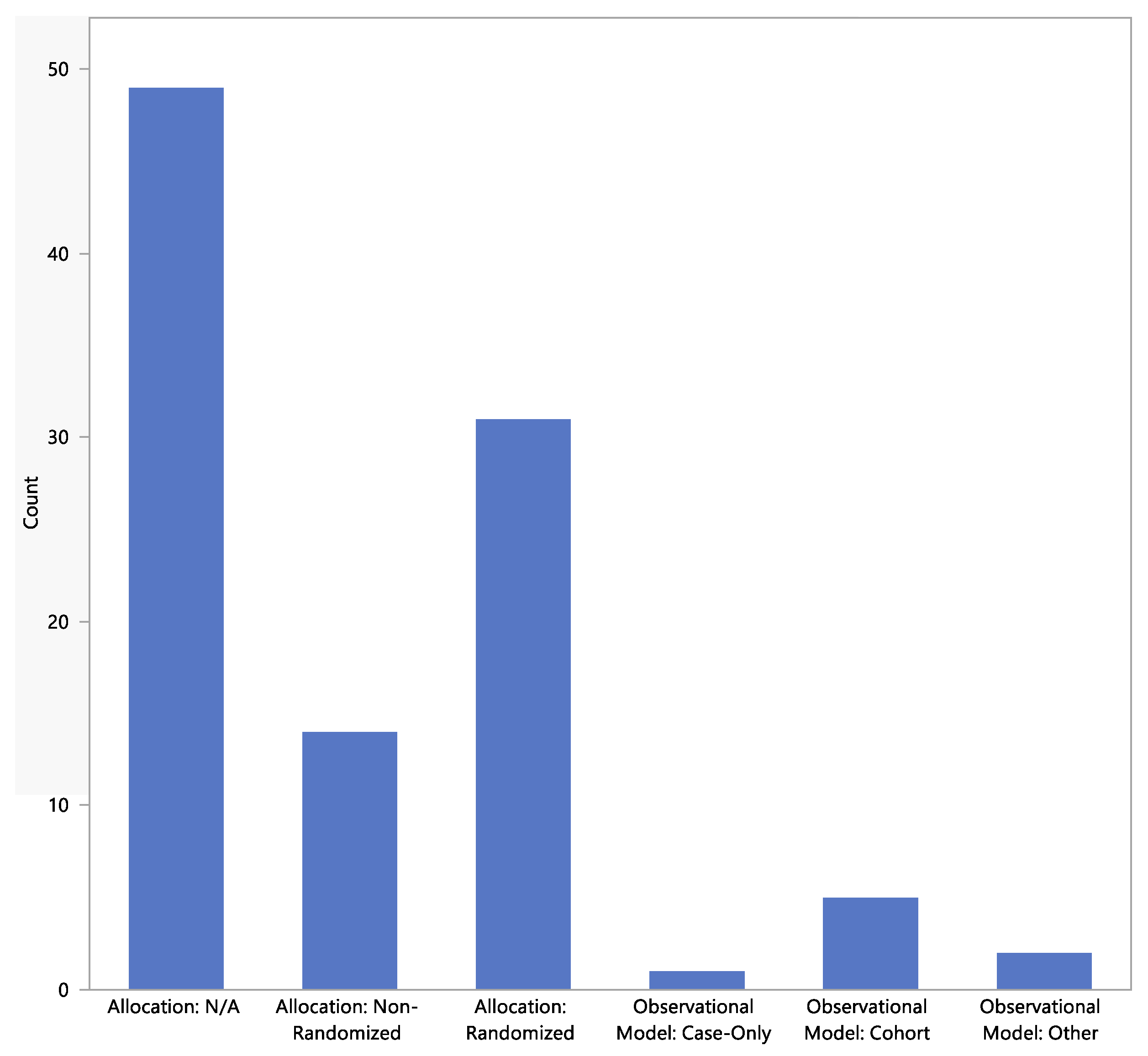
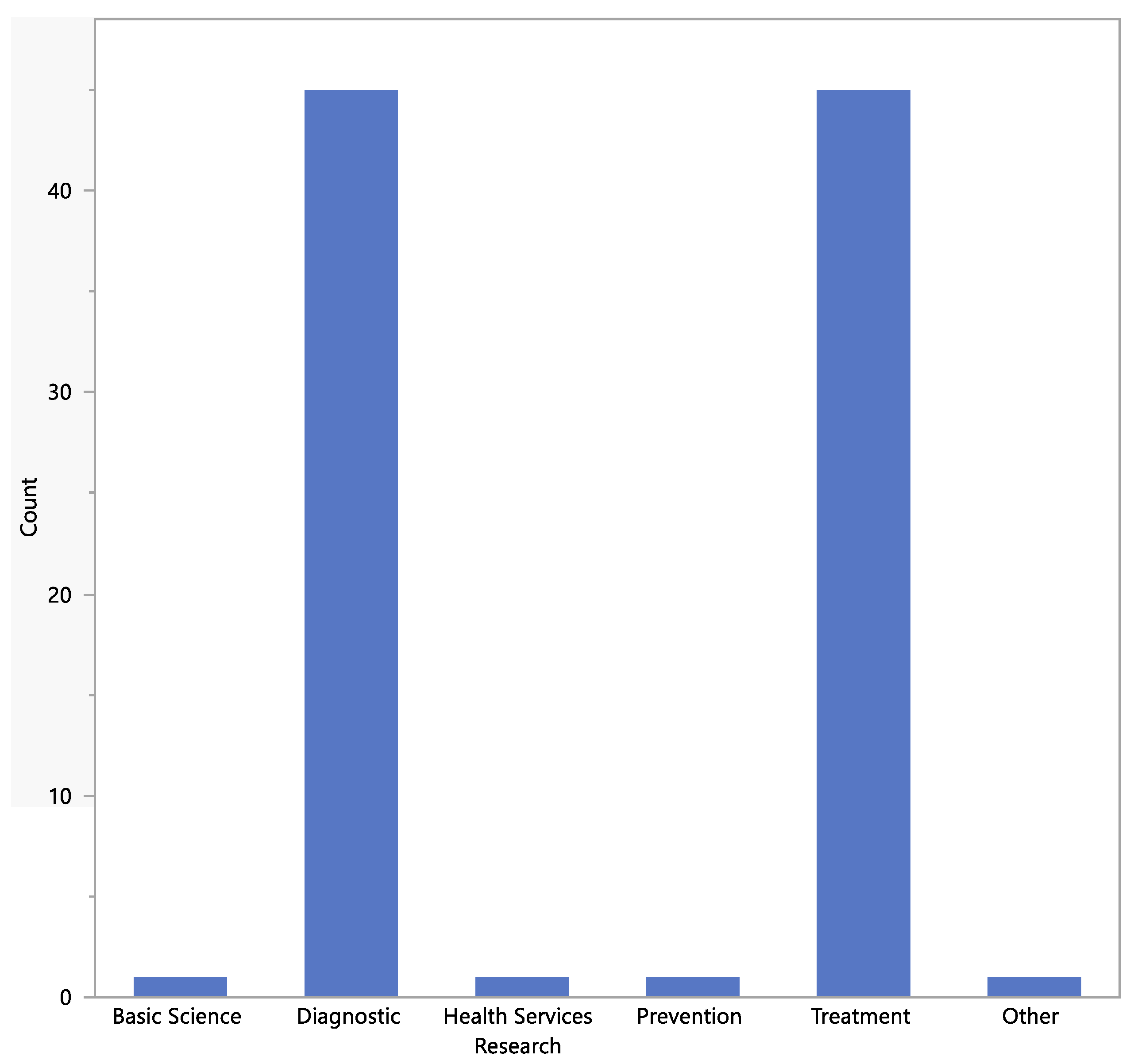
3.1.5. Study Designs
3.1.6. Types of Intervention
3.1.7. Most Recent Studies
3.2. New Treatments
3.2.1. Radiation Therapy
3.2.2. Nanoparticle-Enhanced Radiotherapy
- Nano-radiopharmaceuticals
- Gadolinium-based nanoparticles
- Hafnium oxide particles
- PSMA-targeted gold nanoparticles
3.2.3. Oncolytic Virus Therapy
3.2.4. Precision Medicine
- Prostate Health Index (PHI)
- 4Kscore Test
- MRI Fusion Biopsy
- Liquid Biopsy
- PCA3 Test
3.2.5. Androgen Receptor Targeting
3.2.6. Pharmacological-Induced Ca2+ Cytotoxicity
3.2.7. Immunotherapy
3.2.8. Active Surveillance
4. Discussion
5. Conclusions
Supplementary Materials
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rebello, R.J.; Oing, C.; Knudsen, K.E.; Loeb, S.; Johnson, D.C.; Reiter, R.E.; Gillessen, S.; Van der Kwast, T.; Bristow, R.G. Prostate Cancer. Nat. Rev. Dis. Primer 2021, 7, 9. [Google Scholar] [CrossRef] [PubMed]
- World Cancer Research Fund International. Prostate Cancer Statistics. Available online: https://www.wcrf.org/cancer-trends/prostate-cancer-statistics/ (accessed on 31 March 2023).
- Wang, L.; Lu, B.; He, M.; Wang, Y.; Wang, Z.; Du, L. Prostate Cancer Incidence and Mortality: Global Status and Temporal Trends in 89 Countries From 2000 to 2019. Front. Public Health 2022, 10, 811044. [Google Scholar] [CrossRef] [PubMed]
- Auvinen, A.; Moss, S.M.; Tammela, T.L.J.; Taari, K.; Roobol, M.J.; Schröder, F.H.; Bangma, C.H.; Carlsson, S.; Aus, G.; Zappa, M.; et al. Absolute Effect of Prostate Cancer Screening: Balance of Benefits and Harms by Center within the European Randomized Study of Prostate Cancer Screening. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2016, 22, 243–249. [Google Scholar] [CrossRef] [PubMed]
- Manna, F.L.; Karkampouna, S.; Zoni, E.; De Menna, M.; Hensel, J.; Thalmann, G.N.; Kruithof-de Julio, M. Metastases in Prostate Cancer. Cold Spring Harb. Perspect. Med. 2019, 9, a033688. [Google Scholar] [CrossRef]
- Prostate Cancer—Advanced: Symptoms, Diagnosis & Treatment—Urology Care Foundation. Available online: https://www.urologyhealth.org/urology-a-z/a_/advanced-prostate-cancer (accessed on 10 April 2023).
- Daneshmand, S.; Quek, M.L.; Stein, J.P.; Lieskovsky, G.; Cai, J.; Pinski, J.; Skinner, E.C.; Skinner, D.G. Prognosis of Patients with Lymph Node Positive Prostate Cancer Following Radical Prostatectomy: Long-Term Results. J. Urol. 2004, 172, 2252–2255. [Google Scholar] [CrossRef]
- Datta, K.; Muders, M.; Zhang, H.; Tindall, D.J. Mechanism of Lymph Node Metastasis in Prostate Cancer. Future Oncol. 2010, 6, 823–836. [Google Scholar] [CrossRef] [PubMed]
- Media/Press Resources—ClinicalTrials.Gov. Available online: https://clinicaltrials.gov/ct2/about-site/for-media (accessed on 9 May 2023).
- Espenel, S.; Chargari, C.; Blanchard, P.; Bockel, S.; Morel, D.; Rivera, S.; Levy, A.; Deutsch, E. Practice Changing Data and Emerging Concepts from Recent Radiation Therapy Randomised Clinical Trials. Eur. J. Cancer 2022, 171, 242–258. [Google Scholar] [CrossRef]
- Institute of Cancer Research, United Kingdom. PACE-NODES: A Phase III Randomised Trial of 5 Fraction Prostate SBRT Versus 5 Fraction Prostate and Pelvic Nodal SBRT. Available online: https://clinicaltrials.gov/ct2/show/NCT05613023 (accessed on 31 March 2023).
- Tampere University Hospital. TArgeted STEreotactic Radiotherapy for Oligorecurrent PROstate Cancer (TASTEPRO)—A Randomized Controlled Pilot Trial. Available online: https://clinicaltrials.gov/ct2/show/NCT05067660 (accessed on 31 March 2023).
- Ricketts, K.; Ahmad, R.; Beaton, L.; Cousins, B.; Critchley, K.; Davies, M.; Evans, S.; Fenuyi, I.; Gavriilidis, A.; Harmer, Q.J.; et al. Recommendations for Clinical Translation of Nanoparticle-Enhanced Radiotherapy. Br. J. Radiol. 2018, 91, 20180325. [Google Scholar] [CrossRef]
- Ramnaraign, B.; Sartor, O. PSMA-Targeted Radiopharmaceuticals in Prostate Cancer: Current Data and New Trials. Oncologist 2023, 28, oyac279. [Google Scholar] [CrossRef]
- Hofman, M.S.; Violet, J.; Hicks, R.J.; Ferdinandus, J.; Thang, S.P.; Akhurst, T.; Iravani, A.; Kong, G.; Ravi Kumar, A.; Murphy, D.G.; et al. [177Lu]-PSMA-617 Radionuclide Treatment in Patients with Metastatic Castration-Resistant Prostate Cancer (LuPSMA Trial): A Single-Centre, Single-Arm, Phase 2 Study. Lancet Oncol. 2018, 19, 825–833. [Google Scholar] [CrossRef]
- Sartor, O.; de Bono, J.; Chi, K.N.; Fizazi, K.; Herrmann, K.; Rahbar, K.; Tagawa, S.T.; Nordquist, L.T.; Vaishampayan, N.; El-Haddad, G.; et al. Lutetium-177-PSMA-617 for Metastatic Castration-Resistant Prostate Cancer. N. Engl. J. Med. 2021, 385, 1091–1103. [Google Scholar] [CrossRef] [PubMed]
- Goel, M.; Mackeyev, Y.; Krishnan, S. Radiolabeled Nanomaterial for Cancer Diagnostics and Therapeutics: Principles and Concepts. Cancer Nanotechnol. 2023, 14, 15. [Google Scholar] [CrossRef]
- Nanomedicine Technology for Precision Radiotherapy—NHT. Available online: https://nhtheraguix.com/ (accessed on 11 April 2023).
- Verry, C.; Dufort, S.; Lemasson, B.; Grand, S.; Pietras, J.; Troprès, I.; Crémillieux, Y.; Lux, F.; Mériaux, S.; Larrat, B.; et al. Targeting Brain Metastases with Ultrasmall Theranostic Nanoparticles, a First-in-Human Trial from an MRI Perspective. Sci. Adv. 2020, 6, eaay5279. [Google Scholar] [CrossRef] [PubMed]
- Verry, C.; Dufort, S.; Villa, J.; Gavard, M.; Iriart, C.; Grand, S.; Charles, J.; Chovelon, B.; Cracowski, J.-L.; Quesada, J.-L.; et al. Theranostic AGuIX Nanoparticles as Radiosensitizer: A Phase I, Dose-Escalation Study in Patients with Multiple Brain Metastases (NANO-RAD Trial). Radiother. Oncol. J. Eur. Soc. Ther. Radiol. Oncol. 2021, 160, 159–165. [Google Scholar] [CrossRef] [PubMed]
- NH TherAguix. Clinical Trial Cancer Drugs, AGuIX® Evaluation. Available online: https://nhtheraguix.com/pipeline/ (accessed on 31 March 2023).
- Sancey, L.; Lux, F.; Kotb, S.; Roux, S.; Dufort, S.; Bianchi, A.; Crémillieux, Y.; Fries, P.; Coll, J.-L.; Rodriguez-Lafrasse, C.; et al. The Use of Theranostic Gadolinium-Based Nanoprobes to Improve Radiotherapy Efficacy. Br. J. Radiol. 2014, 87, 20140134. [Google Scholar] [CrossRef]
- Nanobiotix. A Global Biotechnology Company. Available online: https://www.nanobiotix.com/ (accessed on 11 April 2023).
- Patient Clinical + Trials. Available online: https://www.nanobiotix.com/patient-clinical-studies/ (accessed on 11 April 2023).
- Zhang, P.; Marill, J.; Darmon, A.; Mohamed Anesary, N.; Lu, B.; Paris, S. NBTXR3 Radiotherapy-Activated Functionalized Hafnium Oxide Nanoparticles Show Efficient Antitumor Effects Across a Large Panel of Human Cancer Models. Int. J. Nanomed. 2021, 16, 2761–2773. [Google Scholar] [CrossRef]
- Nanobiotix. A Phase I-II Dose-Escalation Study of NBTXR3 Activated by EBRT or EBRT with Brachytherapy in Patients with Newly Diagnosed Unfavorable Intermediate or High Risk Prostate Adenocarcinoma Treated with Androgen Deprivation. Available online: https://clinicaltrials.gov/ct2/show/NCT02805894 (accessed on 31 March 2023).
- Hara, D.; Tao, W.; Totiger, T.M.; Pourmand, A.; Dogan, N.; Ford, J.C.; Shi, J.; Pollack, A. Prostate Cancer Targeted X-ray Fluorescence Imaging via Gold Nanoparticles Functionalized with Prostate-Specific Membrane Antigen (PSMA). Int. J. Radiat. Oncol. Biol. Phys. 2021, 111, 220–232. [Google Scholar] [CrossRef]
- Hara, D.; Tao, W.; Schmidt, R.M.; Yang, Y.-P.; Daunert, S.; Dogan, N.; Ford, J.C.; Pollack, A.; Shi, J. Boosted Radiation Bystander Effect of PSMA-Targeted Gold Nanoparticles in Prostate Cancer Radiosensitization. Nanomaterials 2022, 12, 4440. [Google Scholar] [CrossRef]
- Albanese, A.; Tang, P.S.; Chan, W.C.W. The Effect of Nanoparticle Size, Shape, and Surface Chemistry on Biological Systems. Annu. Rev. Biomed. Eng. 2012, 14, 1–16. [Google Scholar] [CrossRef]
- Adewale, O.B.; Davids, H.; Cairncross, L.; Roux, S. Toxicological Behavior of Gold Nanoparticles on Various Models: Influence of Physicochemical Properties and Other Factors. Int. J. Toxicol. 2019, 38, 357–384. [Google Scholar] [CrossRef]
- Ko, W.-C.; Wang, S.-J.; Hsiao, C.-Y.; Hung, C.-T.; Hsu, Y.-J.; Chang, D.-C.; Hung, C.-F. Pharmacological Role of Functionalized Gold Nanoparticles in Disease Applications. Molecules 2022, 27, 1551. [Google Scholar] [CrossRef] [PubMed]
- Fukuhara, H.; Homma, Y.; Todo, T. Oncolytic Virus Therapy for Prostate Cancer. Int. J. Urol. Off. J. Jpn. Urol. Assoc. 2010, 17, 20–30. [Google Scholar] [CrossRef] [PubMed]
- Taguchi, S.; Fukuhara, H.; Homma, Y.; Todo, T. Current Status of Clinical Trials Assessing Oncolytic Virus Therapy for Urological Cancers. Int. J. Urol. 2017, 24, 342–351. [Google Scholar] [CrossRef] [PubMed]
- Hawkey, N.M.; Broderick, A.; George, D.J.; Sartor, O.; Armstrong, A.J. The Value of Phenotypic Precision Medicine in Prostate Cancer. Oncologist 2022, 28, 93–104. [Google Scholar] [CrossRef]
- Del Pino-Sedeño, T.; Infante-Ventura, D.; de Armas Castellano, A.; de Pablos-Rodríguez, P.; Rueda-Domínguez, A.; Serrano-Aguilar, P.; Trujillo-Martín, M.M. Molecular Biomarkers for the Detection of Clinically Significant Prostate Cancer: A Systematic Review and Meta-Analysis. Eur. Urol. Open Sci. 2022, 46, 105–127. [Google Scholar] [CrossRef]
- Rasmussen, M.; Fredsøe, J.; Tin, A.L.; Vickers, A.J.; Ulhøi, B.; Borre, M.; Eastham, J.; Ehdaie, B.; Guillonneau, B.; Laudone, V.; et al. Independent Validation of a Pre-Specified Four-Kallikrein Marker Model for Prediction of Adverse Pathology and Biochemical Recurrence. Br. J. Cancer 2022, 126, 1004–1009. [Google Scholar] [CrossRef]
- Hamid, S.; Donaldson, I.A.; Hu, Y.; Rodell, R.; Villarini, B.; Bonmati, E.; Tranter, P.; Punwani, S.; Sidhu, H.S.; Willis, S.; et al. The SmartTarget Biopsy Trial: A Prospective, Within-Person Randomised, Blinded Trial Comparing the Accuracy of Visual-Registration and Magnetic Resonance Imaging/Ultrasound Image-Fusion Targeted Biopsies for Prostate Cancer Risk Stratification. Eur. Urol. 2019, 75, 733–740. [Google Scholar] [CrossRef]
- Strati, A.; Markou, A.; Kyriakopoulou, E.; Lianidou, E. Detection and Molecular Characterization of Circulating Tumour Cells: Challenges for the Clinical Setting. Cancers 2023, 15, 2185. [Google Scholar] [CrossRef]
- Boehm, B.E.; York, M.E.; Petrovics, G.; Kohaar, I.; Chesnut, G.T. Biomarkers of Aggressive Prostate Cancer at Diagnosis. Int. J. Mol. Sci. 2023, 24, 2185. [Google Scholar] [CrossRef]
- Gongora, M.; Stranne, J.; Johansson, E.; Bottai, M.; Thellenberg Karlsson, C.; Brasso, K.; Hansen, S.; Jakobsen, H.; Jäderling, F.; Lindberg, H.; et al. Characteristics of Patients in SPCG-15—A Randomized Trial Comparing Radical Prostatectomy with Primary Radiotherapy plus Androgen Deprivation Therapy in Men with Locally Advanced Prostate Cancer. Eur. Urol. Open Sci. 2022, 41, 63–73. [Google Scholar] [CrossRef]
- Petrelli, F.; De Stefani, A.; Vavassori, I.; Motta, F.; Luciani, A.; Trevisan, F. Duration of Androgen Deprivation with Radio-Therapy for High-Risk or Locally Advanced Prostate Cancer: A Network Meta-Analysis. Tumori 2023. [Google Scholar] [CrossRef] [PubMed]
- Braga-Basaria, M.; Travison, T.G.; Taplin, M.-E.; Lin, A.; Dufour, A.B.; Habtemariam, D.; Nguyen, P.L.; Kibel, A.S.; Ravi, P.; Bearup, R.; et al. Gaining Metabolic Insight in Older Men Undergoing Androgen Deprivation Therapy for Prostate Cancer (the ADT & Metabolism Study): Protocol of a Longitudinal, Observational, Cohort Study. PLoS ONE 2023, 18, e0281508. [Google Scholar] [CrossRef]
- Association Pour La Recherche des Thérapeutiques Innovantes en Cancérologie. Evaluation of DAroLutamide Addition to AnDrogen Deprivation Therapy and RadIatioN Therapy in Newly Diagnosed Prostate Cancer with Pelvic Lymph Nodes Metastases. Available online: https://clinicaltrials.gov/ct2/show/NCT05116475 (accessed on 31 March 2023).
- Fondazione IRCCS Istituto Nazionale dei Tumori, Milano. APPROACH: Multimodal Approach in Patients with MHSPC. A Pragmatic Randomized Trial of Apalutamide Plus Androgen Deprivation Therapy (APA-ADT) Versus APA-ADT Plus Local Treatment. A Meet-URO 29 Study. Available online: https://clinicaltrials.gov/ct2/show/NCT05649943 (accessed on 31 March 2023).
- Alaimo, A.; Lorenzoni, M.; Ambrosino, P.; Bertossi, A.; Bisio, A.; Macchia, A.; Zoni, E.; Genovesi, S.; Cambuli, F.; Foletto, V.; et al. Calcium Cytotoxicity Sensitizes Prostate Cancer Cells to Standard-of-Care Treatments for Locally Advanced Tumors. Cell Death Dis. 2020, 11, 1039. [Google Scholar] [CrossRef] [PubMed]
- Nazıroğlu, M.; Blum, W.; Jósvay, K.; Çiğ, B.; Henzi, T.; Oláh, Z.; Vizler, C.; Schwaller, B.; Pecze, L. Menthol Evokes Ca2+ Signals and Induces Oxidative Stress Independently of the Presence of TRPM8 (Menthol) Receptor in Cancer Cells. Redox Biol. 2018, 14, 439–449. [Google Scholar] [CrossRef]
- Mørk, S.K.; Kongsted, P.; Westergaard, M.C.W.; Albieri, B.; Granhøj, J.S.; Donia, M.; Martinenaite, E.; Holmström, M.O.; Madsen, K.; Kverneland, A.H.; et al. First in Man Study: Bcl-Xl_42-CAF®09b Vaccines in Patients with Locally Advanced Prostate Cancer. Front. Immunol. 2023, 14, 1122977. [Google Scholar] [CrossRef]
- Bilusic, M.; Madan, R.A.; Gulley, J.L. Immunotherapy of Prostate Cancer: Facts and Hopes. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2017, 23, 6764–6770. [Google Scholar] [CrossRef]
- Von Amsberg, G.; Alsdorf, W.; Karagiannis, P.; Coym, A.; Kaune, M.; Werner, S.; Graefen, M.; Bokemeyer, C.; Merkens, L.; Dyshlovoy, S.A. Immunotherapy in Advanced Prostate Cancer—Light at the End of the Tunnel? Int. J. Mol. Sci. 2022, 23, 2569. [Google Scholar] [CrossRef]
- Rehman, L.u.; Nisar, M.H.; Fatima, W.; Sarfraz, A.; Azeem, N.; Sarfraz, Z.; Robles-Velasco, K.; Cherrez-Ojeda, I. Immunotherapy for Prostate Cancer: A Current Systematic Review and Patient Centric Perspectives. J. Clin. Med. 2023, 12, 1446. [Google Scholar] [CrossRef]
- Achard, V.; Panje, C.M.; Engeler, D.; Zilli, T.; Putora, P.M. Localized and Locally Advanced Prostate Cancer: Treatment Options. Oncology 2021, 99, 413–421. [Google Scholar] [CrossRef]
- NICE Guidance. Prostate Cancer: Diagnosis and Management: Recommendations. Available online: https://www.nice.org.uk/guidance/ng131/chapter/recommendations (accessed on 14 May 2023).
- Williams, N.; Orczyk, C. PO-1132 RCT Evidence in 2018 ASTRO/ASCO/AUA Guidelines for Hypofractionated Radiotherapy in Prostate Cancer. Radiother. Oncol. 2019, 133, S628. [Google Scholar] [CrossRef]
- Gillessen, S.; Bossi, A.; Davis, I.D.; de Bono, J.; Fizazi, K.; James, N.D.; Mottet, N.; Shore, N.; Small, E.; Smith, M.; et al. Management of Patients with Advanced Prostate Cancer. Part I: Intermediate-/High-Risk and Locally Advanced Disease, Biochemical Relapse, and Side Effects of Hormonal Treatment: Report of the Advanced Prostate Cancer Consensus Conference 2022. Eur. Urol. 2023, 83, 267–293. [Google Scholar] [CrossRef] [PubMed]
- Nabian, N.; Ghalehtaki, R.; Couñago, F. Necessity of Pelvic Lymph Node Irradiation in Patients with Recurrent Prostate Cancer after Radical Prostatectomy in the PSMA PET/CT Era: A Narrative Review. Biomedicines 2023, 11, 38. [Google Scholar] [CrossRef] [PubMed]
- De Meerleer, G.; Berghen, C.; Briganti, A.; Vulsteke, C.; Murray, J.; Joniau, S.; Leliveld, A.M.; Cozzarini, C.; Decaestecker, K.; Rans, K.; et al. Elective Nodal Radiotherapy in Prostate Cancer. Lancet Oncol. 2021, 22, e348–e357. [Google Scholar] [CrossRef]
- Weintraub, K. Biomedicine: The New Gold Standard. Nature 2013, 495, S14–S16. [Google Scholar] [CrossRef] [PubMed]
- Sibuyi, N.R.S.; Thipe, V.C.; Panjtan-Amiri, K.; Meyer, M.; Katti, K.V. Green Synthesis of Gold Nanoparticles Using Acai Berry and Elderberry Extracts and Investigation of Their Effect on Prostate and Pancreatic Cancer Cells. Nanobiomedicine 2021, 8, 1849543521995310. [Google Scholar] [CrossRef] [PubMed]
- Shabnam, N.; Pardha-Saradhi, P. Photosynthetic Electron Transport System Promotes Synthesis of Au-Nanoparticles. PLoS ONE 2013, 8, e71123. [Google Scholar] [CrossRef]
- Schmidt, R.M.; Hara, D.; Vega, J.D.; Abuhaija, M.B.; Tao, W.; Dogan, N.; Pollack, A.; Ford, J.C.; Shi, J. Quantifying Radiosensitization of PSMA-Targeted Gold Nanoparticles on Prostate Cancer Cells at Megavoltage Radiation Energies by Monte Carlo Simulation and Local Effect Model. Pharmaceutics 2022, 14, 2205. [Google Scholar] [CrossRef]
- Breitkreutz, D.Y.; Weil, M.D.; Bazalova-Carter, M. External Beam Radiation Therapy with Kilovoltage X-rays. Phys. Med. Eur. J. Med. Phys. 2020, 79, 103–112. [Google Scholar] [CrossRef]
- Culp, M.B.; Soerjomataram, I.; Efstathiou, J.A.; Bray, F.; Jemal, A. Recent Global Patterns in Prostate Cancer Incidence and Mortality Rates. Eur. Urol. 2020, 77, 38–52. [Google Scholar] [CrossRef]
- Bosland, M.C.; Shittu, O.B.; Ikpi, E.E.; Akinloye, O. Potential New Approaches for Prostate Cancer Management in Resource-Limited Countries in Africa. Ann. Glob. Health 2023, 89, 14. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Country of PI | Number of Studies |
|---|---|
| USA | 36 |
| Canada | 10 |
| Colombia | 1 |
| Brazil | 1 |
| China | 7 |
| Denmark | 6 |
| France | 6 |
| Italy | 6 |
| Netherlands | 6 |
| Belgium | 5 |
| Switzerland | 4 |
| Germany | 3 |
| Norway | 2 |
| Sweden | 2 |
| Austria | 1 |
| Finland | 1 |
| Poland | 1 |
| UK | 1 |
| Turkey | 1 |
| Israel | 1 |
| Japan | 1 |
| Korea | 1 |
| NCT Number | Status * | Planned Enrollment | Study Design |
|---|---|---|---|
| NCT05613023 | Recruiting | 536 | Randomized: curative radiotherapy to the prostate and lymph glands to that of prostate alone |
| NCT05116475 | NYR | 152 | Randomized: Darolutamide vs. placebo |
| NCT04655365 | Recruiting | 50 | Non-randomized: 18 F-DCFPyL-PSMA PET/CT |
| NCT05269550 | Recruiting | 50 | Non-randomized: evaluation of imaging biomarkers post radiotherapy |
| NCT05754580 | NYR | 53 | Non-randomized: High-dose rate (HDR) brachytherapy boost with stereostatic body radiation therapy (SBRT) |
| NCT05847166 | NYR | 80 | Non-randomized: [99 mTc]Tc-PSMA-T4 |
| NCT05596851 | Recruiting | 15 | Observational: β-probe and 68 Ga-PSMA-11 PET/CT |
| NCT05252806 | NYR | 30 | Observational: Quantitative mpMRI to predict metastatic potential of prostate cancer |
| NCT05705700 | Withdrawn | 0 |
| Intervention | Number of Studies |
|---|---|
| Drug | 45 |
| Procedure | 27 |
| Radiation | 22 * |
| Diagnostic test | 14 |
| Biological | 5 |
| Device | 6 |
| Other | 10 |
| Not applicable (observational study) | 3 |
| Type of Radiation Intervention | Number of Studies |
|---|---|
| Radiation therapy | 9 |
| Radiation to the prostate bed with or without addition of lymph node irradiation | 1 |
| Hypofractionation | 2 |
| Intensity-modulated radiation therapy | 2 |
| Intensity-modulated radiotherapy of the pelvic lymph nodes using simultaneous integrated boost (SIB) | 1 |
| Stereotactic ablative radiotherapy | 1 |
| Simultaneous integrated boost (SIB) dose-escalation radiotherapy | 1 |
| Stereotactic body radiotherapy (SBRT) | 2 |
| Stereotactic ablative radiotherapy | 1 |
| Brachytherapy | 1 |
| High-dose brachytherapy | 1 |
| Proton plus carbon ion radiation | 1 |
| [99 mTc]Tc-PSMA-T4 | 1 |
| PET scan, whole-body MRI | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Williams, N.R. Analysis of Clinical Trials and Review of Recent Advances in Therapy Decisions for Locally Advanced Prostate Cancer. J. Pers. Med. 2023, 13, 938. https://doi.org/10.3390/jpm13060938
Williams NR. Analysis of Clinical Trials and Review of Recent Advances in Therapy Decisions for Locally Advanced Prostate Cancer. Journal of Personalized Medicine. 2023; 13(6):938. https://doi.org/10.3390/jpm13060938
Chicago/Turabian StyleWilliams, Norman R. 2023. "Analysis of Clinical Trials and Review of Recent Advances in Therapy Decisions for Locally Advanced Prostate Cancer" Journal of Personalized Medicine 13, no. 6: 938. https://doi.org/10.3390/jpm13060938
APA StyleWilliams, N. R. (2023). Analysis of Clinical Trials and Review of Recent Advances in Therapy Decisions for Locally Advanced Prostate Cancer. Journal of Personalized Medicine, 13(6), 938. https://doi.org/10.3390/jpm13060938