
COPD Patients with Asthma Features in Vietnam: Prevalence and Suitability for Personalized Medicine
 ,
,  ,
,
Abstract
1. Introduction
2. Patients and Methods
2.1. Study Design
2.2. Patients
2.3. Data Collection
2.4. Diagnosing COPD Patients with Asthma Features
2.5. Statistical Analysis
3. Results
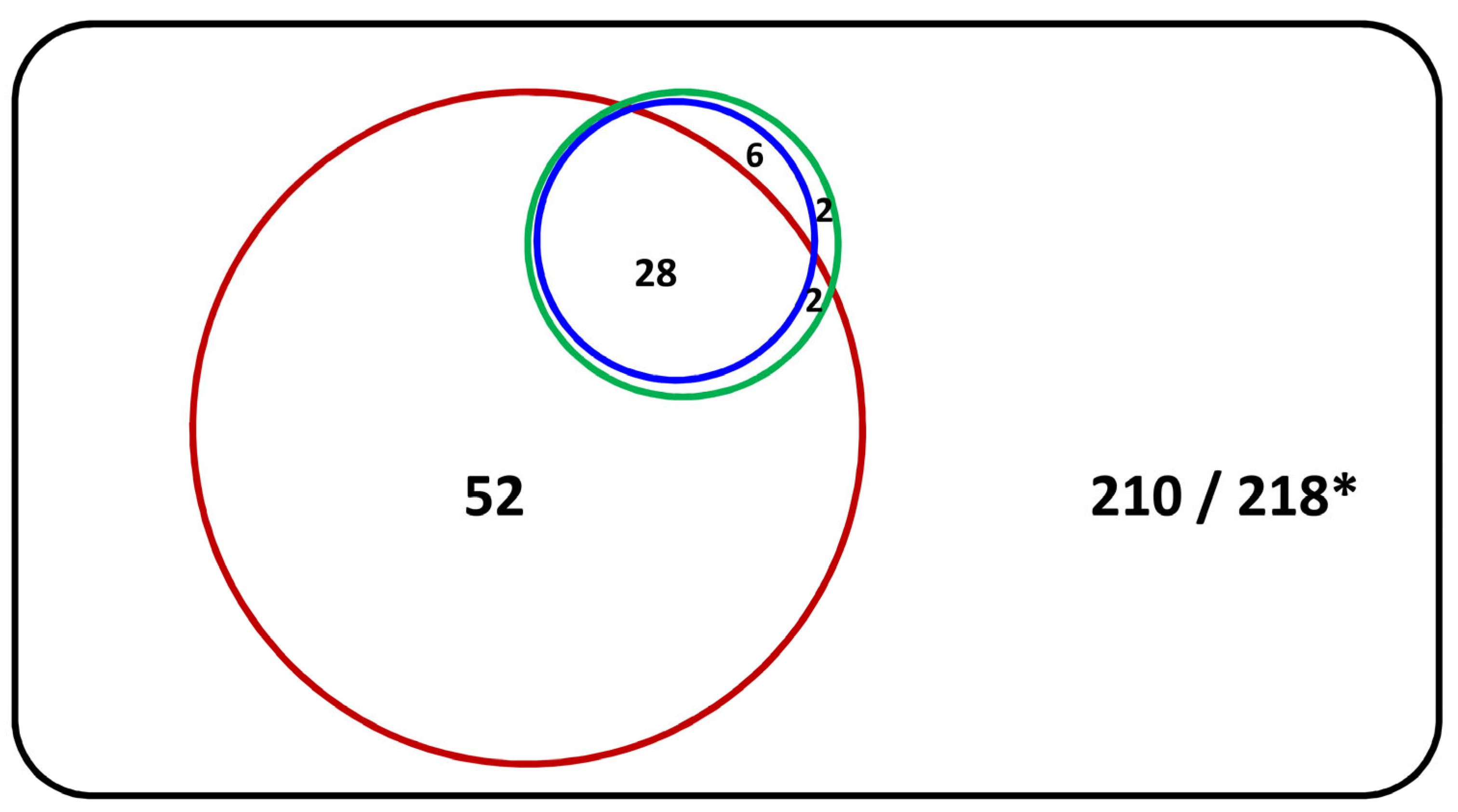
3.1. The Proportion of COPD Patients with Asthma Features
3.2. Characteristics of COPD Patients with Asthma Features
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mekov, E.; Nunez, A.; Sin, D.D.; Ichinose, M.; Rhee, C.K.; Maselli, D.J.; Cote, A.; Suppli Ulrik, C.; Maltais, F.; Anzueto, A.; et al. Update on Asthma-COPD Overlap (ACO): A Narrative Review. Int. J. Chronic Obstr. Pulm. Dis. 2021, 16, 1783–1799. [Google Scholar] [CrossRef] [PubMed]
- Mart, M.F.; Peebles, R.S., Jr. Asthma-chronic obstructive pulmonary disease overlap syndrome. Curr. Opin. Immunol. 2020, 66, 161–166. [Google Scholar] [CrossRef] [PubMed]
- Global Initiative for Asthma (GINA). Global Strategy for Asthma Management and Prevention (Updated 2022). Available online: http://www.ginasthma.org/ (accessed on 5 May 2022).
- Gibson, P.G.; McDonald, V.M. Asthma-COPD overlap 2015: Now we are six. Thorax 2015, 70, 683–691. [Google Scholar] [CrossRef] [PubMed]
- Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease (2023 Report). Available online: http://www.goldcopd.org/ (accessed on 15 November 2022).
- Chung, W.S.; Lin, C.L.; Kao, C.H. Comparison of acute respiratory events between asthma-COPD overlap syndrome and COPD patients: A population-based cohort study. Medicine 2015, 94, e755. [Google Scholar] [CrossRef]
- Hardin, M.; Silverman, E.K.; Barr, R.G.; Hansel, N.N.; Schroeder, J.D.; Make, B.J.; Crapo, J.D.; Hersh, C.P. The clinical features of the overlap between COPD and asthma. Respir. Res. 2011, 12, 127. [Google Scholar] [CrossRef]
- Rhee, C.K.; Yoon, H.K.; Yoo, K.H.; Kim, Y.S.; Lee, S.W.; Park, Y.B.; Lee, J.H.; Kim, Y.; Kim, K.; Kim, J.; et al. Medical utilization and cost in patients with overlap syndrome of chronic obstructive pulmonary disease and asthma. COPD 2014, 11, 163–170. [Google Scholar] [CrossRef]
- Maselli, D.J.; Hardin, M.; Christenson, S.A.; Hanania, N.A.; Hersh, C.P.; Adams, S.G.; Anzueto, A.; Peters, J.I.; Han, M.K.; Martinez, F.J. Clinical Approach to the Therapy of Asthma-COPD Overlap. Chest 2019, 155, 168–177. [Google Scholar] [CrossRef]
- Tho, N.V.; Park, H.Y.; Nakano, Y. Asthma-COPD overlap syndrome (ACOS): A diagnostic challenge. Respirology 2016, 21, 410–418. [Google Scholar] [CrossRef] [PubMed]
- Alsayed, A.R.; Abu-Samak, M.S.; Alkhatib, M. Asthma-COPD Overlap in Clinical Practice (ACO_CP 2023): Toward Precision Medicine. J. Pers. Med. 2023, 13, 677. [Google Scholar] [CrossRef]
- GINA and GOLD. Diagnosis of Diseases of Chronic Airflow Limitation: Asthma, Copd and Asthma-Copd Overlap Syndrome (ACOS) (updated 2015). Available online: http://www.ginasthma.org/ (accessed on 13 April 2015).
- Yanagisawa, S.; Ichinose, M. Definition and diagnosis of asthma-COPD overlap (ACO). Allergol. Int. 2018, 67, 172–178. [Google Scholar] [CrossRef]
- Miravitlles, M.; Alvarez-Gutierrez, F.J.; Calle, M.; Casanova, C.; Cosio, B.G.; Lopez-Vina, A.; Perez de Llano, L.; Quirce, S.; Roman-Rodriguez, M.; Soler-Cataluna, J.J.; et al. Algorithm for identification of asthma-COPD overlap: Consensus between the Spanish COPD and asthma guidelines. Eur. Respir. J. 2017, 49, 1700068. [Google Scholar] [CrossRef] [PubMed]
- Sin, D.D.; Miravitlles, M.; Mannino, D.M.; Soriano, J.B.; Price, D.; Celli, B.R.; Leung, J.M.; Nakano, Y.; Park, H.Y.; Wark, P.A.; et al. What is asthma-COPD overlap syndrome? Towards a consensus definition from a round table discussion. Eur. Respir. J. 2016, 48, 664–673. [Google Scholar] [CrossRef] [PubMed]
- Chu, H.T.; Nguyen, T.C.; Godin, I.; Michel, O. A Proposal to Differentiate ACO, Asthma and COPD in Vietnam. J. Pers. Med. 2022, 13, 78. [Google Scholar] [CrossRef]
- Fouka, E.; Papaioannou, A.I.; Hillas, G.; Steiropoulos, P. Asthma-COPD Overlap Syndrome: Recent Insights and Unanswered Questions. J. Pers. Med. 2022, 12, 708. [Google Scholar] [CrossRef]
- Reddel, H.K.; Vestbo, J.; Agusti, A.; Anderson, G.P.; Bansal, A.T.; Beasley, R.; Bel, E.H.; Janson, C.; Make, B.; Pavord, I.D.; et al. Heterogeneity within and between physician-diagnosed asthma and/or COPD: NOVELTY cohort. Eur. Respir. J. 2021, 58, 2003927. [Google Scholar] [CrossRef] [PubMed]
- Barrecheguren, M.; Pinto, L.; Mostafavi-Pour-Manshadi, S.M.; Tan, W.C.; Li, P.Z.; Aaron, S.D.; Benedetti, A.; Chapman, K.R.; Walker, B.; Fitzgerald, J.M.; et al. Identification and definition of asthma-COPD overlap: The CanCOLD study. Respirology 2020, 25, 836–849. [Google Scholar] [CrossRef] [PubMed]
- Nunez, A.; Sarasate, M.; Loeb, E.; Esquinas, C.; Miravitlles, M.; Barrecheguren, M. Practical Guide to the Identification and Diagnosis of Asthma-COPD Overlap (ACO). COPD 2019, 16, 1–7. [Google Scholar] [CrossRef]
- Leung, C.; Sin, D.D. Asthma-COPD Overlap: What Are the Important Questions? Chest 2022, 161, 330–344. [Google Scholar] [CrossRef]
- Jones, P.W.; Harding, G.; Berry, P.; Wiklund, I.; Chen, W.H.; Kline Leidy, N. Development and first validation of the COPD Assessment Test. Eur. Respir. J. 2009, 34, 648–654. [Google Scholar] [CrossRef]
- Graham, B.L.; Steenbruggen, I.; Miller, M.R.; Barjaktarevic, I.Z.; Cooper, B.G.; Hall, G.L.; Hallstrand, T.S.; Kaminsky, D.A.; McCarthy, K.; McCormack, M.C.; et al. Standardization of Spirometry 2019 Update. An Official American Thoracic Society and European Respiratory Society Technical Statement. Am. J. Respir. Crit. Care Med. 2019, 200, e70–e88. [Google Scholar] [CrossRef]
- Hankinson, J.L.; Kawut, S.M.; Shahar, E.; Smith, L.J.; Stukovsky, K.H.; Barr, R.G. Performance of American Thoracic Society-recommended spirometry reference values in a multiethnic sample of adults: The multi-ethnic study of atherosclerosis (MESA) lung study. Chest 2010, 137, 138–145. [Google Scholar] [CrossRef]
- Inoue, H.; Nagase, T.; Morita, S.; Yoshida, A.; Jinnai, T.; Ichinose, M. Prevalence and characteristics of asthma-COPD overlap syndrome identified by a stepwise approach. Int. J. Chronic Obstr. Pulm. Dis. 2017, 12, 1803–1810. [Google Scholar] [CrossRef]
- Lim, J.U.; Kim, D.K.; Lee, M.G.; Hwang, Y.I.; Shin, K.C.; In, K.H.; Lee, S.Y.; Rhee, C.K.; Yoo, K.H.; Yoon, H.K. Clinical Characteristics and Changes of Clinical Features in Patients with Asthma-COPD Overlap in Korea according to Different Diagnostic Criteria. Tuberc. Respir. Dis. 2020, 83, S34–S45. [Google Scholar] [CrossRef]
- Kang, J.; Zheng, J.; Cai, B.; Wen, F.; Yao, W.; Zhang, X.; Chen, Y.; Wang, G.; Li, W.; Cao, J. Current situation of asthma-COPD overlap in Chinese patients older than 40 years with airflow limitation: A multicenter, cross-sectional, non-interventional study. Ther. Adv. Respir. Dis. 2020, 14, 1753466620961699. [Google Scholar] [CrossRef]
- Barczyk, A.; Maskey-Warzechowska, M.; Gorska, K.; Barczyk, M.; Kuziemski, K.; Sliwinski, P.; Batura-Gabryel, H.; Mroz, R.; Kania, A.; Obojski, A.; et al. Asthma-COPD Overlap-A Discordance Between Patient Populations Defined by Different Diagnostic Criteria. J. Allergy Clin. Immunol. Pract. 2019, 7, 2326–2336.e5. [Google Scholar] [CrossRef]
- Krishnan, J.A.; Nibber, A.; Chisholm, A.; Price, D.; Bateman, E.D.; Bjermer, L.; van Boven, J.F.M.; Brusselle, G.; Costello, R.W.; Dandurand, R.J.; et al. Prevalence and Characteristics of Asthma-Chronic Obstructive Pulmonary Disease Overlap in Routine Primary Care Practices. Ann. Am. Thorac. Soc. 2019, 16, 1143–1150. [Google Scholar] [CrossRef] [PubMed]
- Toledo-Pons, N.; van Boven, J.F.M.; Roman-Rodriguez, M.; Perez, N.; Valera Felices, J.L.; Soriano, J.B.; Cosio, B.G. ACO: Time to move from the description of different phenotypes to the treatable traits. PLoS ONE 2019, 14, e0210915. [Google Scholar] [CrossRef] [PubMed]
- Hashimoto, S.; Sorimachi, R.; Jinnai, T.; Ichinose, M. Asthma and Chronic Obstructive Pulmonary Disease Overlap According to the Japanese Respiratory Society Diagnostic Criteria: The Prospective, Observational ACO Japan Cohort Study. Adv. Ther. 2021, 38, 1168–1184. [Google Scholar] [CrossRef] [PubMed]
- Kondo, M.; Tamaoki, J. Therapeutic approaches of asthma and COPD overlap. Allergol. Int. 2018, 67, 187–190. [Google Scholar] [CrossRef]
- Gershon, A.S.; Campitelli, M.A.; Croxford, R.; Stanbrook, M.B.; To, T.; Upshur, R.; Stephenson, A.L.; Stukel, T.A. Combination long-acting beta-agonists and inhaled corticosteroids compared with long-acting beta-agonists alone in older adults with chronic obstructive pulmonary disease. JAMA 2014, 312, 1114–1121. [Google Scholar] [CrossRef]
- Lee, S.Y.; Park, H.Y.; Kim, E.K.; Lim, S.Y.; Rhee, C.K.; Hwang, Y.I.; Oh, Y.M.; Lee, S.D.; Park, Y.B. Combination therapy of inhaled steroids and long-acting beta2-agonists in asthma-COPD overlap syndrome. Int. J. Chronic Obstr. Pulm. Dis. 2016, 11, 2797–2803. [Google Scholar] [CrossRef] [PubMed]
- Wurst, K.E.; Rheault, T.R.; Edwards, L.; Tal-Singer, R.; Agusti, A.; Vestbo, J. A comparison of COPD patients with and without ACOS in the ECLIPSE study. Eur. Respir. J. 2016, 47, 1559–1562. [Google Scholar] [CrossRef] [PubMed]
- Hiles, S.A.; Gibson, P.G.; McDonald, V.M. Disease burden of eosinophilic airway disease: Comparing severe asthma, COPD and asthma-COPD overlap. Respirology 2021, 26, 52–61. [Google Scholar] [CrossRef] [PubMed]
- Celli, B.R.; Anderson, J.A.; Cowans, N.J.; Crim, C.; Hartley, B.F.; Martinez, F.J.; Morris, A.N.; Quasny, H.; Yates, J.; Vestbo, J.; et al. Pharmacotherapy and Lung Function Decline in Patients with Chronic Obstructive Pulmonary Disease. A Systematic Review. Am. J. Respir. Crit. Care Med. 2021, 203, 689–698. [Google Scholar] [CrossRef]
- Albert, P.; Agusti, A.; Edwards, L.; Tal-Singer, R.; Yates, J.; Bakke, P.; Celli, B.R.; Coxson, H.O.; Crim, C.; Lomas, D.A.; et al. Bronchodilator responsiveness as a phenotypic characteristic of established chronic obstructive pulmonary disease. Thorax 2012, 67, 701–708. [Google Scholar] [CrossRef]
- Alsayed, A.R.; Abed, A.; Jarrar, Y.B.; Alshammari, F.; Alshammari, B.; Basheti, I.A.; Zihlif, M. Alteration of the Respiratory Microbiome in Hospitalized Patients with Asthma-COPD Overlap during and after an Exacerbation. J. Clin. Med. 2023, 12, 2118. [Google Scholar] [CrossRef]


{kind=link}
| Features | COPD with Asthma Features * (n = 82) | COPD Alone * (n = 218) | p-Value |
|---|---|---|---|
| Features that favor asthma | |||
| Symptoms vary over time | 43 (52.4%) | 40 (18.4%) | <0.001 |
| Symptoms vary seasonally | 19 (23.2%) | 9 (4.1%) | <0.001 |
| Symptoms worsen during the night or early morning | 42 (51.2%) | 18 (8.3%) | <0.001 |
| Symptoms are triggered by exercise, emotional change, or exposure to dust/allergens | 42 (51.2%) | 23 (10.6%) | <0.001 |
| Symptoms do not worsen over time | 17 (20.7%) | 3 (1.4%) | <0.001 |
| Symptoms improve spontaneously | 16 (19.5%) | 15 (6.9%) | 0.002 |
| Symptoms improve over weeks with ICS treatment | 37 (45.2%) | 15 (6.9%) | <0.001 |
| Record of reversible airflow limitation | 4 (4.9%) | 12 (5.5%) | 0.828 |
| Allergic rhinitis | 13 (15.9%) | 3 (1.4%) | <0.001 |
| Physician-diagnosed asthma | 28 (34.1%) | 6 (2.8%) | <0.001 |
| Family history of asthma | 9 (11.0%) | 7 (3.2%) | 0.016 |
| Features that favor COPD | |||
| Symptoms onset after 40 years old | 68 (89.5%) | 207 (97.6%) | 0.006 |
| Symptoms persist despite treatment | 33 (40.2%) | 146 (67.0%) | <0.001 |
| Good/bad days but symptoms are observed on a daily basis | 22 (26.8%) | 130 (59.6%) | <0.001 |
| Chronic cough and sputum precede onset of dyspnea and are unrelated to triggers | 40 (48.8%) | 159 (72.9%) | <0.001 |
| Symptoms slowly worsen over time | 52 (63.4%) | 181 (83.0%) | <0.001 |
| Rapid-acting bronchodilator treatment provides only limited relief | 34 (41.5%) | 118 (54.1%) | 0.050 |
| Record of persistent airflow limitation | 80 (97.6%) | 213 (97.7%) | 0.941 |
| Abnormal lung function between symptoms | (n = 52) 52 (100.0%) | (n = 117) 111 (94.9%) | 0.034 |
| Hyperinflation on chest X-ray | (n = 52) 21 (40.4%) | (n = 73) 45 (31.0%) | 0.225 |
| Characteristics | Total (n = 300) | COPD with Asthma Features * (n = 82) | COPD Alone * (n = 218) | p-Value |
|---|---|---|---|---|
| Age (years) | 65.0 ± 9.7 | 62.7 ± 10.6 | 65.8 ± 9.2 | 0.021 |
| Age at symptoms onset (years) | 60.5 ± 12.2 | 56.0 ± 15.8 | 62.1 ± 10.2 | 0.004 |
| Female | 24 (8.0%) | 14 (17.1%) | 10 (4.6%) | <0.001 |
| Weight (kg) | 55.4 ± 9.7 | 55.9 ± 8.8 | 55.2 ± 10.0 | 0.572 |
| Height (cm) | 160.1 ± 6.7 | 159.7 ± 6.8 | 160.2 ± 6.6 | 0.585 |
| BMI (kg/m2) | 21.6 ± 3.6 | 21.9 ± 3.4 | 21.5 ± 3.6 | 0.345 |
| Current smoker | 53 (17.7%) | 15 (18.3%) | 38 (17.4%) | <0.001 |
| Ex-smoker | 202 (67.3%) | 40 (48.8%) | 162 (74.3%) | |
| Non-smoker | 45 (15.0%) | 27 (32.9%) | 18 (8.3%) | |
| Pack-years | (n = 237) 33.7 ± 17.9 | (n = 53) 34.0 ± 18.7 | (n = 184) 33.6 ± 17.7 | 0.884 |
| Comorbidities | ||||
| Hypertension | 56 (18.7%) | 16 (19.5%) | 40 (18.4%) | 0.818 |
| Allergic rhinitis | 16 (5.5%) | 13 (15.9%) | 3 (1.4%) | <0.001 |
| GERD | 16 (5.5%) | 4 (4.9%) | 12 (5.5%) | 0.828 |
| Ischemic heart disease | 14 (4.7%) | 4 (4.9%) | 10 (4.6%) | 0.916 |
| Diabetes mellitus | 10 (3.3%) | 2 (2.4%) | 8 (3.7%) | 0.585 |
| Characteristics | Total (n = 300) | COPD with Asthma Features * (n = 82) | COPD Alone * (n = 218) | p-Value |
|---|---|---|---|---|
| ≥1 exacerbation in the previous year | 90 (30.0%) | 22 (26.8%) | 68 (31.2%) | 0.459 |
| ≥2 exacerbations in the previous year | 45 (15.0%) | 8 (9.8%) | 37 (17.0%) | 0.106 |
| ≥1 hospitalization in the previous year | 45 (15.0%) | 11 (13.4%) | 34 (15.6%) | 0.634 |
| CAT | (n = 181) 16.0 ± 6.3 | (n = 45) 14.8 ± 5.6 | (n = 136) 16.4 ± 6.5 | 0.111 |
| CAT ≥ 10 | 151 (83.4%) | 37 (82.2%) | 114 (83.8%) | 0.804 |
| mMRC | (n = 179) 2 (2; 3) | (n = 54) 2 (2; 3) | (n = 125) 2 (2; 3) | 0.091 |
| mMRC ≥ 2 | 143 (79.9%) | 42 (77.8%) | 101 (80.8%) | 0.646 |
| Blood eosinophil count (per µL) | (n = 36) 190 (102.5; 297.5) | (n = 10) 310 (162.5; 650) | (n = 26) 145 (100; 215) | 0.016 |
| Blood eosinophil percent | 2.3% (1.2%; 3.8%) | 4.4% (2.2%; 6.7%) | 1.9% (1.0%; 2.8%) | 0.004 |
| Blood eosinophil ≥ 300/ µL | 9 (25.0%) | 5 (50.0%) | 4 (15.4%) | 0.038 |
| Blood eosinophil ≥ 3% | 12 (33.3%) | 7 (70.0%) | 5 (19.2%) | 0.007 |
| Characteristics | Total | COPD with Asthma Features * | COPD Alone * | p-Value |
|---|---|---|---|---|
| Latest spirometric measurement | ||||
| (n = 201) | (n = 54) | (n = 147) | ||
| % post-BD FEV1 | 54.6 ± 18.1 | 61.7 ± 16.1 | 52.0 ± 18.2 | <0.001 |
| % post-BD FVC | 74.2 ± 16.8 | 80.8 ± 14.4 | 71.8 ± 17.0 | <0.001 |
| Post-BD FEV1/FVC | 53.6 ± 11.6 | 57.4 ± 8.4 | 52.2 ± 12.3 | <0.001 |
| Bronchodilator reversibility at the first spirometric measurement | ||||
| (n = 284) | (n = 77) | (n = 207) | ||
| FEV1 change (mL) | 80 (20; 170) | 120 (50; 215) | 70 (20; 150) | 0.001 |
| %FEV1 change (%) | 7.9 (2.1; 15.7) | 11.8 (2.7; 21.6) | 7.0 (1.7; 14.2) | 0.014 |
| FEV1 increase ≥200 mL and ≥12% | 45 (15.8%) | 24 (31.2%) | 21 (10.1%) | <0.001 |
| FEV1 increase ≥400 mL and ≥15% | 7 (2.5%) | 5 (6.5%) | 2 (1.0%) | 0.017 |
| FEV1 change between the best and worst measurements during 3 years of follow up | ||||
| (n = 117) | (n = 36) | (n = 81) | ||
| Pre-BD FEV1 change (mL) | 240 (85; 420) | 300 (170; 600) | 200 (75; 355) | 0.012 |
| % pre-BD FEV1 change (%) | 8 (3; 17) | 10 (4; 24) | 7.0 (3; 15.5) | 0.298 |
| FEV1 increase ≥200 mL and ≥12% | 45 (38.5%) | 16 (44.4%) | 29 (35.8%) | 0.377 |
| FEV1 increase ≥400 mL and ≥15% | 22 (18.8%) | 11 (30.6%) | 11 (13.6%) | 0.035 |
| Medications | Total (n = 300) | COPD with Asthma Features * (n = 82) | COPD Alone * (n = 218) | p-Value |
|---|---|---|---|---|
| LABA † | 42 (14.0%) | 6 (7.3%) | 36 (16.5%) | 0.031 |
| LAMA | 104 (34.7%) | 24 (29.3%) | 80 (36.7%) | 0.224 |
| LABA/ICS ‡ | 240 (80.0%) | 73 (89.0%) | 167 (76.6%) | 0.012 |
| LABA/ICS + LAMA § | 70 (23.3%) | 20 (24.4%) | 50 (22.9%) | 0.791 |
| LTRA | 50 (16.7%) | 25 (30.5%) | 25 (11.5%) | <0.001 |
| Theophylline | 92 (30.7%) | 14 (17.1%) | 78 (35.8%) | 0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Van Tho, N.; Phan, T.P.; Dinh-Xuan, A.T.; Ngo, Q.C.; Lan, L.T.T. COPD Patients with Asthma Features in Vietnam: Prevalence and Suitability for Personalized Medicine. J. Pers. Med. 2023, 13, 901. https://doi.org/10.3390/jpm13060901
Van Tho N, Phan TP, Dinh-Xuan AT, Ngo QC, Lan LTT. COPD Patients with Asthma Features in Vietnam: Prevalence and Suitability for Personalized Medicine. Journal of Personalized Medicine. 2023; 13(6):901. https://doi.org/10.3390/jpm13060901
Chicago/Turabian StyleVan Tho, Nguyen, Thu Phuong Phan, Anh Tuan Dinh-Xuan, Quy Chau Ngo, and Le Thi Tuyet Lan. 2023. "COPD Patients with Asthma Features in Vietnam: Prevalence and Suitability for Personalized Medicine" Journal of Personalized Medicine 13, no. 6: 901. https://doi.org/10.3390/jpm13060901
APA StyleVan Tho, N., Phan, T. P., Dinh-Xuan, A. T., Ngo, Q. C., & Lan, L. T. T. (2023). COPD Patients with Asthma Features in Vietnam: Prevalence and Suitability for Personalized Medicine. Journal of Personalized Medicine, 13(6), 901. https://doi.org/10.3390/jpm13060901