
Effects of Adenotonsillectomy on Vocal Function



Abstract
1. Introduction
Objectives of the Study
2. Materials and Methods
2.1. Sample Collection
- (1)
- Medical History included information such as the following:
- -
- the mode of respiration as reported by parents (oral, nasal, or mixed);
- -
- the presence of breathing difficulties, nocturnal snoring, and/or obstructive apnea;
- -
- the presence of allergies; and
- -
- resting oral posture (closed, partially closed, or open).
- -
- the presence of closed nasality; and
- -
- the presence of subjective symptoms associated with phonatory activity (e.g., burning sensation, need to clear the throat, vocal fatigue, unstable voice, the feeling of a foreign body, muscular pain, etc.).
- (2)
- Otorhinolaryngological Clinical Investigation:
- -
- Grade 1 was characterized by intraglandular tonsils located behind the anterior tonsillar pillar.
- -
- Grade 2 tonsils were slightly hypertrophied and protruded just beyond the anterior pillar.
- -
- Grade 3 tonsils were hypertrophic and occupied three-quarters of the available space in the throat.
- -
- (3)
- Logopedic Evaluation of Pneumophonic Function:
- (4)
- Speech and Language Assessment:
- -
- Stable phonemes refer to the phonemes a child has acquired and uses reliably and systematically in his linguistic repertoire.
- -
- Occasional phonemes refer to the sounds that are consistently present in a child’s language but are occasionally replaced by other articulatory points.
- -
- Absent phonemes refer to articulating words absent in the child’s language.
- (5)
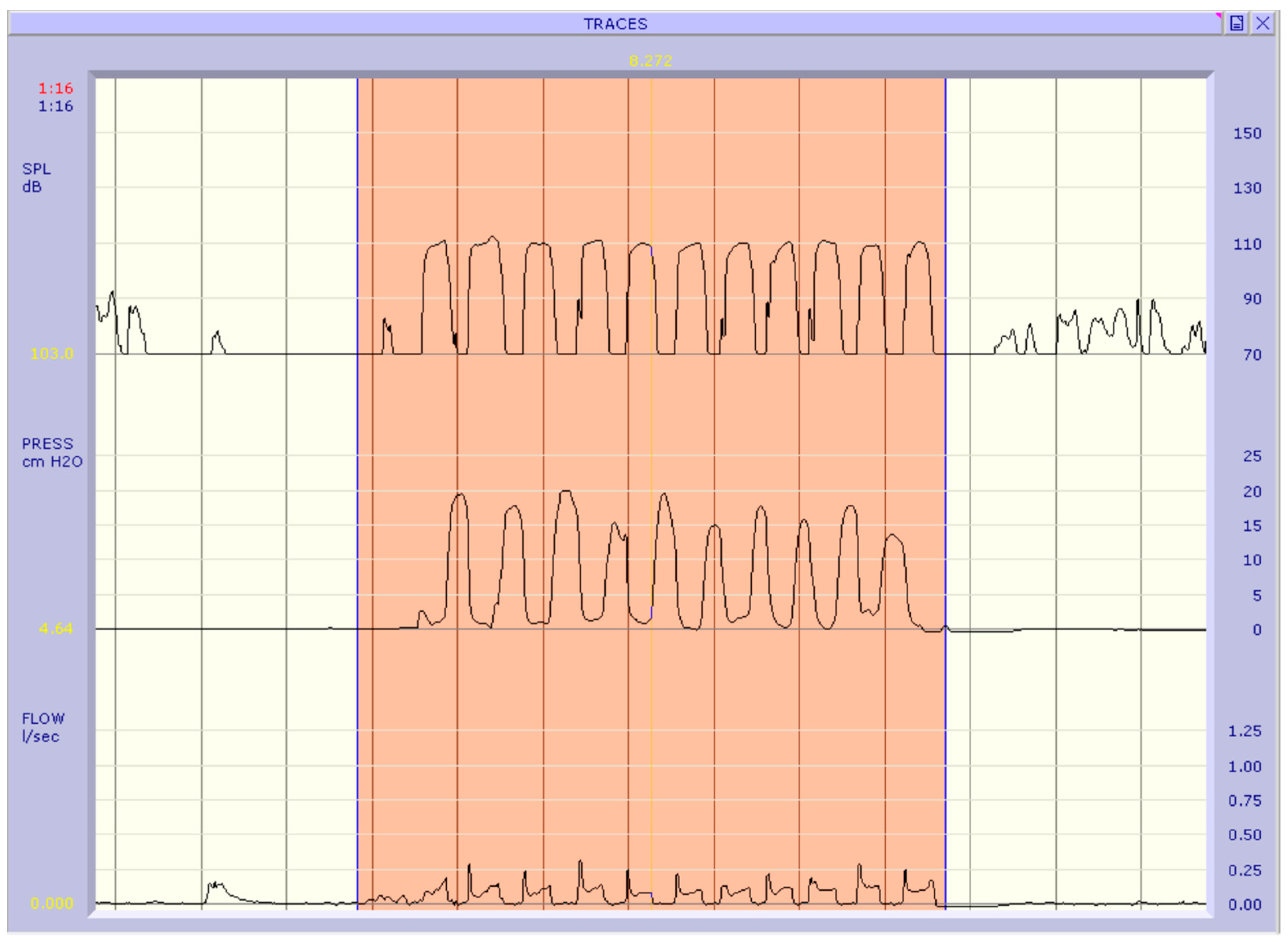
- Objective Aerophonic Examination:
- -
- the phonatory flow rate index (Phonatory Flow Rate, phonatory flow rate (PFR) index in l/s) represents the volume of airflow per unit of time during vocalization; and
- -
2.2. Statistical Analysis
3. Results
- (1)
- Breathing Modalities:
- -
- Approximately 14 (70%) patients preferred mouth breathing.
- -
- A total of 6 (30%) patients exhibited mixed respiratory patterns, using both the oral and nasal channels.
- -
- There was no evidence of a preferential nasal respiratory pattern in any of the cases.
- (2)
- Respiratory Difficulties:
- -
- A total of 16 (80%) cases reported allergies (to pollen, dust, mites, etc.).
- -
- All subjects displayed nocturnal snoring, whereas 50% of the cases had obstructive apnea.
- (3)
- Oral Posture at Rest:
- -
- In total, 12 (60%) patients demonstrated an open oral posture at rest.
- -
- Moreover, 8 (40%) patients showed a semi-closed oral posture at rest.
- -
- At rest, none of the cases presented a correct oral posture (a closed posture indicative of healthy respiratory mode).
- -
- A total of 17 (85%) patients reported subjective symptoms closely related to phonatory activity.
- -
- A total of 14 (82.35%) patients demonstrated an actual change in their voice.
- -
- Although 3 (17.64%) patients complained of subjective phonatory activity disorders, they did not exhibit any vocal disorders.
- -
- The 3 patients who did not report subjective symptoms did not present dysphonia or vocal function changes.The subjective symptoms that patients reported most frequently were as follows:
- vocal fatigue: 62%;
- need to clear the throat: 50%; and
- oro-pharyngeal burning sensation: 75%
- The pitch level of all individuals was found to be regular and appropriate for their gender and age.
- The vocal intensity was as follows:
- -
- normal in 8 (40%) cases;
- -
- high in 10 (50%) cases; and
- -
- inconsistent in 2 (10%) cases.
- The vocal timbre was as follows:
- -
- personal (unique to the individual) in 4 (20%) cases;
- -
- hoarse in 13 (65%) cases; and
- -
- husky in 3 (15%) cases.
- The phonetic onset was as follows:
- -
- correct in 4 (20%) cases;
- -
- harsh in 13 (65%) cases; and
- -
- inconsistent in 3 (15%) cases.
- The vocal stability was as follows:
- -
- Regular in 8 (40%) cases;
- -
- Inconsistent in 12 (60%) cases.
- The duration of phonation was as follows:
- -
- regular in 8 (40%) cases; and
- -
- inconsistent (reduced) in 12 (60%) cases.
- The respiratory pattern during phonation was as follows:
- -
- chest-apical in 9 (45%) cases;
- -
- mixed in 11 (55%) cases; and
- -
- none of the patients exclusively demonstrated the costal-diaphragmatic respiratory mechanism.
- -
- Devoicing of the occlusive phonemes /b/, /d/, /g/, and sometimes also of the fricative phoneme /z/.
- -
- Interdental sigmatism, meaning the production of the fricative phoneme /s/ with the tip of the tongue placed between the upper and lower incisors.
- -
- Frequent interdentalizations of the alveolar phonemes /s/, /z/, /t/, /d/, /l/, /r/.
- -
- Rotacism, the production of the /r/ phoneme without the proper periodic vibration of the tip of the tongue.
- -
- Structure simplifications, i.e., modifications in the syllabic structure of words, such as reductions in consonant clusters, were also found in some patients.
- -
- the phonatory flow was lower in 16 (80%) patients, while its higher values were observed in the remaining four (20%) patients; and
- -
- the subglottic pressure was higher in 17 (85%) patients, while it was lower in the remaining three (15%) patients than in the rest of the examined group.
Normality Test
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mozzanica, F.; Ginocchio, D.; Barillari, R.; Barozzi, S.; Maruzzi, P.; Ottaviani, F.; Schindler, A. Prevalence and Voice Characteristics of Laryngeal Pathology in an Italian Voice Therapy-seeking Population. J. Voice 2016, 30, 774.e13–774.e21. [Google Scholar] [CrossRef]
- Cardoso, R.; Meneses, R.F.; Lumini-Oliveira, J.; Pestana, P.; Guimarães, B. Associations between Teachers’ Posture, Muscle Tension and Voice Complaints. J. Voice 2021, 35, 933.e23–933.e31. [Google Scholar] [CrossRef] [PubMed]
- Rickert, S.M.; O’Cathain, E. Pediatric Voice. Pediatr. Clin. N. Am. 2022, 69, 329–347. [Google Scholar] [CrossRef] [PubMed]
- Cai, Y.; Gu, W.; Wang, J. Evaluation of postoperative pain after tonsil-sparing styloidectomy. Eur. Arch. Otorhinolaryngol. 2020, 277, 2011–2015. [Google Scholar] [CrossRef] [PubMed]
- Yoon, A.; Abdelwahab, M.; Bockow, R.; Vakili, A.; Lovell, K.; Chang, I.; Ganguly, R.; Liu, S.Y.; Kushida, C.; Hong, C. Impact of rapid palatal expansion on the size of adenoids and tonsils in children. Sleep Med. 2022, 92, 96–102. [Google Scholar] [CrossRef]
- Mitchell, R.B.; Archer, S.M.; Ishman, S.L.; Rosenfeld, R.M.; Coles, S.; Finestone, S.A.; Friedman, N.R.; Giordano, T.; Hildrew, D.M.; Kim, T.W.; et al. Clinical Practice Guideline: Tonsillectomy in Children (Update)-Executive Summary. Otolaryngol. Head Neck Surg. 2019, 160, 187–205. [Google Scholar] [CrossRef]
- Motta, S.; Galli, I.; Di Rienzo, L. Aerodynamic findings in esophageal voice. Arch. Otolaryngol. Head Neck Surg. 2001, 127, 700–704. [Google Scholar] [CrossRef]
- Traser, L.; Burk, F.; Özen, A.C.; Burdumy, M.; Bock, M.; Blaser, D.; Richter, B.; Echternach, M. Respiratory kinematics and the regulation of subglottic pressure for phonation of pitch jumps—A dynamic MRI study. PLoS ONE 2020, 15, e0244539. [Google Scholar] [CrossRef]
- Lamb, J.R.; Schultz, S.A.; Scholp, A.J.; Wendel, E.R.; Jiang, J.J. Retest Reliability for Complete Airway Interruption Systems of Aerodynamic Measurement. J. Voice 2022, 36, 27–33. [Google Scholar] [CrossRef]
- Salami, A.; Jankowska, B.; Dellepiane, M.; Crippa, B.; Mora, R. The impact of tonsillectomy with or without adenoidectomy on speech and voice. Int. J. Pediatr. Otorhinolaryngol. 2008, 72, 1377–1384. [Google Scholar] [CrossRef]
- Mora, R.; Crippa, B.; Dellepiane, M.; Jankowska, B. Effects of adenotonsillectomy on speech spectrum in children. Int. J. Pediatr. Otorhinolaryngol. 2007, 71, 1299–1304. [Google Scholar] [CrossRef] [PubMed]
- Maryn, Y.; Van Lierde, K.; De Bodt, M.; Van Cauwenberge, P. The effects of adenoidectomy and tonsillectomy on speech and nasal resonance. Folia Phoniatr. Logop. 2004, 56, 182–191. [Google Scholar] [CrossRef] [PubMed]
- Finkelstein, Y.; Nachmani, A.; Ophir, D. The functional role of the tonsils in speech. Arch. Otolaryngol. Head Neck Surg. 1994, 120, 846–851. [Google Scholar] [CrossRef] [PubMed]
- Inja, R.R.; Paul, R.R.; Varghese, L.; Santosh, S.; Sebastian, T.; Mathews, S.S. Voice Change Following Adenotonsillectomy in Pediatric Population: Myth or Reality?-A Pilot Study. Indian J. Otolaryngol. Head Neck Surg. 2019, 71 (Suppl. S1), 574–579. [Google Scholar] [CrossRef] [PubMed]
- Paulson, L.M.; MacArthur, C.J.; Beaulieu, K.B.; Brockman, J.H.; Milczuk, H.A. Speech Outcomes after Tonsillectomy in Patients with Known Velopharyngeal Insufficiency. Int. J. Otolaryngol. 2012, 2012, 912767. [Google Scholar] [CrossRef]
- Yang, J.J.; Cheng, L.Y.; Xu, W. Study on changes of voice characteristics after adenotonsillectomy or adenoidectomy in children. Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi 2021, 56, 724–729. (In Chinese) [Google Scholar] [CrossRef]
- Neagos, A.; Dumitru, M.; Neagos, C.M.; Mitroi, M.; Vrinceanu, D. Correlations between Morphology, the Functional Properties of Upper Airways, and the Severity of Sleep Apnea. J. Clin. Med. 2022, 11, 5347. [Google Scholar] [CrossRef]
- Lundeborg, I.; Hultcrantz, E.; Ericsson, E.; McAllister, A. Acoustic and Perceptual Aspects of Vocal Function in Children with Adenotonsillar Hypertrophy—Effects of Surgery. J. Voice 2012, 26, 480–487. [Google Scholar] [CrossRef]
- Farronato, M.; Lanteri, V.; Fama, A.; Maspero, C. Correlation between Malocclusion and Allergic Rhinitis in Pediatric Patients: A Systematic Review. Children 2020, 7, 260. [Google Scholar] [CrossRef]
- Lofstrand-Tidestrom, B.; Hultcrantz, E. The development of snoring and sleep related breathing distress from 4 to 6 years in a cohort of Swedish children. Int. J. Pediatr. Otorhinolaryngol. 2007, 71, 1025–1033. [Google Scholar] [CrossRef]
- Kummer, A.W.; Billmire, D.A.; Myer, C.M., 3rd. Hypertrophic tonsils: The effect on resonance and velopharyngeal closure. Otolaryngol. Head Neck Surg. 1996, 115, 319–323. [Google Scholar] [CrossRef]
- Hori, Y.; Koike, Y.; Ohyama, G.; Otsu, S.Y.; Abe, K. Effects of tonsillectomy on articulation. Acta Otolaryngol. Suppl. 1996, 523, 248–251. [Google Scholar] [PubMed]
- Andreassen, M.L.; Leeper, H.A.; Macrae, D.L.; Nicholson, I.R. Aerodynamic, acoustic, and perceptual changes following adenoidectomy. Cleft Palate-Craniofacial J. 1994, 31, 263–270. [Google Scholar] [CrossRef] [PubMed]
- Zalzal, H.G.; Coutras, S. Palatine Tonsil Stenting of the Airway as Determined by Drug-Induced Sleep Endoscopy. Case Rep. Otolaryngol. 2018, 2018, 2614143. [Google Scholar] [CrossRef] [PubMed]
- Bilgiç, F.; Damlar, I.; Sürmelioğlu, Ö.; Sözer, Ö.A.; Tatlı, U. Relationship between voice function and skeletal effects of rapid maxillary expansion. Angle Orthod. 2018, 88, 202–207. [Google Scholar] [CrossRef]
- Mesolella, M.; Allosso, S.; Coronella, V.; Massimilla, E.A.; Mansi, N.; Motta, G.; Salerno, G.; Motta, G. Extracapsular Tonsillectomy versus Intracapsular Tonsillotomy in Paediatric Patients with OSAS. J. Pers. Med. 2023, 13, 806. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Mean | Standard Deviation | Count | Column N % | ||
|---|---|---|---|---|---|
| Age | 6.75 | 2.53 | |||
| Pharyngo-tonsillitis (Episodes per year) | 6.75 | 1.52 | |||
| Sex | F | 10 | 50% | ||
| M | 10 | 50% | |||
| Breathing Modalities | Mixed | 6 | 30% | ||
| Mouth breathing | 14 | 70% | |||
| Allergies | No | 4 | 20% | ||
| Yes | 16 | 80% | |||
| Sleep Disorders | nocturnal snoring, | 10 | 50% | ||
| nocturnal snoring and obstructive apnea | 10 | 50% | |||
| Oral Posture at Rest | Open | 12 | 60% | ||
| Semi-closed | 8 | 40% | |||
| Subjective symptoms | No | 3 | 15% | ||
| Yes | 17 | 85% | |||
| Dysphonia | No | 6 | 30% | ||
| Yes | 14 | 70% | |||
| Vocal intensity | High | 10 | 50% | ||
| Inconsistent | 2 | 10% | |||
| Normal | 8 | 40% | |||
| Vocal timbre | Personal | 4 | 20% | ||
| Hoarse | 13 | 65% | |||
| Husky | 3 | 15% | |||
| Phonetic onset | Correct | 4 | 20% | ||
| Harsh | 13 | 65% | |||
| Inconsistent | 3 | 15% | |||
| Vocal stability | Inconsistent | 12 | 60% | ||
| Regular | 8 | 40% | |||
| Duration of phonation | Inconsistent | 12 | 60% | ||
| Regular | 8 | 40% | |||
| Respiratory pattern | Mixed | 11 | 55% | ||
| Chest—Apical | 9 | 45% | |||
| Vocal Examination | Negative | 6 | 30% | ||
| Positive | 14 | 70% | |||
| Speech articulation problems | No | 4 | 20% | ||
| Yes | 16 | 80% | |||
| Disarticulation | No | 4 | 20% | ||
| Yes | 16 | 80% | |||
| Sigmacism | No | 7 | 35% | ||
| Yes | 13 | 65% | |||
| Rotacism | No | 11 | 55% | ||
| Yes | 9 | 45% | |||
| Interdentalizations | No | 7 | 35% | ||
| Yes | 13 | 65% | |||
| Reductions in consonant clusters | No | 8 | 40% | ||
| Yes | 12 | 60% | |||
| Fonatory Flow Rate | Higl | 4 | 20% | ||
| Low | 16 | 80% | |||
| Subglottal Pressure | High | 17 | 85% | ||
| Low | 3 | 15% | |||
| Numerical Fonatory Flow | 0.10 | 0.03 | |||
| Numerical Subglottal Flow | 14.95 | 2.53 | |||
| Shapiro-Wilk | Statistic | df | Sig. |
|---|---|---|---|
| Age | 0.874 | 60 | <0.001 |
| Numerical Fonatory Flow | 0.891 | 60 | <0.001 |
| Numerical Subglottal Flow | 0.920 | 60 | <0.001 |
| Shapiro-Wilk | ||||
|---|---|---|---|---|
| Statistic | df | Sig. | ||
| GROUP A—POST SURGERY | Age | 0.882 | 20 | 0.019 |
| Numerical Fonatory Flow | 0.960 | 20 | 0.546 | |
| Numerical Subglottal Flow | 0.878 | 20 | 0.017 | |
| GROUP A—PRE SURGERY | Age | 0.882 | 20 | 0.019 |
| Numerical Fonatory Flow | 0.729 | 20 | <0.001 | |
| Numerical Subglottal Flow | 0.895 | 20 | 0.033 | |
| GROUP B | Age | 0.878 | 20 | 0.016 |
| Numerical Fonatory Flow | 0.753 | 20 | <0.001 | |
| Numerical Subglottal Flow | 0.914 | 20 | 0.076 | |
| Group A—Pre Surgery | Group B | |||||||
|---|---|---|---|---|---|---|---|---|
| Median | Count | Column N % | Median | Count | Column N % | p-Value | ||
| Age | 6.50 | 6.00 | 0.758 b | |||||
| Sex | F | 10.00 | 50.00 | 10.00 | 50.00 | 1.000 a | ||
| M | 10.00 | 50.00 | 10.00 | 50.00 | ||||
| Breathing Modalities | Mixed | 6.00 | 30.00 | 9.00 | 45.00 | 0.327 a | ||
| Mouth breathing | 14.00 | 70.00 | 11.00 | 55.00 | ||||
| Oral Posture at Rest | Open | 12.00 | 60.00 | 11.00 | 55.00 | 0.749 a | ||
| Semi-closed | 8.00 | 40.00 | 9.00 | 45.00 | ||||
| Subjective symptoms | No | 3.00 | 15.00 | 5.00 | 25.00 | 0.429 a | ||
| Yes | 17.00 | 85.00 | 15.00 | 75.00 | ||||
| Vocal intensity | High | 10.00 | 50.00 | 10.00 | 50.00 | 0.372 a | ||
| Inconsistent | 2.00 | 10.00 | 5.00 | 25.00 | ||||
| Normal | 8.00 | 40.00 | 5.00 | 25.00 | ||||
| Vocal timbre | Personal | 4.00 | 20.00 | 9.00 | 45.00 | 0.082 a | ||
| Hoarse | 13.00 | 65.00 | 6.00 | 30.00 | ||||
| Husky | 3.00 | 15.00 | 5.00 | 25.00 | ||||
| Phonetic onset | Correct | 4.00 | 20.00 | 5.00 | 25.00 | 0.234 a | ||
| Harsh | 13.00 | 65.00 | 8.00 | 40.00 | ||||
| Inconsistent | 3.00 | 15.00 | 7.00 | 35.00 | ||||
| Interdentalizations | No | 7.00 | 35.00 | 5.00 | 25.00 | 0.490 a | ||
| Yes | 13.00 | 65.00 | 15.00 | 75.00 | ||||
| Fonatory Flow Rate | 0.09 | 0.08 | 0.253 b | |||||
| Subglottal Pressure | 15.77 | 16.07 | 0.678 b | |||||
| Group A—Post-Surgery | Group A—Pre-Surgery | |||||||
|---|---|---|---|---|---|---|---|---|
| Median | Count | Column N % | Median | Count | Column N % | p-Value | ||
| Breathing Modalities | Mixed | 2.00 | 10.00 | 6.00 | 30.00 | <0.001 a | ||
| Nasal breathing | 18.00 | 90.00 | 0.00 | 0.00 | ||||
| Mouth breathing | 0.00 | 0.00 | 14.00 | 70.00 | ||||
| Oral Posture at Rest | Open | 0.00 | 0.00 | 12.00 | 60.00 | |||
| Close | 18.00 | 90.00 | 0.00 | 0.00 | <0.001 a | |||
| Oral | 2.00 | 10.00 | 0.00 | 0.00 | ||||
| Semi-closed | 0.00 | 0.00 | 8.00 | 40.00 | ||||
| Subjective symptoms | No | 18.00 | 90.00 | 3.00 | 15.00 | <0.001 a | ||
| Yes | 0.00 | 0.00 | 17.00 | 85.00 | ||||
| Vocal intensity | High | 3.00 | 15.00 | 10.00 | 50.00 | 0.011 a | ||
| Inconsistent | 0.00 | 0.00 | 2.00 | 10.00 | ||||
| Normal | 17.00 | 85.00 | 8.00 | 40.00 | ||||
| Vocal timbre | Personal | 15.00 | 75.00 | 4.00 | 20.00 | 0.002 a | ||
| Hoarse | 5.00 | 25.00 | 13.00 | 65.00 | ||||
| Husky | .00 | 0.00 | 3.00 | 15.00 | ||||
| Phonetic onset | Correct | 16.00 | 80.00 | 4.00 | 20.00 | <0.001 a | ||
| Harsh | 4.00 | 20.00 | 13.00 | 65.00 | ||||
| Inconsistent | 0.00 | 0.00 | 3.00 | 15.00 | ||||
| Interdentalizations | No | 20.00 | 100.00 | 7.00 | 35.00 | <0.001 a | ||
| Yes | 0.00 | 0.00 | 13.00 | 65.00 | ||||
| Fonatory Flow Rate | 0.15 | 0.09 | <0.01 b | |||||
| Subglottal Pressure | 11.00 | 15.77 | <0.001 b | |||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mesolella, M.; Motta, G.; Allosso, S.; Motta, G. Effects of Adenotonsillectomy on Vocal Function. J. Pers. Med. 2023, 13, 1002. https://doi.org/10.3390/jpm13061002
Mesolella M, Motta G, Allosso S, Motta G. Effects of Adenotonsillectomy on Vocal Function. Journal of Personalized Medicine. 2023; 13(6):1002. https://doi.org/10.3390/jpm13061002
Chicago/Turabian StyleMesolella, Massimo, Giovanni Motta, Salvatore Allosso, and Gaetano Motta. 2023. "Effects of Adenotonsillectomy on Vocal Function" Journal of Personalized Medicine 13, no. 6: 1002. https://doi.org/10.3390/jpm13061002
APA StyleMesolella, M., Motta, G., Allosso, S., & Motta, G. (2023). Effects of Adenotonsillectomy on Vocal Function. Journal of Personalized Medicine, 13(6), 1002. https://doi.org/10.3390/jpm13061002