
Personalized Medicine of Omega-3 Fatty Acids in Depression Treatment in Obese and Metabolically Dysregulated Patients

 , ,
, ,  , , ,
, , ,
Abstract
1. Introduction
2. MDD, Stress, and Neuropsychoimmunity
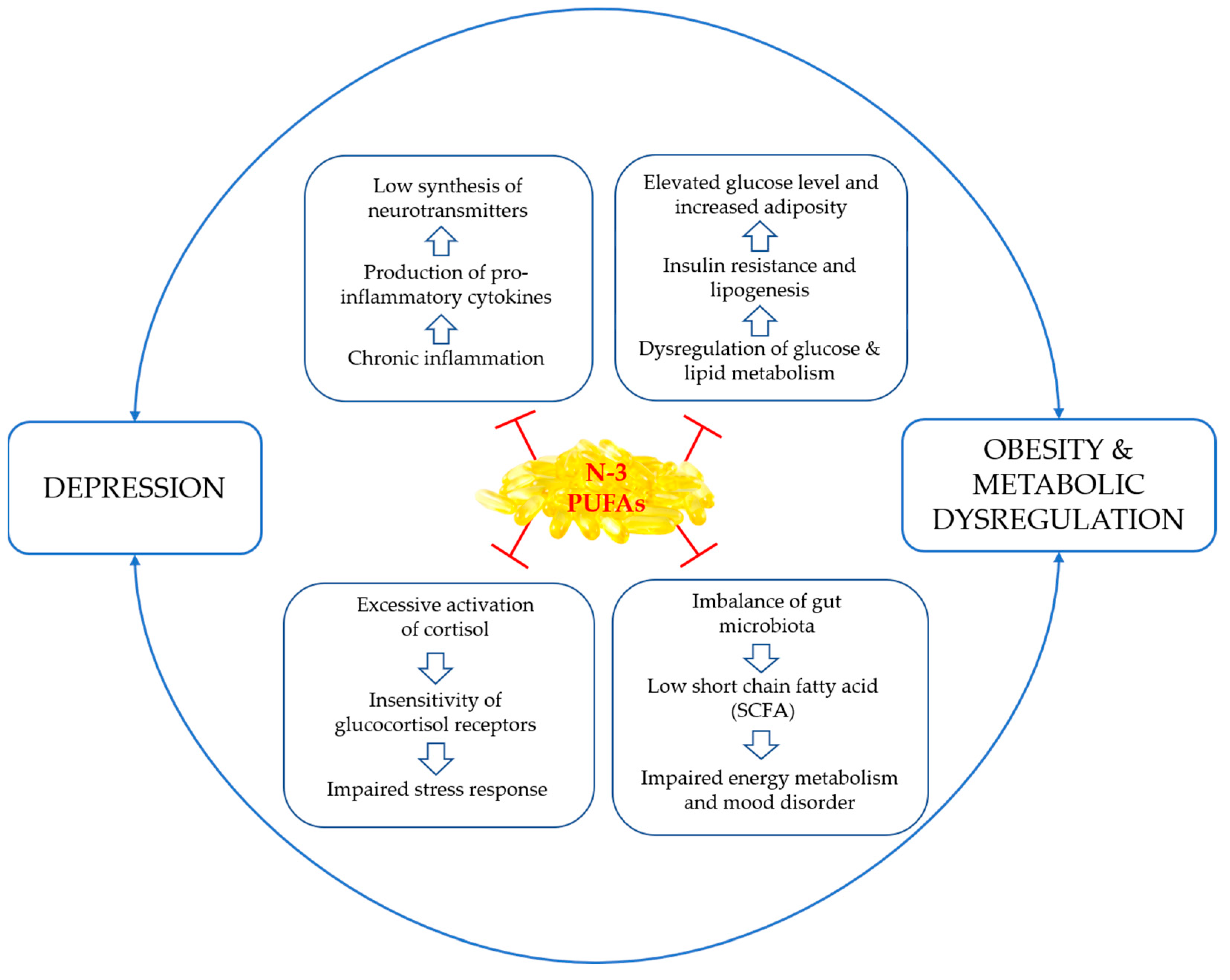
3. The Interplay between Depression, Obesity, and Metabolic Dysregulation
4. Personalized Omega-3 Polyunsaturated Fatty Acids (n-3 PUFAs) Intervention in Depression
5. Omega-3 Polyunsaturated Fatty Acids (n-3 PUFAs) for Depression Treatment in Obese and Metabolically Dysregulated Patients
6. Future Perspective
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. Depression Fact Sheet [Fact Sheet]. Available online: https://www.who.int/news-room/fact-sheets/detail/depression (accessed on 12 March 2023).
- COVID-19 Mental Disorders Collaborators. Global prevalence and burden of depressive and anxiety disorders in 204 countries and territories in 2020 due to the COVID-19 pandemic. Lancet 2021, 398, 1700–1712. [Google Scholar] [CrossRef]
- Zisook, S.; Lesser, I.; Stewart, J.W.; Wisniewski, S.R.; Balasubramani, G.K.; Fava, M.; Gilmer, W.S.; Dresselhaus, T.R.; Thase, M.E.; Nierenberg, A.A.; et al. Effect of Age at Onset on the Course of Major Depressive Disorder. Am. J. Psychiatry 2007, 164, 1539–1546. [Google Scholar] [CrossRef]
- Picco, L.; Subramaniam, M.; Abdin, E.; Vaingankar, J.A.; Chong, S.A. Gender differences in major depressive disorder: Findings from the Singapore Mental Health Study. Singap. Med. J. 2017, 58, 649–655. [Google Scholar] [CrossRef]
- Mehdi, S.; Manohar, K.; Shariff, A.; Kinattingal, N.; Wani, S.U.D.; Alshehri, S.; Imam, M.T.; Shakeel, F.; Krishna, K.L. Omega-3 Fatty Acids Supplementation in the Treatment of Depression: An Observational Study. J. Pers. Med. 2023, 13, 224. [Google Scholar] [CrossRef]
- Twenge, J.M. Increases in Depression, Self-Harm, and Suicide Among U.S. Adolescents After 2012 and Links to Technology Use: Possible Mechanisms. Psychiatr. Res. Clin. Pract. 2020, 2, 19–25. [Google Scholar] [CrossRef]
- Hammer-Helmich, L.; Haro, J.M.; Jönsson, B.; Tanguy Melac, A.; Di Nicola, S.; Chollet, J.; Milea, D.; Rive, B.; Saragoussi, D. Functional impairment in patients with major depressive disorder: The 2-year PERFORM study. Neuropsychiatr. Dis. Treat. 2018, 14, 239–249. [Google Scholar] [CrossRef]
- Greenberg, P.E.; Fournier, A.-A.; Sisitsky, T.; Simes, M.; Berman, R.; Koenigsberg, S.H.; Kessler, R.C. The Economic Burden of Adults with Major Depressive Disorder in the United States (2010 and 2018). PharmacoEconomics 2021, 39, 653–665. [Google Scholar] [CrossRef]
- Christensen, M.C.; Wong, C.M.J.; Baune, B.T. Symptoms of Major Depressive Disorder and Their Impact on Psychosocial Functioning in the Different Phases of the Disease: Do the Perspectives of Patients and Healthcare Providers Differ? Front. Psychiatry 2020, 11, 280. [Google Scholar] [CrossRef]
- Culpepper, L. Understanding the burden of depression. J. Clin. Psychiatry 2011, 72, e19. [Google Scholar] [CrossRef]
- Fulton, S.; Décarie-Spain, L.; Fioramonti, X.; Guiard, B.; Nakajima, S. The menace of obesity to depression and anxiety prevalence. Trends Endocrinol. Metab. 2022, 33, 18–35. [Google Scholar] [CrossRef]
- Luppino, F.S.; de Wit, L.M.; Bouvy, P.F.; Stijnen, T.; Cuijpers, P.; Penninx, B.W.; Zitman, F.G. Overweight, obesity, and depression: A systematic review and meta-analysis of longitudinal studies. Arch. Gen. Psychiatry 2010, 67, 220–229. [Google Scholar] [CrossRef]
- Pan, A.; Keum, N.; Okereke, O.I.; Sun, Q.; Kivimaki, M.; Rubin, R.R.; Hu, F.B. Bidirectional association between depression and metabolic syndrome: A systematic review and meta-analysis of epidemiological studies. Diabetes Care 2012, 35, 1171–1180. [Google Scholar] [CrossRef] [PubMed]
- Penninx, B.W.J.H.; Lange, S.M.M. Metabolic syndrome in psychiatric patients: Overview, mechanisms, and implications. Dialogues Clin. Neurosci. 2018, 20, 63–73. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Cheng, Y.; Li, Y.; Han, J.; Yuan, Z.; Li, Q.; Zhong, F.; Wu, Y.; Fan, X.; Bo, T.; et al. The Relationship Between Obesity and Depression Is Partly Dependent on Metabolic Health Status: A Nationwide Inpatient Sample Database Study. Front. Endocrinol. 2022, 13, 880230. [Google Scholar] [CrossRef] [PubMed]
- Patsalos, O.; Keeler, J.; Schmidt, U.; Penninx, B.W.J.H.; Young, A.H.; Himmerich, H. Diet, Obesity, and Depression: A Systematic Review. J. Pers. Med. 2021, 11, 176. [Google Scholar] [CrossRef]
- Milaneschi, Y.; Simmons, W.K.; van Rossum, E.F.C.; Penninx, B.W. Depression and obesity: Evidence of shared biological mechanisms. Mol. Psychiatry 2019, 24, 18–33. [Google Scholar] [CrossRef]
- Mannan, M.; Mamun, A.; Doi, S.; Clavarino, A. Prospective Associations between Depression and Obesity for Adolescent Males and Females- A Systematic Review and Meta-Analysis of Longitudinal Studies. PLoS ONE 2016, 11, e0157240. [Google Scholar] [CrossRef]
- Nigatu, Y.T.; Reijneveld, S.A.; de Jonge, P.; van Rossum, E.; Bültmann, U. The Combined Effects of Obesity, Abdominal Obesity and Major Depression/Anxiety on Health-Related Quality of Life: The LifeLines Cohort Study. PLoS ONE 2016, 11, e0148871. [Google Scholar] [CrossRef]
- Nishi, D.; Su, K.P.; Usuda, K.; Pei-Chen Chang, J.; Chiang, Y.J.; Chen, H.T.; Chien, Y.C.; Guu, T.W.; Okazaki, E.; Hamazaki, K.; et al. The Efficacy of Omega-3 Fatty Acids for Depressive Symptoms among Pregnant Women in Japan and Taiwan: A Randomized, Double-Blind, Placebo-Controlled Trial (SYNCHRO; NCT01948596). Psychother. Psychosom. 2019, 88, 122–124. [Google Scholar] [CrossRef]
- Nishi, D.; Su, K.-P.; Usuda, K.; Chiang, Y.-J.J.; Guu, T.-W.; Hamazaki, K.; Nakaya, N.; Sone, T.; Sano, Y.; Ito, H.; et al. Omega-3 fatty acid supplementation for expectant mothers with depressive symptoms in Japan and Taiwan: An open-label trial. Psychiatry Clin. Neurosci. 2016, 70, 253–254. [Google Scholar] [CrossRef]
- Su, K.P.; Huang, S.Y.; Chiu, T.H.; Huang, K.C.; Huang, C.L.; Chang, H.C.; Pariante, C.M. Omega-3 fatty acids for major depressive disorder during pregnancy: Results from a randomized, double-blind, placebo-controlled trial. J. Clin. Psychiatry 2008, 69, 644–651. [Google Scholar] [CrossRef] [PubMed]
- Guu, T.W.; Mischoulon, D.; Sarris, J.; Hibbeln, J.; McNamara, R.K.; Hamazaki, K.; Freeman, M.P.; Maes, M.; Matsuoka, Y.J.; Belmaker, R.H.; et al. International Society for Nutritional Psychiatry Research Practice Guidelines for Omega-3 Fatty Acids in the Treatment of Major Depressive Disorder. Psychother. Psychosom. 2019, 88, 263–273. [Google Scholar] [CrossRef] [PubMed]
- Nemets, H.; Nemets, B.; Apter, A.; Bracha, Z.; Belmaker, R.H. Omega-3 treatment of childhood depression: A controlled, double-blind pilot study. Am. J. Psychiatry 2006, 163, 1098–1100. [Google Scholar] [CrossRef] [PubMed]
- Rondanelli, M.; Giacosa, A.; Opizzi, A.; Pelucchi, C.; La Vecchia, C.; Montorfano, G.; Negroni, M.; Berra, B.; Politi, P.; Rizzo, A.M. Effect of omega-3 fatty acids supplementation on depressive symptoms and on health-related quality of life in the treatment of elderly women with depression: A double-blind, placebo-controlled, randomized clinical trial. J. Am. Coll. Nutr. 2010, 29, 55–64. [Google Scholar] [CrossRef]
- Mischoulon, D.; Dunlop, B.W.; Kinkead, B.; Schettler, P.J.; Lamon-Fava, S.; Rakofsky, J.J.; Nierenberg, A.A.; Clain, A.J.; Mletzko Crowe, T.; Wong, A.; et al. Omega-3 Fatty Acids for Major Depressive Disorder with High Inflammation: A Randomized Dose-Finding Clinical Trial. J. Clin. Psychiatry 2022, 83, 42432. [Google Scholar] [CrossRef] [PubMed]
- Rapaport, M.H.; Nierenberg, A.A.; Schettler, P.J.; Kinkead, B.; Cardoos, A.; Walker, R.; Mischoulon, D. Inflammation as a predictive biomarker for response to omega-3 fatty acids in major depressive disorder: A proof-of-concept study. Mol. Psychiatry 2016, 21, 71–79. [Google Scholar] [CrossRef]
- Khalili, L.; Valdes-Ramos, R.; Harbige, L.S. Effect of n-3 (Omega-3) Polyunsaturated Fatty Acid Supplementation on Metabolic and Inflammatory Biomarkers and Body Weight in Patients with Type 2 Diabetes Mellitus: A Systematic Review and Meta-Analysis of RCTs. Metabolites 2021, 11, 742. [Google Scholar] [CrossRef]
- Ferrari, A.J.; Charlson, F.J.; Norman, R.E.; Patten, S.B.; Freedman, G.; Murray, C.J.L.; Vos, T.; Whiteford, H.A. Burden of Depressive Disorders by Country, Sex, Age, and Year: Findings from the Global Burden of Disease Study 2010. PLoS Med. 2013, 10, e1001547. [Google Scholar] [CrossRef]
- Mikulska, J.; Juszczyk, G.; Gawrońska-Grzywacz, M.; Herbet, M. HPA Axis in the Pathomechanism of Depression and Schizophrenia: New Therapeutic Strategies Based on Its Participation. Brain Sci. 2021, 11, 1298. [Google Scholar] [CrossRef]
- Nandam, L.S.; Brazel, M.; Zhou, M.; Jhaveri, D.J. Cortisol and Major Depressive Disorder-Translating Findings From Humans to Animal Models and Back. Front. Psychiatry 2019, 10, 974. [Google Scholar] [CrossRef]
- Liu, W.; Liu, J.; Xia, J.; Xue, X.; Wang, H.; Qi, Z.; Ji, L. Leptin receptor knockout-induced depression-like behaviors and attenuated antidepressant effects of exercise are associated with STAT3/SOCS3 signaling. Brain Behav. Immun. 2017, 61, 297–305. [Google Scholar] [CrossRef] [PubMed]
- Liao, G.-Y.; An, J.J.; Gharami, K.; Waterhouse, E.G.; Vanevski, F.; Jones, K.R.; Xu, B. Dendritically targeted Bdnf mRNA is essential for energy balance and response to leptin. Nat. Med. 2012, 18, 564–571. [Google Scholar] [CrossRef]
- Cao, B.; Chen, Y.; Brietzke, E.; Cha, D.; Shaukat, A.; Pan, Z.; Park, C.; Subramaniapillai, M.; Zuckerman, H.; Grant, K.; et al. Leptin and adiponectin levels in major depressive disorder: A systematic review and meta-analysis. J. Affect. Disord. 2018, 238, 101–110. [Google Scholar] [CrossRef]
- Zhang, D.; Guo, M.; Zhang, W.; Lu, X.Y. Adiponectin stimulates proliferation of adult hippocampal neural stem/progenitor cells through activation of p38 mitogen-activated protein kinase (p38MAPK)/glycogen synthase kinase 3β (GSK-3β)/β-catenin signaling cascade. J. Biol. Chem. 2011, 286, 44913–44920. [Google Scholar] [CrossRef]
- Zhang, D.; Wang, X.; Lu, X.Y. Adiponectin Exerts Neurotrophic Effects on Dendritic Arborization, Spinogenesis, and Neurogenesis of the Dentate Gyrus of Male Mice. Endocrinology 2016, 157, 2853–2869. [Google Scholar] [CrossRef] [PubMed]
- Sun, F.; Lei, Y.; You, J.; Li, C.; Sun, L.; Garza, J.; Zhang, D.; Guo, M.; Scherer, P.E.; Lodge, D.; et al. Adiponectin modulates ventral tegmental area dopamine neuron activity and anxiety-related behavior through AdipoR1. Mol. Psychiatry 2019, 24, 126–144. [Google Scholar] [CrossRef] [PubMed]
- Formolo, D.A.; Lee, T.H.-Y.; Yau, S.-Y. Increasing Adiponergic System Activity as a Potential Treatment for Depressive Disorders. Mol. Neurobiol. 2019, 56, 7966–7976. [Google Scholar] [CrossRef] [PubMed]
- Nicolas, S.; Debayle, D.; Béchade, C.; Maroteaux, L.; Gay, A.S.; Bayer, P.; Heurteaux, C.; Guyon, A.; Chabry, J. Adiporon, an adiponectin receptor agonist acts as an antidepressant and metabolic regulator in a mouse model of depression. Transl. Psychiatry 2018, 8, 159. [Google Scholar] [CrossRef]
- Lindqvist, D.; Dhabhar, F.S.; James, S.J.; Hough, C.M.; Jain, F.A.; Bersani, F.S.; Reus, V.I.; Verhoeven, J.E.; Epel, E.S.; Mahan, L.; et al. Oxidative stress, inflammation and treatment response in major depression. Psychoneuroendocrinology 2017, 76, 197–205. [Google Scholar] [CrossRef]
- Gałecka, M.; Bliźniewska-Kowalska, K.; Orzechowska, A.; Szemraj, J.; Maes, M.; Berk, M.; Su, K.-P.; Gałecki, P. Inflammatory versus Anti-Inflammatory Profiles in Major Depressive Disorders—The Role of IL-17, IL-21, IL-23, IL-35 and Foxp3. J. Pers. Med. 2021, 11, 66. [Google Scholar] [CrossRef]
- Alavi, M.; Grebely, J.; Matthews, G.V.; Petoumenos, K.; Yeung, B.; Day, C.; Lloyd, A.R.; Van Beek, I.; Kaldor, J.M.; Hellard, M.; et al. Effect of pegylated interferon-α-2a treatment on mental health during recent hepatitis C virus infection. J. Gastroenterol. Hepatol. 2012, 27, 957–965. [Google Scholar] [CrossRef] [PubMed]
- Raison, C.L.; Demetrashvili, M.; Capuron, L.; Miller, A.H. Neuropsychiatric adverse effects of interferon-alpha: Recognition and management. CNS Drugs 2005, 19, 105–123. [Google Scholar] [CrossRef] [PubMed]
- Cheng, S.W.; Li, J.X.; Chien, Y.C.; Chang, J.P.; Shityakov, S.; Huang, S.Y.; Galecki, P.; Su, K.P. Genetic Variations of Ionotropic Glutamate Receptor Pathways on Interferon-α-induced Depression in Patients with Hepatitis C Viral Infection. Brain Behav. Immun. 2021, 93, 16–22. [Google Scholar] [CrossRef]
- Horikawa, N.; Yamazaki, T.; Izumi, N.; Uchihara, M. Incidence and clinical course of major depression in patients with chronic hepatitis type C undergoing interferon-alpha therapy: A prospective study. Gen. Hosp. Psychiatry 2003, 25, 34–38. [Google Scholar] [CrossRef]
- Miller, A.H.; Raison, C.L. The role of inflammation in depression: From evolutionary imperative to modern treatment target. Nat. Rev. Immunol. 2016, 16, 22–34. [Google Scholar] [CrossRef]
- Oriolo, G.; Huet, L.; Dexpert, S.; Beau, C.; Forestier, D.; Ledaguenel, P.; Magne, E.; Martin-Santos, R.; Capuron, L. History of major depression is associated with neuropsychiatric symptoms but not systemic inflammation in a cross-sectional study in obese patients. Brain Behav. Immun. 2019, 76, 215–222. [Google Scholar] [CrossRef]
- Finberg, J.P.M.; Rabey, J.M. Inhibitors of MAO-A and MAO-B in Psychiatry and Neurology. Front. Pharmacol. 2016, 7, 340. [Google Scholar] [CrossRef]
- Dogaru, I.-A.; Puiu, M.G.; Manea, M.; Dionisie, V. Current Perspectives on Pharmacological and Non-Pharmacological Interventions for the Inflammatory Mechanism of Unipolar Depression. Brain Sci. 2022, 12, 1403. [Google Scholar] [CrossRef]
- Woo, Y.; Seo, H.-J.; McIntyre, R.; Bahk, W.-M. Obesity and Its Potential Effects on Antidepressant Treatment Outcomes in Patients with Depressive Disorders: A Literature Review. Int. J. Mol. Sci. 2016, 17, 80. [Google Scholar] [CrossRef]
- Green, E.; Goldstein-Piekarski, A.N.; Schatzberg, A.F.; Rush, A.J.; Ma, J.; Williams, L. Personalizing antidepressant choice by sex, body mass index, and symptom profile: An iSPOT-D report. Pers. Med. Psychiatry 2017, 1–2, 65–73. [Google Scholar] [CrossRef]
- Jha, M.K.; Wakhlu, S.; Dronamraju, N.; Minhajuddin, A.; Greer, T.L.; Trivedi, M.H. Validating pre-treatment body mass index as moderator of antidepressant treatment outcomes: Findings from CO-MED trial. J. Affect. Disord. 2018, 234, 34–37. [Google Scholar] [CrossRef]
- Targum, S.D.; Catania, C.J. Impact of morbid obesity on treatment outcome in a clinical trial of major depressive disorder. Pers. Med. Psychiatry 2017, 3, 18–23. [Google Scholar] [CrossRef]
- Rush, A.J.; Trivedi, M.H.; Wisniewski, S.R.; Nierenberg, A.A.; Stewart, J.W.; Warden, D.; Niederehe, G.; Thase, M.E.; Lavori, P.W.; Lebowitz, B.D.; et al. Acute and longer-term outcomes in depressed outpatients requiring one or several treatment steps: A STAR*D report. Am. J. Psychiatry 2006, 163, 1905–1917. [Google Scholar] [CrossRef] [PubMed]
- Xiao, L.; Zhou, J.; Galling, B.; Chen, R.-s.; Wang, G. The association of body mass index (BMI) with treatment outcomes in patients with major depressive disorder. J. Affect. Disord. 2021, 281, 799–804. [Google Scholar] [CrossRef]
- Lin, C.-H.; Chen, C.-C.; Wong, J.; McIntyre, R.S. Both body weight and BMI predicts improvement in symptom and functioning for patients with major depressive disorder. J. Affect. Disord. 2014, 161, 123–126. [Google Scholar] [CrossRef]
- De Filippis, S.; Pugliese, A.; Christensen, M.C.; Rosso, G.; Di Nicola, M.; Simonsen, K.; Ren, H. Effectiveness of Vortioxetine in Patients with Major Depressive Disorder in Real-World Clinical Practice in Italy: Results from the RELIEVE Study. Neuropsychiatr. Dis. Treat. 2022, 18, 1665–1677. [Google Scholar] [CrossRef] [PubMed]
- Cipriani, A.; Furukawa, T.A.; Salanti, G.; Chaimani, A.; Atkinson, L.Z.; Ogawa, Y.; Leucht, S.; Ruhe, H.G.; Turner, E.H.; Higgins, J.P.T.; et al. Comparative efficacy and acceptability of 21 antidepressant drugs for the acute treatment of adults with major depressive disorder: A systematic review and network meta-analysis. Lancet 2018, 391, 1357–1366. [Google Scholar] [CrossRef] [PubMed]
- Cascio, G.; Schiera, G.; Di Liegro, I. Dietary fatty acids in metabolic syndrome, diabetes and cardiovascular diseases. Curr. Diabetes Rev. 2012, 8, 2–17. [Google Scholar] [CrossRef]
- Chu, K.; Cadar, D.; Iob, E.; Frank, P. Excess body weight and specific types of depressive symptoms: Is there a mediating role of systemic low-grade inflammation? Brain Behav. Immun. 2023, 108, 233–244. [Google Scholar] [CrossRef]
- Capuron, L.; Lasselin, J.; Castanon, N. Role of Adiposity-Driven Inflammation in Depressive Morbidity. Neuropsychopharmacology 2017, 42, 115–128. [Google Scholar] [CrossRef]
- Capuron, L.; Su, S.; Miller, A.H.; Bremner, J.D.; Goldberg, J.; Vogt, G.J.; Maisano, C.; Jones, L.; Murrah, N.V.; Vaccarino, V. Depressive symptoms and metabolic syndrome: Is inflammation the underlying link? Biol. Psychiatry 2008, 64, 896–900. [Google Scholar] [CrossRef] [PubMed]
- Izaola, O.; de Luis, D.; Sajoux, I.; Domingo, J.C.; Vidal, M. [Inflammation and obesity (lipoinflammation)]. Nutr. Hosp. 2015, 31, 2352–2358. [Google Scholar] [CrossRef]
- Pataky, Z.; Bobbioni-Harsch, E.; Golay, A. Obesity: A Complex Growing Challenge. Exp. Clin. Endocrinol. Diabetes 2010, 118, 427–433. [Google Scholar] [CrossRef]
- Esser, N.; Legrand-Poels, S.; Piette, J.; Scheen, A.J.; Paquot, N. Inflammation as a link between obesity, metabolic syndrome and type 2 diabetes. Diabetes Res. Clin. Pract. 2014, 105, 141–150. [Google Scholar] [CrossRef] [PubMed]
- Hernandez, J.D.; Li, T.; Rau, C.M.; Lesuer, W.E.; Wang, P.; Coletta, D.K.; Madura, J.A.; Jacobsen, E.A.; De Filippis, E. ω-3PUFA supplementation ameliorates adipose tissue inflammation and insulin-stimulated glucose disposal in subjects with obesity: A potential role for apolipoprotein E. Int. J. Obes. 2021, 45, 1331–1341. [Google Scholar] [CrossRef]
- Kyrou, I.; Chrousos, G.P.; Tsigos, C. Stress, visceral obesity, and metabolic complications. Ann. N. Y. Acad. Sci. 2006, 1083, 77–110. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.H.; Paz-Filho, G.; Mastronardi, C.; Licinio, J.; Wong, M.-L. Is increased antidepressant exposure a contributory factor to the obesity pandemic? Transl. Psychiatry 2016, 6, e759. [Google Scholar] [CrossRef]
- Keller, J.; Gomez, R.; Williams, G.; Lembke, A.; Lazzeroni, L.; Murphy, G.M., Jr.; Schatzberg, A.F. HPA axis in major depression: Cortisol, clinical symptomatology and genetic variation predict cognition. Mol. Psychiatry 2017, 22, 527–536. [Google Scholar] [CrossRef]
- Gafoor, R.; Booth, H.P.; Gulliford, M.C. Antidepressant utilisation and incidence of weight gain during 10 years’ follow-up: Population based cohort study. Bmj 2018, 361, k1951. [Google Scholar] [CrossRef]
- Chao, A.M.; Jastreboff, A.M.; White, M.A.; Grilo, C.M.; Sinha, R. Stress, cortisol, and other appetite-related hormones: Prospective prediction of 6-month changes in food cravings and weight. Obesity 2017, 25, 713–720. [Google Scholar] [CrossRef]
- Obradovic, M.; Sudar-Milovanovic, E.; Soskic, S.; Essack, M.; Arya, S.; Stewart, A.J.; Gojobori, T.; Isenovic, E.R. Leptin and Obesity: Role and Clinical Implication. Front. Endocrinol. 2021, 12, 585887. [Google Scholar] [CrossRef] [PubMed]
- Ohashi, K.; Kihara, S.; Ouchi, N.; Kumada, M.; Fujita, K.; Hiuge, A.; Hibuse, T.; Ryo, M.; Nishizawa, H.; Maeda, N.; et al. Adiponectin replenishment ameliorates obesity-related hypertension. Hypertension 2006, 47, 1108–1116. [Google Scholar] [CrossRef] [PubMed]
- Tuppad, S.; Medala, K.; Umesh, M.; Gaur, A.; Ganji, V.; Sakthivadivel, V.; Kumar, P. Serum Adiponectin and Nitric Oxide Levels in Type II Diabetes and Its Correlation with Lipid Profile. Cureus 2022, 14, e24613. [Google Scholar] [CrossRef]
- Nakamura, Y.; Shimada, K.; Fukuda, D.; Shimada, Y.; Ehara, S.; Hirose, M.; Kataoka, T.; Kamimori, K.; Shimodozono, S.; Kobayashi, Y.; et al. Implications of plasma concentrations of adiponectin in patients with coronary artery disease. Heart 2004, 90, 528–533. [Google Scholar] [CrossRef] [PubMed]
- Weber-Hamann, B.; Kratzsch, J.; Kopf, D.; Lederbogen, F.; Gilles, M.; Heuser, I.; Deuschle, M. Resistin and adiponectin in major depression: The association with free cortisol and effects of antidepressant treatment. J. Psychiatr. Res. 2007, 41, 344–350. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, A.F.; Rocha, D.Q.; McIntyre, R.S.; Mesquita, L.M.; Kohler, C.A.; Hyphantis, T.N.; Sales, P.M.; Machado-Vieira, R.; Berk, M. Adipokines as emerging depression biomarkers: A systematic review and meta-analysis. J. Psychiatr. Res. 2014, 59, 28–37. [Google Scholar] [CrossRef] [PubMed]
- Coín-Aragüez, L.; Pavón, F.J.; Contreras, A.; Gentile, A.-M.; Lhamyani, S.; De Diego-Otero, Y.; Casado, Y.; Oliva Olivera, W.; Olveira, G.; Tinahones, F.J.; et al. Inflammatory gene expression in adipose tissue according to diagnosis of anxiety and mood disorders in obese and non-obese subjects. Sci. Rep. 2018, 8, 17518. [Google Scholar] [CrossRef] [PubMed]
- Kahl, K.G.; Greggersen, W.; Schweiger, U.; Cordes, J.; Balijepalli, C.; Lösch, C.; Moebus, S. Prevalence of the metabolic syndrome in unipolar major depression. Eur. Arch. Psychiatry Clin. Neurosci. 2012, 262, 313–320. [Google Scholar] [CrossRef]
- Panda, S.S.; Nayak, A.; Shah, S.; Aich, P. A Systematic Review on the Association between Obesity and Mood Disorders and the Role of Gut Microbiota. Metabolites 2023, 13, 488. [Google Scholar] [CrossRef]
- Michielan, A.; D’Incà, R. Intestinal Permeability in Inflammatory Bowel Disease: Pathogenesis, Clinical Evaluation, and Therapy of Leaky Gut. Mediat. Inflamm. 2015, 2015, 628157. [Google Scholar] [CrossRef]
- Stojanov, S.; Berlec, A.; Štrukelj, B. The Influence of Probiotics on the Firmicutes/Bacteroidetes Ratio in the Treatment of Obesity and Inflammatory Bowel disease. Microorganisms 2020, 8, 1715. [Google Scholar] [CrossRef] [PubMed]
- Aizawa, E.; Tsuji, H.; Asahara, T.; Takahashi, T.; Teraishi, T.; Yoshida, S.; Ota, M.; Koga, N.; Hattori, K.; Kunugi, H. Possible association of Bifidobacterium and Lactobacillus in the gut microbiota of patients with major depressive disorder. J. Affect. Disord. 2016, 202, 254–257. [Google Scholar] [CrossRef] [PubMed]
- Palmas, V.; Pisanu, S.; Madau, V.; Casula, E.; Deledda, A.; Cusano, R.; Uva, P.; Vascellari, S.; Loviselli, A.; Manzin, A.; et al. Gut microbiota markers associated with obesity and overweight in Italian adults. Sci. Rep. 2021, 11, 5532. [Google Scholar] [CrossRef] [PubMed]
- Liu, T.; Hougen, H.; Vollmer, A.C.; Hiebert, S.M. Gut bacteria profiles of Mus. musculus at the phylum and family levels are influenced by saturation of dietary fatty acids. Anaerobe 2012, 18, 331–337. [Google Scholar] [CrossRef]
- Yu, H.N.; Zhu, J.; Pan, W.S.; Shen, S.R.; Shan, W.G.; Das, U.N. Effects of fish oil with a high content of n-3 polyunsaturated fatty acids on mouse gut microbiota. Arch. Med. Res. 2014, 45, 195–202. [Google Scholar] [CrossRef]
- Nogal, A.; Valdes, A.M.; Menni, C. The role of short-chain fatty acids in the interplay between gut microbiota and diet in cardio-metabolic health. Gut Microbes 2021, 13, 1897212. [Google Scholar] [CrossRef]
- Ohlsson, L.; Gustafsson, A.; Lavant, E.; Suneson, K.; Brundin, L.; Westrin, Å.; Ljunggren, L.; Lindqvist, D. Leaky gut biomarkers in depression and suicidal behavior. Acta Psychiatr. Scand. 2019, 139, 185–193. [Google Scholar] [CrossRef]
- Ciocan, D.; Cassard, A.-M.; Becquemont, L.; Verstuyft, C.; Voican, C.S.; El Asmar, K.; Colle, R.; David, D.; Trabado, S.; Feve, B.; et al. Blood microbiota and metabolomic signature of major depression before and after antidepressant treatment: A prospective case–control study. J. Psychiatry Neurosci. 2021, 46, E358–E368. [Google Scholar] [CrossRef]
- Thesing, C.S.; Bot, M.; Milaneschi, Y.; Giltay, E.J.; Penninx, B.W.J.H. Bidirectional longitudinal associations of omega-3 polyunsaturated fatty acid plasma levels with depressive disorders. J. Psychiatr. Res. 2020, 124, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Lin, P.Y.; Huang, S.Y.; Su, K.P. A meta-analytic review of polyunsaturated fatty acid compositions in patients with depression. Biol. Psychiatry 2010, 68, 140–147. [Google Scholar] [CrossRef] [PubMed]
- Cussotto, S.; Delgado, I.; Oriolo, G.; Kemper, J.; Begarie, D.; Dexpert, S.; Sauvant, J.; Leboyer, M.; Aouizerate, B.; Martin-Santos, R.; et al. Low omega–3 polyunsaturated fatty acids predict reduced response to standard antidepressants in patients with major depressive disorder. Depress. Anxiety 2022, 39, 407–418. [Google Scholar] [CrossRef]
- Zhou, L.; Xiong, J.Y.; Chai, Y.Q.; Huang, L.; Tang, Z.Y.; Zhang, X.F.; Liu, B.; Zhang, J.T. Possible antidepressant mechanisms of omega-3 polyunsaturated fatty acids acting on the central nervous system. Front. Psychiatry 2022, 13, 933704. [Google Scholar] [CrossRef]
- Gertsik, L.; Poland, R.E.; Bresee, C.; Rapaport, M.H. Omega-3 fatty acid augmentation of citalopram treatment for patients with major depressive disorder. J. Clin. Psychopharmacol. 2012, 32, 61–64. [Google Scholar] [CrossRef] [PubMed]
- Jazayeri, S.; Keshavarz, S.A.; Tehrani-Doost, M.; Djalali, M.; Hosseini, M.; Amini, H.; Chamari, M.; Djazayery, A. Effects of eicosapentaenoic acid and fluoxetine on plasma cortisol, serum interleukin-1beta and interleukin-6 concentrations in patients with major depressive disorder. Psychiatry Res. 2010, 178, 112–115. [Google Scholar] [CrossRef]
- Nishi, D.; Su, K.P.; Usuda, K.; Chang, J.P.; Hamazaki, K.; Ishima, T.; Sano, Y.; Ito, H.; Isaka, K.; Tachibana, Y.; et al. Plasma estradiol levels and antidepressant effects of omega-3 fatty acids in pregnant women. Brain Behav. Immun. 2019, 85, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Mocking, R.J.; Harmsen, I.; Assies, J.; Koeter, M.W.; Ruhé, H.G.; Schene, A.H. Meta-analysis and meta-regression of omega-3 polyunsaturated fatty acid supplementation for major depressive disorder. Transl. Psychiatry 2016, 6, e756. [Google Scholar] [CrossRef] [PubMed]
- Lamon-Fava, S.; Liu, M.; Dunlop, B.W.; Kinkead, B.; Schettler, P.J.; Felger, J.C.; Ziegler, T.R.; Fava, M.; Mischoulon, D.; Rapaport, M.H. Clinical response to EPA supplementation in patients with major depressive disorder is associated with higher plasma concentrations of pro-resolving lipid mediators. Neuropsychopharmacology 2023, 48, 929–935. [Google Scholar] [CrossRef]
- Tu, C.H.; Chen, C.M.; Yang, C.C.; Gałecki, P.; Su, K.P. Brain Responses to Emotional Stimuli after Eicosapentaenoic Acid and Docosahexaenoic Acid Treatments in Major Depressive Disorder: Toward Personalized Medicine with Anti-Inflammatory Nutraceuticals. J. Pers. Med. 2020, 10, 283. [Google Scholar] [CrossRef]
- Schefft, C.; Kilarski, L.L.; Bschor, T.; Köhler, S. Efficacy of adding nutritional supplements in unipolar depression: A systematic review and meta-analysis. Eur. Neuropsychopharmacol. 2017, 27, 1090–1109. [Google Scholar] [CrossRef]
- Su, K.P.; Lai, H.C.; Yang, H.T.; Su, W.P.; Peng, C.Y.; Chang, J.P.; Chang, H.C.; Pariante, C.M. Omega-3 fatty acids in the prevention of interferon-alpha-induced depression: Results from a randomized, controlled trial. Biol. Psychiatry 2014, 76, 559–566. [Google Scholar] [CrossRef]
- Liao, Y.; Xie, B.; Zhang, H.; He, Q.; Guo, L.; Subramanieapillai, M.; Fan, B.; Lu, C.; McIntyre, R.S. Efficacy of omega-3 PUFAs in depression: A meta-analysis. Transl. Psychiatry 2019, 9, 190. [Google Scholar] [CrossRef]
- Jiang, W.; Whellan, D.J.; Adams, K.F.; Babyak, M.A.; Boyle, S.H.; Wilson, J.L.; Patel, C.B.; Rogers, J.G.; Harris, W.S.; O’Connor, C.M. Long-Chain Omega-3 Fatty Acid Supplements in Depressed Heart Failure Patients: Results of the OCEAN Trial. JACC Heart Fail. 2018, 6, 833–843. [Google Scholar] [CrossRef]
- Chang, J.P.; Chang, S.S.; Yang, H.T.; Chen, H.T.; Chien, Y.C.; Yang, B.; Su, H.; Su, K.P. Omega-3 polyunsaturated fatty acids in cardiovascular diseases comorbid major depressive disorder—Results from a randomized controlled trial. Brain Behav. Immun. 2020, 85, 14–20. [Google Scholar] [CrossRef]
- Mazereeuw, G.; Herrmann, N.; Oh, P.I.; Ma, D.W.; Wang, C.T.; Kiss, A.; Lanctôt, K.L. Omega-3 Fatty Acids, Depressive Symptoms, and Cognitive Performance in Patients with Coronary Artery Disease: Analyses From a Randomized, Double-Blind, Placebo-Controlled Trial. J. Clin. Psychopharmacol. 2016, 36, 436–444. [Google Scholar] [CrossRef]
- Xu, W.; Finitsis, D.; Salner, A.; Judge, M. Feasibility of Investigational Procedures and Efficacy of a Personalized Omega-3 Dietary Intervention in Alleviating Pain and Psychoneurological Symptoms in Breast Cancer Survivors. Pain Manag. Nurs. 2023, 24, 78–88. [Google Scholar] [CrossRef]
- Bot, M.; Pouwer, F.; Assies, J.; Jansen, E.H.; Beekman, A.T.; de Jonge, P. Supplementation with eicosapentaenoic omega-3 fatty acid does not influence serum brain-derived neurotrophic factor in diabetes mellitus patients with major depression: A randomized controlled pilot study. Neuropsychobiology 2011, 63, 219–223. [Google Scholar] [CrossRef]
- Keshavarz, S.A.; Mostafavi, S.A.; Akhondzadeh, S.; Mohammadi, M.R.; Hosseini, S.; Eshraghian, M.R.; Chamari, M. Omega-3 supplementation effects on body weight and depression among dieter women with co-morbidity of depression and obesity compared with the placebo: A randomized clinical trial. Clin. Nutr. ESPEN 2018, 25, 37–43. [Google Scholar] [CrossRef] [PubMed]
- da Silva, T.M.; Munhoz, R.P.; Alvarez, C.; Naliwaiko, K.; Kiss, A.; Andreatini, R.; Ferraz, A.C. Depression in Parkinson’s disease: A double-blind, randomized, placebo-controlled pilot study of omega-3 fatty-acid supplementation. J. Affect. Disord. 2008, 111, 351–359. [Google Scholar] [CrossRef] [PubMed]
- Chiu, C.C.; Su, K.P.; Cheng, T.C.; Liu, H.C.; Chang, C.J.; Dewey, M.E.; Stewart, R.; Huang, S.Y. The effects of omega-3 fatty acids monotherapy in Alzheimer’s disease and mild cognitive impairment: A preliminary randomized double-blind placebo-controlled study. Prog. Neuropsychopharmacol. Biol. Psychiatry 2008, 32, 1538–1544. [Google Scholar] [CrossRef]
- Freund-Levi, Y.; Basun, H.; Cederholm, T.; Faxén-Irving, G.; Garlind, A.; Grut, M.; Vedin, I.; Palmblad, J.; Wahlund, L.O.; Eriksdotter-Jönhagen, M. Omega-3 supplementation in mild to moderate Alzheimer’s disease: Effects on neuropsychiatric symptoms. Int. J. Geriatr. Psychiatry 2008, 23, 161–169. [Google Scholar] [CrossRef] [PubMed]
- Okereke, O.I.; Vyas, C.M.; Mischoulon, D.; Chang, G.; Cook, N.R.; Weinberg, A.; Bubes, V.; Copeland, T.; Friedenberg, G.; Lee, I.M.; et al. Effect of Long-term Supplementation with Marine Omega-3 Fatty Acids vs Placebo on Risk of Depression or Clinically Relevant Depressive Symptoms and on Change in Mood Scores. JAMA 2021, 326, 2385. [Google Scholar] [CrossRef] [PubMed]
- Freeman, M.P.; Davis, M.; Sinha, P.; Wisner, K.L.; Hibbeln, J.R.; Gelenberg, A.J. Omega-3 fatty acids and supportive psychotherapy for perinatal depression: A randomized placebo-controlled study. J. Affect. Disord. 2008, 110, 142–148. [Google Scholar] [CrossRef] [PubMed]
- Trebatická, J.; Hradečná, Z.; Surovcová, A.; Katrenčíková, B.; Gushina, I.; Waczulíková, I.; Sušienková, K.; Garaiova, I.; Šuba, J.; Ďuračková, Z. Omega-3 fatty-acids modulate symptoms of depressive disorder, serum levels of omega-3 fatty acids and omega-6/omega-3 ratio in children. A randomized, double-blind and controlled trial. Psychiatry Res. 2020, 287, 112911. [Google Scholar] [CrossRef]
- Amminger, G.P.; Schäfer, M.R.; Papageorgiou, K.; Klier, C.M.; Cotton, S.M.; Harrigan, S.M.; Mackinnon, A.; McGorry, P.D.; Berger, G.E. Long-chain omega-3 fatty acids for indicated prevention of psychotic disorders: A randomized, placebo-controlled trial. Arch. Gen. Psychiatry 2010, 67, 146–154. [Google Scholar] [CrossRef] [PubMed]
- Robinson, D.G.; Gallego, J.A.; John, M.; Hanna, L.A.; Zhang, J.P.; Birnbaum, M.L.; Greenberg, J.; Naraine, M.; Peters, B.D.; McNamara, R.K.; et al. A potential role for adjunctive omega-3 polyunsaturated fatty acids for depression and anxiety symptoms in recent onset psychosis: Results from a 16 week randomized placebo-controlled trial for participants concurrently treated with risperidone. Schizophr. Res. 2019, 204, 295–303. [Google Scholar] [CrossRef] [PubMed]
- Matsuoka, Y.; Nishi, D.; Hamazaki, K.; Yonemoto, N.; Matsumura, K.; Noguchi, H.; Hashimoto, K.; Hamazaki, T. Docosahexaenoic acid for selective prevention of posttraumatic stress disorder among severely injured patients: A randomized, placebo-controlled trial. J. Clin. Psychiatry 2015, 76, e1015–e1022. [Google Scholar] [CrossRef]
- Ryan, M.; Eatmon, C.V.; Slevin, J.T. Drug treatment strategies for depression in Parkinson disease. Expert. Opin. Pharmacother. 2019, 20, 1351–1363. [Google Scholar] [CrossRef]
- Brites, D.; Fernandes, A. Neuroinflammation and Depression: Microglia Activation, Extracellular Microvesicles and microRNA Dysregulation. Front. Cell. Neurosci. 2015, 9, 476. [Google Scholar] [CrossRef]
- Lin, P.Y.; Cheng, C.; Satyanarayanan, S.K.; Chiu, L.T.; Chien, Y.C.; Chuu, C.P.; Lan, T.H.; Su, K.P. Omega-3 fatty acids and blood-based biomarkers in Alzheimer’s disease and mild cognitive impairment: A randomized placebo-controlled trial. Brain Behav. Immun. 2022, 99, 289–298. [Google Scholar] [CrossRef]
- Borsini, A.; Nicolaou, A.; Camacho-Muñoz, D.; Kendall, A.C.; Di Benedetto, M.G.; Giacobbe, J.; Su, K.P.; Pariante, C.M. Omega-3 polyunsaturated fatty acids protect against inflammation through production of LOX and CYP450 lipid mediators: Relevance for major depression and for human hippocampal neurogenesis. Mol. Psychiatry 2021, 26, 6773–6788. [Google Scholar] [CrossRef]
- Chiu, C.C.; Frangou, S.; Chang, C.J.; Chiu, W.C.; Liu, H.C.; Sun, I.W.; Liu, S.I.; Lu, M.L.; Chen, C.H.; Huang, S.Y.; et al. Associations between n-3 PUFA concentrations and cognitive function after recovery from late-life depression. Am. J. Clin. Nutr. 2012, 95, 420–427. [Google Scholar] [CrossRef]
- Sinn, N.; Milte, C.M.; Street, S.J.; Buckley, J.D.; Coates, A.M.; Petkov, J.; Howe, P.R.C. Effects of n-3 fatty acids, EPAv. DHA, on depressive symptoms, quality of life, memory and executive function in older adults with mild cognitive impairment: A 6-month randomised controlled trial. Br. J. Nutr. 2012, 107, 1682–1693. [Google Scholar] [CrossRef]
- Yang, C.P.; Chang, C.M.; Yang, C.C.; Pariante, C.M.; Su, K.P. Long COVID and long chain fatty acids (LCFAs): Psychoneuroimmunity implication of omega-3 LCFAs in delayed consequences of COVID-19. Brain Behav. Immun. 2022, 103, 19–27. [Google Scholar] [CrossRef]
- Zailani, H.; Satyanarayanan, S.K.; Liao, W.C.; Liao, H.F.; Huang, S.Y.; Gałecki, P.; Su, K.P.; Chang, J.P. Omega-3 Polyunsaturated Fatty Acids in Managing Comorbid Mood Disorders in Chronic Obstructive Pulmonary Disease (COPD): A Review. J. Clin. Med. 2023, 12, 2653. [Google Scholar] [CrossRef]
- Chang, J.P.; Su, K.P. Nutritional Neuroscience as Mainstream of Psychiatry: The Evidence- Based Treatment Guidelines for Using Omega-3 Fatty Acids as a New Treatment for Psychiatric Disorders in Children and Adolescents. Clin. Psychopharmacol. Neurosci. 2020, 18, 469–483. [Google Scholar] [CrossRef]
- Zhang, M.M.; Zou, Y.; Li, S.M.; Wang, L.; Sun, Y.H.; Shi, L.; Lu, L.; Bao, Y.P.; Li, S.X. The efficacy and safety of omega-3 fatty acids on depressive symptoms in perinatal women: A meta-analysis of randomized placebo-controlled trials. Transl. Psychiatry 2020, 10, 193. [Google Scholar] [CrossRef]
- Bender, N.; Portmann, M.; Heg, Z.; Hofmann, K.; Zwahlen, M.; Egger, M. Fish or n3-PUFA intake and body composition: A systematic review and meta-analysis. Obes. Rev. 2014, 15, 657–665. [Google Scholar] [CrossRef]
- Harden, C.J.; Dible, V.A.; Russell, J.M.; Garaiova, I.; Plummer, S.F.; Barker, M.E.; Corfe, B.M. Long-chain polyunsaturated fatty acid supplementation had no effect on body weight but reduced energy intake in overweight and obese women. Nutr. Res. 2014, 34, 17–24. [Google Scholar] [CrossRef]
- Payahoo, L.; Ostadrahimi, A.; Farrin, N.; Khaje-Bishak, Y. Effects of n-3 Polyunsaturated Fatty Acid Supplementation on Serum Leptin Levels, Appetite Sensations, and Intake of Energy and Macronutrients in Obese People: A Randomized Clinical Trial. J. Diet. Suppl. 2018, 15, 596–605. [Google Scholar] [CrossRef]
- Suzuki, K.; Jayasena, C.N.; Bloom, S.R. Obesity and appetite control. Exp. Diabetes Res. 2012, 2012, 824305. [Google Scholar] [CrossRef]
- Madison, A.A.; Belury, M.A.; Andridge, R.; Renna, M.E.; Rosie Shrout, M.; Malarkey, W.B.; Lin, J.; Epel, E.S.; Kiecolt-Glaser, J.K. Omega-3 supplementation and stress reactivity of cellular aging biomarkers: An ancillary substudy of a randomized, controlled trial in midlife adults. Mol. Psychiatry 2021, 26, 3034–3042. [Google Scholar] [CrossRef]
- Liu, H.; Wang, F.; Liu, X.; Xie, Y.; Xia, H.; Wang, S.; Sun, G. Effects of marine-derived and plant-derived omega-3 polyunsaturated fatty acids on erythrocyte fatty acid composition in type 2 diabetic patients. Lipids Health Dis. 2022, 21, 20. [Google Scholar] [CrossRef]
- Rafraf, M.; Mohammadi, E.; Asghari-Jafarabadi, M.; Farzadi, L. Omega-3 fatty acids improve glucose metabolism without effects on obesity values and serum visfatin levels in women with polycystic ovary syndrome. J. Am. Coll. Nutr. 2012, 31, 361–368. [Google Scholar] [CrossRef]


{kind=link}
| Biological specificity | Population | Study Design | Intervention | Main Findings | References | |
| ||||||
| IFN-induced depression | n = 152, HCV patients | Double-blind, RCT | 2-week treatment with EPA (3.5 g/day) (n = 50); DHA (1.75 g/day) (n = 51); placebo (n = 50) | EPA-treated, not DHA-treated significantly decreased the incidence of IFN-α-induced depression in HCV patients (10%, 28%, respectively, compared to 30% placebo, p = 0.037). | [101] | |
| Cardiovascular disease comorbidity | n = 59, CVD patients with comorbid MDD | RCT | 2-week treatment with n-3 PUFAs (EPA 2.0 g/day and DHA 1.0 g/day) (n = 30); placebo (n = 29) | No significant differences between groups in HAMD and BDI-II total scores, but n-3 PUFAs significantly reduced HAMD cognition at week 8 (p < 0.05) and the HAMD core subscale in very severe MDD at week 12 (p < 0.05). | [104] | |
| n = 108, CHF patients with comorbid MDD | Double-blind, RCT | 2-week treatment with n-3 PUFAs (2:1 EPA/DHA 2.0 g/day) (n = 36); EPA (2 g/day) (n = 36); placebo (n = 36) | No significant differences between groups in HAMD and BDI-II total scores. BDI-II cognitive depressive subscales were strongly associated with the high EPA group (p < 0.05). | [103] | ||
| n = 92, CAD patients with comorbid MDD | Double-blind, RCT | 2-week treatment with n-3 PUFAs (1.9 g/day) (n = 45); placebo (n = 47) | Plasma EPA and DHA levels increased (p < 0.01), but no significant differences between groups in HAMD (p = 0.20) and BDI-II (p = 0.50) total scores. | [105] | ||
| Pain comorbidity | n = 46, Breast cancer survivor | Prospective, RCT | 6-week diet intervention with high n-3 PUFAs (2040 mg, 12 ounces/week wild-caught Alaskan salmon) (n = 24) and low PUFAs (1020 mg, 6 ounces/week) (n = 15) | High n-3 PUFA group significantly decreased pain (p < 0.01), perceived stress (p < 0.05), sleep (p < 0.001), depression (p < 0.001), and fatigue (p < 0.01). | [106] | |
| Obesity and metabolic comorbidity | n = 25, Diabetes patients with MDD | Double-blind, RCT | 12-week treatment with EPA (1 g/day) (n = 13), placebo (n = 12) | No significant impact on BDNF (p = 0.887) and no significant association between changes in BDNF levels and depression severity (p = 0.593). | [107] | |
| n = 45, Obese patient with MDD | Double-blind, RCT | 12-week treatment with n-3 PUFAs (1.08 g/d EPA and 0.72 g/d DHA) (n = 24); placebo (n = 21) | Significantly reduced depression (p = 0.05) in n-3 treatment groups. | [108] | ||
| n = 61, Obese patient with MDD | Double-blind, RCT | 12-week treatment with EPA (1 g/d, n = 15; 2 g/d, n = 15; 4 g/day, n = 16); placebo (n = 15) | EPA 4 g/d produced a sustained effect on IDS-30 scores at both weeks 8 and 12. A potential dose-response relationship between EPA dose and change in IDS-C30 scores, but this was not statistically significant. | [26] | ||
| ||||||
| Parkinson’s disease comorbidity | n = 29, Parkinson’s disease with MDD | Double-blind, RCT | 12-week treatment with n-3 PUFAs (1200 mg/d) (n = 14); placebo (n = 15) | Significant decrease in MADRS and CGI-Depression scores but not in BDI in the n-3 PUFAs group. | [109] | |
| Alzheimer’s disease comorbidity | n = 26, Patients with MCI or AD | Double-blind, RCT | 24-week treatment with n-3 PUFAs (1080 mg/d EPA and 720 mg/d DHA) (n = 20); placebo (n = 15) | No associations were found between the randomization group and ADAS-cog, MMSE, or HDRS scores. | [110] | |
| n = 204, Patient with AD | Double-blind, RCT | 6-month treatment with n-3 PUFAs (0.6 g/d EPA and 1.7 g/d DHA) (n = 103); placebo (n = 103) | No overall n-3 PUFA effect on neuropsychiatric symptoms. Possible positive effects of MADRS in non-APOEv4 carriers (p = 0.005). | [111] | ||
| Late-life depression | n = 18,353, Adults aged 50 years or older without depression | RCT | Median of 5.3 years of treatment with n-3 PUFAs (65 mg/d EPA and 375 mg/d DHA) (n = 9171), placebo (n = 9182) | No significant improvement in the n-3 PUFA group in the prevention of depression. | [112] | |
| ||||||
| Perinatal depression | n = 59, Perinatal and postpartum women | Double-blind, RCT | 8-week treatment with n-3 PUFAs (1.9 g/d) (n = 28), placebo (n = 23) | Both groups experienced significant decreases in EPDS and HAM-D scores (p < 0.0001) from baseline. | [113] | |
| n = 36, Perinatal women with MDD | Double-blind, RCT | 8-week treatment with n-3 PUFAs (3.4 g/d) (n = 18), placebo (n = 18) | Significantly lower EDPS and BDI were observed in the n-3 PUFA group. | [22] | ||
| Safety consideration | Special populations | |||||
| Children and adolescents with depression | n = 60, Children with DD or MADD | Double-blind, RCT | 12-week treatment n-3 PUFAs (2.4 g/d) (n = 30), n-6 PUFAs (n = 30) | Significant reductions in CDI scores were observed in the n-3 PUFAs group and the DD subgroup compared to the n-6 PUFAs and MADD subgroup. No serious side effects were observed, except for increased defecation reported by one participant in the n-3 PUFA group. | [114] | |
| High-risk psychosis | n = 81, Patients with an ultra-high risk of psychotic disorder | Double-blind, RCT | 12-week treatment with n-3 PUFAs (1.2 g/d) (n = 41), placebo (n = 40) | Significant improvement was observed in PANSS and GAF scores but not in MADRS scores. No significant adverse effects between the treatment groups. | [115] | |
| n = 50, Patients with schizophrenia-spectrum or bipolar disorders on medication | RCT | 16-week n-3 PUFAs (740 mg/d EPA and 400 mg/d DHA) (n = 27), placebo (n = 26) | The n-3 PUFA group showed significant improvement in BPRS scores compared to placebo among a subgroup of patients (n = 23) who did not receive lorazepam. Lower rates of confusion, anxiety, depression, irritability, and tiredness/fatigue in the n-3 PUFAs group as compared to those on placebo. | [116] | ||
| n = 110, Injured patients with PTSD | Double-blind, RCT | 12-week n-3 PUFAs (1470 mg/d DHA and 147 mg/d EPA) (n = 53), placebo (n = 57) | Serum BDNF and pro-BDNF changes at week 12 were linked to depression severity, but DHA had no specific effect on these levels. Adverse events, including loose stool and constipation, were reported, but there were no significant differences between the two groups. | [117] | ||
| Pregnant women with MDD | n = 36, Perinatal women with MDD | Double-blind, RCT | 8-week treatment with n-3 PUFAs (3.4 g/d) (n = 18), placebo (n = 18) | Well tolerated, and there were no adverse effects on the subjects or newborns. | [22] | |
| References | Sample | Study Design | Intervention | Outcome Scale | Main Findings | Notes and Limitations |
|---|---|---|---|---|---|---|
| Bot et al. (2011) [107] | n = 25, Women with MDD and diabetes on antidepressants | Double-blind, RCT | 12-week treatment with EPA (1 g/day) (n = 13), placebo (n = 12) | MADRS, Serum BDNF | No significant impact on BDNF (p = 0.887) and no significant association between changes in BDNF levels and depression severity (p = 0.593). | First clinical study to examine the effects of n-3 PUFAs on BDNF. Small sample size. One patient reported an allergic reaction and discontinued using EPA; no other severe adverse events were reported. |
| Keshavarz et al. (2018) [108] | n = 45, Women with depression and comorbid obesity (BMI ≥ 25 kg/m2) without antidepressants | Double-blind, RCT, | 12-week treatment with n-3 PUFAs (EPA 1.08 g/day and DHA 0.72 g/day) (n = 24); placebo (n = 21) | Body weight, height, BMI, waist and hip circumferences, total body fat, muscle percentage, BDI, food craving questionnaire, appetite, and food abstinence visual Analogue scales | Reduced depression (p = 0.05) and body weight (p = 0.049) in n-3 treatment groups | Weight regains after a one-month follow-up. Side effects include nausea, skin rash, hemorrhagia, and increased appetite, which were reported in both groups. |
| Mischoulon et al. (2022) [26] | n = 61, Patient with MDD comorbid overweight/obese (BMI ≥ 25 kg/m2), without antidepressants | Double-blind, RCT | 12-week treatment with EPA (1 g/d, n = 15; 2 g/d, n = 15; 4 g/day, n = 16); placebo (n = 15) | IL-6, LPS-stimulated TNF level, plasma hs-CRP level, IDS-C30 | EPA 4 g/d produced a sustained effect on IDS-30 scores at both weeks 8 and 12. A potential dose-response relationship between EPA dose and change in IDS-C30 scores, but this was not statistically significant. | 1st dose-finding trial of EPA in MDD to focus on inflammatory biomarkers as a primary outcome among overweight/obese subjects with elevated hs-CRP |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, S.-K.; Chen, W.-J.; Chang, J.P.-C.; Guu, T.-W.; Hsin, M.-C.; Huang, C.-K.; Mischoulon, D.; Capuron, L.; Su, K.-P. Personalized Medicine of Omega-3 Fatty Acids in Depression Treatment in Obese and Metabolically Dysregulated Patients. J. Pers. Med. 2023, 13, 1003. https://doi.org/10.3390/jpm13061003
Wu S-K, Chen W-J, Chang JP-C, Guu T-W, Hsin M-C, Huang C-K, Mischoulon D, Capuron L, Su K-P. Personalized Medicine of Omega-3 Fatty Acids in Depression Treatment in Obese and Metabolically Dysregulated Patients. Journal of Personalized Medicine. 2023; 13(6):1003. https://doi.org/10.3390/jpm13061003
Chicago/Turabian StyleWu, Suet-Kei, Wei-Jen Chen, Jane Pei-Chen Chang, Ta-Wei Guu, Ming-Che Hsin, Chih-Kun Huang, David Mischoulon, Lucile Capuron, and Kuan-Pin Su. 2023. "Personalized Medicine of Omega-3 Fatty Acids in Depression Treatment in Obese and Metabolically Dysregulated Patients" Journal of Personalized Medicine 13, no. 6: 1003. https://doi.org/10.3390/jpm13061003
APA StyleWu, S.-K., Chen, W.-J., Chang, J. P.-C., Guu, T.-W., Hsin, M.-C., Huang, C.-K., Mischoulon, D., Capuron, L., & Su, K.-P. (2023). Personalized Medicine of Omega-3 Fatty Acids in Depression Treatment in Obese and Metabolically Dysregulated Patients. Journal of Personalized Medicine, 13(6), 1003. https://doi.org/10.3390/jpm13061003