
Long-Term Outcomes after Transcatheter Mitral Valve-in-Valve or Valve-in-Ring Procedures

 , , ,
, , ,
Abstract
1. Introduction
2. Patients and Methods
2.1. Study Design and Inclusion and Exclusion Criteria
2.2. Data Collection, Ethic Statement, and Study Endpoints
2.3. Patients, Study Groups, and Follow-Up
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
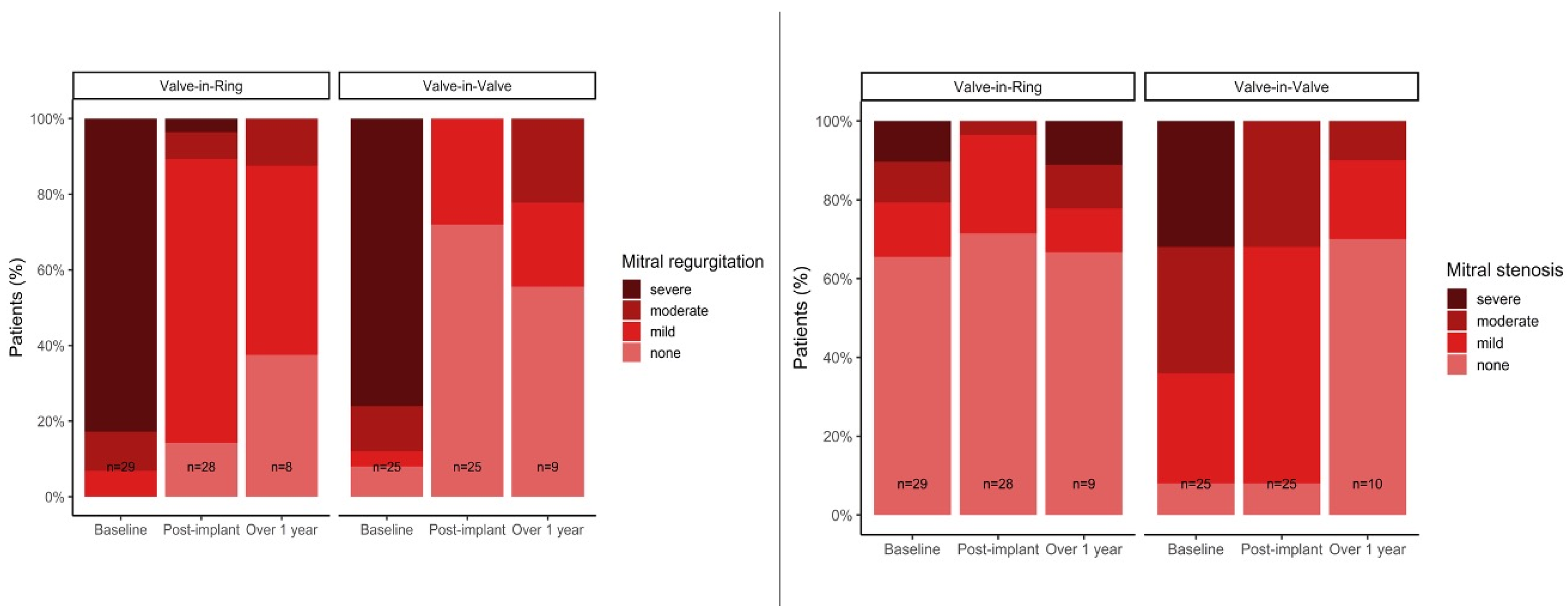
3.2. Echocardiographic Baselines
3.3. Procedural Data
3.4. Postoperative Course and Hospital Outcomes
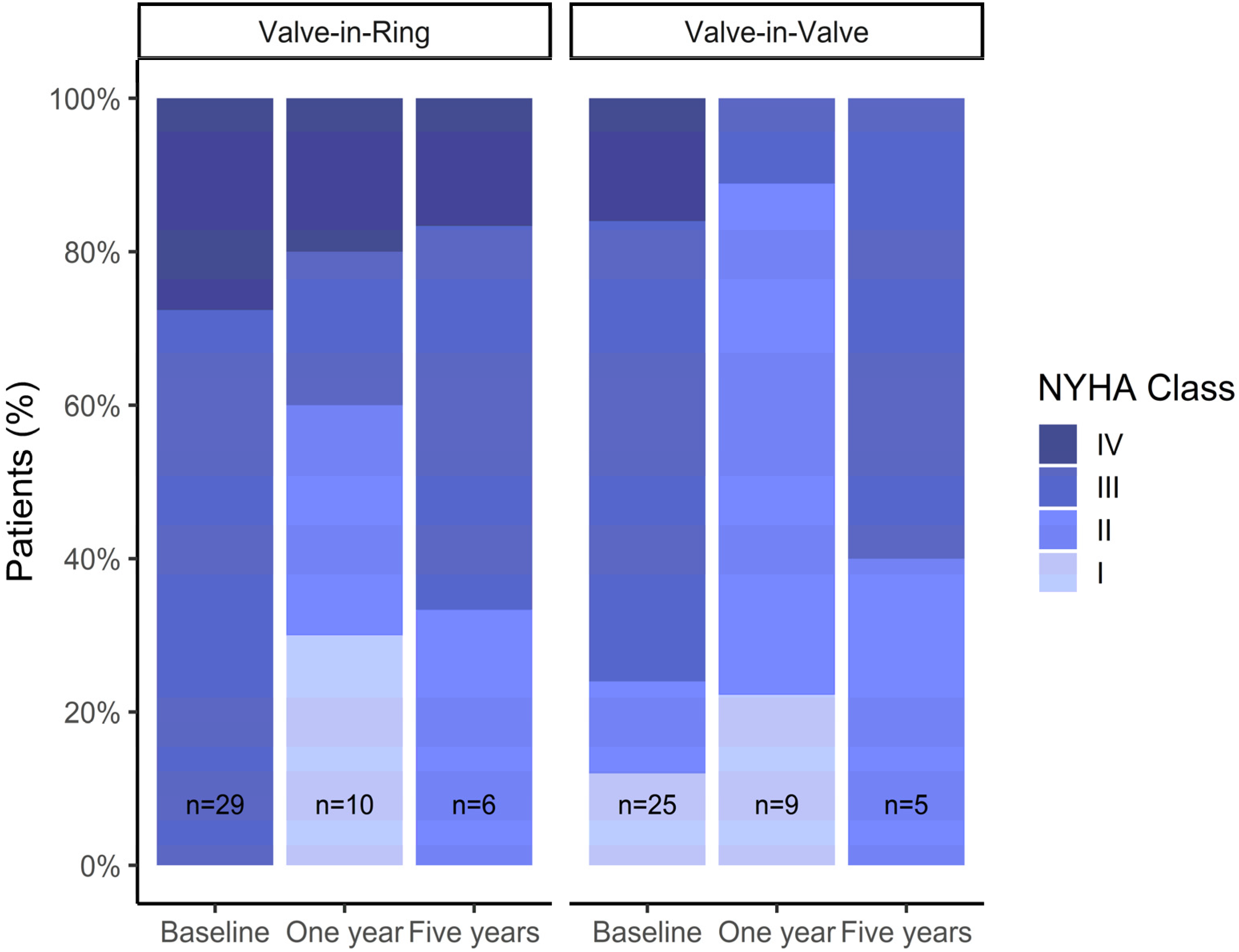
3.5. Follow-Up Data
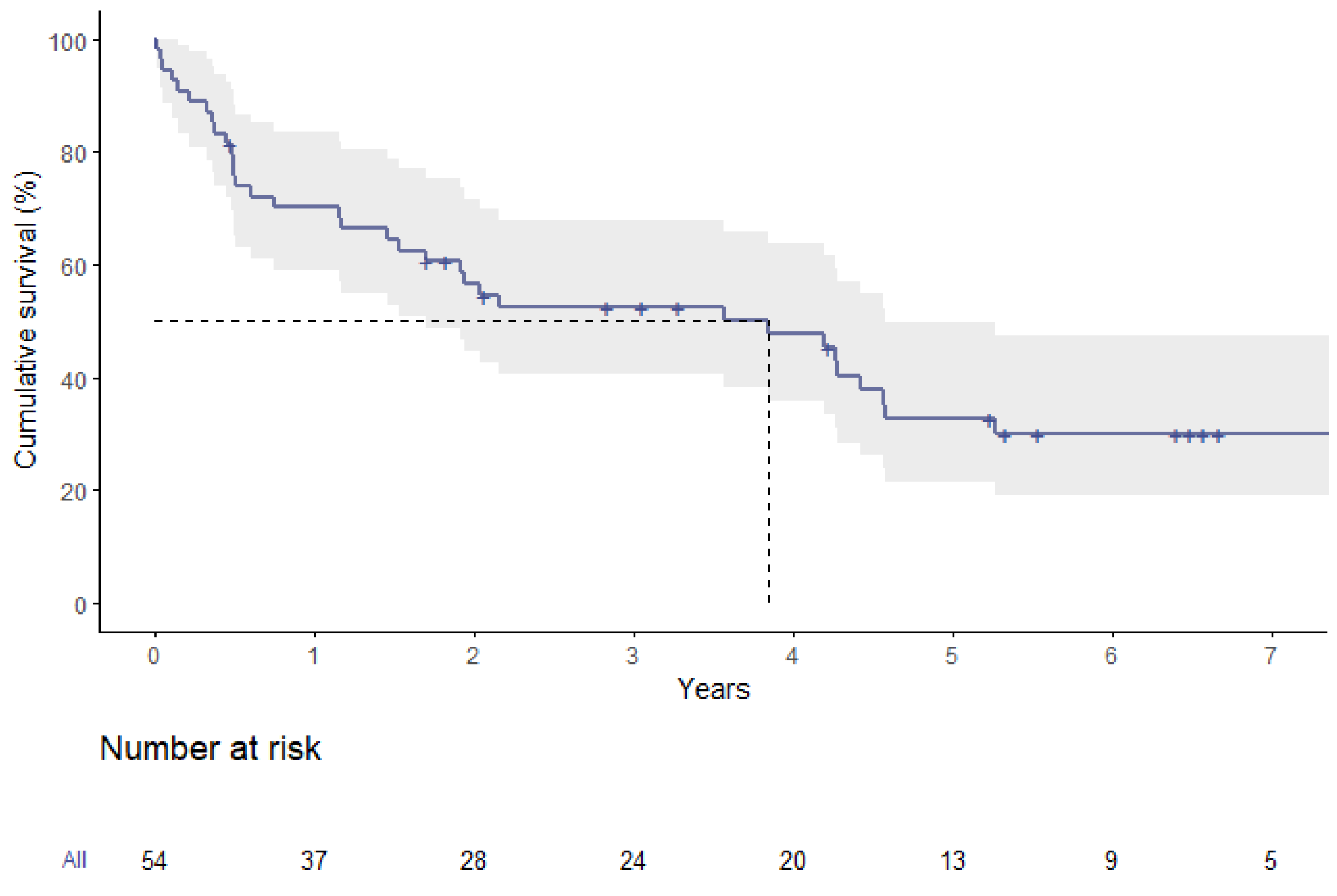
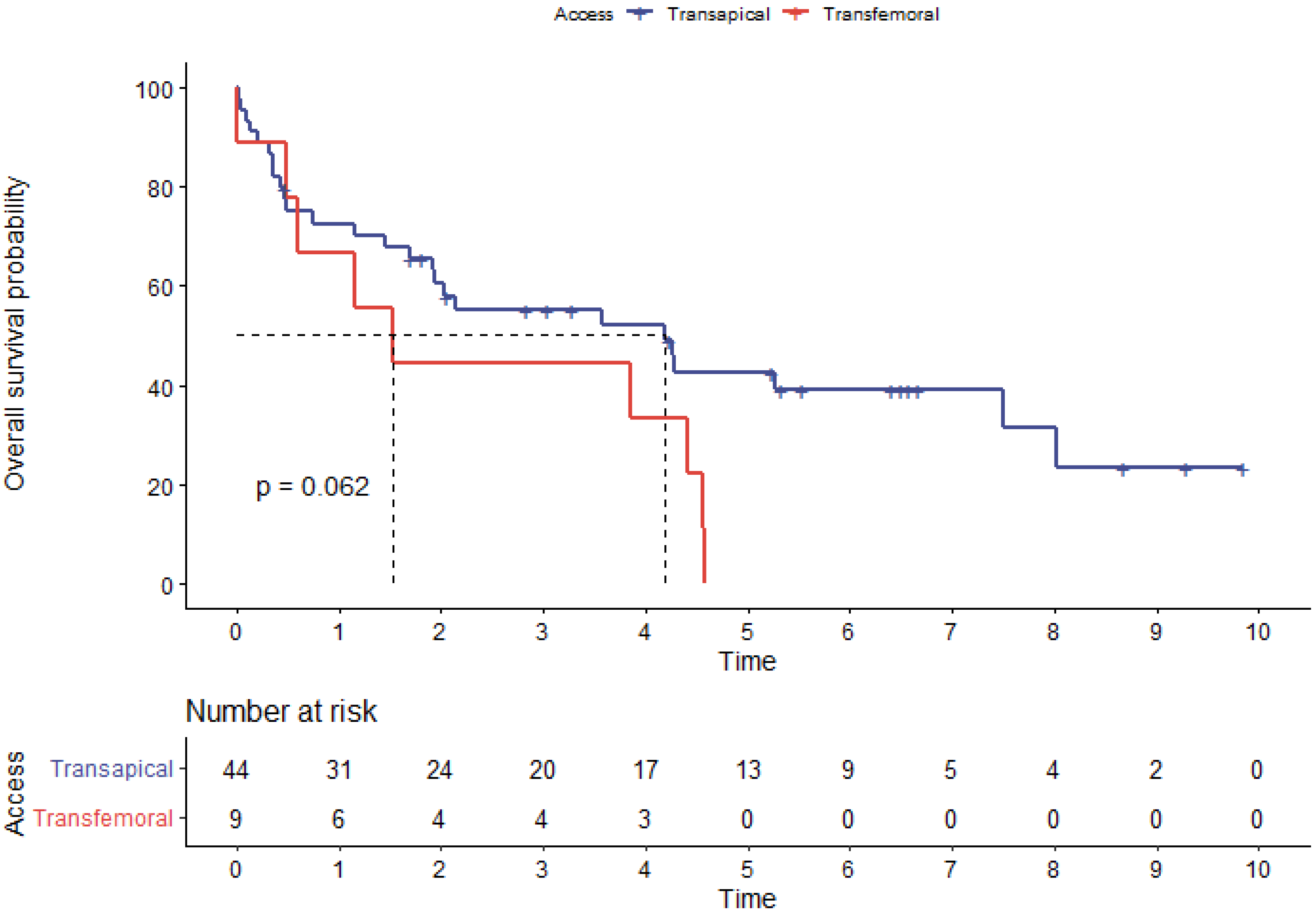
3.6. Survival Analysis
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Vahanian, A.; Beyersdorf, F.; Praz, F.; Milojevic, M.; Baldus, S.; Bauersachs, J.; Capodanno, D.; Conradi, L.; de Bonis, M.; de Paulis, R.; et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur. Heart J. 2022, 43, 561–632. [Google Scholar] [CrossRef] [PubMed]
- Kempfert, J.; van Linden, A.; Linke, A.; Borger, M.A.; Rastan, A.; Mukherjee, C.; Ender, J.; Schuler, G.; Mohr, F.W.; Walther, T. Transapical off-pump valve-in-valve implantation in patients with degenerated aortic xenografts. Ann. Thorac. Surg. 2010, 89, 1934–1941. [Google Scholar] [CrossRef]
- Walther, T.; Falk, V.; Dewey, T.; Kempfert, J.; Emrich, F.; Pfannmüller, B.; Bröske, P.; Borger, M.A.; Schuler, G.; Mack, M.; et al. Valve-in-a-valve concept for transcatheter minimally invasive repeat xenograft implantation. J. Am. Coll. Cardiol. 2007, 50, 56–60. [Google Scholar] [CrossRef]
- Cribier, A.; Eltchaninoff, H.; Bash, A.; Borenstein, N.; Tron, C.; Bauer, F.; Derumeaux, G.; Anselme, F.; Laborde, F.; Leon, M.B. Percutaneous transcatheter implantation of an aortic valve prosthesis for calcific aortic stenosis: First human case description. Circulation 2002, 106, 3006–3008. [Google Scholar] [CrossRef]
- Wilbring, M.; Alexiou, K.; Tugtekin, S.M.; Arzt, S.; Ibrahim, K.; Matschke, K.; Kappert, U. Pushing the limits-further evolutions of transcatheter valve procedures in the mitral position, including valve-in-valve, valve-in-ring, and valve-in-native-ring. J. Thorac. Cardiovasc. Surg. 2014, 147, 210–219. [Google Scholar] [CrossRef] [PubMed]
- Wilbring, M.; Alexiou, K.; Tugtekin, S.M.; Sill, B.; Hammer, P.; Schmidt, T.; Simonis, G.; Matschke, K.; Kappert, U. Transapical transcatheter valve-in-valve implantation for deteriorated mitral valve bioprostheses. Ann. Thorac. Surg. 2013, 95, 111–117. [Google Scholar] [CrossRef] [PubMed]
- Cheung, A.; Webb, J.G.; Wong, D.R.; Ye, J.; Masson, J.-B.; Carere, R.G.; Lichtenstein, S.V. Transapical transcatheter mitral valve-in-valve implantation in a human. Ann. Thorac. Surg. 2009, 87, e18–e20. [Google Scholar] [CrossRef] [PubMed]
- Speiser, U.; Pohling, D.; Tugtekin, S.-M.; Charitos, E.; Matschke, K.; Wilbring, M. Redo surgery for noninfective isolated mitral valve disease: Initial outcome and further follow-up compared to primary surgery. J. Card. Surg. 2022, 37, 1990–1997. [Google Scholar] [CrossRef] [PubMed]
- Yoon, S.-H.; Whisenant, B.K.; Bleiziffer, S.; Delgado, V.; Schofer, N.; Eschenbach, L.; Fujita, B.; Sharma, R.; Ancona, M.; Yzeiraj, E.; et al. Transcatheter Mitral Valve Replacement for Degenerated Bioprosthetic Valves and Failed Annuloplasty Rings. J. Am. Coll. Cardiol. 2017, 70, 1121–1131. [Google Scholar] [CrossRef] [PubMed]
- Dvir, D.; Webb, J.G.; Bleiziffer, S.; Pasic, M.; Waksman, R.; Kodali, S.; Barbanti, M.; Latib, A.; Schaefer, U.; Rodés-Cabau, J.; et al. Transcatheter aortic valve implantation in failed bioprosthetic surgical valves. JAMA 2014, 312, 162–170. [Google Scholar] [CrossRef] [PubMed]
- Yoon, S.-H.; Whisenant, B.K.; Bleiziffer, S.; Delgado, V.; Dhoble, A.; Schofer, N.; Eschenbach, L.; Bansal, E.; Murdoch, D.J.; Ancona, M.; et al. Outcomes of transcatheter mitral valve replacement for degenerated bioprostheses, failed annuloplasty rings, and mitral annular calcification. Eur. Heart J. 2019, 40, 441–451. [Google Scholar] [CrossRef] [PubMed]
- Simonato, M.; Whisenant, B.; Ribeiro, H.B.; Webb, J.G.; Kornowski, R.; Guerrero, M.; Wijeysundera, H.; Søndergaard, L.; de Backer, O.; Villablanca, P.; et al. Transcatheter Mitral Valve Replacement after Surgical Repair or Replacement: Comprehensive Midterm Evaluation of Valve-in-Valve and Valve-in-Ring Implantation from the VIVID Registry. Circulation 2021, 143, 104–116. [Google Scholar] [CrossRef] [PubMed]
- Iung, B.; Delgado, V.; Rosenhek, R.; Price, S.; Prendergast, B.; Wendler, O.; de Bonis, M.; Tribouilloy, C.; Evangelista, A.; Bogachev-Prokophiev, A.; et al. Contemporary Presentation and Management of Valvular Heart Disease: The EURObservational Research Programme Valvular Heart Disease II Survey. Circulation 2019, 140, 1156–1169. [Google Scholar] [CrossRef] [PubMed]
- Stone, G.W.; Adams, D.H.; Abraham, W.T.; Kappetein, A.P.; Généreux, P.; Vranckx, P.; Mehran, R.; Kuck, K.-H.; Leon, M.B.; Piazza, N.; et al. Clinical trial design principles and endpoint definitions for transcatheter mitral valve repair and replacement: Part 2: Endpoint definitions: A consensus document from the Mitral Valve Academic Research Consortium. Eur. Heart J. 2015, 36, 1878–1891. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, S.M.; Shahian, D.M.; Filardo, G.; Ferraris, V.A.; Haan, C.K.; Rich, J.B.; Normand, S.-L.T.; DeLong, E.R.; Shewan, C.M.; Dokholyan, R.S.; et al. The Society of Thoracic Surgeons 2008 cardiac surgery risk models: Part 2—Isolated valve surgery. Ann. Thorac. Surg. 2009, 88, S23–S42. [Google Scholar] [CrossRef] [PubMed]
- Nashef, S.A.M.; Roques, F.; Sharples, L.D.; Nilsson, J.; Smith, C.; Goldstone, A.R.; Lockowandt, U. EuroSCORE II. Eur. J. Cardiothorac. Surg. 2012, 41, 734–744; discussion 744–745. [Google Scholar] [CrossRef] [PubMed]
- R Development Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020. [Google Scholar]
- Guerrero, M.; Vemulapalli, S.; Xiang, Q.; Wang, D.D.; Eleid, M.; Cabalka, A.K.; Sandhu, G.; Salinger, M.; Russell, H.; Greenbaum, A.; et al. Thirty-Day Outcomes of Transcatheter Mitral Valve Replacement for Degenerated Mitral Bioprostheses (Valve-in-Valve), Failed Surgical Rings (Valve-in-Ring), and Native Valve With Severe Mitral Annular Calcification (Valve-in-Mitral Annular Calcification) in the United States: Data from the Society of Thoracic Surgeons/American College of Cardiology/Transcatheter Valve Therapy Registry. Circ. Cardiovasc. Interv. 2020, 13, e008425. [Google Scholar] [CrossRef] [PubMed]
- Hu, J.; Chen, Y.; Cheng, S.; Zhang, S.; Wu, K.; Wang, W.; Zhou, Y. Transcatheter mitral valve implantation for degenerated mitral bioprostheses or failed surgical annuloplasty rings: A systematic review and meta-analysis. J. Card. Surg. 2018, 33, 508–519. [Google Scholar] [CrossRef] [PubMed]
- Wan, S.; Lee, A.P.W.; Jin, C.-N.; Wong, R.H.L.; Chan, H.H.M.; Ng, C.S.H.; Wan, I.Y.P.; Underwood, M.J. The choice of mitral annuloplastic ring-beyond “surgeon’s preference”. Ann. Cardiothorac. Surg. 2015, 4, 261–265. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Valve-in-Valve (n = 25) | Valve-in-Ring (n = 29) | p-Value | |
|---|---|---|---|
| Age (years) | 77.4 ± 6.3 | 75.8 ± 6.7 | 0.35 |
| Gender male | 13 (52.0%) | 17 (58.6%) | 0.83 |
| BMI (kg/m2) | 25.4 ± 4.5 | 28.1 ± 5.5 | 0.08 |
| Arterial hypertension | 24 (96.0%) | 27 (93.1%) | 1.00 |
| Diabetes mellitus | 9 (36.0%) | 11 (37.9%) | 1.00 |
| Dyslipidemia | 16 (64.0%) | 20 (69.0%) | 0.92 |
| Coronary artery disease | 15 (60.0%) | 19 (65.5%) | 0.89 |
| Chronic obstructive lung disease | 6 (24.0%) | 4 (13.8%) | 0.49 |
| Pulmonary arterial hypertension | |||
| None | 4 (16.0%) | 6 (20.7%) | |
| Moderate | 7 (28.0%) | 16 (55.2%) | 0.06 |
| Severe | 14 (56.0%) | 7 (24.1%) | |
| Chronic kidney disease | 21 (84.0%) | 29 (100%) | 0.04 |
| Preoperative dialysis | 1 (4.0%) | 1 (3.4%) | 1.00 |
| GFR (ml/min) | 53.0 ± 21.2 | 44.5 ± 19.0 | 0.12 |
| Peripheral arterial disease | 6 (24.0%) | 4 (13.8%) | 0.49 |
| History of stroke | 0.54 | ||
| None | 21 (84.0%) | 27 (93.1%) | |
| TIA | 2 (8.0%) | 1 (3.4%) | |
| Stroke | 2 (8.0%) | 1 (3.4%) | |
| Atrial fibrillation | 20 (80.0%) | 24 (82.8%) | 1.00 |
| Preoperative pacemaker | 5 (20.0%) | 20 (69.0%) | <0.001 |
| NYHA Class | 0.04 | ||
| I | 3 (12.0%) | 0 (0%) | |
| II | 3 (12.0%) | 0 (0%) | |
| III | 15 (60.0%) | 21 (72.4%) | |
| IV | 4 (16.0%) | 8 (27.6%) | |
| EuroSCORE II (%) | 11.5 ± 7.5 | 16.9 ± 9.0 | <0.01 |
| STS-PROM score (%) | 5.9 ± 3.7 | 8.7 ± 4.3 | <0.01 |
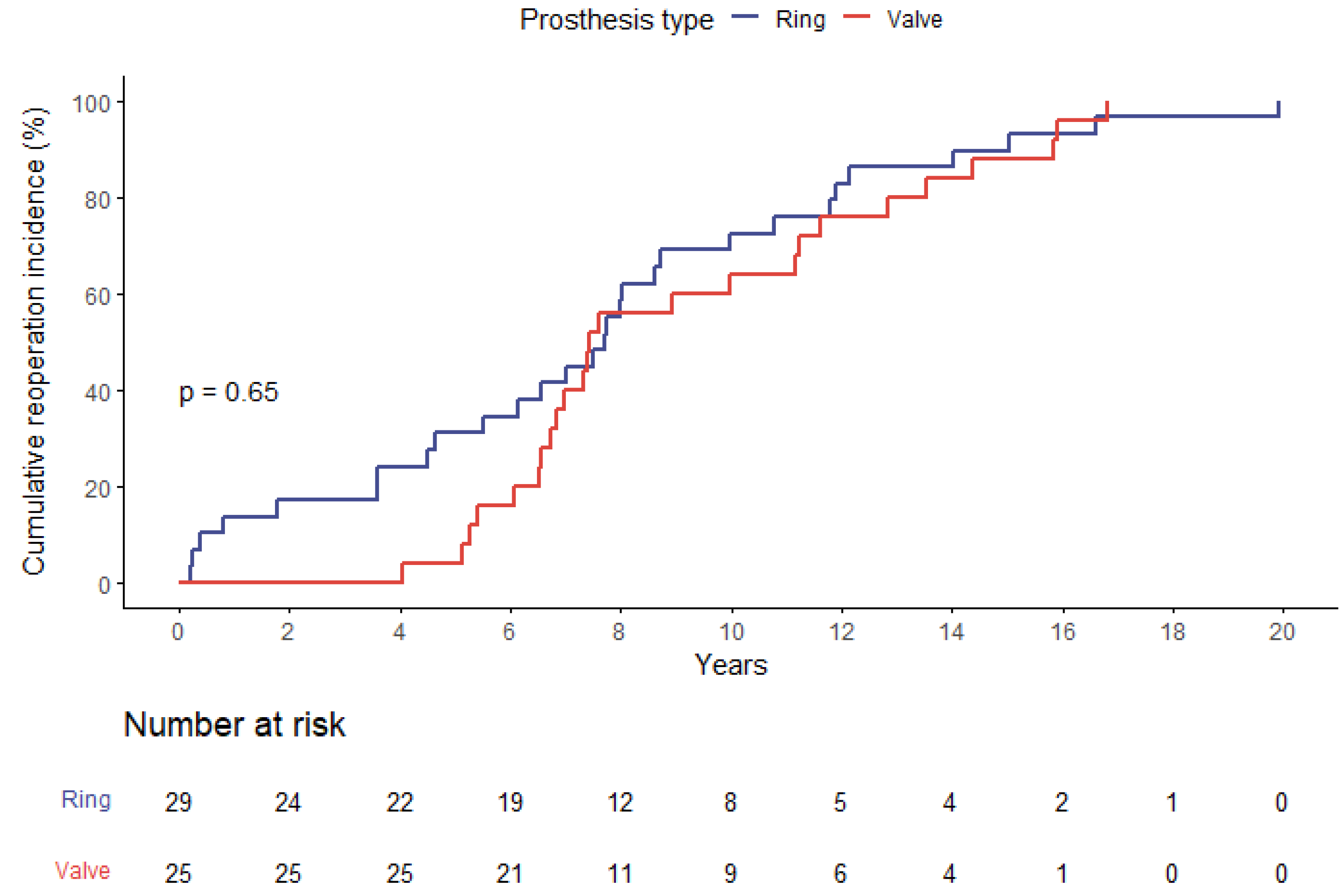
| Years since index operation | 9.3 ± 3.8 | 7.7 ± 5.0 | 0.200 |
| Initial operation for endocarditis | 7 (28.0%) | 0 (0%) | <0.01 |
| Initial operation indication | <0.001 | ||
| Structural mitral disease | 21 (84.0%) | 8 (27.6%) | |
| Functional mitral disease | 4 (16.0%) | 21 (72.4%) | |
| History of coronary bypass | 6 (24.0%) | 7 (24.1%) | 1.000 |
| Size of initial prosthesis (mm) | 29.7 ± 1.1 | 28.4 ± 1.5 | <0.001 |
| Valve-in-Valve (n = 25) | Valve-in-Ring (n = 29) | p-Value | |
|---|---|---|---|
| Ejection fraction (%) | 53.6 ± 12.4 | 39.3 ± 15.1 | <0.001 |
| LVEDD (mm) | 49.1 ± 6.5 | 58.6 ± 7.8 | <0.001 |
| Right ventricular function | 0.56 | ||
| Normal | 8 (32.0%) | 9 (31.0%) | |
| Mildly reduced | 6 (24.0%) | 9 (31.0%) | |
| Moderately reduced | 9 (36.0%) | 7 (24.1%) | |
| Severely reduced | 2 (8.0%) | 4 (13.8%) | |
| Mitral regurgitation | 0.62 | ||
| None | 2 (8.0%) | 0 (0%) | |
| Mild | 1 (4.0%) | 2 (6.9%) | |
| Moderate | 3 (12.0%) | 3 (10.3%) | |
| Severe | 19 (76.0%) | 24 (82.8%) | |
| Mitral stenosis | <0.001 | ||
| None | 2 (8.0%) | 19 (65.5%) | |
| Mild | 7 (28.0%) | 4 (13.8%) | |
| Moderate | 8 (32.0%) | 3 (10.3%) | |
| Severe | 8 (32.0%) | 3 (10.3%) | |
| Mitral valve area (cm2) | 1.3 ± 0.6 | 2.4 ± 1.2 | 0.16 |
| Peak gradient (mmHg) | 27.4 ± 6.4 | 18.4 ± 6.6 | <0.001 |
| Mean gradient (mmHg) | 10.7 ± 3.5 | 6.3 ± 2.7 | <0.001 |
| Valve-in-Valve (n = 25) | Valve-in-Ring (n = 29) | p-Value | |
|---|---|---|---|
| Indication for redo procedure (according to the leading pathology) | 0.76 | ||
| Mitral regurgitation | 18 (72.0%) | 23 (79.3%) | |
| Mitral stenosis | 7 (28.0%) | 6 (20.7%) | |
| Access | 0.48 | ||
| Transapical | 22 (88.0%) | 22 (75.9%) | |
| Transfemoral | 3 (12.0%) | 6 (20.7%) | |
| Right anterolateral minithoracotomy (transatrial) | 0 (0%) | 1 (3.4%) | |
| Prosthesis model | 1 | ||
| 8 (32.0%) | 10 (34.5%) | |
| 17 (68.0%) | 19 (65.5%) | |
| Prosthesis labeled size (mm) | 27.9 ± 1.5 | 25.9 ± 1.7 | <0.001 |
| Surgery time (min) | 62.7 ± 34.7 | 73.9 ± 70.9 | 0.59 |
| Conversion | 0 (0%) | 2 (6.9%) | 0.49 |
| M-VARC procedural success a | 5 (20.0%) | 3 (10.3%) | 0.45 |
| Modified procedural success b | 18 (72.0%) | 20 (69.0%) | 1 |
| Mitral stenosis | <0.001 | ||
| None | 2 (8.0%) | 21 (72.4%) | |
| Mild | 15 (60.0%) | 7 (24.1%) | |
| Moderate | 8 (32.0%) | 1 (3.4%) | |
| Severe | 0 (0%) | 0 (0%) | |
| Mitral regurgitation | <0.001 | ||
| None | 18 (72.0%) | 5 (17.2%) | |
| Mild | 7 (28.0%) | 21 (72.4%) | |
| Moderate | 0 (0%) | 2 (6.9%) | |
| Severe | 0 (0%) | 1 (3.4%) | |
| Type of regurgitation | <0.001 | ||
| None | 21 (84.0%) | 5 (17.2%) | |
| Transvalvular | 1 (4.0%) | 4 (13.8%) | |
| Paravalvular | 3 (12.0%) | 19 (65.5%) | |
| Both | 0 (0%) | 1 (3.4%) | |
| LVOT obstruction | 1 (4.0%) | 2 (6.9%) | 1.00 |
| Valve-in-Valve (n = 25) | Valve-in-Ring (n = 29) | p-Value | |
|---|---|---|---|
| Pacemaker implantation | 0 (0%) | 1 (3.5%) | 1.00 |
| Acute kidney injury | 6 (24.0%) | 6 (20.7%) | 1.00 |
| New-onset dialysis | 1 (4.0%) | 5 (17.2%) | 0.20 |
| Wound-healing disorder | 0 (0%) | 0 (0%) | 1.00 |
| Sepsis | 2 (8.0%) | 3 (10.3%) | 1.00 |
| Stroke | 2 (8.0%) | 1 (3.4%) | 0.59 |
| TIA | 0 (0%) | 1 (3.4%) | 1.00 |
| CPR | 3 (12.0%) | 2 (6.9%) | 0.65 |
| Ventilation time | 1.00 | ||
| Under 12 h | 0 (0%) | 0 (0%) | |
| Under 24 h | 23 (92.0%) | 25 (86.2%) | |
| Over 24 h | 1 (4.0%) | 1 (3.4%) | |
| RBC transfusion (units) | 0.7 ± 2.0 | 2.3 ± 3.8 | 0.02 |
| ICU stay (days) | 3.8 ± 6.8 | 4.3 ± 6.3 | 0.96 |
| Hospital stay (days) | 9.9 ± 5.9 | 13.5 ± 8.0 | 0.13 |
| 30-day mortality | 1 (4.0%) | 2 (6.9%) | 1.00 |
| Overall mortality | |||
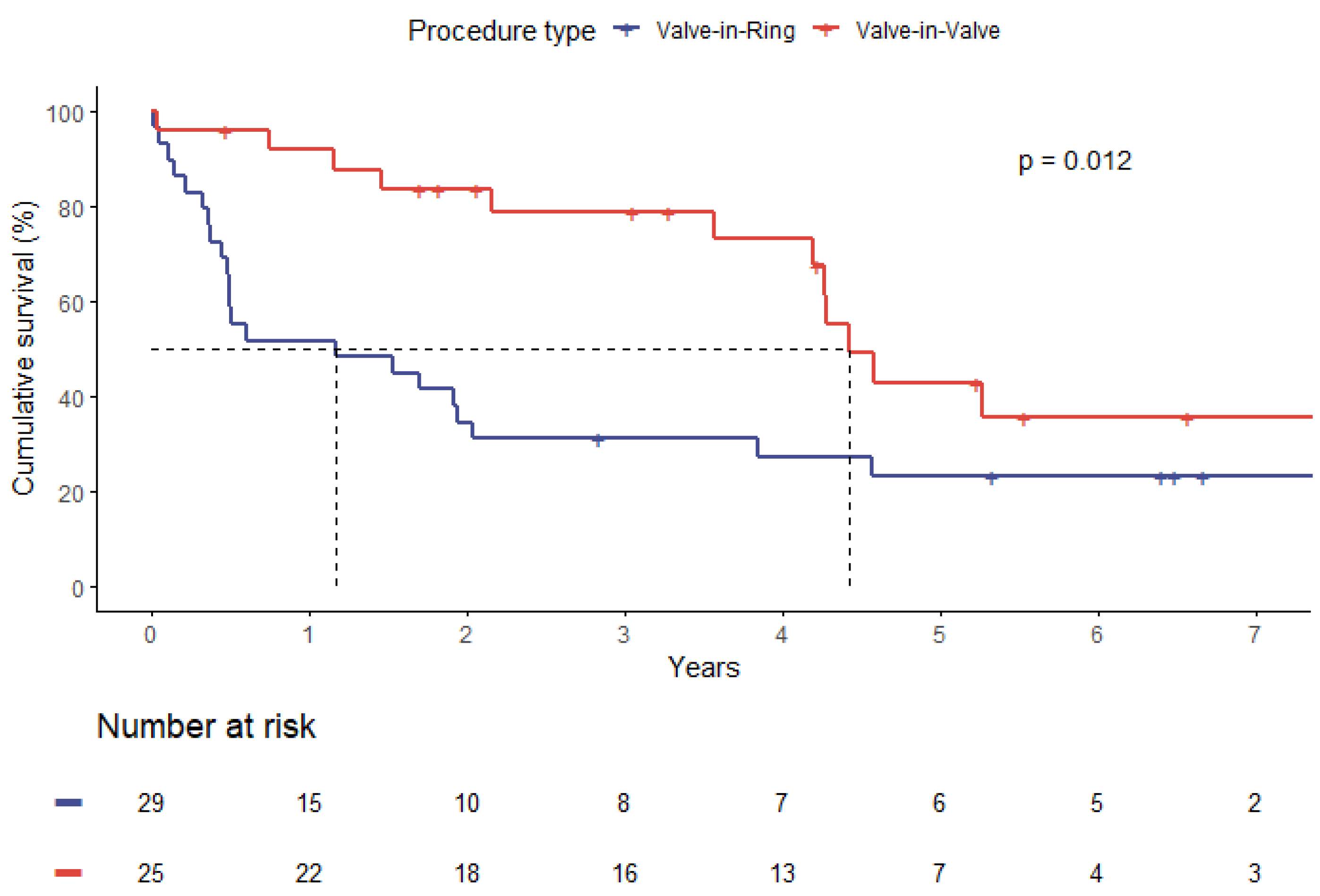
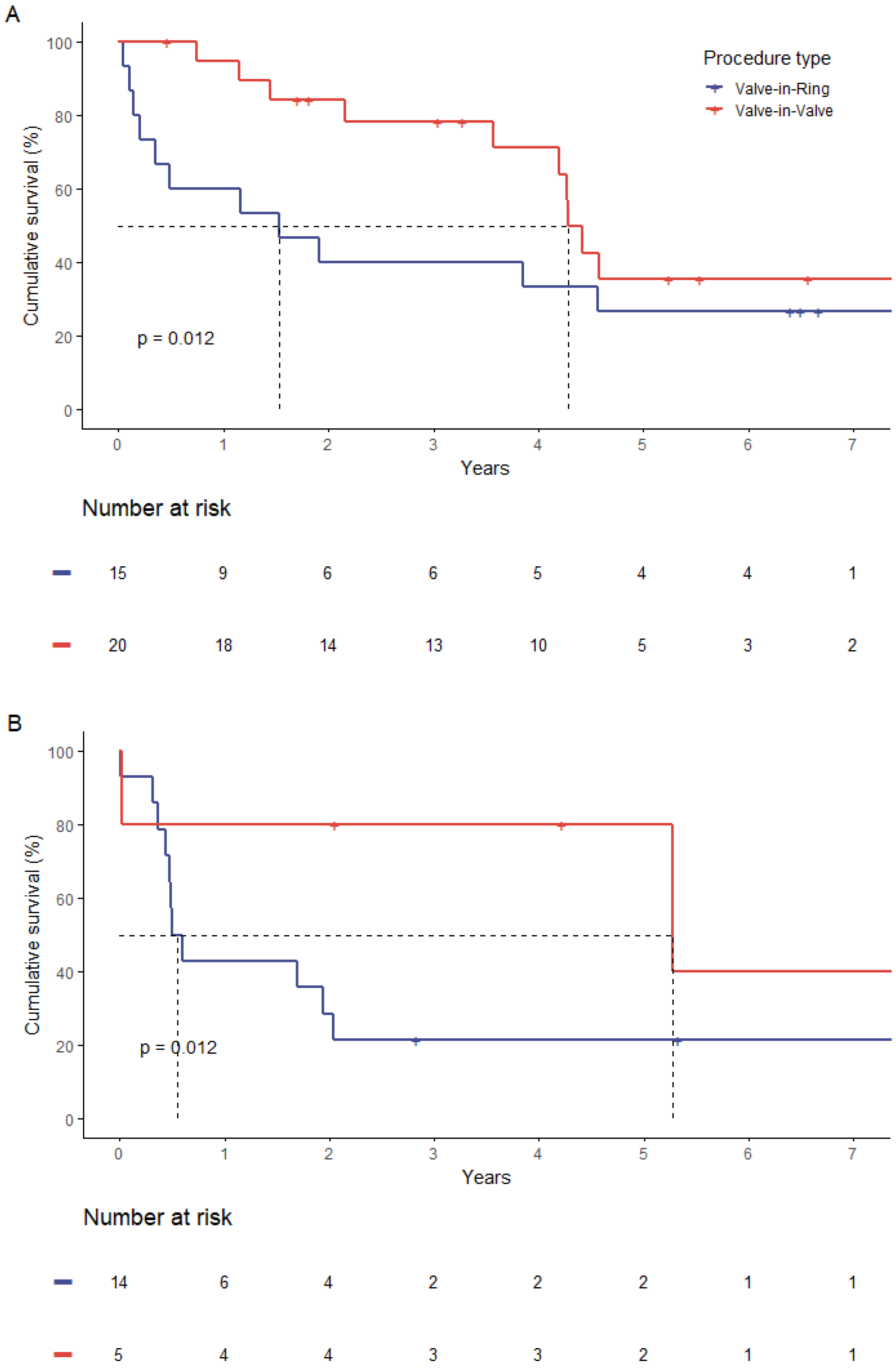
| Cardiac death | 5 (38.5%) | 12 (52.2%) | 0.66 |
| Median survival time (years) | 4.2 | 1.2 | 0.01 |
| Hazard Ratio | 95% CI | p | |
|---|---|---|---|
| STS-PROM | 1.07 | 0.99–1.15 | 0.08 |
| EuroSCORE II | 1.04 | 1.00–1.08 | 0.06 |
| Age | 1.02 | 0.97–1.08 | 0.38 |
| Sex (female) | 2.14 | 1.07–4.27 | 0.03 |
| BMI | 1.03 | 0.97–1.09 | 0.39 |
| Diabetes on insulin | 1.68 | 0.59–4.77 | 0.33 |
| COPD | 1.25 | 0.51–3.07 | 0.62 |
| Pulmonary hypertension | 2.13 | 0.75–6.06 | 0.16 |
| Chronic kidney disease | 1.65 | 0.83–3.26 | 0.15 |
| GFR | 0.99 | 0.97–1.00 | 0.14 |
| Peripheral vascular disease | 0.76 | 0.29–1.96 | 0.57 |
| Atrial fibrillation | 1.44 | 0.34–6.03 | 0.62 |
| Preoperative pacemaker | 1.77 | 0.92–3.43 | 0.09 |
| Type of valve disease (functional) | 1.55 | 0.80–3.00 | 0.19 |
| Type of heart failure (HFrEF) | 1.70 | 0.84–3.41 | 0.14 |
| Baseline LVEF | 0.98 | 0.96–1.00 | 0.10 |
| History of stroke | 1.12 | 0.46–2.7 | 0.80 |
| Time since initial operation | 1.07 | 0.99–1.16 | 0.11 |
| Procedure duration | 1.02 | 1.01–1.03 | <0.001 |
| Procedure type (ViR) | 2.36 | 1.19–4.67 | 0.01 |
| Valve size | 0.93 | 0.77–1.10 | 0.41 |
| Conversion to sternotomy | 29.33 | 4.82–178.4 | <0.001 |
| Transfemoral access | 2.06 | 0.95–4.46 | 0.06 |
| Hazard Ratio | 95% CI | p | |
|---|---|---|---|
| Sex (female) | 2.49 | 1.19–5.20 | 0.02 |
| Conversion to sternotomy | 22.49 | 3.47–145.92 | 0.001 |
| Procedure type (ViR) | 2.06 | 1.01–4.21 | 0.05 |
| EuroSCORE II | 1.06 | 1.07–1.11 | 0.03 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wilbring, M.; Petrov, A.; Arzt, S.; Eiselt, J.P.; Taghizadeh-Waghefi, A.; Matschke, K.; Kappert, U.; Alexiou, K. Long-Term Outcomes after Transcatheter Mitral Valve-in-Valve or Valve-in-Ring Procedures. J. Pers. Med. 2023, 13, 803. https://doi.org/10.3390/jpm13050803
Wilbring M, Petrov A, Arzt S, Eiselt JP, Taghizadeh-Waghefi A, Matschke K, Kappert U, Alexiou K. Long-Term Outcomes after Transcatheter Mitral Valve-in-Valve or Valve-in-Ring Procedures. Journal of Personalized Medicine. 2023; 13(5):803. https://doi.org/10.3390/jpm13050803
Chicago/Turabian StyleWilbring, Manuel, Asen Petrov, Sebastian Arzt, Julia Patricia Eiselt, Ali Taghizadeh-Waghefi, Klaus Matschke, Utz Kappert, and Konstantin Alexiou. 2023. "Long-Term Outcomes after Transcatheter Mitral Valve-in-Valve or Valve-in-Ring Procedures" Journal of Personalized Medicine 13, no. 5: 803. https://doi.org/10.3390/jpm13050803
APA StyleWilbring, M., Petrov, A., Arzt, S., Eiselt, J. P., Taghizadeh-Waghefi, A., Matschke, K., Kappert, U., & Alexiou, K. (2023). Long-Term Outcomes after Transcatheter Mitral Valve-in-Valve or Valve-in-Ring Procedures. Journal of Personalized Medicine, 13(5), 803. https://doi.org/10.3390/jpm13050803