
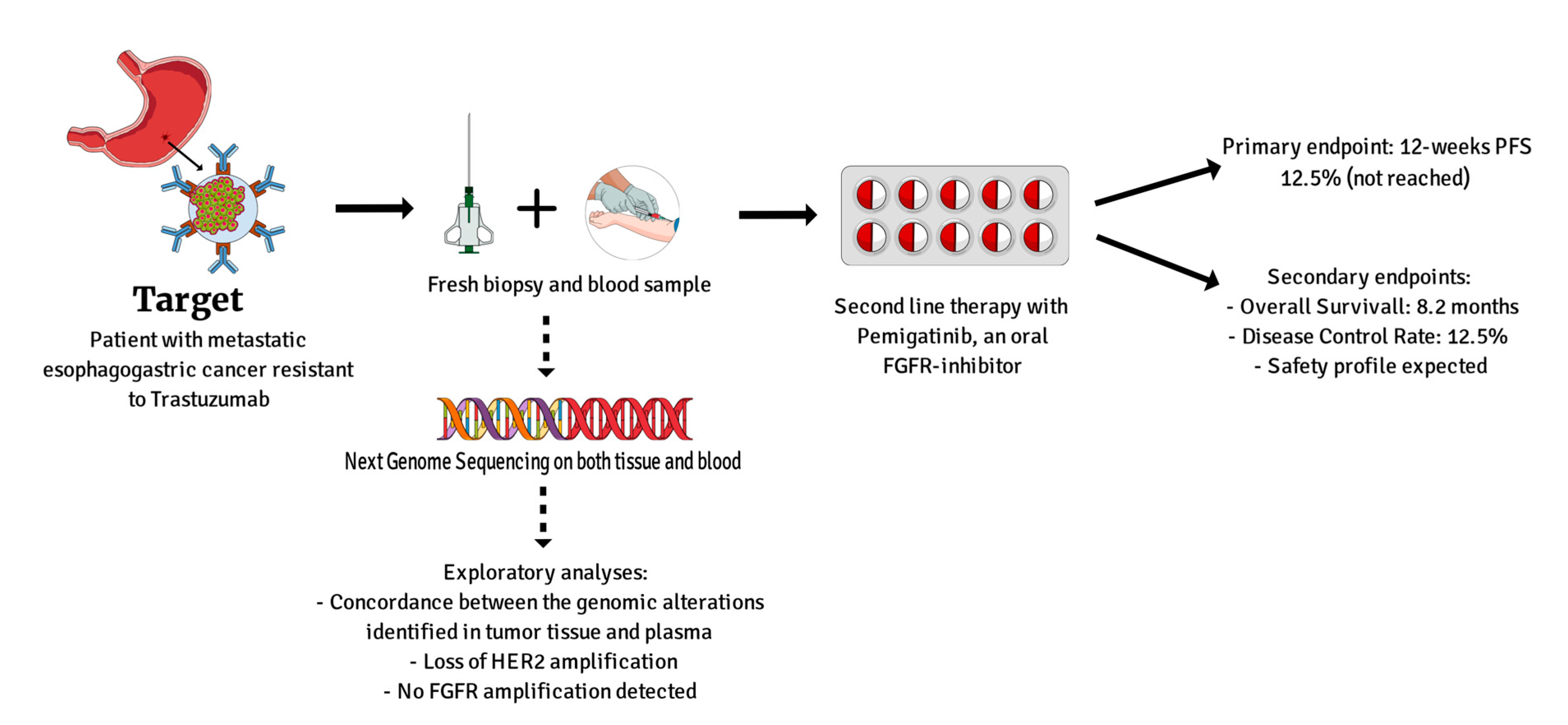
Targeting FGFR Pathway Is Not an Effective Therapeutic Strategy in Patients with Unselected Metastatic Esophagogastric Cancer Resistant to Trastuzumab

 , ,
, ,  , ,
, , 
Abstract

1. Introduction
2. Materials and Methods
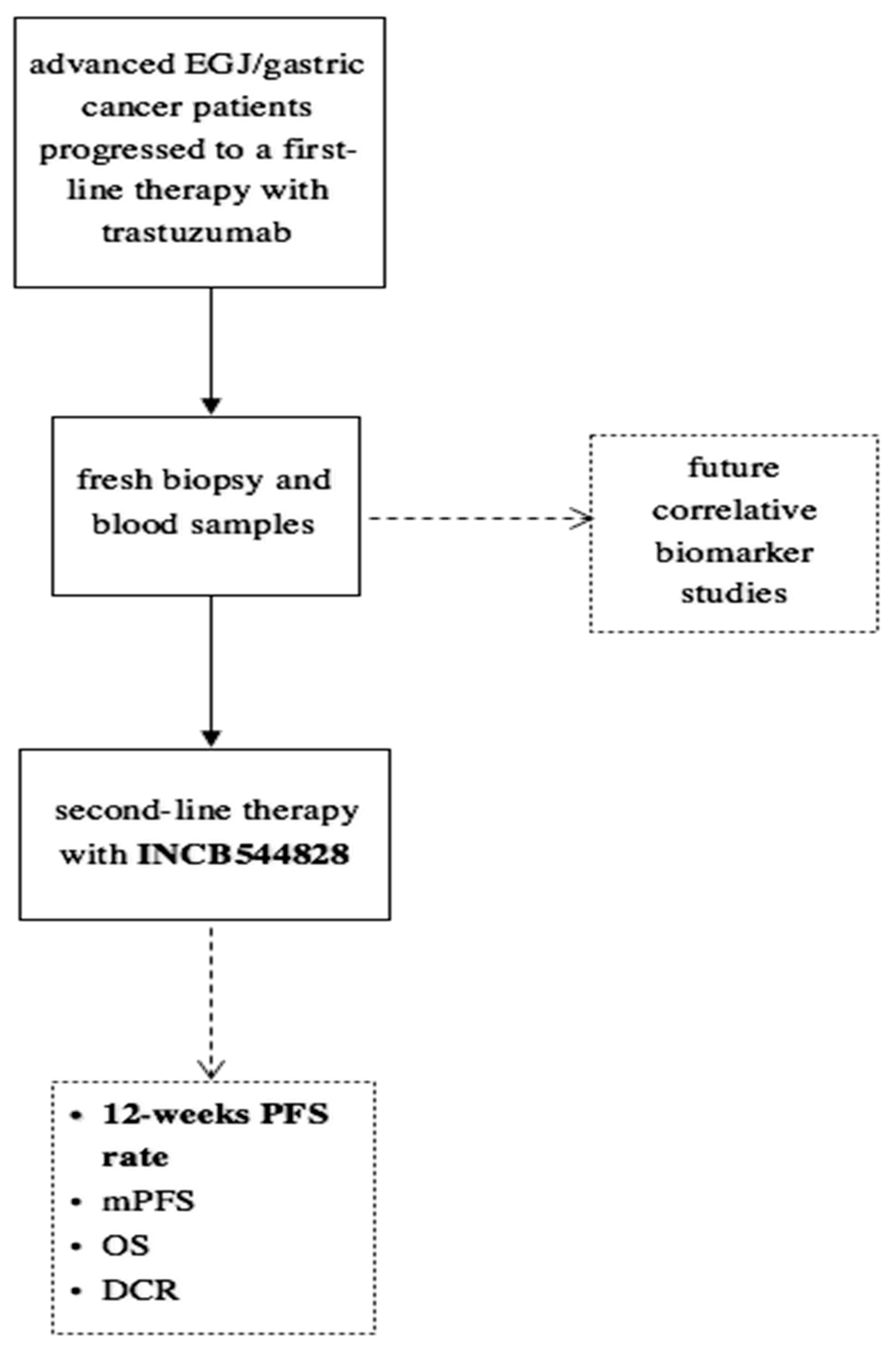
2.1. Patients
2.2. Study Treatment
2.3. End Points and Assessment
2.4. Statistical Design and Sample Size
2.5. Translational Research Analyses
3. Results
3.1. Patient Characteristics
3.2. Treatment Compliance and Safety
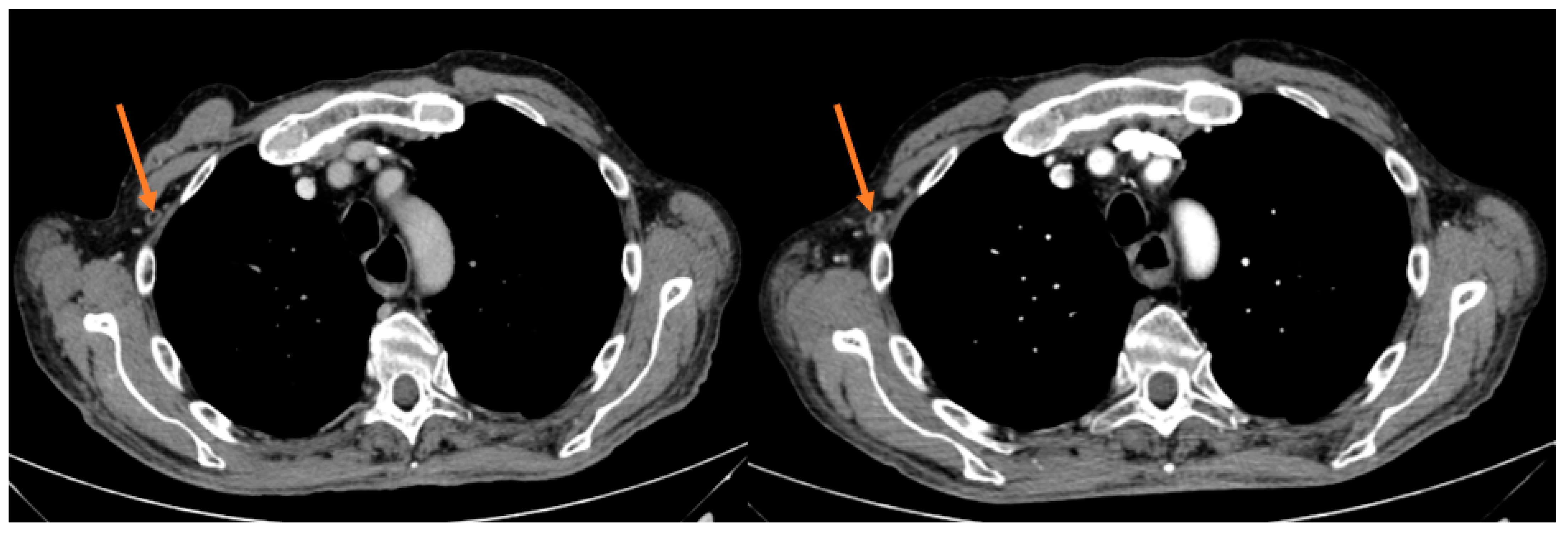
3.3. Activity
3.4. Translational Analyses
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA A Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Cancer Genome Atlas Research Network. Comprehensive molecular characterization of gastric adenocarcinoma. Nature 2014, 513, 202–209. [Google Scholar] [CrossRef]
- Bang, Y.J.; Van Cutsem, E.; Feyereislova, A.; Chung, H.C.; Shen, L.; Sawaki, A.; Lordick, F.; Ohtsu, A.; Omuro, Y.; Satoh, T.; et al. Trastuzumab in combination with chemotherapy versus chemotherapy alone for treatment of HER2-positive advanced gastric or gastro-oesophageal junction cancer (ToGA): A phase 3, open-label, randomised controlled trial. Lancet 2010, 376, 687–697. [Google Scholar] [CrossRef]
- Janjigian, Y.Y.; Sanchez-Vega, F.; Jonsson, P.; Chatila, W.K.; Hechtman, J.F.; Ku, G.Y.; Riches, J.C.; Tuvy, Y.; Kundra, R.; Bouvier, N.; et al. Genetic Predictors of Response to Systemic Therapy in Esophagogastric Cancer. Cancer Discov. 2018, 8, 49–58. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Vega, F.; Hechtman, J.F.; Castel, P.; Ku, G.Y.; Tuvy, Y.; Won, H.; Fong, C.J.; Bouvier, N.; Nanjangud, G.J.; Soong, J.; et al. EGFR and MET Amplifications Determine Response to HER2 Inhibition in ERBB2-Amplified Esophagogastric Cancer. Cancer Discov. 2019, 9, 199–209. [Google Scholar] [CrossRef] [PubMed]
- Touat, M.; Ileana, E.; Postel-Vinay, S.; Andre, F.; Soria, J.C. Targeting FGFR Signaling in Cancer. Clin. Cancer Res. 2015, 21, 2684–2694. [Google Scholar] [CrossRef] [PubMed]
- Piro, G.; Carbone, C.; Cataldo, I.; Di Nicolantonio, F.; Giacopuzzi, S.; Aprile, G.; Simionato, F.; Boschi, F.; Zanotto, M.; Mina, M.M.; et al. An FGFR3 Autocrine Loop Sustains Acquired Resistance to Trastuzumab in Gastric Cancer Patients. Clin. Cancer Res. 2016, 22, 6164–6175. [Google Scholar] [CrossRef]
- Merz, V.; Zecchetto, C.; Melisi, D. Pemigatinib, a potent inhibitor of FGFRs for the treatment of cholangiocarcinoma. Future Oncol. 2020, 17, 389–402. [Google Scholar] [CrossRef]
- Merz, V.; Zecchetto, C.; Simionato, F.; Cavaliere, A.; Casalino, S.; Pavarana, M.; Giacopuzzi, S.; Bencivenga, M.; Tomezzoli, A.; Santoro, R.; et al. A phase II trial of the FGFR inhibitor pemigatinib in patients with metastatic esophageal-gastric junction/gastric cancer trastuzumab resistant: The FiGhTeR trial. Ther. Adv. Med. Oncol. 2020, 12, 1758835920937889. [Google Scholar] [CrossRef] [PubMed]
- Simon, R. Optimal two-stage designs for phase II clinical trials. Control Clin. Trials 1989, 10, 1–10. [Google Scholar] [CrossRef]
- Nakamura, Y.; Kawazoe, A.; Lordick, F.; Janjigian, Y.Y.; Shitara, K. Biomarker-targeted therapies for advanced-stage gastric and gastro-oesophageal junction cancers: An emerging paradigm. Nat. Rev. Clin. Oncol. 2021, 18, 473–487. [Google Scholar] [CrossRef] [PubMed]
- Cancer Genome Atlas Research Network; Analysis Working Group: Asan University; BC Cancer Agency; Brigham and Women’s Hospital; Broad Institute; Brown University; Case Western Reserve University; Dana-Farber Cancer Institute; Duke University; Greater Poland Cancer Centre; et al. Integrated genomic characterization of oesophageal carcinoma. Nature 2017, 541, 169–175. [Google Scholar] [CrossRef] [PubMed]
- Klempner, S.J.; Madison, R.; Pujara, V.; Ross, J.S.; Miller, V.A.; Ali, S.M.; Schrock, A.B.; Kim, S.T.; Maron, S.B.; Dayyani, F.; et al. FGFR2-Altered Gastroesophageal Adenocarcinomas Are an Uncommon Clinicopathologic Entity with a Distinct Genomic Landscape. Oncologist 2019, 24, 1462–1468. [Google Scholar] [CrossRef] [PubMed]
- Maron, S.B.; Chase, L.M.; Lomnicki, S.; Kochanny, S.; Moore, K.L.; Joshi, S.S.; Landron, S.; Johnson, J.; Kiedrowski, L.A.; Nagy, R.J.; et al. Circulating Tumor DNA Sequencing Analysis of Gastroesophageal Adenocarcinoma. Clin. Cancer Res. 2019, 25, 7098–7112. [Google Scholar] [CrossRef] [PubMed]
- Deng, N.; Goh, L.K.; Wang, H.; Das, K.; Tao, J.; Tan, I.B.; Zhang, S.; Lee, M.; Wu, J.; Lim, K.H.; et al. A comprehensive survey of genomic alterations in gastric cancer reveals systematic patterns of molecular exclusivity and co-occurrence among distinct therapeutic targets. Gut 2012, 61, 673–684. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.S.; Liu, Z.X.; Lu, Y.X.; Bao, H.; Wu, X.; Zeng, Z.L.; Liu, Z.; Zhao, Q.; He, C.Y.; Lu, J.H.; et al. Liquid biopsies to track trastuzumab resistance in metastatic HER2-positive gastric cancer. Gut 2019, 68, 1152–1161. [Google Scholar] [CrossRef]
- Ulaganathan, V.K.; Sperl, B.; Rapp, U.R.; Ullrich, A. Germline variant FGFR4 p.G388R exposes a membrane-proximal STAT3 binding site. Nature 2015, 528, 570–574. [Google Scholar] [CrossRef]
- Abou-Alfa, G.K.; Sahai, V.; Hollebecque, A.; Vaccaro, G.; Melisi, D.; Al-Rajabi, R.; Paulson, A.S.; Borad, M.J.; Gallinson, D.; Murphy, A.G.; et al. Pemigatinib for previously treated, locally advanced or metastatic cholangiocarcinoma: A multicentre, open-label, phase 2 study. Lancet Oncol. 2020, 21, 671–684. [Google Scholar] [CrossRef]
- Seo, S.; Ryu, M.H.; Park, Y.S.; Ahn, J.Y.; Park, Y.; Park, S.R.; Ryoo, B.Y.; Lee, G.H.; Jung, H.Y.; Kang, Y.K. Loss of HER2 positivity after anti-HER2 chemotherapy in HER2-positive gastric cancer patients: Results of the GASTric cancer HER2 reassessment study 3 (GASTHER3). Gastric Cancer Off. J. Int. Gastric Cancer Assoc. Jpn. Gastric Cancer Assoc. 2019, 22, 527–535. [Google Scholar] [CrossRef] [PubMed]
- Guo, X.; Liang, X.; Wang, Y.; Cheng, A.; Zhang, H.; Qin, C.; Wang, Z. Significance of Tumor Mutation Burden Combined With Immune Infiltrates in the Progression and Prognosis of Advanced Gastric Cancer. Front. Genet. 2021, 12, 642608. [Google Scholar] [CrossRef] [PubMed]
- Wainberg, Z.A.; Enzinger, P.C.; Kang, Y.-K.; Yamaguchi, K.; Qin, S.; Lee, K.-W.; Oh, S.C.; Li, J.; Turk, H.M.; Teixeira, A.C.; et al. Randomized double-blind placebo-controlled phase 2 study of bemarituzumab combined with modified FOLFOX6 (mFOLFOX6) in first-line (1L) treatment of advanced gastric/gastroesophageal junction adenocarcinoma (FIGHT). J. Clin. Oncol. 2021, 39, 160. [Google Scholar] [CrossRef]
- Pearson, A.; Smyth, E.; Babina, I.S.; Herrera-Abreu, M.T.; Tarazona, N.; Peckitt, C.; Kilgour, E.; Smith, N.R.; Geh, C.; Rooney, C.; et al. High-Level Clonal FGFR Amplification and Response to FGFR Inhibition in a Translational Clinical Trial. Cancer Discov. 2016, 6, 838–851. [Google Scholar] [CrossRef] [PubMed]
- Quinzii, A.; Zecchetto, C.; Casalino, S.; Gaule, M.; Pesoni, C.; Merz, V.; Contarelli, S.; Pietrobono, S.; Benhadji, K.A.; Melisi, D. Clinical Response to Futibatinib in Patients with High-Level FGFR2-Amplified Advanced Gastric Cancer: Two Case Reports. Clin. Drug Investig. 2022, 42, 697–701. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Characteristics | n = 8 |
|---|---|
| Gender | |
| Male | 7 (88%) |
| Female | 1 (12%) |
| Age, median (range) | 65.0 (CI 95% 51.6–78.4) |
| Performance status (ECOG) | |
| 0 | 6 (75%) |
| 1 | 2 (25%) |
| Adverse Events | n = 8 Grade 1–2 | Grade 3 |
|---|---|---|
| Any | 8 (100%) | 0 |
| Hyperphosphataemia | 7 (87.5%) | 0 |
| Fatigue | 3 (37.5%) | 0 |
| Diarrhea | 2 (25%) | 0 |
| Mucositis | 1 (12.5%) | 0 |
| Hypercreatininemia | 1 (12.5%) | 0 |
| Category | n = 8 | % (95% CI) |
|---|---|---|
| Best overall response at first CT-scan | ||
| Partial response | 1 | 12.50% |
| Stable disease | 1 | 12.50% |
| Progression disease | 6 | 75 |
| 12-week PFS rate | ||
| Stable disease | 1 | 12.50% |
| Progression disease | 7 | 87.50% |
| Progression-Free Survival (months) | 2.1 | 1.1–3.1 |
| Disease control rate | 1 | 12.50% |
| Median Overall Survival (months) | 8.2 | 4.9–11.5 |
| Patient ID | IHC HER2/AMP | IHC FGFR1-3 | NGS Solid | NGS Liquid |
|---|---|---|---|---|
| 001 | 3+/− | 1+, 2−, 3− | Insufficient tumor sample | TMB medium MSI stable KRAS 5 copies TP53 p.P72R c.215C>G BRCA1 p.K1183R c.3548A>G CCND3 p.S259A c.775T>G RICTOR 2 copies PDGFRA p.G79D c.236G>A TP53 p.D281N c841G>A |
| 002 | 3+/+ | 1−, 2−, 3+ | TMB medium MSI stable ERRB2 39 copies FGFR4 p.G388R c.1162G>A KDR p.Q472H c.1416A>T TP53 p.G266E c.797G>A KRAS p.Q61H c.183A>C ATM p.5707P c.2119T>C | TMB medium MSI stable ERRB2 9 copies FGFR4 p.G388R c.1162G>A KDR p.Q472H c.1416A>T TP53 p.P72R c.215C>G ASXL1 p.L815P c.2444T>C CCND3 p.S259A c.775T>G TP53 p.G266E c.797G>A KRAS p.Q61H c.183A>C ATM p.5707P c.2119T>C PIK3CA p.E726K c.2176G>A |
| 003 | 3+/+ | 1−, 2−, 3++ | TMB medium MSI stable ERRB2 73 copies EGFR 3 copies TP53 p.P72R c.215C>G PALB2 p.L939W c.2816T>G | TMB high (37.4 muts/Mb) MSI stable ERBB2 21 copies ASXL1 p.L815P c.2444T>C TP53 p.P72R c.215C>G PALB2 p.L939W c.2816T>G BRCA1 p.K1183R c.2816T>G PPM1D p.S468* c.1403C>G GNAQ p.Y101*c.303C>A CHEK2 p.Y488*c.1464C>A |
| 004 | 3+/− | 1−, 2−, 3− | TMB low MSI stable CDK4 3 copy number FGFR4 p.G388R c.1162G>A BRCA1 p.K1183R c.3548A>G APC p.I1307K c.3920T>A CDKN2A p.H83D c.247C>G TP53 p.L130H c.389T>A TP53 p.R273P c.818G>C | TMB low MSI stable FGFR4 p.G388R c.1162G>A BRCA1 p.K1183R c.3548A>G APC p.I1307K c.3920T>A ASXL1 p.L815P c.2444T>C CCND3 p.5259° c.775T>G |
| 005 | 3+/− | 1−, 2−, 3− | Insufficient tumor sample | TMB low MSI stable BRCA1 p.K1183R c.3548A>G TP53 p.P72R c.215C>G FGFR4 p.G388R c.1162G>A KDR p.Q472H c.1416A>T ASXL1 p.L815P c.2444T>C CCND3 p.S259A c.775T>G SLX4 p.N1834S c.5501A>G DNM3A p.E616 c.1846G>T |
| 006 | 3+/− | 1−, 2−, 3− | TMB low MSI stable ERBB2 11 copies TP53 p.C275Vfs c.823delT TP53 p.P72R c.215C>G KDR p.Q472H c.1416A>T PIK3CA p.R93W c.277C>T | TMB low MSI stable ERBB2 3 copies TP53 p.C275Vfs c.823delT TP53 p.P72R c.215C>G KDR p.Q472H c.1416A>T PIK3CA p.R93W c.277C>T ASXL1 p.L815P c.2444T>C KIT p.M541L c.1621A>C SMC1A p.R711Q c.2132G>A DNMT3A p.R598 c.1792C>T |
| 007 | 3+/− | Insufficient tumor sample | Insufficient tumor sample | TMB high 25.5 Muts/Mb MSI stable ERBB2 6 copies TP53 p.P72R c.215C>G BRCA1 p.K1183R c.3548A>G ASXL1 p.L815P c.2444T>C KIT p.M541L c.1621A>C CCND3 p.S259A c.775T>G TP53 p.G244D c.731G>A TP53 p.C275Y c.824G>A TP53 p.Y220C c659A>G CREBBP p.A981T c.2941G>A |
| 008 | 3+/− | Insufficient tumor sample | Insufficient tumor sample | TMB high 20.0 Muts/Mb MSI stable ERBB2 2 copies TP53 p.P72R c.215C>G BRCA1 p.K1183R c.3548A>G FGFR4 p.G388R c.1162G>A ASXL1 p.L815P c.2444T>C KIT p.M541L c.1621A>C CCND3 p.S259A c.775T>G TP53 p.C238Y c.713G>A TP53 p.R158H c473G>A CHEK2 p.R180Q c.539G>A |
| Genomic Alterations | n = 8 |
|---|---|
| TP53 p.P72R c.215C>G | 7 (87.5%) |
| ASXL1 p.L815P c.2444T>C | 7 (87.5%) |
| CCND3 p.S259A c.775T>G | 6 (75%) |
| BRCA1 p.K1183R c.3548A>G | 5 (62.5%) |
| FGFR4 p.G388R c.1162G>A | 4 (50%) |
| KDR p.Q472H c.1416A>T | 3 (37.5%) |
| KIT p.M541L c.1621A>C | 3 (37.5%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zecchetto, C.; Quinzii, A.; Casalino, S.; Gaule, M.; Pesoni, C.; Merz, V.; Pietrobono, S.; Mangiameli, D.; Pasquato, M.; Milleri, S.; et al. Targeting FGFR Pathway Is Not an Effective Therapeutic Strategy in Patients with Unselected Metastatic Esophagogastric Cancer Resistant to Trastuzumab. J. Pers. Med. 2023, 13, 508. https://doi.org/10.3390/jpm13030508
Zecchetto C, Quinzii A, Casalino S, Gaule M, Pesoni C, Merz V, Pietrobono S, Mangiameli D, Pasquato M, Milleri S, et al. Targeting FGFR Pathway Is Not an Effective Therapeutic Strategy in Patients with Unselected Metastatic Esophagogastric Cancer Resistant to Trastuzumab. Journal of Personalized Medicine. 2023; 13(3):508. https://doi.org/10.3390/jpm13030508
Chicago/Turabian StyleZecchetto, Camilla, Alberto Quinzii, Simona Casalino, Marina Gaule, Camilla Pesoni, Valeria Merz, Silvia Pietrobono, Domenico Mangiameli, Martina Pasquato, Stefano Milleri, and et al. 2023. "Targeting FGFR Pathway Is Not an Effective Therapeutic Strategy in Patients with Unselected Metastatic Esophagogastric Cancer Resistant to Trastuzumab" Journal of Personalized Medicine 13, no. 3: 508. https://doi.org/10.3390/jpm13030508
APA StyleZecchetto, C., Quinzii, A., Casalino, S., Gaule, M., Pesoni, C., Merz, V., Pietrobono, S., Mangiameli, D., Pasquato, M., Milleri, S., Giacopuzzi, S., Bencivenga, M., Tomezzoli, A., de Manzoni, G., & Melisi, D. (2023). Targeting FGFR Pathway Is Not an Effective Therapeutic Strategy in Patients with Unselected Metastatic Esophagogastric Cancer Resistant to Trastuzumab. Journal of Personalized Medicine, 13(3), 508. https://doi.org/10.3390/jpm13030508