
Differences and Similarities in Empathy Deficit and Its Neural Basis between Logopenic and Amnesic Alzheimer’s Disease

 , , , ,
, , , ,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Neuropsychological Evaluation, Empathy, and Facial Emotion Recognition Assessment
2.3. Apolipoprotein E (APOE) Genotyping
2.4. Amyloidosis and Neurodegeneration Biomarkers Analysis
2.5. FDG-PET Brain Imaging
2.6. Statistical Analysis
2.7. SPM Analysis
2.8. Data Availability
3. Results
3.1. Demographic Features and Biomarkers Analysis
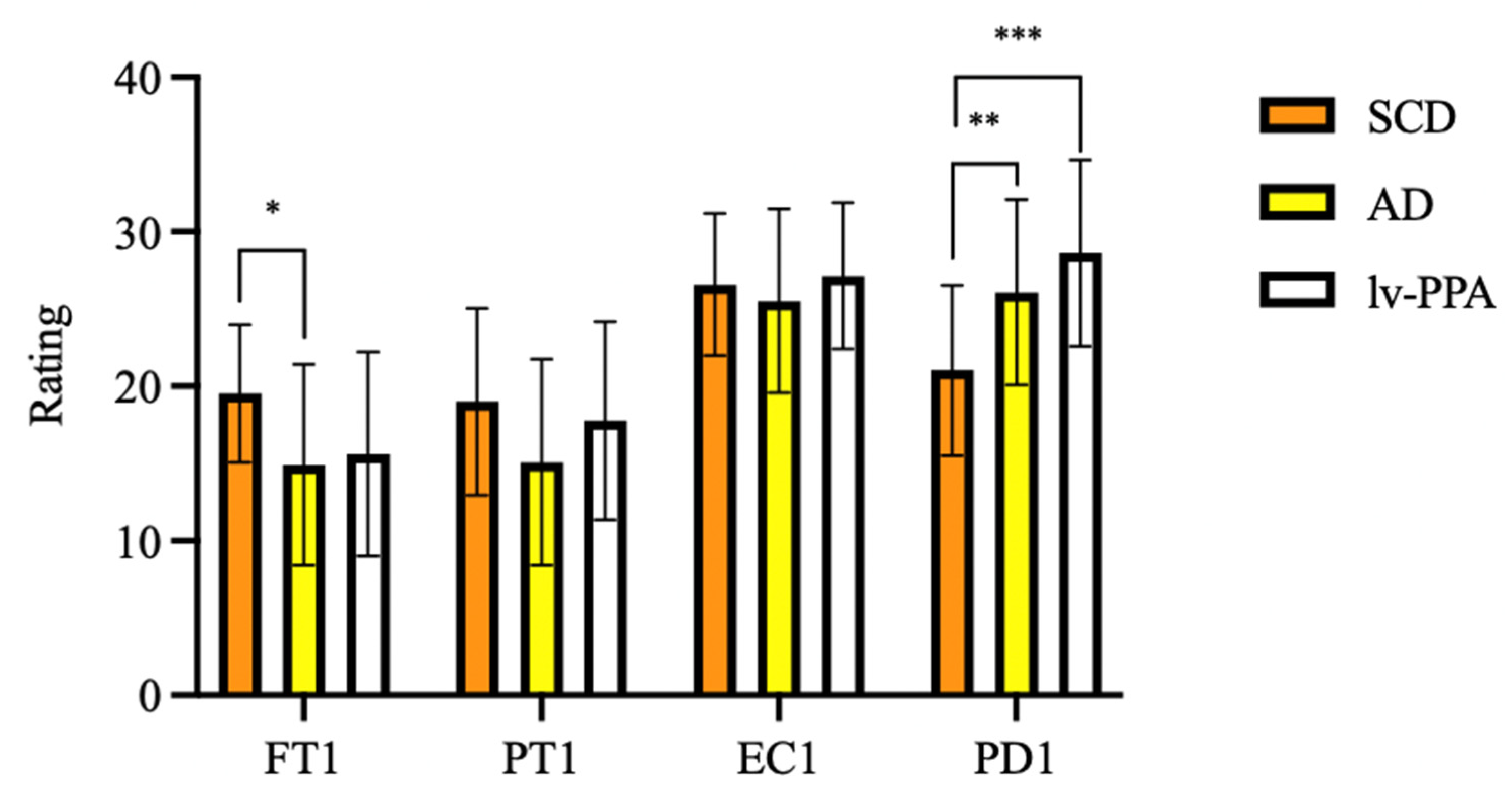
3.2. IRI Empathy Results
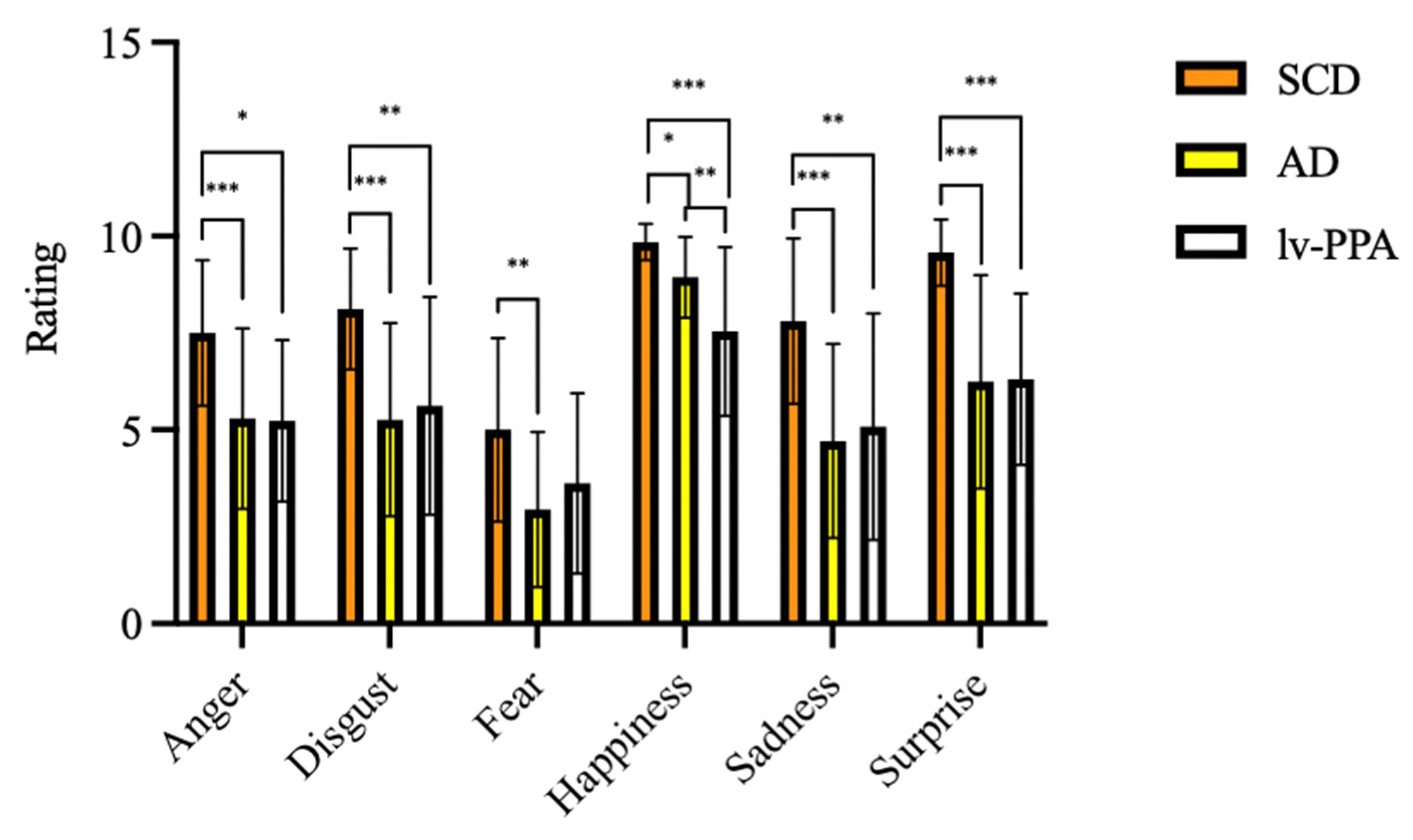
3.3. EK-60 F Emotion Recognition Results
3.4. Correlations between Demographic Data, Neuropsychological Variables, Empathy, and Emotion Recognition
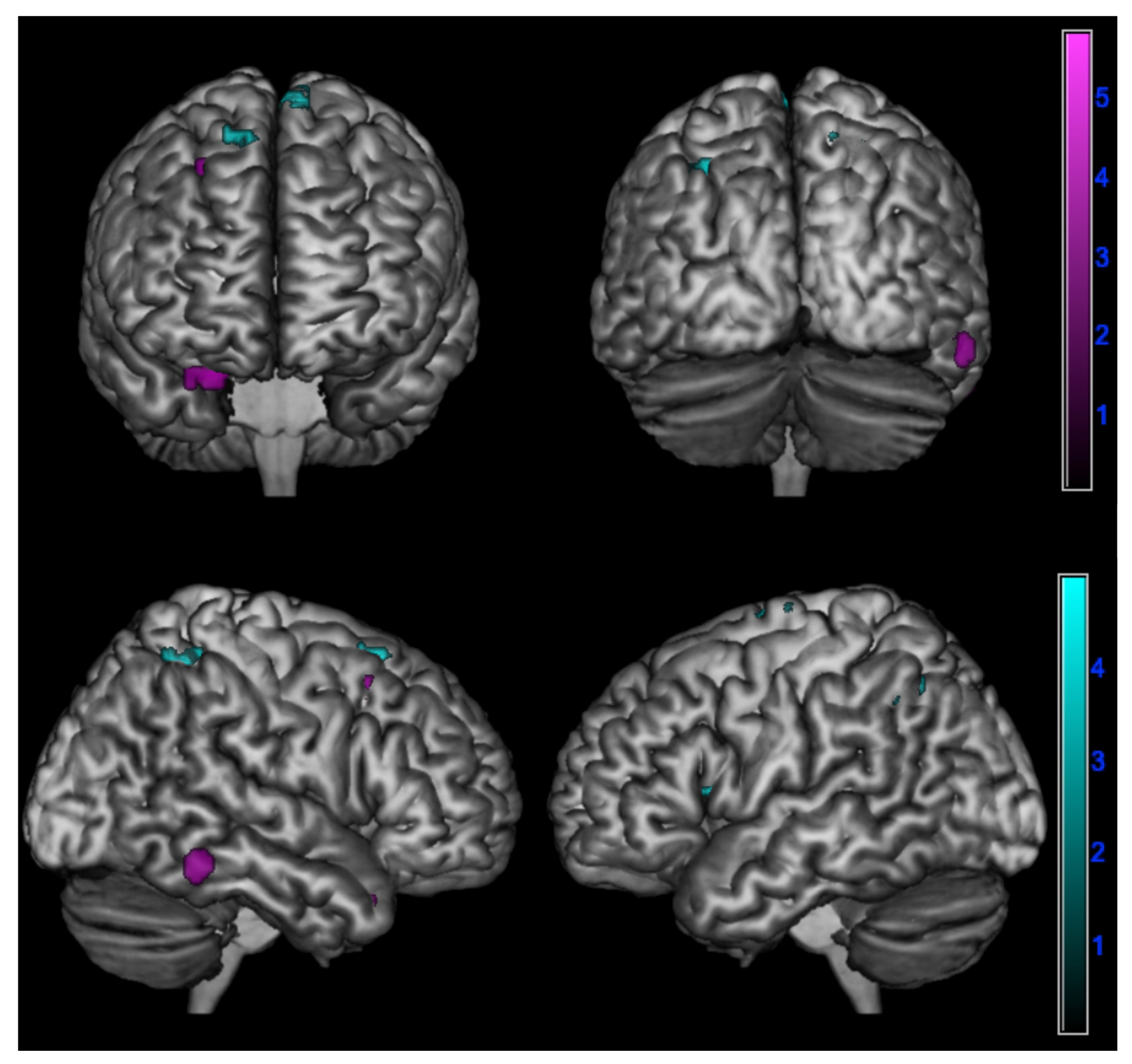
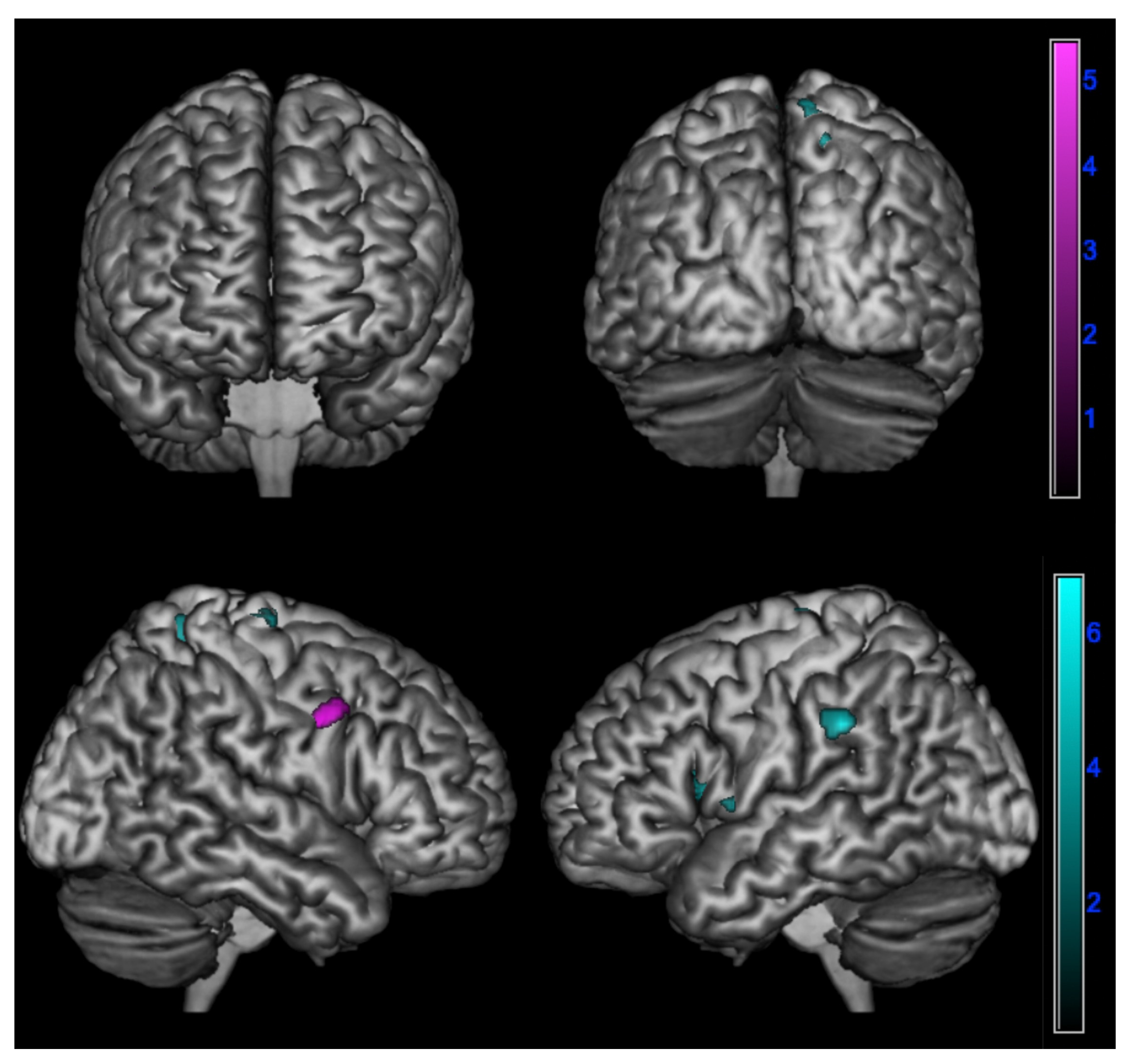
3.5. SPM Results
- In amnesic AD in the right superior temporal gyrus, fusiform gyrus, and middle frontal gyrus (p < 0.005);
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bartochowski, Z.; Gatla, S.; Khoury, R.; Al-Dahhak, R.; Grossberg, G.T. Empathy changes in neurocognitive disorders: A review. Ann. Clin. Psychiatry 2018, 30, 220–232. [Google Scholar] [PubMed]
- Bernhardt, B.C.; Singer, T. The neural basis of empathy. Annu. Rev. Neurosci. 2012, 35, 1–23. [Google Scholar] [CrossRef] [PubMed]
- Decety, J.; Jackson, P.L. The functional architecture of human empathy. Behav. Cogn. Neurosci. Rev. 2004, 3, 71–100. [Google Scholar] [CrossRef]
- Rankin, K.P.; Kramer, J.H.; Mychack, P.; Miller, B.L. Double dissociation of social functioning in frontotemporal dementia. Neurology 2003, 60, 266–271. [Google Scholar] [CrossRef] [PubMed]
- Cerami, C.; Dodich, A.; Iannaccone, S.; Marcone, A.; Lettieri, G.; Crespi, C.; Gianolli, L.; Cappa, S.F.; Perani, D. Right Limbic FDG-PET Hypometabolism Correlates with Emotion Recognition and Attribution in Probable Behavioral Variant of Frontotemporal Dementia Patients. PLoS ONE 2015, 10, e0141672. [Google Scholar] [CrossRef] [PubMed]
- Rascovsky, K.; Hodges, J.R.; Knopman, D.; Mendez, M.F.; Kramer, J.H.; Neuhaus, J.; van Swieten, J.C.; Seelaar, H.; Dopper, E.G.P.; Onyike, C.U.; et al. Sensitivity of revised diagnostic criteria for the behavioural variant of frontotemporal dementia. Brain 2011, 134, 2456–2477. [Google Scholar] [CrossRef]
- Fischer, A.; Landeira-Fernandez, J.; Sollero de Campos, F.; Mograbi, D.C. Empathy in Alzheimer’s Disease: Review of Findings and Proposed Model. J. Alzheimers Dis. 2019, 69, 921–933. [Google Scholar] [CrossRef]
- Giacomucci, G.; Galdo, G.; Polito, C.; Berti, V.; Padiglioni, S.; Mazzeo, S.; Chiaro, E.; De Cristofaro, M.T.; Bagnoli, S.; Nacmias, B.; et al. Unravelling neural correlates of empathy deficits in Subjective Cognitive Decline, Mild Cognitive Impairment and Alzheimer’s Disease. Behav. Brain Res. 2022, 428, 113893. [Google Scholar] [CrossRef]
- Gorno-Tempini, M.L.; Hillis, A.E.; Weintraub, S.; Kertesz, A.; Mendez, M.; Cappa, S.F.; Ogar, J.M.; Rohrer, J.D.; Black, S.; Boeve, B.F.; et al. Classification of primary progressive aphasia and its variants. Neurology 2011, 76, 1006–1014. [Google Scholar] [CrossRef]
- Fittipaldi, S.; Ibanez, A.; Baez, S.; Manes, F.; Sedeno, L.; Garcia, A.M. More than words: Social cognition across variants of primary progressive aphasia. Neurosci. Biobehav. Rev. 2019, 100, 263–284. [Google Scholar] [CrossRef]
- Gallese, V. Before and below “theory of mind”: Embodied simulation and the neural correlates of social cognition. Philos. Trans. R. Soc. Lond. B Biol. Sci. 2007, 362, 659–669. [Google Scholar] [CrossRef] [PubMed]
- Adolfi, F.; Couto, B.; Richter, F.; Decety, J.; Lopez, J.; Sigman, M.; Manes, F.; Ibáñez, A. Convergence of interoception, emotion, and social cognition: A twofold fMRI meta-analysis and lesion approach. Cortex 2017, 88, 124–142. [Google Scholar] [CrossRef]
- Binney, R.J.; Henry, M.L.; Babiak, M.; Pressman, P.S.; Santos-Santos, M.A.; Narvid, J.; Mandelli, M.L.; Strain, P.J.; Miller, B.L.; Rankin, K.P.; et al. Reading words and other people: A comparison of exception word, familiar face and affect processing in the left and right temporal variants of primary progressive aphasia. Cortex 2016, 82, 147–163. [Google Scholar] [CrossRef]
- Irish, M.; Kumfor, F.; Hodges, J.R.; Piguet, O. A tale of two hemispheres: Contrasting socioemotional dysfunction in right- versus left-lateralised semantic dementia. Dement. Neuropsychol. 2013, 7, 88–95. [Google Scholar] [CrossRef] [PubMed]
- Hazelton, J.L.; Irish, M.; Hodges, J.R.; Piguet, O.; Kumfor, F. Cognitive and Affective Empathy Disruption in Non-Fluent Primary Progressive Aphasia Syndromes. Brain Impair. 2017, 18, 117–129. [Google Scholar] [CrossRef]
- Piguet, O.; Leyton, C.E.; Gleeson, L.D.; Hoon, C.; Hodges, J.R. Memory and emotion processing performance contributes to the diagnosis of non-semantic primary progressive aphasia syndromes. J. Alzheimers Dis. 2015, 44, 541–547. [Google Scholar] [CrossRef]
- McKhann, G.M.; Knopman, D.S.; Chertkow, H.; Hyman, B.T.; Jack, C.R.; Kawas, C.H.; Klunk, W.E.; Koroshetz, W.J.; Manly, J.J.; Mayeux, R.; et al. The diagnosis of dementia due to Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011, 7, 263–269. [Google Scholar] [CrossRef]
- Davis, M.H. Measuring individual differences in empathy: Evidence for a multidimensional approach. J. Personal. Soc. Psychol. 1983, 44, 113–126. [Google Scholar] [CrossRef]
- Albiero, P.; Lo Coco, A.; Ingoglia, S. Contributo all’adattamento italiano dell’Interpersonal Reactivity Index. Test. Psicometria Metodol. 2007, 13, 107–125. [Google Scholar]
- Ekman, P.; Friesen, W. Pictures of Facial Affect; Consulting Psychologists Press: Palo Alto, CA, USA, 1976. [Google Scholar]
- Dodich, A.; Cerami, C.; Canessa, N.; Crespi, C.; Marcone, A.; Arpone, M.; Realmuto, S.; Cappa, S.F. Emotion recognition from facial expressions: A normative study of the Ekman 60-Faces Test in the Italian population. Neurol. Sci. 2014, 35, 1015–1021. [Google Scholar] [CrossRef]
- Jessen, F.; Amariglio, R.E.; van Boxtel, M.; Breteler, M.; Ceccaldi, M.; Chételat, G.; Dubois, B.; Dufouil, C.; Ellis, K.A.; van der Flier, W.M.; et al. Subjective Cognitive Decline Initiative (SCD-I) Working Group A conceptual framework for research on subjective cognitive decline in preclinical Alzheimer’s disease. Alzheimers Dement. 2014, 10, 844–852. [Google Scholar] [CrossRef] [PubMed]
- Bracco, L.; Amaducci, L.; Pedone, D.; Bino, G.; Lazzaro, M.P.; Carella, F.; D’Antona, R.; Gallato, R.; Denes, G. Italian Multicentre Study on Dementia (SMID): A neuropsychological test battery for assessing Alzheimer’s disease. J. Psychiatr. Res. 1990, 24, 213–226. [Google Scholar] [CrossRef]
- Carlesimo, G.; Buccione, I.; Fadda, L.; Graceffa, A.; Mauri, M.; Lorusso, S.; Bevilacqua, G.; Caltagirone, C. Normative data of two memory tasks: Short-Story recall and Rey’s Figure. Nuova Riv. Neurol. 2002, 12, 1–13. [Google Scholar]
- Spinnler, H.; Tognoni, G. Standardizzazione e Taratura Italiana di Test Neuropsicologici: Gruppo Italiano per lo Studio Neuropsicologico Dell’invecchiamento; Masson Italia Periodici: Milano, Italy, 1987. [Google Scholar]
- Caffarra, P.; Vezzadini, G.; Dieci, F.; Zonato, F.; Venneri, A. Rey-Osterrieth complex figure: Normative values in an Italian population sample. Neurol. Sci. 2002, 22, 443–447. [Google Scholar] [CrossRef] [PubMed]
- Baddeley, A.; Della Sala, S.; Papagno, C.; Spinnler, H. Dual-task performance in dysexecutive and nondysexecutive patients with a frontal lesion. Neuropsychology 1997, 11, 187–194. [Google Scholar] [CrossRef]
- Giovagnoli, A.R.; Del Pesce, M.; Mascheroni, S.; Simoncelli, M.; Laiacona, M.; Capitani, E. Trail making test: Normative values from 287 normal adult controls. Ital. J. Neurol. Sci. 1996, 17, 305–309. [Google Scholar] [CrossRef]
- Basso, A.; Capitani, E.; Laiacona, M. Raven’s coloured progressive matrices: Normative values on 305 adult normal controls. Funct. Neurol. 1987, 2, 189–194. [Google Scholar]
- Brazzelli, M.; Della Sala, S.; Laiacona, M. Calibration of the Italian version of the Rivermead Behavioural Memory Test: A test for the ecological evaluation of memory. Bollet. Psicol. Appl. 1993, 206, 33–42. [Google Scholar]
- Catricalà, E.; Gobbi, E.; Battista, P.; Miozzo, A.; Polito, C.; Boschi, V.; Esposito, V.; Cuoco, S.; Barone, P.; Sorbi, S.; et al. SAND: A Screening for Aphasia in NeuroDegeneration. Development and normative data. Neurol. Sci. 2017, 38, 1469–1483. [Google Scholar] [CrossRef]
- Capasso, R. Esame Neuropsicologico per l’Afasia—E.N.P.A.; Springer: Berlin/Heidelberg, Germany, 2001. [Google Scholar]
- Hamilton, M. A rating scale for depression. J. Neurol. Neurosurg. Psychiatry 1960, 23, 56–62. [Google Scholar] [CrossRef]
- Sturm, V.E.; Yokoyama, J.S.; Seeley, W.W.; Kramer, J.H.; Miller, B.L.; Rankin, K.P. Heightened emotional contagion in mild cognitive impairment and Alzheimer’s disease is associated with temporal lobe degeneration. Proc. Natl. Acad. Sci. USA 2013, 110, 9944–9949. [Google Scholar] [CrossRef] [PubMed]
- Rankin, K.P.; Gorno-Tempini, M.L.; Allison, S.C.; Stanley, C.M.; Glenn, S.; Weiner, M.W.; Miller, B.L. Structural anatomy of empathy in neurodegenerative disease. Brain 2006, 129, 2945–2956. [Google Scholar] [CrossRef] [PubMed]
- Sorbi, S.; Nacmias, B.; Forleo, P.; Latorraca, S.; Gobbini, I.; Bracco, L.; Piacentini, S.; Amaducci, L. ApoE allele frequencies in Italian sporadic and familial Alzheimer’s disease. Neurosci. Lett. 1994, 177, 100–102. [Google Scholar] [CrossRef] [PubMed]
- Alcolea, D.; Pegueroles, J.; Muñoz, L.; Camacho, V.; López-Mora, D.; Fernández-León, A.; Bastard, N.L.; Huyck, E.; Nadal, A.; Olmedo, V.; et al. Agreement of amyloid PET and CSF biomarkers for Alzheimer’s disease on Lumipulse. Ann. Clin. Transl. Neurol. 2019, 6, 1815–1824. [Google Scholar] [CrossRef] [PubMed]
- Minoshima, S.; Drzezga, A.E.; Barthel, H.; Bohnen, N.; Djekidel, M.; Lewis, D.H.; Mathis, C.A.; McConathy, J.; Nordberg, A.; Sabri, O.; et al. SNMMI Procedure Standard/EANM Practice Guideline for Amyloid PET Imaging of the Brain 1.0. J. Nucl. Med. 2016, 57, 1316–1322. [Google Scholar] [CrossRef] [PubMed]
- Jack, C.R.; Bennett, D.A.; Blennow, K.; Carrillo, M.C.; Dunn, B.; Haeberlein, S.B.; Holtzman, D.M.; Jagust, W.; Jessen, F.; Karlawish, J.; et al. NIA-AA Research Framework: Toward a biological definition of Alzheimer’s disease. Alzheimers Dement. 2018, 14, 535–562. [Google Scholar] [CrossRef]
- Varrone, A.; Asenbaum, S.; Vander Borght, T.; Booij, J.; Nobili, F.; Någren, K.; Darcourt, J.; Kapucu, Ö.L.; Tatsch, K.; Bartenstein, P.; et al. EANM procedure guidelines for PET brain imaging using [18F]F.D.G.; version 2. Eur. J. Nuclear Med. Mol. Imaging 2009, 36, 2103–2110. [Google Scholar] [CrossRef]
- Perani, D.; Della Rosa, P.A.; Cerami, C.; Gallivanone, F.; Fallanca, F.; Vanoli, E.G.; Panzacchi, A.; Nobili, F.; Pappatà, S.; Marcone, A.; et al. EADC-PET Consortium. Validation of an optimized SPM procedure for FDG-PET in dementia diagnosis in a clinical setting. Neuroimage Clin. 2014, 6, 445–454. [Google Scholar] [CrossRef]
- Dermody, N.; Wong, S.; Ahmed, R.; Piguet, O.; Hodges, J.R.; Irish, M. Uncovering the Neural Bases of Cognitive and Affective Empathy Deficits in Alzheimer’s Disease and the Behavioral-Variant of Frontotemporal Dementia. J. Alzheimers Dis. 2016, 53, 801–816. [Google Scholar] [CrossRef]
- Narme, P.; Mouras, H.; Roussel, M.; Devendeville, A.; Godefroy, O. Assessment of socioemotional processes facilitates the distinction between frontotemporal lobar degeneration and Alzheimer’s disease. J. Clin. Exp. Neuropsychol. 2013, 35, 728–744. [Google Scholar] [CrossRef]
- Bond, R.L.; Downey, L.E.; Weston, P.S.J.; Slattery, C.F.; Clark, C.N.; Macpherson, K.; Mummery, C.J.; Warren, J.D. Processing of Self versus Non-Self in Alzheimer’s Disease. Front. Hum. Neurosci. 2016, 10, 97. [Google Scholar] [CrossRef] [PubMed]
- Jessen, F.; Amariglio, R.E.; Buckley, R.F.; van der Flier, W.M.; Han, Y.; Molinuevo, J.L.; Rabin, L.; Rentz, D.M.; Rodriguez-Gomez, O.; Saykin, A.J.; et al. The characterisation of subjective cognitive decline. Lancet Neurol. 2020, 19, 271–278. [Google Scholar] [CrossRef] [PubMed]
- Pernigo, S.; Gambina, G.; Valbusa, V.; Condoleo, M.T.; Broggio, E.; Beltramello, A.; Moretto, G.; Moro, V. Behavioral and neural correlates of visual emotion discrimination and empathy in mild cognitive impairment. Behav. Brain Res. 2015, 294, 111–122. [Google Scholar] [CrossRef] [PubMed]
- Spoletini, I.; Marra, C.; Di Iulio, F.; Gianni, W.; Sancesario, G.; Giubilei, F.; Trequattrini, A.; Bria, P.; Caltagirone, C.; Spalletta, G. Facial Emotion Recognition Deficit in Amnestic Mild Cognitive Impairment and Alzheimer Disease. Am. J. Geriatr. Psychiatry 2008, 16, 389–398. [Google Scholar] [CrossRef]
- Weiss, E.M.; Kohler, C.G.; Vonbank, J.; Stadelmann, E.; Kemmler, G.; Hinterhuber, H.; Marksteiner, J. Impairment in Emotion Recognition Abilities in Patients With Mild Cognitive Impairment, Early and Moderate Alzheimer Disease Compared With Healthy Comparison Subjects. Am. J. Geriatr. Psychiatry 2008, 16, 974–980. [Google Scholar] [CrossRef]
- Pietschnig, J.; Aigner-Wöber, R.; Reischenböck, N.; Kryspin-Exner, I.; Moser, D.; Klug, S.; Auff, E.; Dal-Bianco, P.; Pusswald, G.; Lehrner, J. Facial emotion recognition in patients with subjective cognitive decline and mild cognitive impairment. Int. Psychogeriatr. 2016, 28, 477–485. [Google Scholar] [CrossRef] [PubMed]
- Johnen, A.; Reul, S.; Wiendl, H.; Meuth, S.G.; Duning, T. Apraxia profiles-A single cognitive marker to discriminate all variants of frontotemporal lobar degeneration and Alzheimer’s disease. Alzheimers Dement. 2018, 10, 363–371. [Google Scholar] [CrossRef] [PubMed]
- Multani, N.; Galantucci, S.; Wilson, S.M.; Shany-Ur, T.; Poorzand, P.; Growdon, M.E.; Jang, J.Y.; Kramer, J.H.; Miller, B.L.; Rankin, K.P.; et al. Emotion detection deficits and changes in personality traits linked to loss of white matter integrity in primary progressive aphasia. Neuroimage Clin. 2017, 16, 447–454. [Google Scholar] [CrossRef]
- Henry, J.D.; Ruffman, T.; McDonald, S.; O’Leary, M.-A.P.; Phillips, L.H.; Brodaty, H.; Rendell, P.G. Recognition of disgust is selectively preserved in Alzheimer’s disease. Neuropsychologia 2008, 46, 1363–1370. [Google Scholar] [CrossRef]
- Kim, H.; Han, S. Does personal distress enhance empathic interaction or block it? Personal. Individ. Differ. 2018, 124, 77–83. [Google Scholar] [CrossRef]
- Frith, U.; Frith, C.D. Development and neurophysiology of mentalizing. Philos. Trans. R. Soc. Lond. B 2003, 358, 459–473. [Google Scholar] [CrossRef] [PubMed]
- de Waal, F.B.M.; Preston, S.D. Mammalian empathy: Behavioural manifestations and neural basis. Nat. Rev. Neurosci. 2017, 18, 498–509. [Google Scholar] [CrossRef] [PubMed]
- Wong, C.; Gallate, J. The function of the anterior temporal lobe: A review of the empirical evidence. Brain Res. 2012, 1449, 94–116. [Google Scholar] [CrossRef] [PubMed]
- Miller, B.L.; Cummings, J.L. The Human Frontal Lobes: Third Edition: Functions and Disorders; Guilford Press: New York, NY, USA.
- Nejati, V.; Majdi, R.; Salehinejad, M.A.; Nitsche, M.A. The role of dorsolateral and ventromedial prefrontal cortex in the processing of emotional dimensions. Sci. Rep. 2021, 11, 1971. [Google Scholar] [CrossRef] [PubMed]
- Rizzolatti, G.; Sinigaglia, C. The mirror mechanism: A basic principle of brain function. Nat. Rev. Neurosci. 2016, 17, 757–765. [Google Scholar] [CrossRef]
- Rizzolatti, G.; Fabbri-Destro, M.; Cattaneo, L. Mirror neurons and their clinical relevance. Nat. Clin. Pract. Neurol. 2009, 5, 24–34. [Google Scholar] [CrossRef]
- Hennenlotter, A.; Schroeder, U.; Erhard, P.; Castrop, F.; Haslinger, B.; Stoecker, D.; Lange, K.W.; Ceballos-Baumann, A.O. A common neural basis for receptive and expressive communication of pleasant facial affect. Neuroimage 2005, 26, 581–591. [Google Scholar] [CrossRef]
- Wicker, B.; Keysers, C.; Plailly, J.; Royet, J.P.; Gallese, V.; Rizzolatti, G. Both of us disgusted in My insula: The common neural basis of seeing and feeling disgust. Neuron 2003, 40, 655–664. [Google Scholar] [CrossRef]
- Shamay-Tsoory, S.G. The neural bases for empathy. Neuroscientist 2011, 17, 18–24. [Google Scholar] [CrossRef]
- Yamada, M.; Decety, J. Unconscious affective processing and empathy: An investigation of subliminal priming on the detection of painful facial expressions. Pain 2009, 143, 71–75. [Google Scholar] [CrossRef]
- Rabinovici, G.D.; Rosen, H.J.; Alkalay, A.; Kornak, J.; Furst, A.J.; Agarwal, N.; Mormino, E.C.; O’Neil, J.P.; Janabi, M.; Karydas, A.; et al. Amyloid vs FDG-PET in the differential diagnosis of AD and FTLD. Neurology 2011, 77, 2034–2042. [Google Scholar] [CrossRef] [PubMed]
- Rabinovici, G.D.; Jagust, W.J.; Furst, A.J.; Ogar, J.M.; Racine, C.A.; Mormino, E.C.; O’Neil, J.P.; Lal, R.A.; Dronkers, N.F.; Miller, B.L.; et al. Abeta amyloid and glucose metabolism in three variants of primary progressive aphasia. Ann. Neurol. 2008, 64, 388–401. [Google Scholar] [CrossRef] [PubMed]
- Rankin, K.P.; Kramer, J.H.; Miller, B.L. Patterns of cognitive and emotional empathy in frontotemporal lobar degeneration. Cogn. Behav. Neurol. 2005, 18, 28–36. [Google Scholar] [CrossRef] [PubMed]
- Shany-Ur, T.; Poorzand, P.; Grossman, S.N.; Growdon, M.E.; Jang, J.Y.; Ketelle, R.S.; Miller, B.L.; Rankin, K.P. Comprehension of insincere communication in neurodegenerative disease: Lies, sarcasm, and theory of mind. Cortex 2012, 48, 1329–1341. [Google Scholar] [CrossRef]
- Singleton, E.H.; Fieldhouse, J.L.P.; van’t Hooft, J.J.; Scarioni, M.; van Engelen, M.-P.E.; Sikkes, S.A.M.; de Boer, C.; Bocancea, D.; van den Berg, E.; Scheltens, P.; et al. Social cognition deficits and biometric signatures in the behavioural variant of Alzheimer’s disease. Brain, 2022; awac382, ahead of print. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| SCD n = 31 | AD n = 38 | lv-PPA n = 18 | |
|---|---|---|---|
| Gender (M/F) | 4/27 *α | 17/21 * | 9/9 α |
| Age at onset (years) | 54.94 ± 10.08 βγ | 66.53 ± 6.71 β | 64.50 ± 7.60 γ |
| Age at empathy (years) | 65.61 ± 9.48 δ | 71.04 ± 7.33 δ | 68.65 ± 7.02 |
| Disease duration (years) | 9.62 ± 7.51 εη | 4.44 ± 3.59 ε | 2.87 ± 1.54 η |
| Family history of dementia | 22/6 θ | 16/17 θ | 6/11 |
| Years of education | 12.58 ± 3.40 ι | 9.80 ± 4.65 ικ | 13.22 ± 4.45 κ |
| MMSE | 27.43 ± 2.04 λμ | 17.03 ± 5.28 λ | 16.69 ± 6.37 μ |
| APOE ε4+ | 30.77% | 50.00% | 50.00% |
| A+/A− | 8/12 (40%) ν° | 30/0 (100%) ν | 18/0 (100%) ° |
| AD | lv-PPA | |||||
|---|---|---|---|---|---|---|
| Mean ± SD | z | p | Mean ± SD | z | p | |
| IRI 0 IRI 1 | 81.26 ± 13.31 81.95 ± 13.35 | −0.828 | 0.408 | 83.41 ± 11.12 83.76 ± 14.90 | −0.166 | 0.868 |
| FT 0 FT 1 | 17.11 ± 5.09 15.05 ± 6.21 | −2.464 | 0.014 | 17.18 ± 5.89 15.24 ± 6.21 | −1.574 | 0.115 |
| PT 0 PT 1 | 21.08 ± 6.15 15.42 ± 6.66 | −4.752 | <0.001 | 23.94 ± 6.40 15.82 ± 6.61 | −3.435 | 0.001 |
| EC 0 EC 1 | 26.39 ± 4.45 25.76 ± 5.70 | −1.185 | 0.236 | 25.94 ± 5.12 24.35 ± 6.47 | −1.250 | 0.211 |
| PD 0 PD 1 | 17.08 ± 4.99 26.03 ± 5.72 | −5.204 | <0.001 | 15.76 ± 5.47 28.35 ± 6.07 | −3.623 | <0.001 |
| SCD | AD | lv-PPA | F | p | p between SCD and AD | p between SCD and lv-PPA | p between AD and lv-PPA | |
|---|---|---|---|---|---|---|---|---|
| EK-60 F total score | 47.58 ± 5.14 | 33.29 ± 7.56 | 32.25 ± 8.09 | 42.863 | p < 0.001 | p < 0.001 | p < 0.001 | p = 1.000 |
| Execution time (seconds) | 290 ± 56.19 | 445.74 ± 124.03 | 425.08 ± 103.60 | 21.427 | p < 0.001 | p < 0.001 | p < 0.001 | p = 1.000 |
| Anger | 7.35 ± 1.80 | 5.29 ± 2.33 | 5.08 ± 2.11 | 9.480 | p < 0.001 | p = 0.001 | p = 0.006 | p = 1.000 |
| Disgust | 8.10 ± 1.45 | 5.26 ± 2.49 | 5.25 ± 2.60 | 16.134 | p < 0.001 | p < 0.001 | p = 0.001 | p = 1.000 |
| Fear | 5.10 ± 2.68 | 2.94 ± 2.00 | 3.67 ± 2.43 | 6.862 | p = 0.002 | p = 0.001 | p = 0.235 | p = 1.000 |
| Happiness | 9.84 ± 0.45 | 8.94 ± 1.043 | 7.33 ± 2.15 | 21.962 | p < 0.001 | p = 0.006 | p < 0.001 | p < 0.001 |
| Sadness | 7.97 ± 2.01 | 4.71 ± 2.51 | 4.75 ± 2.80 | 17.476 | p < 0.001 | p < 0.001 | p < 0.001 | p = 1.000 |
| Surprise | 9.48 ± 1.03 | 6.24 ± 2.75 | 6.17 ± 2.25 | 21.666 | p < 0.001 | p < 0.001 | p < 0.001 | p = 1.000 |
| Negative Correlation between ∆PT (PT-T0 - PT-T1) and Brain Metabolism | ||||||
| Cluster Extent | Talairach Coordinates (mm) | T Score | ||||
| x | y | z | ||||
| Amnesic AD | ||||||
| R Superior Temporal Gyrus | 130 | 32.0 | 16.0 | −24.0 | 4.90 | |
| R Middle Frontal Gyrus | 90 | 24.0 | 18.0 | 43.0 | 3.69 | |
| R Fusiform Gyrus | 67 | 57.0 | −43.0 | −8.0 | 3.38 | |
| lv-PPA | ||||||
| L Inferior Parietal Lobule | 138 | −30.0 | −50.0 | 45.0 | 4.95 | |
| L Superior Frontal Gyrus | 125 | −8.0 | −1.0 | 66.0 | 4.83 | |
| L Middle Frontal Gyrus | −10.0 | −11.0 | 58.0 | 3.15 | ||
| R Posterior Paracentral Lobule | 156 | 20.0 | −42.0 | 56.0 | 4.74 | |
| R Superior Frontal Gyrus | 68 | 10.0 | 24.0 | 52.0 | 4.48 | |
| L Insula | 64 | −38.0 | 14.0 | 10.0 | 4.13 | |
| L Insula | −38.0 | 22.0 | 12.0 | 4.11 | ||
| Positive Correlation between ∆PD (PD-T0 - PD-T1) and Brain Metabolism | ||||||
| Cluster Extent | Talairach Coordinates (mm) | T Score | ||||
| x | y | z | ||||
| Amnesic AD | ||||||
| R Inferior Frontal Gyrus | 121 | 42.0 | 7.0 | 33.0 | 5.43 | |
| lv-PPA | ||||||
| L Inferior Parietal Lobule | 85 | −50.0 | −31.0 | 33.0 | 6.77 | |
| R Superior Frontal Gyrus | 68 | 14.0 | −12.0 | 67.0 | 4.94 | |
| L Insula | 168 | −44.0 | 4.0 | 5.0 | 4.93 | |
| R Precuneus | 158 | 14.0 | −48.0 | 56.0 | 4.51 | |
| L Superior Frontal Gyrus | 77 | −12.0 | −14.0 | 67.0 | 4.42 | |
| L Superior Frontal Gyrus | −6.0 | −6.0 | 67.0 | 3.36 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Giacomucci, G.; Polito, C.; Berti, V.; Padiglioni, S.; Galdo, G.; Mazzeo, S.; Bergamin, E.; Moschini, V.; Morinelli, C.; Nuti, C.; et al. Differences and Similarities in Empathy Deficit and Its Neural Basis between Logopenic and Amnesic Alzheimer’s Disease. J. Pers. Med. 2023, 13, 208. https://doi.org/10.3390/jpm13020208
Giacomucci G, Polito C, Berti V, Padiglioni S, Galdo G, Mazzeo S, Bergamin E, Moschini V, Morinelli C, Nuti C, et al. Differences and Similarities in Empathy Deficit and Its Neural Basis between Logopenic and Amnesic Alzheimer’s Disease. Journal of Personalized Medicine. 2023; 13(2):208. https://doi.org/10.3390/jpm13020208
Chicago/Turabian StyleGiacomucci, Giulia, Cristina Polito, Valentina Berti, Sonia Padiglioni, Giulia Galdo, Salvatore Mazzeo, Enrico Bergamin, Valentina Moschini, Carmen Morinelli, Claudia Nuti, and et al. 2023. "Differences and Similarities in Empathy Deficit and Its Neural Basis between Logopenic and Amnesic Alzheimer’s Disease" Journal of Personalized Medicine 13, no. 2: 208. https://doi.org/10.3390/jpm13020208
APA StyleGiacomucci, G., Polito, C., Berti, V., Padiglioni, S., Galdo, G., Mazzeo, S., Bergamin, E., Moschini, V., Morinelli, C., Nuti, C., De Cristofaro, M. T., Ingannato, A., Bagnoli, S., Nacmias, B., Sorbi, S., & Bessi, V. (2023). Differences and Similarities in Empathy Deficit and Its Neural Basis between Logopenic and Amnesic Alzheimer’s Disease. Journal of Personalized Medicine, 13(2), 208. https://doi.org/10.3390/jpm13020208